
Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity



Abstract
1. Introduction
2. Materials and Methods
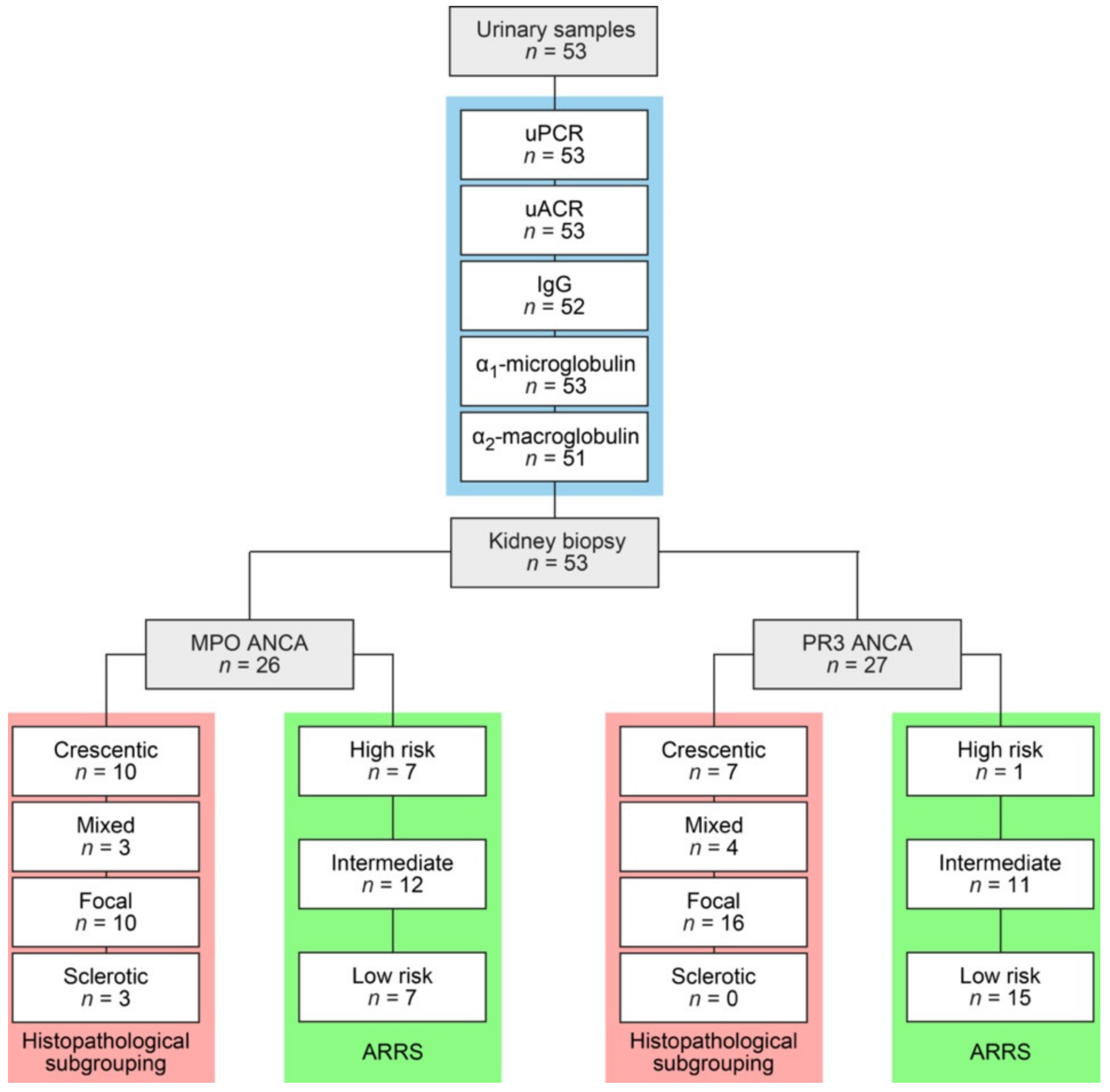
2.1. Study Population
2.2. Urinary Analysis
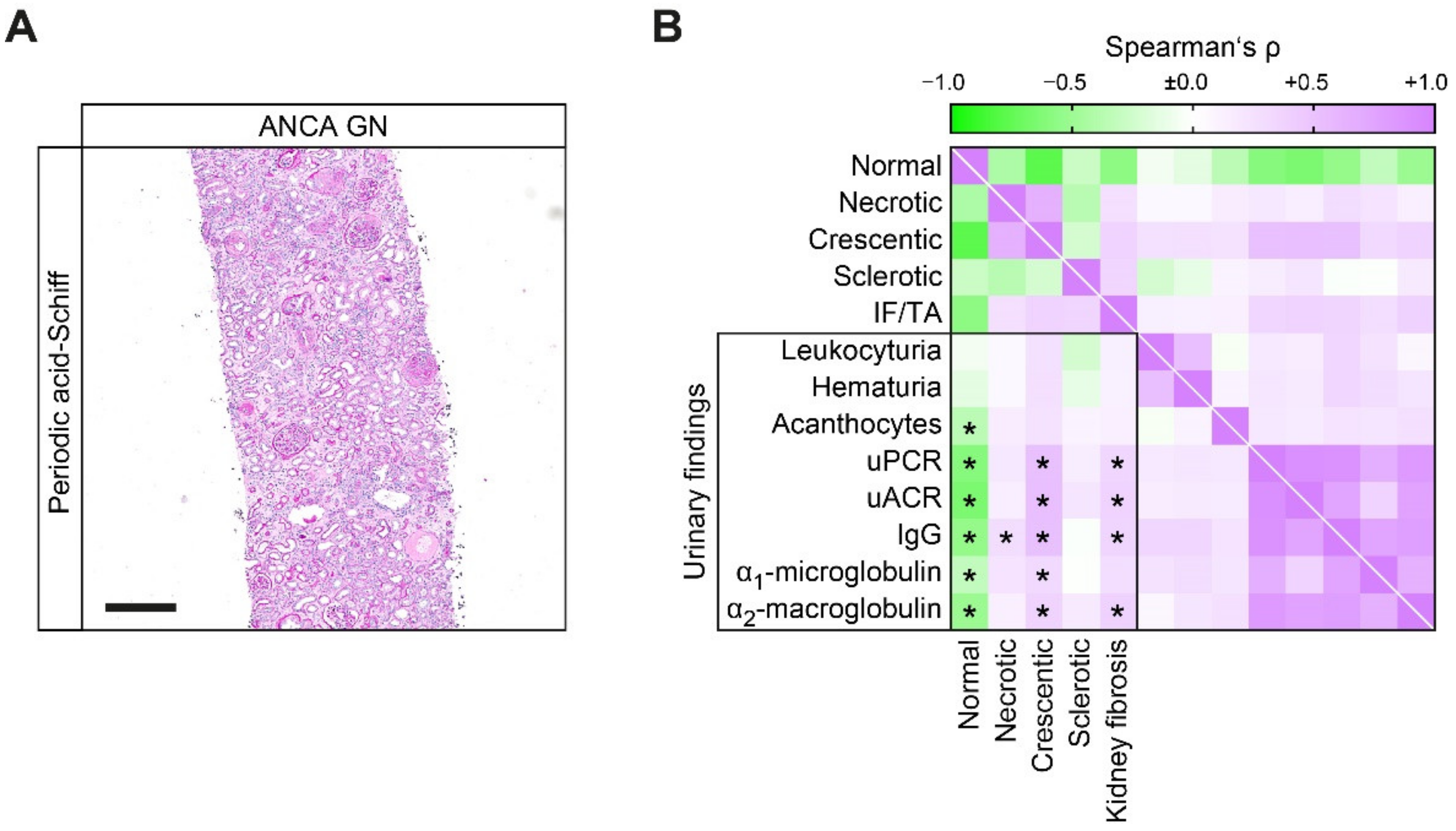
2.3. Renal Histopathology
2.4. Statistical Methods
3. Results
3.1. Proteinuric Findings in ANCA GN
3.2. Proteinuric Findings in Correlation with Histopathological Findings in ANCA GN
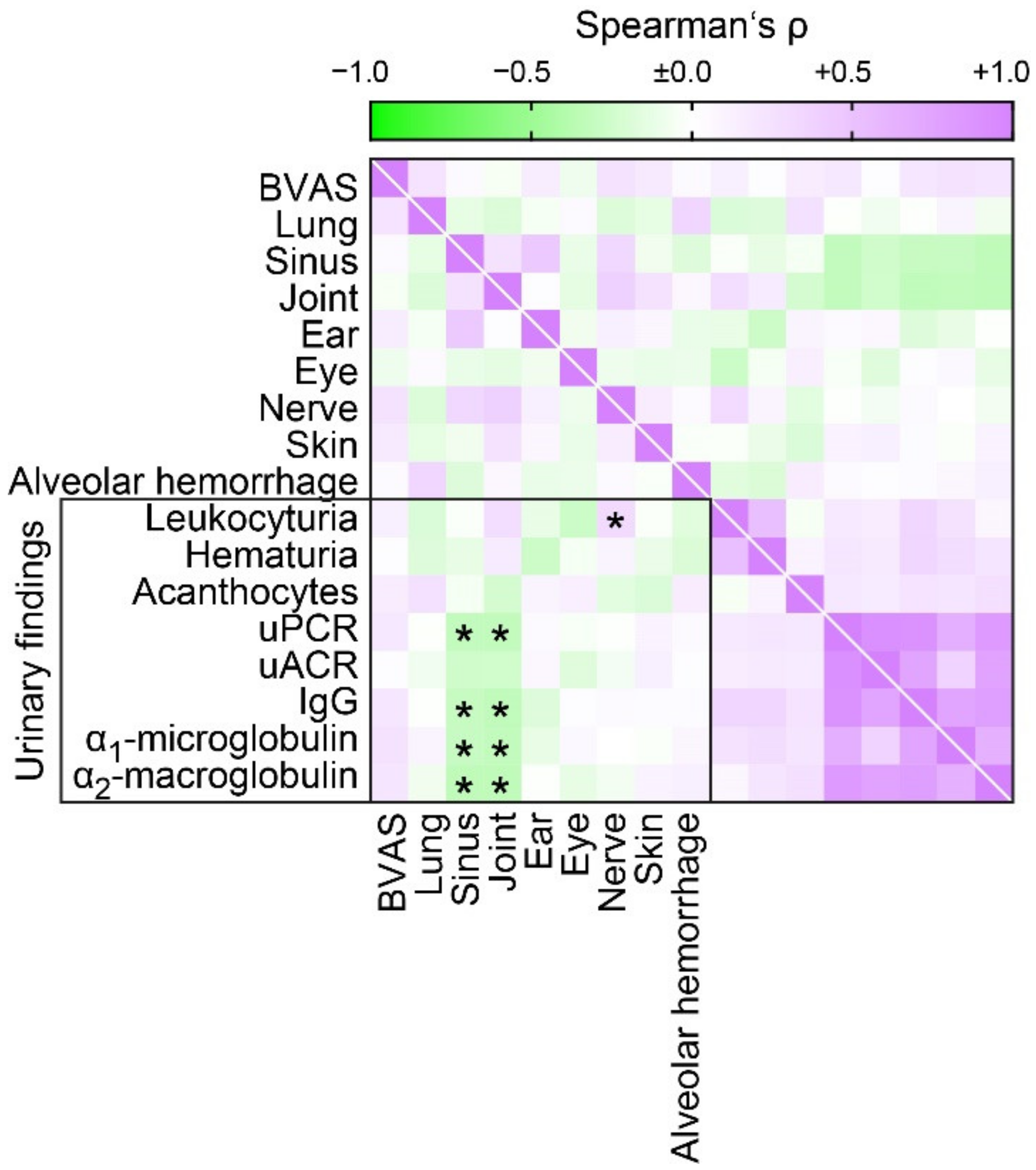
3.3. Proteinuric Findings in Correlation with Extrarenal Manifestations of AAV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hruskova, Z.; Stel, V.S.; Jayne, D.; Aasarod, K.; De Meester, J.; Ekstrand, A.; Eller, K.; Heaf, J.G.; Hoitsma, A.; Martos Jimenez, C.; et al. Characteristics and Outcomes of Granulomatosis With Polyangiitis (Wegener) and Microscopic Polyangiitis Requiring Renal Replacement Therapy: Results From the European Renal Association-European Dialysis and Transplant Association Registry. Am. J. Kidney Dis. 2015, 66, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Demiselle, J.; Auchabie, J.; Beloncle, F.; Gatault, P.; Grange, S.; Du Cheyron, D.; Dellamonica, J.; Boyer, S.; Beauport, D.T.; Piquilloud, L.; et al. Patients with ANCA-associated vasculitis admitted to the intensive care unit with acute vasculitis manifestations: A retrospective and comparative multicentric study. Ann. Intensive Care 2017, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Hagen, E.C.; Hermans, J.; Noel, L.H.; Waldherr, R.; Ferrario, F.; Van Der Woude, F.J.; Bruijn, J.A. Kidney biopsy as a predictor for renal outcome in ANCA-associated necrotizing glomerulonephritis. Kidney Int. 1999, 56, 1751–1758. [Google Scholar] [CrossRef] [PubMed]
- Hauer, H.A.; Bajema, I.M.; Van Houwelingen, H.C.; Ferrario, F.; Noel, L.H.; Waldherr, R.; Jayne, D.R.; Rasmussen, N.; Bruijn, J.A.; Hagen, E.C.; et al. Determinants of outcome in ANCA-associated glomerulonephritis: A prospective clinico-histopathological analysis of 96 patients. Kidney Int. 2002, 62, 1732–1742. [Google Scholar] [CrossRef]
- Van Wijngaarden, R.A.D.L.; Hauer, H.A.; Wolterbeek, R.; Jayne, D.R.; Gaskin, G.; Rasmussen, N.; Noel, L.H.; Ferrario, F.; Waldherr, R.; Hagen, E.C.; et al. Clinical and histologic determinants of renal outcome in ANCA-associated vasculitis: A prospective analysis of 100 patients with severe renal involvement. J. Am. Soc. Nephrol. 2006, 17, 2264–2274. [Google Scholar] [CrossRef]
