
Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience

 , ,
, ,
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Diagnostic Procedures
2.3. Treatments
2.4. Adverse Events Reporting
2.5. Statistical Analysis
3. Results
3.1. Patients and Treatments
3.2. Biological Characteristics
3.3. Treatment Details
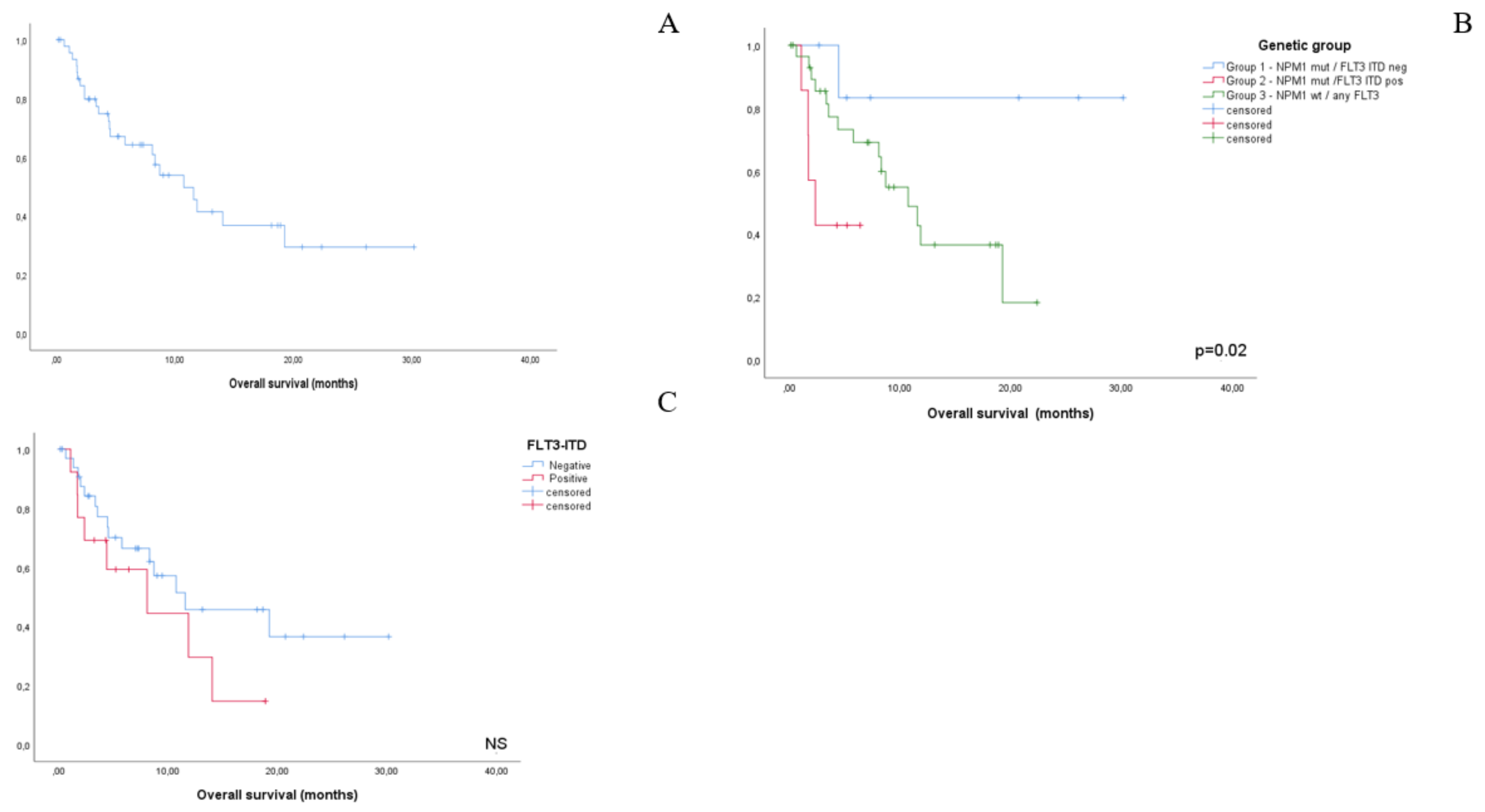
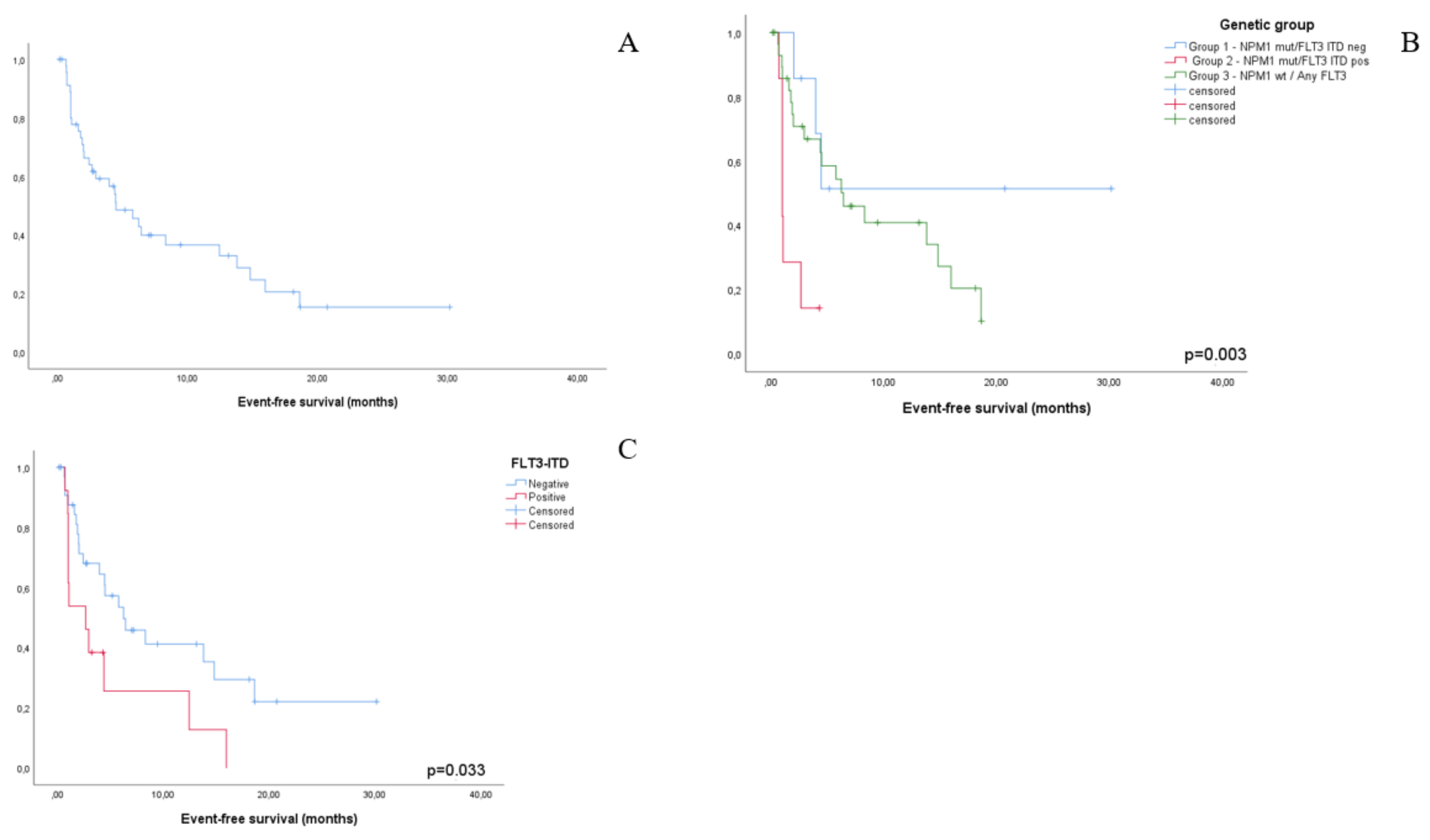
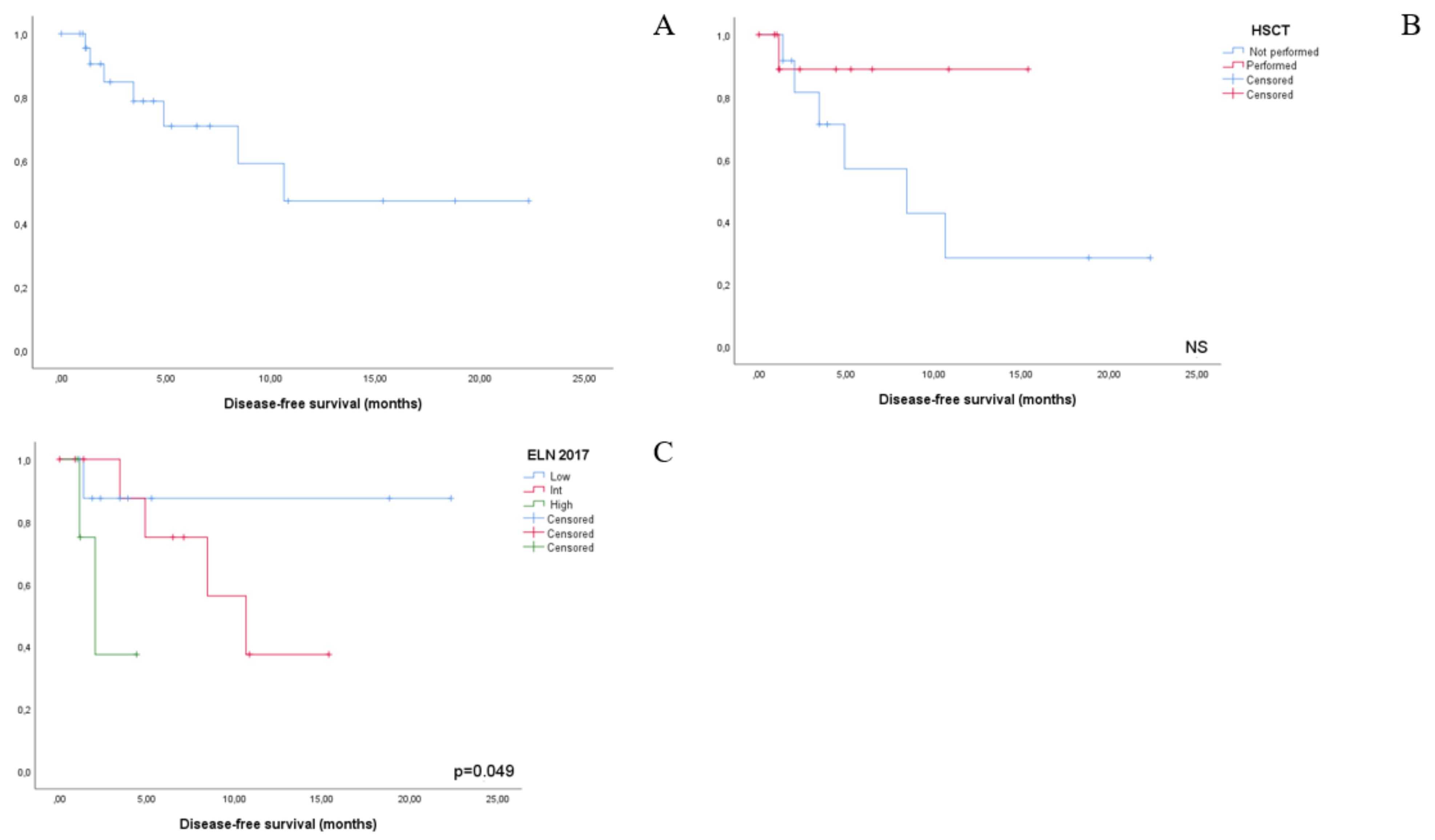
3.4. Outcomes
3.5. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Thol, F.; Schlenk, R.F.; Heuser, M.; Ganser, A. How I treat refractory and early relapsed acute myeloid leukemia. Blood 2015, 126, 319–327. [Google Scholar] [CrossRef]
- Megias-Vericat, J.D.; Martinez-Cauadron, D. Salvage regimens using conventional chemotherapy agents for relapsed a/refractory adult AML patients: A systematic literature review. Ann. Hematol. 2018, 97, 1115–1153. [Google Scholar] [CrossRef]
- Cortes, J.E.; Khaled, S. Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukemia (Quantum-R): A multicenter, randomized, controlled, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 984–997. [Google Scholar] [CrossRef]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef]
- Tzogani, K.; Roshold, H. The European Medicines Agency review of Gilteritinib (Xospata) for the treatment of adult patients with relapsed or refractory acute myeloid leukemia with an FLT3 mutation. Oncologist 2020, 25, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.M.; Dinardo, C.D.; Pollyea, D.A.; Fathi, A.T.; Roboz, G.J.; Altman, J.K.; Stone, R.M.; DeAngelo, D.J.; Levine, R.L.; Flinn, I.W.; et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood 2017, 130, 722–731. [Google Scholar] [CrossRef]
