
Delayed Improvement of Depression and Anxiety after Transcatheter Aortic Valve Implantation (TAVI) in Stages of Extended Extra-Valvular Cardiac Damage

 ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Cohort
2.2. Acquisition of Depression and Anxiety, Quality of Life and Health Status
2.3. Assessment of the Level of Extra-Valvular Cardiac Damage According to the 2017 Staging Classification
2.4. Statistics
3. Results
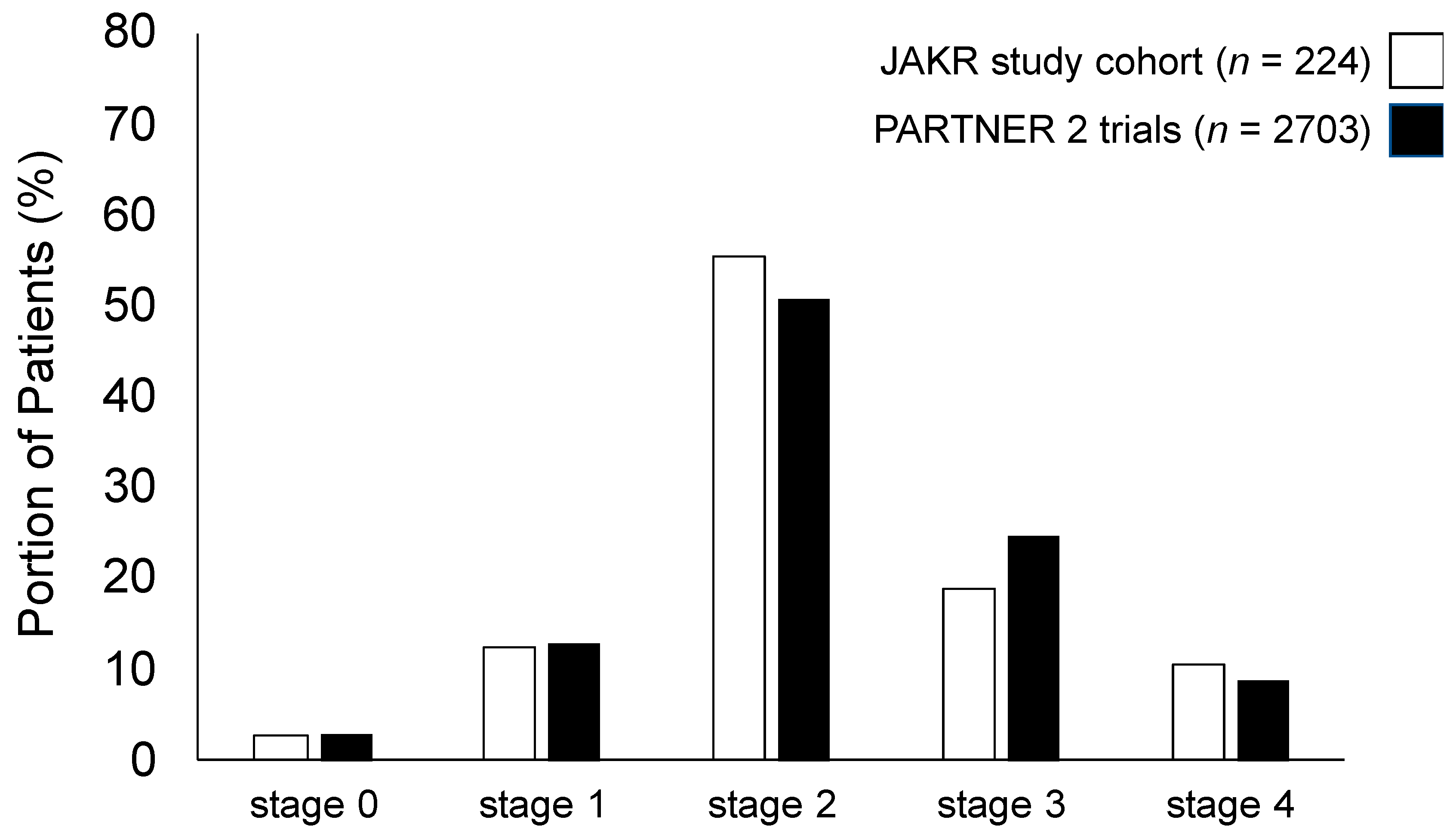
3.1. Characterization of the Study Population and Assignment to the Staging Classification of Extra-Valvular Cardiac Damage
3.2. Assessment of Depression and Anxiety Prior to TAVI
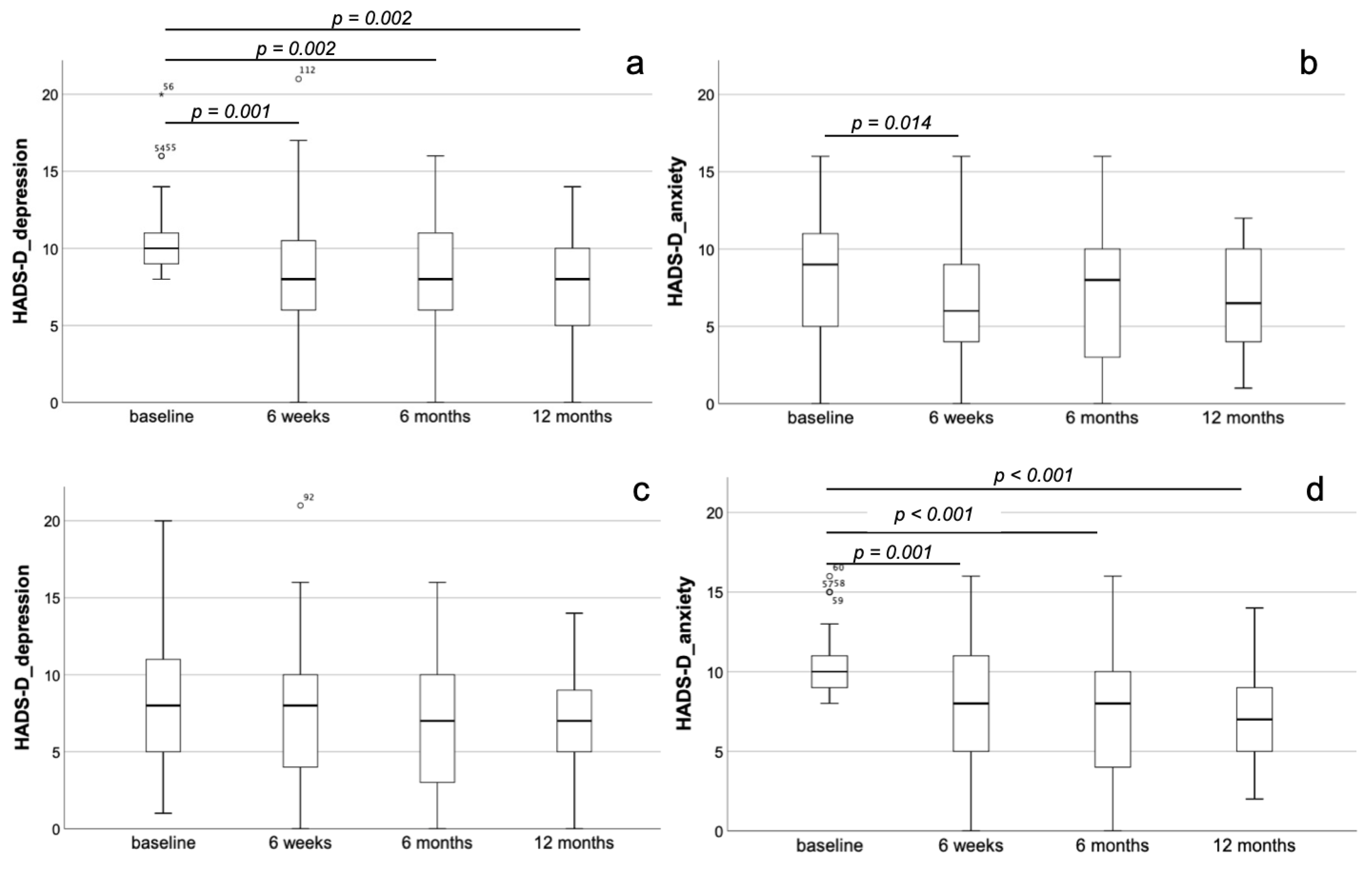
3.3. Dynamics of Depression and Anxiety in Short- and Long-Term Follow-Up after TAVI
3.4. Predefined Subgroups According to Depression and Anxiety (HADS-D) in the Entire Collective
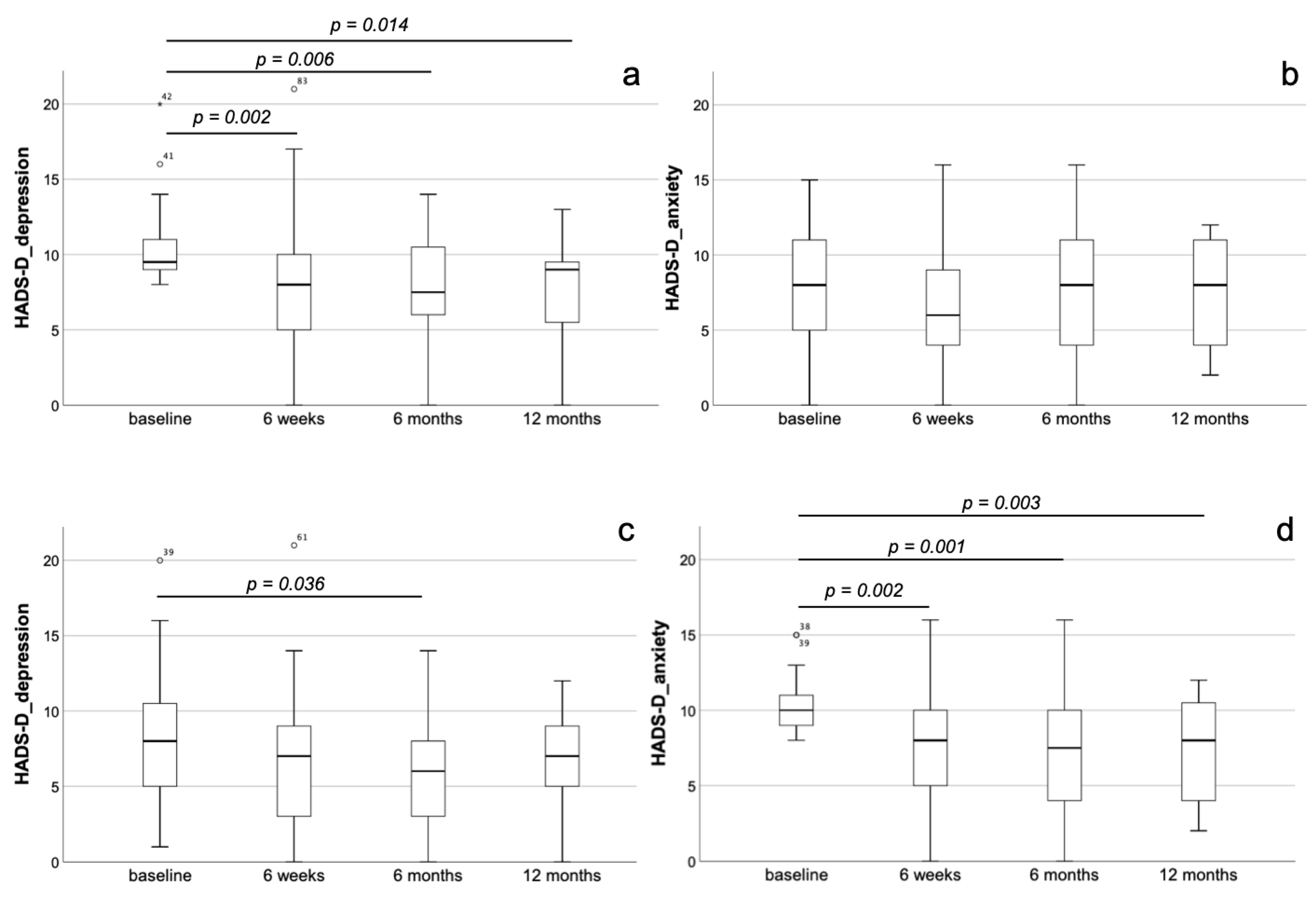
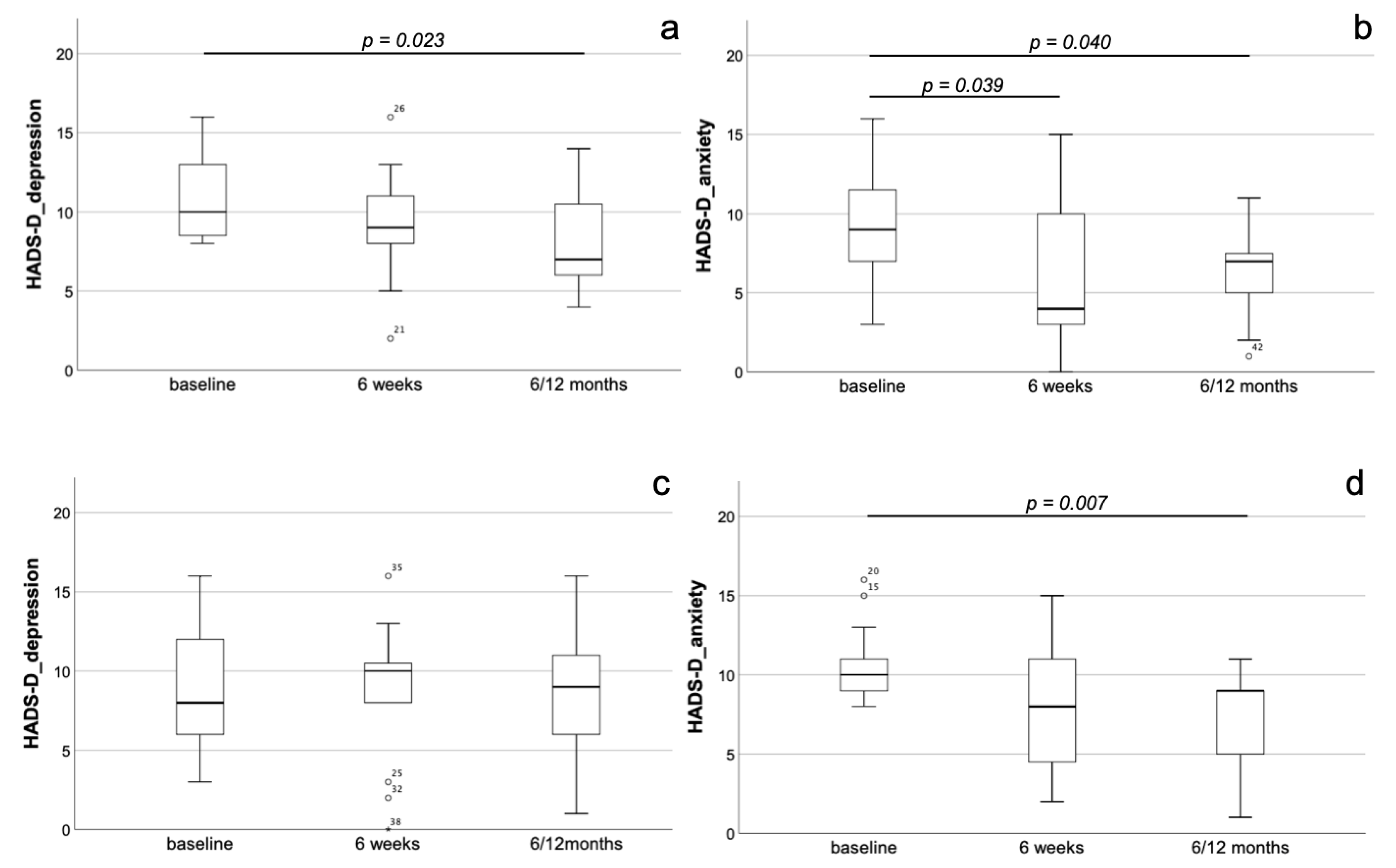
3.5. Predefined Subgroups According to Depression and Anxiety (HADS-D) Comparing Staging Group A and B
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Widder, J.D.; Bauersachs, J. Therapy of aortic valve stenosis. Internist 2014, 55, 1391–1392. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Munoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Spaccarotella, C.; Mongiardo, A.; Indolfi, C. Pathophysiology of aortic stenosis and approach to treatment with percutaneous valve implantation. Circ. J. 2011, 75, 11–19. [Google Scholar] [CrossRef]
- Figulla, H.R.; Franz, M.; Lauten, A. The history of Transcatheter Aortic Valve Implantation (TAVI)-A personal view over 25years of development. Cardiovasc. Revasc. Med. 2019. [Google Scholar] [CrossRef]