- Bajema, I.M.; Hagen, E.C.; Hansen, B.E.; Hermans, J.; Noel, L.H.; Waldherr, R.; Ferrario, F.; van der Woude, F.J.; Bruijn, J.A. The renal histopathology in systemic vasculitis: An international survey study of inter- and intra-observer agreement. Nephrol. Dial. Transplant. 1996, 11, 1989–1995. [Google Scholar] [CrossRef]
- Berden, A.E.; Ferrario, F.; Hagen, E.C.; Jayne, D.R.; Jennette, J.C.; Joh, K.; Neumann, I.; Noel, L.H.; Pusey, C.D.; Waldherr, R.; et al. Histopathologic classification of ANCA-associated glomerulonephritis. J. Am. Soc. Nephrol. 2010, 21, 1628–1636. [Google Scholar] [CrossRef]
- Chang, D.Y.; Wu, L.H.; Liu, G.; Chen, M.; Kallenberg, C.G.; Zhao, M.H. Re-evaluation of the histopathologic classification of ANCA-associated glomerulonephritis: A study of 121 patients in a single center. Nephrol. Dial. Transplant. 2012, 27, 2343–2349. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ellis, C.L.; Manno, R.L.; Havill, J.P.; Racusen, L.C.; Geetha, D. Validation of the new classification of pauci-immune glomerulonephritis in a United States cohort and its correlation with renal outcome. BMC Nephrol. 2013, 14, 210. [Google Scholar] [CrossRef]
- Togashi, M.; Komatsuda, A.; Nara, M.; Omokawa, A.; Okuyama, S.; Sawada, K.; Wakui, H. Validation of the 2010 histopathological classification of ANCA-associated glomerulonephritis in a Japanese single-center cohort. Mod. Rheumatol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Rahmattulla, C.; Bruijn, J.A.; Bajema, I.M. Histopathological classification of antineutrophil cytoplasmic antibody-associated glomerulonephritis: An update. Curr. Opin. Nephrol. Hypertens. 2014, 23, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Gasim, A.; Derebail, V.K.; Chung, Y.; McGregor, J.G.; Lionaki, S.; Poulton, C.J.; Hogan, S.L.; Jennette, J.C.; Falk, R.J.; et al. Predictors of treatment outcomes in ANCA-associated vasculitis with severe kidney failure. Clin. J. Am. Soc. Nephrol. 2014, 9, 905–913. [Google Scholar] [CrossRef]