- Dinardo, C.D.; Stein, E.M.; De Botton, S.; Roboz, G.J.; Altman, J.K.; Mims, A.S.; Swords, R.; Collins, R.H.; Mannis, G.N.; Pollyea, D.A.; et al. Durable Remissions with Ivosidenib inIDH1-Mutated Relapsed or Refractory AML. N. Engl. J. Med. 2018, 378, 2386–2398. [Google Scholar] [CrossRef] [PubMed]
- Thol, F.; Ganser, A. Treatment of Relapsed Acute Myeloid Leukemia. Curr. Treat. Options Oncol. 2020, 21, 1–11. [Google Scholar] [CrossRef]
- Dinardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.H.; Montesinos, P. Venetoclax plus LDAC for newly diagnosed AML ineligible for intensive chemotherapy: A phase III randomised placebo-controlled trial. Blood 2020, 135, 2137–2145. [Google Scholar] [CrossRef]
- Konopleva, M.; Pollyea, D.A. Efficacy and biological correlates of response in aphase II study of Venetoclax monotherapy in patients with acute myelogenous leukemia. Cancer Discov. 2016, 6, 1106–1117. [Google Scholar] [CrossRef] [PubMed]
- Dinardo, C.D.; Rausch, C.R.; Benton, C.; Kadia, T.; Jain, N.; Pemmaraju, N.; Daver, N.; Covert, W.; Marx, K.R.; Mace, M.; et al. Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am. J. Hematol. 2018, 93, 401–407. [Google Scholar] [CrossRef]
- Aldoss, I.; Yang, D.; Aribi, A.; Ali, H.; Sandhu, K.; Al Malki, M.M.; Mei, M.; Salhotra, A.; Khaled, S.; Nakamura, R.; et al. Efficacy of the combination of venetoclax and hypomethylating agents in relapsed/refractory acute myeloid leukemia. Haematologica 2018, 103, e404–e407. [Google Scholar] [CrossRef]
- Wang, Y.W.; Tsai, C.H. Cytogenetics and mutations could predict outcome in relapsed and refractory acute myeloid leukemia patients receiving BCL-2 inhibitor venetoclax. Ann. Hematol. 2020, 99, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Ganzel, C.; Ram, R.; Gural, A.; Wolach, O.; Gino-Moor, S.; Vainstein, V.; Nachmias, B.; Apel, A.; Koren-Michowitz, M.; Pasvolsky, O.; et al. Venetoclax is safe and efficacious in relapsed/refractory AML. Leuk. Lymphoma 2020, 61, 2221–2225. [Google Scholar] [CrossRef]