- Deeb, G.M.; Reardon, M.J.; Chetcuti, S.; Patel, H.J.; Grossman, P.M.; Yakubov, S.J.; Kleiman, N.S.; Coselli, J.S.; Gleason, T.G.; Lee, J.S.; et al. 3-Year Outcomes in High-Risk Patients Who Underwent Surgical or Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 67, 2565–2574. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Sondergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef]
- Sondergaard, L.; Steinbruchel, D.A.; Ihlemann, N.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Ngo, A.T.; Olsen, N.T.; Chang, Y.; Franzen, O.W.; et al. Two-Year Outcomes in Patients With Severe Aortic Valve Stenosis Randomized to Transcatheter Versus Surgical Aortic Valve Replacement: The All-Comers Nordic Aortic Valve Intervention Randomized Clinical Trial. Circ. Cardiovasc. Interv. 2016, 9. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Boureau, A.S.; Trochu, J.N.; Rouaud, A.; Hureau, R.; Jaafar, P.; Manigold, T.; Letocart, V.; Guerin, P.; Berrut, G.; de Decker, L. Predictors of Health-Related Quality of Life Decline after Transcatheter Aortic Valve Replacement in Older Patients with Severe Aortic Stenosis. J. Nutr. Health Aging 2017, 21, 105–111. [Google Scholar] [CrossRef]
- Celano, C.M.; Villegas, A.C.; Albanese, A.M.; Gaggin, H.K.; Huffman, J.C. Depression and Anxiety in Heart Failure: A Review. Harv. Rev. Psychiatry 2018, 26, 175–184. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, e28–e292. [Google Scholar] [CrossRef]
- Huffman, J.C.; Celano, C.M.; Beach, S.R.; Motiwala, S.R.; Januzzi, J.L. Depression and cardiac disease: Epidemiology, mechanisms, and diagnosis. Cardiovasc. Psychiatry Neurol. 2013, 2013, 695925. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, J.H.; Froelicher, E.S.; Blumenthal, J.A.; Carney, R.M.; Doering, L.V.; Frasure-Smith, N.; Freedland, K.E.; Jaffe, A.S.; Leifheit-Limson, E.C.; Sheps, D.S.; et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: Systematic review and recommendations: A scientific statement from the American Heart Association. Circulation 2014, 129, 1350–1369. [Google Scholar] [CrossRef]
