
Trends in Hospital Admissions for Chronic Obstructive Pulmonary Disease in Men and Women in Spain, 1998 to 2018


 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2020 Report) [Internet]. Available online: https://goldcopd.org/gold-reports/ (accessed on 26 October 2020).
- Donaldson, G.C.; Law, M.; Kowlessar, B.; Singh, R.; Brill, S.E.; Allinson, J.P.; Wedzicha, J.A. Impact of Prolonged Exacerbation Recovery in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2015, 192, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Seemungal, T.A.; Donaldson, G.C.; Paul, E.A.; Bestall, J.C.; Jeffries, D.J.; Wedzicha, J.A. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157 Pt 1, 1418–1422. [Google Scholar] [CrossRef]
- Müllerova, H.; Maselli, D.J.; Locantore, N.; Vestbo, J.; Hurst, J.R.; Wedzicha, J.A.; Bakke, P.; Agusti, A.; Anzueto, A. Hospitalized exacerbations of COPD: Risk factors and outcomes in the ECLIPSE cohort. Chest 2015, 147, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Soler-Cataluña, J.J.; Martínez-García, M.A.; Román Sánchez, P.; Salcedo, E.; Navarro, M.; Ochando, R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005, 60, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Toy, E.L.; Gallagher, K.F.; Stanley, E.L.; Swensen, A.R.; Duh, M.S. The economic impact of exacerbations of chronic obstructive pulmonary disease and exacerbation definition: A review. COPD 2010, 7, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Carney, L.; Soljak, M.; Bottle, A.; Partridge, M.; Bell, D.; Abi-Aad, G.; Aylin, P.; Majeed, A. Association of population and primary healthcare factors with hospital admission rates for chronic obstructive pulmonary disease in England: National cross-sectional study. Thorax 2011, 66, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Bottle, A.; Honeyford, K.; Chowdhury, F.; Bell, D.; Aylin, P. Factors Associated with Hospital Emergency Readmission and Mortality Rates in Patients with Heart Failure or Chronic Obstructive Pulmonary Disease; A National Observational Study; NIHR Journals Library: Southampton, UK, 2018. [Google Scholar]
- Hunter, L.C.; Lee, R.J.; Butcher, I.; Weir, C.J.; Fischbacher, C.M.; McAllister, D.; Wild, S.H.; Hewitt, N.; Hardie, R.M. Patient characteristics associated with risk of first hospital admission and readmission for acute exacerbation of chronic obstructive pulmonary disease (COPD) following primary care COPD diagnosis: A cohort study using linked electronic patient records. BMJ Open 2016, 6, e009121. [Google Scholar] [CrossRef]
- Wong, A.W.; Gan, W.Q.; Burns, J.; Sin, D.D.; van Eeden, S.F. Acute exacerbation of chronic obstructive pulmonary disease: Influence of social factors in determining length of hospital stay and readmission rates. Can. Respir. J. 2008, 15, 361–364. [Google Scholar] [CrossRef]
- Abadias Medrano, M.J.; Yuguero Torres, O.; Bardés Robles, I.; Casas-Méndez, L.F.; Barbé, F.; de Batlle, J. Exacerbations of chronic obstructive pulmonary disease: An analysis of the care process in a regional hospital emergency department. Medicine 2018, 97, e11601. [Google Scholar] [CrossRef]
- Andreas, S.; Röver, C.; Heinz, J.; Straube, S.; Watz, H.; Friede, T. Decline of COPD exacerbations in clinical trials over two decades—A systematic review and meta-regression. Respir. Res. 2019, 20, 186. [Google Scholar] [CrossRef]
- Han, M.K.; Arteaga-Solis, E.; Blenis, J.; Bourjeily, G.; Clegg, D.J.; DeMeo, D.; Duffy, J.; Gaston, B.; Heller, N.M.; Hemnes, A.; et al. Female Sex and Gender in Lung/Sleep Health and Disease. Increased Understanding of Basic Biological, Pathophysiological, and Behavioral Mechanisms Leading to Better Health for Female Patients with Lung Disease. Am. J. Respir. Crit. Care Med. 2018, 198, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, C.R.; Chapman, K.R.; Donohue, J.F.; Roche, N.; Tsiligianni, I.; Han, M.K. Improving the management of COPD in women. Chest 2017, 151, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Birring, S.S.; Brightling, C.E.; Bradding, P.; Entwisle, J.J.; Vara, D.D.; Grigg, J.; Wardlaw, A.J.; Pavord, I.D. Clinical, radiologic, and induced sputum features of chronic obstructive pulmonary disease in nonsmokers: A descriptive study. Am. J. Respir. Crit. Care Med. 2002, 166, 1078–1083. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Portal Estadístico. Conjunto Mínimo Básico de Datos de Hospitalización (CMBD-H). Available online: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/Comun/ArbolNodos.aspx?idNodo=6383 (accessed on 26 October 2020).