- Dohner, H.; Estey, E. Diagnosis and management of AML in adults: 2017 ELN reccommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Falini, B.; Mecucci, C.; Tiacci, E.; Alcalay, M.; Rosati, R.; Pasqualucci, L.; La Starza, R.; Diverio, D.; Colombo, E.; Santucci, A.; et al. Cytoplasmic Nucleophosmin in Acute Myelogenous Leukemia with a Normal Karyotype. N. Engl. J. Med. 2005, 352, 254–266. [Google Scholar] [CrossRef]
- Noguera, N.I.; Ammatuna, E.; Zangrilli, D.; Lavorgna, S.; Divona, M.; Buccisano, F.; Amadori, S.; Mecucci, C.; Falini, B.; Lo-Coco, F. Simultaneous detection of NPM1 and FLT3-ITD mutations by capillary electrophoresis in acute myeloid leukemia. Leukemia 2005, 19, 1479–1482. [Google Scholar] [CrossRef] [PubMed]
- Preudhomme, C.; Sagot, C.; Boissel, N.; Cayuela, J.-M.; Tigaud, I.; De Botton, S.; Thomas, X.; Raffoux, E.; Lamandin, C.; Castaigne, S.; et al. Favorable prognostic significance of CEBPA mutations in patients with de novo acute myeloid leukemia: A study from the Acute Leukemia French Association (ALFA). Blood 2002, 100, 2717–2723. [Google Scholar] [CrossRef]
- Schlenk, R.F.; Kayser, S.; Bullinger, L.; Kobbe, G.; Casper, J.; Ringhoffer, M.; Held, G.; Brossart, P.; Lübbert, M.; Salih, H.R.; et al. Differential impact of allelic ratio and insertion site in FLT3-ITD-positive AML with respect to allogeneic transplantation. Blood 2014, 124, 3441–3449. [Google Scholar] [CrossRef] [PubMed]
- Jonas, B.A.; Pollyea, D.A. How we use venetoclax with hypomethylating agents for the treatment of newly diagnosed patients with acute myeloid leukemia. Leukemia 2019, 33, 2795–2804. [Google Scholar] [CrossRef]