- Diaz-Crespo, F.; Villacorta, J.; Acevedo, M.; Cavero, T.; Guerrero, C.; Garcia Diaz, E.; Orradre, J.L.; Martinez, M.A.; Praga, M.; Fernandez-Juarez, G. The predictive value of kidney biopsy in renal vasculitis: A multicenter cohort study. Hum. Pathol. 2016, 52, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Nohr, E.; Girard, L.; James, M.; Benediktsson, H. Validation of a histopathologic classification scheme for antineutrophil cytoplasmic antibody-associated glomerulonephritis. Hum. Pathol. 2014, 45, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Noone, D.G.; Twilt, M.; Hayes, W.N.; Thorner, P.S.; Benseler, S.; Laxer, R.M.; Parekh, R.S.; Hebert, D. The new histopathologic classification of ANCA-associated GN and its association with renal outcomes in childhood. Clin. J. Am. Soc. Nephrol. 2014, 9, 1684–1691. [Google Scholar] [CrossRef]
- Quintana, L.F.; Perez, N.S.; De Sousa, E.; Rodas, L.M.; Griffiths, M.H.; Sole, M.; Jayne, D. ANCA serotype and histopathological classification for the prediction of renal outcome in ANCA-associated glomerulonephritis. Nephrol. Dial. Transplant. 2014, 29, 1764–1769. [Google Scholar] [CrossRef] [PubMed]
- Hilhorst, M.; Wilde, B.; van Breda Vriesman, P.; van Paassen, P.; Cohen Tervaert, J.W.; Limburg Renal, R. Estimating renal survival using the ANCA-associated GN classification. J. Am. Soc. Nephrol. 2013, 24, 1371–1375. [Google Scholar] [CrossRef]
- Iwakiri, T.; Fujimoto, S.; Kitagawa, K.; Furuichi, K.; Yamahana, J.; Matsuura, Y.; Yamashita, A.; Uezono, S.; Shimao, Y.; Hisanaga, S.; et al. Validation of a newly proposed histopathological classification in Japanese patients with anti-neutrophil cytoplasmic antibody-associated glomerulonephritis. BMC Nephrol. 2013, 14, 125. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ford, S.L.; Polkinghorne, K.R.; Longano, A.; Dowling, J.; Dayan, S.; Kerr, P.G.; Holdsworth, S.R.; Kitching, A.R.; Summers, S.A. Histopathologic and clinical predictors of kidney outcomes in ANCA-associated vasculitis. Am. J. Kidney Dis. 2014, 63, 227–235. [Google Scholar] [CrossRef]
- Naidu, G.S.; Sharma, A.; Nada, R.; Kohli, H.S.; Jha, V.; Gupta, K.L.; Sakhuja, V.; Rathi, M. Histopathological classification of pauci-immune glomerulonephritis and its impact on outcome. Rheumatol. Int. 2014, 34, 1721–1727. [Google Scholar] [CrossRef] [PubMed]
- Moroni, G.; Binda, V.; Leoni, A.; Raffiotta, F.; Quaglini, S.; Banfi, G.; Messa, P. Predictors of renal survival in ANCA-associated vasculitis. Validation of a histopatological classification schema and review of the literature. Clin. Exp. Rheumatol. 2015, 33, S56–S63. [Google Scholar]