- Thombs, B.D.; de Jonge, P.; Coyne, J.C.; Whooley, M.A.; Frasure-Smith, N.; Mitchell, A.J.; Zuidersma, M.; Eze-Nliam, C.; Lima, B.B.; Smith, C.G.; et al. Depression screening and patient outcomes in cardiovascular care: A systematic review. JAMA 2008, 300, 2161–2171. [Google Scholar] [CrossRef] [PubMed]
- Somberg, T.C.; Arora, R.R. Depression and heart disease: Therapeutic implications. Cardiology 2008, 111, 75–81. [Google Scholar] [CrossRef]
- Williams, J.B.; Alexander, K.P.; Morin, J.F.; Langlois, Y.; Noiseux, N.; Perrault, L.P.; Smolderen, K.; Arnold, S.V.; Eisenberg, M.J.; Pilote, L.; et al. Preoperative anxiety as a predictor of mortality and major morbidity in patients aged >70 years undergoing cardiac surgery. Am. J. Cardiol. 2013, 111, 137–142. [Google Scholar] [CrossRef]
- Lange, R.; Beckmann, A.; Neumann, T.; Krane, M.; Deutsch, M.A.; Landwehr, S.; Kotting, J.; Welz, A.; Zahn, R.; Cremer, J.; et al. Quality of Life after Transcatheter Aortic Valve Replacement: Prospective Data from GARY (German Aortic Valve Registry). JACC Cardiovasc. Interv. 2016, 9, 2541–2554. [Google Scholar] [CrossRef]
- Drudi, L.M.; Ades, M.; Turkdogan, S.; Huynh, C.; Lauck, S.; Webb, J.G.; Piazza, N.; Martucci, G.; Langlois, Y.; Perrault, L.P.; et al. Association of Depression With Mortality in Older Adults Undergoing Transcatheter or Surgical Aortic Valve Replacement. JAMA Cardiol. 2018, 3, 191–197. [Google Scholar] [CrossRef]