- National Cancer Institute. Joinpoint Regresion Program, Version 4.6.0; Nacional Cancer Institute: Bethesda, ML, USA, 2013. Available online: http://surveillance.cancer.gov/joinpoint/ (accessed on 26 October 2020).
- De Miguel-Díez, J.; Jiménez-García, R.; Hernández-Barrera, V.; Puente-Maestu, L.; Rodríguez-Rodríguez, P.; López de Andrés, A.; Carrasco-Garrido, P. Trends in hospital admissions for acute exacerbation of COPD in Spain from 2006 to 2010. Respir. Med. 2013, 107, 717–723. [Google Scholar] [CrossRef][Green Version]
- Librero, J.; Ibañez-Beroiz, B.; Peiró, S.; Ridao-López, M.; Rodríguez-Bernal, C.L.; Gómez-Romero, F.J.; Bernal-Delgado, E. Spanish Atlas of Medical Practice Variation Research Group. Trends and area variations in Potentially Preventable Admissions for COPD in Spain (2002–2013): A significant decline and convergence between areas. BMC Health Serv. Res. 2016, 16, 367. [Google Scholar] [CrossRef]
- Soriano, J.B.; Alfageme, I.; Miravitlles, M.; De Lucas, P.; Soler-Cataluña, J.J.; García-Rio, F.; Casanova, C.; Rodriguez Gonzalez-Moro, J.M.; Cosio, B.G.; Sanchez, G.; et al. A New study of the Prevalence of COPD in Spain: EPISCAN II. Eur. Respir. J. 2019, 54 (Suppl. 63). [Google Scholar] [CrossRef]
- Di Marco, F.; Verga, M.; Reggente, M.; Maria Casanova, F.; Santus, P.; Blasi, F.; Allegra, L.; Centanni, S. Anxiety and depression in COPD patients: The roles of gender and disease severity. Respir. Med. 2006, 100, 1767–1774. [Google Scholar] [CrossRef]
- Underner, M.; Cuvelier, A.; Peiffer, G.; Perriot, J.; Jaafari, N. Influence de l’anxiété et de la dépression sur les exacerbations au cours de la BPCO [The influence of anxiety and depression on COPD exacerbations]. Rev. Mal. Respir. 2018, 35, 604–625. (In French) [Google Scholar] [CrossRef]
- Chapman, K.R.; Tashkin, D.P.; Pye, D.J. Gender bias in the diagnosis of COPD. Chest 2001, 119, 1691–1695. [Google Scholar] [CrossRef]
- Martinez, C.H.; Raparla, S.; Plauschinat, C.A.; Giardino, N.D.; Rogers, B.; Beresford, J.; Bentkover, J.D.; Schachtner-Appel, A.; Curtis, J.L.; Martinez, F.J.; et al. Gender differences in symptoms and care delivery for chronic obstructive pulmonary disease. J. Womens Health 2012, 21, 1267–1274. [Google Scholar] [CrossRef]
- Zhu, M.; Wang, T.; Wang, C.; Ji, Y. The association between vitamin D and COPD risk, severity, and exacerbation: An updated systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2597–2607. [Google Scholar] [CrossRef] [PubMed]
- Navarro Valverde, C.; Quesada Gómez, J.M. Deficiencia de vitamina D en España: ¿Realidad o mito? Rev. de Osteoporos. y Metab. Miner. 2014, 6, 5–10. [Google Scholar] [CrossRef][Green Version]
- Chen, S.L.; Lee, W.L.; Liang, T.; Liao, I.C. Factors associated with gender differences in medication adherence: A longitudinal study. J. Adv. Nurs. 2014, 70, 2031–2040. [Google Scholar] [CrossRef] [PubMed]
- Thunander Sundbom, L.; Bingefors, K. Women and men report different behaviours in, and reasons for medication non-adherence: A nationwide Swedish survey. Pharm. Pract. 2012, 10, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Aryal, S.; Diaz-Guzman, E.; Mannino, D.M. Influence of sex on chronic obstructive pulmonary disease risk and treatment outcomes. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 1145–1154. [Google Scholar] [PubMed]