- Shouval, R.; Bonifazi, F.; Fein, J.; Boschini, C.; Oldani, E.; Labopin, M.; Raimondi, R.; Sacchi, N.; Dabash, O.; Unger, R.; et al. Validation of the acute leukemia-EBMT score for prediction of mortality following allogeneic stem cell transplantation in a multi-center GITMO cohort. Am. J. Hematol. 2017, 92, 429–434. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health and National Cancer Institute. Common Terminology Criteria for AdverseEvents (CTCAE), v5.0; National Institutes of Health and National Cancer Institute: Bethesda, MD, USA, 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 1 March 2021).
- Pastore, D.; Specchia, G.; Carluccio, P.; Liso, A.; Mestice, A.; Rizzi, R.; Greco, G.; Buquicchio, C.; Liso, V. FLAG-IDA in the treatment of refractory/relapsed acute myeloid leukemia: Single-center experience. Ann. Hematol. 2003, 82, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Bejanyan, N.; Weisdorf, D.J.; Logan, B.R.; Wang, H.-L.; Devine, S.M.; De Lima, M.; Bunjes, D.W.; Zhang, M.-J. Survival of Patients with Acute Myeloid Leukemia Relapsing after Allogeneic Hematopoietic Cell Transplantation: A Center for International Blood and Marrow Transplant Research Study. Biol. Blood Marrow Transplant. 2015, 21, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Gianfaldoni, G.; Mannelli, F.; Intermesoli, T.; Bencini, S.; Giupponi, D.; Farina, G.; Cutini, I.; Bonetti, M.I.; Masciulli, A.; Audisio, E.; et al. Early peripheral clearance of leukemia-associated immunophenotypes in AML: Centralized analysis of a randomized trial. Blood Adv. 2020, 4, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Dinardo, C.D.; Jonas, B.A. Azacitidine and Venetoclax in previously untreated acute myeloid leukemia. NEJM 2020, 383, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Aldoss, I.; Zhang, J.; Mei, M.; Al Malki, M.M.; Arslan, S.; Ngo, D.; Aribi, A.; Ali, H.; Sandhu, K.; Salhotra, A.; et al. Venetoclax and hypomethylating agents in FLT3-mutated acute myeloid leukemia. Am. J. Hematol. 2020, 95, 1193–1199. [Google Scholar] [CrossRef]