- Baz, L.; Wiesel, M.; Mobius-Winkler, S.; Westphal, J.G.; Schulze, P.C.; Franz, M.; Dannberg, G. Depression and anxiety in elderly patients with severe symptomatic aortic stenosis persistently improves after transcatheter aortic valve replacement (TAVR). Int. J. Cardiol. 2020, 309, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Genereux, P.; Pibarot, P.; Redfors, B.; Mack, M.J.; Makkar, R.R.; Jaber, W.A.; Svensson, L.G.; Kapadia, S.; Tuzcu, E.M.; Thourani, V.H.; et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur. Heart J. 2017, 38, 3351–3358. [Google Scholar] [CrossRef] [PubMed]
- Hermann-Lingen, C.; Buss, K.; Snaith, R.P. Hospital Anxiety and Depression Scale—Deutsche Version (HADS-D), 3rd ed.; Verlag Hans Huber: Bern, Germany, 2011. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Snaith, R.P. The Hospital Anxiety and Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [PubMed]
- EuroQol, G. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Bagienski, M.; Kleczynski, P.; Dziewierz, A.; Rzeszutko, L.; Sorysz, D.; Trebacz, J.; Sobczynski, R.; Tomala, M.; Stapor, M.; Dudek, D. Incidence of Postoperative Delirium and Its Impact on Outcomes After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2017, 120, 1187–1192. [Google Scholar] [CrossRef]
- Nechwatal, R.M.; Duck, C.; Gruber, G. Physical training as interval or continuous training in chronic heart failure for improving functional capacity, hemodynamics and quality of life—A controlled study. Z. Kardiol. 2002, 91, 328–337. [Google Scholar] [CrossRef]
- Abdelbasset, W.K.; Alqahtani, B.A. A randomized controlled trial on the impact of moderate-intensity continuous aerobic exercise on the depression status of middle-aged patients with congestive heart failure. Medicine 2019, 98, e15344. [Google Scholar] [CrossRef]
- Lossnitzer, N.; Feisst, M.; Wild, B.; Katus, H.A.; Schultz, J.H.; Frankenstein, L.; Stock, C. Cross-lagged analyses of the bidirectional relationship between depression and markers of chronic heart failure. Depress. Anxiety 2020, 37, 898–907. [Google Scholar] [CrossRef]