- Andreiana, I.; Stancu, S.; Avram, A.; Taran, L.; Mircescu, G. ANCA positive crescentic glomerulonephritis outcome in a Central East European cohort: A retrospective study. BMC Nephrol. 2015, 16, 90. [Google Scholar] [CrossRef] [PubMed]
- Tanna, A.; Guarino, L.; Tam, F.W.; Rodriquez-Cubillo, B.; Levy, J.B.; Cairns, T.D.; Griffith, M.; Tarzi, R.M.; Caplin, B.; Salama, A.D.; et al. Long-term outcome of anti-neutrophil cytoplasm antibody-associated glomerulonephritis: Evaluation of the international histological classification and other prognostic factors. Nephrol. Dial. Transplant. 2015, 30, 1185–1192. [Google Scholar] [CrossRef]
- Cordova-Sanchez, B.M.; Mejia-Vilet, J.M.; Morales-Buenrostro, L.E.; Loyola-Rodriguez, G.; Uribe-Uribe, N.O.; Correa-Rotter, R. Clinical presentation and outcome prediction of clinical, serological, and histopathological classification schemes in ANCA-associated vasculitis with renal involvement. Clin. Rheumatol. 2016, 35, 1805–1816. [Google Scholar] [CrossRef]
- Van Daalen, E.; Ferrario, F.; Noel, L.H.; Waldherr, R.; Hagen, E.C.; Bruijn, J.A.; Bajema, I.M. Twenty-five years of RENHIS: A history of histopathological studies within EUVAS. Nephrol. Dial. Transplant. 2015, 30, i31–i36. [Google Scholar] [CrossRef]
- Bjorneklett, R.; Sriskandarajah, S.; Bostad, L. Prognostic Value of Histologic Classification of ANCA-Associated Glomerulonephritis. Clin. J. Am. Soc. Nephrol. 2016, 11, 2159–2167. [Google Scholar] [CrossRef][Green Version]
- Chen, Y.X.; Xu, J.; Pan, X.X.; Shen, P.Y.; Li, X.; Ren, H.; Chen, X.N.; Ni, L.Y.; Zhang, W.; Chen, N. Histopathological Classification and Renal Outcome in Patients with Antineutrophil Cytoplasmic Antibodies-associated Renal Vasculitis: A Study of 186 Patients and Metaanalysis. J. Rheumatol. 2017, 44, 304–313. [Google Scholar] [CrossRef]
- Brix, S.R.; Noriega, M.; Tennstedt, P.; Vettorazzi, E.; Busch, M.; Nitschke, M.; Jabs, W.J.; Ozcan, F.; Wendt, R.; Hausberg, M.; et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018, 94, 1177–1188. [Google Scholar] [CrossRef]
- Neumann, I.; Kain, R.; Regele, H.; Soleiman, A.; Kandutsch, S.; Meisl, F.T. Histological and clinical predictors of early and late renal outcome in ANCA-associated vasculitis. Nephrol. Dial. Transplant. 2005, 20, 96–104. [Google Scholar] [CrossRef]