- Daver, N.; Altman, J.K.; Maly, J.; Levis, M.; Ritchie, E.; Litzow, M.; McCloskey, J.K.; Smith, C.C.; Schiller, G.J.; Bradley, T.; et al. Efficacy and Safety of Venetoclax in Combination with Gilteritinib for Relapsed/Refractory FLT3-Mutated Acute Myeloid Leukemia in the Expansion Cohort of a Phase 1b Study. In Proceedings of the 62nd ASH Meeting 2020, San Diego, CA, USA, 5–8 December 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Parameter | n (%) |
|---|---|
| Patient number | 47 |
| Sex | |
| Male | 26 (55.3%) |
| Female | 21 (44.7%) |
| Median Age (range) | 56 (33–74) |
| Age ≥ 60 | 20 (42.5%) |
| Age ≥ 70 | 5 (10%) |
| De novo AML | 40 (85%) |
| Secondary AML | 7 (15%) MDS, n = 4 Therapy-related, n = 3 |
| ELN 2017 risk at diagnosis | |
| Favorable | 16 (34%) |
| Intermediate | 17 (36%) |
| Adverse | 7 (15%) |
| NA | 7 (15%) |
| NPM1/FLT3 status | |
| NPM1mut FLT3-ITDwt | 7 (15%) |
| NPM1mut FLT3-ITDpos | 6 (13%) |
| NPM1neg FLT3-ITDwt | 27 (57%) |
| NPM1neg FLT3-ITDpos | 7 (15%) |
| Cytogenetic risk | |
| Low risk | 5 (11%) |
| Intermediate risk | 31 (66%) |
| Poor risk | 8 (17%) |
| Unknow | 13 (28%) |
| Setting | |
| First relapse | 20 (43%) |
| Subsequent relapse | 5 (11%) |
| Relapse after HSCT | 11 (23%) |
| Partner drug | |
| Azacitidine | 29 (62%) |
| Decitabine | 5 (11%) |
| Low-dose cytarabine | 13 (28%) |
| Median cycle number (range) | 2 (1–24) |
| Intention to treat | |
| Intention to HSCT | 24 (51%) |
| Nointention to HSCT | 23 (49%) |
| HSCT performed | 13/24 (54%) |
| Total Patients (n = 47) | NPM1mut FLT3-ITDneg (n = 7) | NPM1mut FLT3-ITDpos (n = 6) | NPMwt FLT3any (n = 34) | |