- Xiong, G.L.; Fiuzat, M.; Kuchibhatla, M.; Krishnan, R.; O’Connor, C.M.; Jiang, W.; Investigators, S.-C. Health status and depression remission in patients with chronic heart failure: Patient-reported outcomes from the SADHART-CHF trial. Circ. Heart Fail. 2012, 5, 688–692. [Google Scholar] [CrossRef]
- Chiala, O.; Vellone, E.; Klompstra, L.; Ortali, G.A.; Stromberg, A.; Jaarsma, T. Relationships between exercise capacity and anxiety, depression, and cognition in patients with heart failure. Heart Lung 2018, 47, 465–470. [Google Scholar] [CrossRef]
- Newhouse, A.; Jiang, W. Heart failure and depression. Heart Fail. Clin. 2014, 10, 295–304. [Google Scholar] [CrossRef]
- Aguiar, V.B.; Ochiai, M.E.; Cardoso, J.N.; Del Carlo, C.H.; Morgado, P.C.; Munhoz, R.T.; Pereira-Barretto, A.C. Relationship between depression, BNP levels and ventricular impairment in heart failure. Arq. Bras. Cardiol. 2010, 95, 732–737. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dikic, A.; Radmilo, L.; Zivanovic, Z.; Kekovic, G.; Sekulic, S.; Kovacic, Z.; Radmilo, R. Cognitive impairment and depression after acute myocardial infarction: Associations with ejection fraction and demographic characteristics. Acta Neurol. Belg. 2020. [Google Scholar] [CrossRef]
- Kato, N.; Kinugawa, K.; Shiga, T.; Hatano, M.; Takeda, N.; Imai, Y.; Watanabe, M.; Yao, A.; Hirata, Y.; Kazuma, K.; et al. Depressive symptoms are common and associated with adverse clinical outcomes in heart failure with reduced and preserved ejection fraction. J. Cardiol. 2012, 60, 23–30. [Google Scholar] [CrossRef]