- Franssen, C.F.; Stegeman, C.A.; Oost-Kort, W.W.; Kallenberg, C.G.; Limburg, P.C.; Tiebosch, A.; De Jong, P.E.; Tervaert, J.W. Determinants of renal outcome in anti-myeloperoxidase-associated necrotizing crescentic glomerulonephritis. J. Am. Soc. Nephrol. 1998, 9, 1915–1923. [Google Scholar]
- Hakroush, S.; Tampe, D.; Korsten, P.; Stroebel, P.; Zeisberg, M.; Tampe, B. Histopathological findings predict renal recovery in severe ANCA-associated vasculitis requiring intensive care treatment. Front. Med. 2020, 7, 622028. [Google Scholar] [CrossRef] [PubMed]
- Van Daalen, E.E.; Neeskens, P.; Zandbergen, M.; Harper, L.; Karras, A.; Vaglio, A.; de Zoysa, J.; Bruijn, J.A.; Bajema, I.M. Podocytes and Proteinuria in ANCA-Associated Glomerulonephritis: A Case-Control Study. Front. Immunol. 2019, 10, 1405. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef]
- Waikar, S.S.; Sabbisetti, V.S.; Bonventre, J.V. Normalization of urinary biomarkers to creatinine during changes in glomerular filtration rate. Kidney Int. 2010, 78, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Abuelo, J.G. Proteinuria: Diagnostic principles and procedures. Ann. Intern. Med. 1983, 98, 186–191. [Google Scholar] [CrossRef]
- Vyssoulis, G.P.; Tousoulis, D.; Antoniades, C.; Dimitrakopoulos, S.; Zervoudaki, A.; Stefanadis, C. Alpha-1 microglobulin as a new inflammatory marker in newly diagnosed hypertensive patients. Am. J. Hypertens. 2007, 20, 1016–1021. [Google Scholar] [CrossRef][Green Version]
- Mogensen, C.E. Progression of nephropathy in long-term diabetics with proteinuria and effect of initial anti-hypertensive treatment. Scand. J. Clin. Lab. Investig. 1976, 36, 383–388. [Google Scholar] [CrossRef]
- Row, P.G.; Cameron, J.S.; Turner, D.R.; Evans, D.J.; White, R.H.; Ogg, C.S.; Chantler, C.; Brown, C.B. Membranous nephropathy long-term follow-up and association with neoplasia. QJM Int. J. Med. 1975, 44, 207–239. [Google Scholar]