|---|---|---|---|---|
| CCR—no. (%) CRi/CRp—no. (%) | 26 (55%) 13 (50% of all CCR patients) | |||
| SD—no. (%) | 6 (12%) | |||
| PD—no. (%) | 15 (32%) | |||
| DSF mo (median) | 10.6 | NR | (4.5) | (11.5) |
| EFS mo (median) | 4.5 | NR | (1) | (6.4) |
| OS mo (median) | 10.7 | NR | (2.03) | 10.7 |
| Adverse Events | n (%) |
|---|---|
| • Thrombocytopenia ≥ G4 | 45 (95.7%) |
| • Neutropenia ≥ G4 | 47 (100%) |
| • Febrile neutropenia | 21 (45%) |
| • Anemia ≥ G3 | 45 (95.7%) |
| • Infections | 17 (36%) |
| • Mucositis | 10 (21%) |
| • Tumor lysis syndrome | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccini, M.; Pilerci, S.; Merlini, M.; Grieco, P.; Scappini, B.; Bencini, S.; Peruzzi, B.; Caporale, R.; Signori, L.; Pancani, F.; et al. Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience. J. Clin. Med. 2021, 10, 1684. https://doi.org/10.3390/jcm10081684
Piccini M, Pilerci S, Merlini M, Grieco P, Scappini B, Bencini S, Peruzzi B, Caporale R, Signori L, Pancani F, et al. Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience. Journal of Clinical Medicine. 2021; 10(8):1684. https://doi.org/10.3390/jcm10081684
Chicago/Turabian StylePiccini, Matteo, Sofia Pilerci, Marta Merlini, Pietro Grieco, Barbara Scappini, Sara Bencini, Benedetta Peruzzi, Roberto Caporale, Leonardo Signori, Fabiana Pancani, and et al. 2021. "Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience" Journal of Clinical Medicine 10, no. 8: 1684. https://doi.org/10.3390/jcm10081684
APA StylePiccini, M., Pilerci, S., Merlini, M., Grieco, P., Scappini, B., Bencini, S., Peruzzi, B., Caporale, R., Signori, L., Pancani, F., Vannucchi, A. M., & Gianfaldoni, G. (2021). Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience. Journal of Clinical Medicine, 10(8), 1684. https://doi.org/10.3390/jcm10081684