- Jiang, W.; Alexander, J.; Christopher, E.; Kuchibhatla, M.; Gaulden, L.H.; Cuffe, M.S.; Blazing, M.A.; Davenport, C.; Califf, R.M.; Krishnan, R.R.; et al. Relationship of depression to increased risk of mortality and rehospitalization in patients with congestive heart failure. Arch. Intern. Med. 2001, 161, 1849–1856. [Google Scholar] [CrossRef]
- Sherwood, A.; Blumenthal, J.A.; Trivedi, R.; Johnson, K.S.; O’Connor, C.M.; Adams, K.F., Jr.; Dupree, C.S.; Waugh, R.A.; Bensimhon, D.R.; Gaulden, L.; et al. Relationship of depression to death or hospitalization in patients with heart failure. Arch. Intern. Med. 2007, 167, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.K.; Hsu, B.C.; Li, Y.D.; Chen, C.H.; Lin, J.W.; Chien, C.Y.; Weng, C.Y. Prognostic Value of Anxiety Between Heart Failure With Reduced Ejection Fraction and Heart Failure With Preserved Ejection Fraction. J. Am. Heart Assoc. 2019, 8, e010739. [Google Scholar] [CrossRef]
- Munyombwe, T.; Hall, M.; Dondo, T.B.; Alabas, O.A.; Gerard, O.; West, R.M.; Pujades-Rodriguez, M.; Hall, A.; Gale, C.P. Quality of life trajectories in survivors of acute myocardial infarction: A national longitudinal study. Heart 2020, 106, 33–39. [Google Scholar] [CrossRef]
- Evangelista, L.S.; Dracup, K.; Moser, D.K.; Westlake, C.; Erickson, V.; Hamilton, M.A.; Fonarow, G.C. Two-year follow-up of quality of life in patients referred for heart transplant. Heart Lung 2005, 34, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.; Santos, M.; Vicente, M.; Furtado, I.; Cruz, C.; Melo, A.; Carvalho, L.; Goncalves, F.; Sa-Couto, P.; Almeida, L. Health-Related Quality of Life in Pulmonary Hypertension and Its Clinical Correlates: A Cross-Sectional Study. Biomed. Res. Int. 2018, 2018, 3924517. [Google Scholar] [CrossRef] [PubMed]