- Cameron, J.S. Proteinuria and progression in human glomerular diseases. Am. J. Nephrol. 1990, 10, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Gall, M.A.; Nielsen, F.S.; Smidt, U.M.; Parving, H.H. The course of kidney function in type 2 (non-insulin-dependent) diabetic patients with diabetic nephropathy. Diabetologia 1993, 36, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.J.; Hunsicker, L.G.; Bain, R.P.; Rohde, R.D. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N. Engl. J. Med. 1993, 329, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Myers, B.D.; Nelson, R.G.; Tan, M.; Beck, G.J.; Bennett, P.H.; Knowler, W.C.; Blouch, K.; Mitch, W.E. Progression of overt nephropathy in non-insulin-dependent diabetes. Kidney Int. 1995, 47, 1781–1789. [Google Scholar] [CrossRef][Green Version]
- Christensen, P.K.; Rossing, P.; Nielsen, F.S.; Parving, H.H. Natural course of kidney function in Type 2 diabetic patients with diabetic nephropathy. Diabet. Med. 1999, 16, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Philibert, D.; Cattran, D. Remission of proteinuria in primary glomerulonephritis: We know the goal but do we know the price? Nat. Clin. Pract. Nephrol. 2008, 4, 550–559. [Google Scholar] [CrossRef]
- Shihabi, Z.K.; Konen, J.C.; O’Connor, M.L. Albuminuria vs urinary total protein for detecting chronic renal disorders. Clin. Chem. 1991, 37, 621–624. [Google Scholar] [CrossRef]
- Hruskova, Z.; Honsova, E.; Berden, A.E.; Rychlik, I.; Lanska, V.; Zabka, J.; Bajema, I.M.; Tesar, V. Repeat protocol renal biopsy in ANCA-associated renal vasculitis. Nephrol. Dial. Transplant. 2014, 29, 1728–1732. [Google Scholar] [CrossRef]
- Xu, P.C.; Chen, T.; Gao, S.; Hu, S.Y.; Wei, L.; Yan, T.K. Clinical and pathologic characteristics of pauci-immune anti-myeloperoxidase antibody associated glomerulonephritis with nephrotic range proteinuria. Ren. Fail. 2018, 40, 554–560. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Clinical data | |
| Female sex—no. (%) | 23 (43.4) |
| Age (IQR)—years | 65 (54.5–74.5) |
| Disease onset—days before admission (IQR) | 18 (7–46) |
| Kidney biopsy—days after admission (IQR) | 6 (3–9.5) |
| MPO/PR3 subtype—no. (%) | 26/27 (49.1/50.9) |
| MPA/GPA subtype—no. (%) | 26/27 (49.1/50.9) |
| New diagnosis—no. (%) | 45 (84.9) |
| Systemic disease activity | |
| BVAS (IQR)—points | 18 (15–20.5) |
| Extrarenal manifestation—no. (%) | 44 (83) |
| Lung involvement—no. (%) | 31 (58.5) |
| Alveolar hemorrhage—no. (%) | 7 (13.2) |
| Sinus involvement—no. (%) | 9 (17) |
| Joint involvement—no. (%) | 12 (22.6) |
| Ear involvement—no. (%) | 4 (7.5) |