- Cassady, S.J.; Ramani, G.V. Right Heart Failure in Pulmonary Hypertension. Cardiol. Clin. 2020, 38, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Rymuza, B.; Zbroński, K.; Scisło, P.; Wilimski, R.; Kochman, J.; Ćwiek, A.; Filipiak, K.J.; Opolski, G.; Huczek, Z. Left ventricular remodelling pattern and its relation to clinical outcomes in patients with severe aortic stenosis treated with transcatheter aortic valve implantation. Postepy Kardiol. Interwencyjnej 2017, 13, 288–294. [Google Scholar] [CrossRef]
- Rymuza, B.; Zbroński, K.; Scisło, P.; Grodecki, K.; Kochman, J.; Filipiak, K.J.; Opolski, G.; Huczek, Z. Thromboelastography for predicting bleeding in patients with aortic stenosis treated with transcatheter aortic valve implantation. Kardiol. Pol. 2018, 76, 418–425. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients (n = 224) | Staging Group A (n = 158) | Staging Group B (n = 66) | p-Value (Staging Group A vs. Group B) |
|---|---|---|---|---|
| Age (years) | 77.9 ± 7.5 | 77.5 ± 7.5 | 78.7 ± 7.5 | n.s. |
| Male (%) | 45.1 | 44.3 | 47 | n.s. |
| STS score | 4.4 ± 3.1 | 3.9 ± 2.5 | 5.5 ± 3.8 | 0.005 |
| NYHA stage > II (%) | 72.4 (n = 221) | 70.7 (n = 157) | 76.6 (n = 64) | n.s. |
| Angina pectoris (%) | 30 (n = 223) | 31 | 27.7 (n = 65) | n.s. |
| CAD (%) | 61.6 | 56.3 | 74.2 | 0.012 |
| PAD (%) | 12.5 | 12 | 13.6 | n.s. |
| Diabetes (%) | 41.7 | 44.9 | 34.8 | n.s. |
| COPD (%) | 18.3 | 20.9 | 12.1 | n.s. |
| Atrial fibrillation (%) | 46.6 (n = 223) | 35 (n = 157) | 74.2 | <0.001 |
| Pacemaker pre TAVI (%) | 13.4 | 12.7 | 15.2 | n.s. |
| GFR ≤ 30 mL/min. (%) | 16.1 | 13.9 | 21.2 | n.s. |
| BNP ≥ 100 (%) | 90.2 (n = 205) | 87.4 (n = 143) | 90.9 (n = 62) | 0.038 |
| LVEF (%) | 58.6 ± 14.3 (n = 221) | 60.7 ± 13 | 53.6 ± 16 | 0.001 |
| Mitral regurgitation ≥ II° (%) | 36.5 (n = 222) | 26.9 (156) | 56.1 | <0.001 |
| Tricuspid regurgitation ≥ II° (%) | 24.9 (n = 221) | 0 | 78.8 | <0.001 |
| Stage 0–4 (%) | ||||
| 0 | 2.7 | 3.8 | - | |