| Eye involvement—no. (%) | 3 (5.7) |
| Peripheral nerve involvement—no. (%) | 6 (11.3) |
| Skin involvement—no. (%) | 8 (15.1) |
| CRP (IQR)—mg/L | 57.4 (19.1–107) |
| Renal injury | |
| Serum creatinine (IQR)—μmol/L | 269 (116–437) |
| eGFR (IQR)—mL/min/1.73 m2 | 19 (9.7–50.2) |
| Dialysis within 30 days after admission—no. (%) | 16 (30.2) |
| Proteinuric findings | |
| Leukocyturia (IQR)—per HPF | 2 (1–4) |
| Hematuria (IQR)—per HPF | 4 (3–4) |
| Acanthocytes—no. (%) | 8 (15.1) |
| uPCR (IQR)—mg/g | 904 (505–1653) |
| uACR (IQR)—mg/g | 445 (164–855) |
| IgG/creatinine (IQR)—mg/g | 44.1 (20.5–191) |
| α1-microglobulin/creatinine (IQR)—mg/g | 69.6 (34.8–172) |
| α2-macroglobulin/creatinine (IQR)—mg/g | 5.05 (2.92–11.1) |
| Histopathological findings | |
| Total glomeruli (IQR)—no. | 17 (11–28) |
| Normal glomeruli (IQR)—% | 48.9 (26.2–73) |
| Glomerular necrosis (IQR)—% | 15.2 (0–44.7) |
| Glomerular crescents (IQR)—% | 30.8 (9.76–55.1) |
| Glomerular sclerosis (IQR)—% | 5.13 (0–26.2) |
| IF/TA (IQR)—% | 20 (10–40) |
| Berden Classification | Paratemeter | p Value |
|---|---|---|
| uPCR | ||
| Crescentic class—mg/g | 1348 (755–1939) | |
| Focal class—mg/g | 573 (359–1213) | |
| Mixed class—mg/g | 1540 (729–2536) | |
| Sclerotic class—mg/g | 5318 (5285–8129) | 0.0006 |
| uACR | ||
| Crescentic class—mg/g | 678 (338–1047) | |
| Focal class—mg/g | 202 (86.1–504) | |
| Mixed class—mg/g | 1021 (458–1701) | |
| Sclerotic class—mg/g | 3604 (3043–4429) | 0.0002 |
| Urinary IgG | ||
| Crescentic class—mg/g | 89.1 (43.2–232) | |
| Focal class—mg/g | 25 (11.2–96.4) | |
| Mixed class—mg/g | 56.5 (20.1–149) | |
| Sclerotic class—mg/g | 352 (271–542) | 0.0018 |
| Urinary α1-microglobulin | ||
| Crescentic class—mg/g | 101 (52.9–197) | |
| Focal class—mg/g | 41.4 (17.6–113) | |
| Mixed class—mg/g | 67.2 (7.24–150) | |
| Sclerotic class—mg/g | 191 (62.2–310) | 0.1092 |
| Urinary α2-macroglobulin | ||
| Crescentic class—mg/g | 5.44 (3.55–9.03) | |
| Focal class—mg/g | 3.13 (1.99–6.27) | |
| Mixed class—mg/g | 10 (4.91–14.1) | |
| Sclerotic class—mg/g | 32.8 (16.8–60.8) | 0.0026 |
| ARRS | Parameter | p Value |
|---|---|---|
| uPCR | ||
| High risk—mg/g | 5264 (1959–7426) | |
| Medium risk—mg/g | 977 (627–1743) | |
| Low risk—mg/g | 573 (359–1201) | <0.0001 |
| uACR | ||
| High risk—mg/g | 2946 (996–4223) | |