| 1 | 12.5 | 17.7 | - | |
| 2 | 55.4 | 78.5 | - | |
| 3 | 18.8 | - | 63.6 | |
| 4 | 10.7 | - | 36.4 | |
| Edwards Sapien 3 (%) | 62.9 | 63.3 | 62.1 | n.s. |
| CoreValve Evolut (%) | 36.2 | 36.1 | 36.4 | n.s. |
| Acurate neo (%) | 0.9 | 0.6 | 1.5 | n.s. |
| HADS-D_depression ≥ 8 (%) | 25.4 | 26.6 | 22.7 | n.s. |
| HADS-D_anxiety ≥ 8 (%) | 26.8 | 24.7 | 31.8 | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bäz, L.; Puscholt, M.; Lasch, C.; Diab, M.; Möbius-Winkler, S.; Schulze, P.C.; Dannberg, G.; Franz, M. Delayed Improvement of Depression and Anxiety after Transcatheter Aortic Valve Implantation (TAVI) in Stages of Extended Extra-Valvular Cardiac Damage. J. Clin. Med. 2021, 10, 1579. https://doi.org/10.3390/jcm10081579
Bäz L, Puscholt M, Lasch C, Diab M, Möbius-Winkler S, Schulze PC, Dannberg G, Franz M. Delayed Improvement of Depression and Anxiety after Transcatheter Aortic Valve Implantation (TAVI) in Stages of Extended Extra-Valvular Cardiac Damage. Journal of Clinical Medicine. 2021; 10(8):1579. https://doi.org/10.3390/jcm10081579
Chicago/Turabian StyleBäz, Laura, Marisa Puscholt, Claudia Lasch, Mahmoud Diab, Sven Möbius-Winkler, P. Christian Schulze, Gudrun Dannberg, and Marcus Franz. 2021. "Delayed Improvement of Depression and Anxiety after Transcatheter Aortic Valve Implantation (TAVI) in Stages of Extended Extra-Valvular Cardiac Damage" Journal of Clinical Medicine 10, no. 8: 1579. https://doi.org/10.3390/jcm10081579
APA StyleBäz, L., Puscholt, M., Lasch, C., Diab, M., Möbius-Winkler, S., Schulze, P. C., Dannberg, G., & Franz, M. (2021). Delayed Improvement of Depression and Anxiety after Transcatheter Aortic Valve Implantation (TAVI) in Stages of Extended Extra-Valvular Cardiac Damage. Journal of Clinical Medicine, 10(8), 1579. https://doi.org/10.3390/jcm10081579