| Medium risk—mg/g | 470/314–839) | |
| Low risk—mg/g | 227 (86.1–504) | 0.0003 |
| Urinary IgG | ||
| High risk—mg/g | 261 (246–495) | |
| Medium risk—mg/g | 57.9 (30.8–159) | |
| Low risk—mg/g | 24.4 (13.3–37.3) | <0.0001 |
| Urinary α1-microglobulin | ||
| High risk—mg/g | 174 (116–280) | |
| Medium risk—mg/g | 92.3 (47.1–204) | |
| Low risk—mg/g | 37.1 (6.24–82.9) | 0.0009 |
| Urinary α2-macroglobulin | ||
| High risk—mg/g | 15.7 (8.29–28.2) | |
| Medium risk—mg/g | 5.06 (3.06–11.1) | |
| Low risk—mg/g | 3.33 (2.09–6.27) | 0.001 |
| Variable | β | SE | p Value |
|---|---|---|---|
| uPCR | |||
| Normal glomeruli—% | −47.963 | 14.352 | 0.0016 |
| Glomerular crescents—% | −18.551 | 12.725 | 0.1513 |
| IF/TA—% | 11.895 | 14.609 | 0.4195 |
| uACR | |||
| Normal glomeruli—% | −33.080 | 9.736 | 0.0014 |
| Glomerular crescents—% | −10.111 | 8.633 | 0.2472 |
| IF/TA—% | 0.456 | 0.911 | 0.9635 |
| Urinary IgG | |||
| Normal glomeruli—% | −2.237 | 1.269 | 0.0845 |
| Glomerular necrosis—% | −1.662 | 1.117 | 0.1435 |
| Glomerular crescents—% | 0.865 | 1.512 | 0.5697 |
| IF/TA—% | 2.032 | 1.117 | 0.1129 |
| Urinary α1-microglobulin | |||
| Normal glomeruli—% | −0.255 | 1.207 | 0.8336 |
| Glomerular crescents—% | 0.757 | 1.217 | 0.5367 |
| Urinary α2-macroglobulin | |||
| Normal glomeruli—% | −0.333 | 0.073 | <0.0001 |
| Glomerular crescents—% | −0.211 | 0.065 | 0.002 |
| IF/TA—% | −0.083 | 0.075 | 0.2726 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tampe, D.; Korsten, P.; Ströbel, P.; Hakroush, S.; Tampe, B. Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity. J. Clin. Med. 2021, 10, 1538. https://doi.org/10.3390/jcm10071538
Tampe D, Korsten P, Ströbel P, Hakroush S, Tampe B. Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity. Journal of Clinical Medicine. 2021; 10(7):1538. https://doi.org/10.3390/jcm10071538
Chicago/Turabian StyleTampe, Désirée, Peter Korsten, Philipp Ströbel, Samy Hakroush, and Björn Tampe. 2021. "Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity" Journal of Clinical Medicine 10, no. 7: 1538. https://doi.org/10.3390/jcm10071538
APA StyleTampe, D., Korsten, P., Ströbel, P., Hakroush, S., & Tampe, B. (2021). Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity. Journal of Clinical Medicine, 10(7), 1538. https://doi.org/10.3390/jcm10071538