- Watson, L.; Vestbo, J.; Postma, D.S.; Decramer, M.; Rennard, S.; Kiri, V.A.; Vermeire, P.A.; Soriano, J.B. Gender differences in the management and experience of Chronic Obstructive Pulmonary Disease. Respir. Med. 2004, 98, 1207–1213. [Google Scholar] [CrossRef]
- Ancochea, J.; Miravitlles, M.; García-Río, F.; Muñoz, L.; Sánchez, G.; Sobradillo, V.; Duran-Tauleria, E.; Soriano, J.B. Underdiagnosis of chronic obstructive pulmonary disease in women: Quantification of the problem, determinants and proposed actions. Arch. Bronconeumol. 2013, 49, 223–229. [Google Scholar] [CrossRef]
- Ford, E.S. Hospital discharges, readmissions, and ED visits for COPD or bronchiectasis among US adults: Findings from the nationwide inpatient sample 2001–2012 and Nationwide Emergency Department Sample 2006–2011. Chest 2015, 147, 989–998. [Google Scholar] [CrossRef]
- American Lung Association. Taking Her Breath Away; The Rise of COPD in Women: New York, NY, USA, 2013; Available online: http://ala2.pub30.convio.net/our-initiatives/research/lung-health-disparities/the-rise-of-copd-in-women.html (accessed on 26 October 2020).
- Morton, K.; MacNeill, S.; Sanderson, E.; Dixon, P.; King, A.; Jenkins, S.; Metcalfe, C.; Shaw, A.; Chalder, M.; Benger, J.; et al. Evaluation of ‘care bundles’ for patients with chronic obstructive pulmonary disease (COPD): A multisite study in the UK. BMJ Open Respir. Res. 2019, 6, e000425. [Google Scholar] [CrossRef]
- Ospina, M.B.; Mrklas, K.; Deuchar, L.; Rowe, B.H.; Leigh, R.; Bhutani, M.; Stickland, M.K. A systematic review of the effectiveness of discharge care bundles for patients with COPD. Thorax 2017, 72, 31–39. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Características e Indicadores de Salud 2019. Comisión Europea, Organización para la Cooperación y Desarrollo Económico-OCDE y Observatorio Europeo de Salud de la OMS. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/docs/presentacion_es.pdf (accessed on 26 October 2020).
- Miravitlles, M.; Soler-Cataluña, J.J.; Calle, M.; Molina, J.; Almagro, P.; Quintano, J.A.; Trigueros, J.A.; Cosío, B.G.; Casanova, C.; Antonio Riesco, J.; et al. Spanish Guidelines for Management of Chronic Obstructive Pulmonary Disease (GesEPOC) 2017. Pharmacological Treatment of Stable Phase. Arch. Bronconeumol. 2017, 53, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Gut-Gobert, C.; Cavaillès, A.; Dixmier, A.; Guillot, S.; Jouneau, S.; Leroyer, C.; Marchand-Adam, S.; Marquette, D.; Meurice, J.C.; Desvigne, N.; et al. Women and COPD: Do we need more evidence? Eur. Respir. Rev. 2019, 28, 180055. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Segment 1 | Segment 2 | Segment 3 | Segment 4 | Overall (1998–2018) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | Period | APC | 95% CI | Period | APC | 95% CI | Period | APC | 95% CI | Period | APC | 95% CI | AAPC | 95% CI |
| Women | ||||||||||||||
| Total | 1998–2010 | −6.0 * | (−7.1, −4.9) | 2010–2018 | 7.8 * | (5.5, 10.2) | −0.7 | (−1.7, 0.3) | ||||||
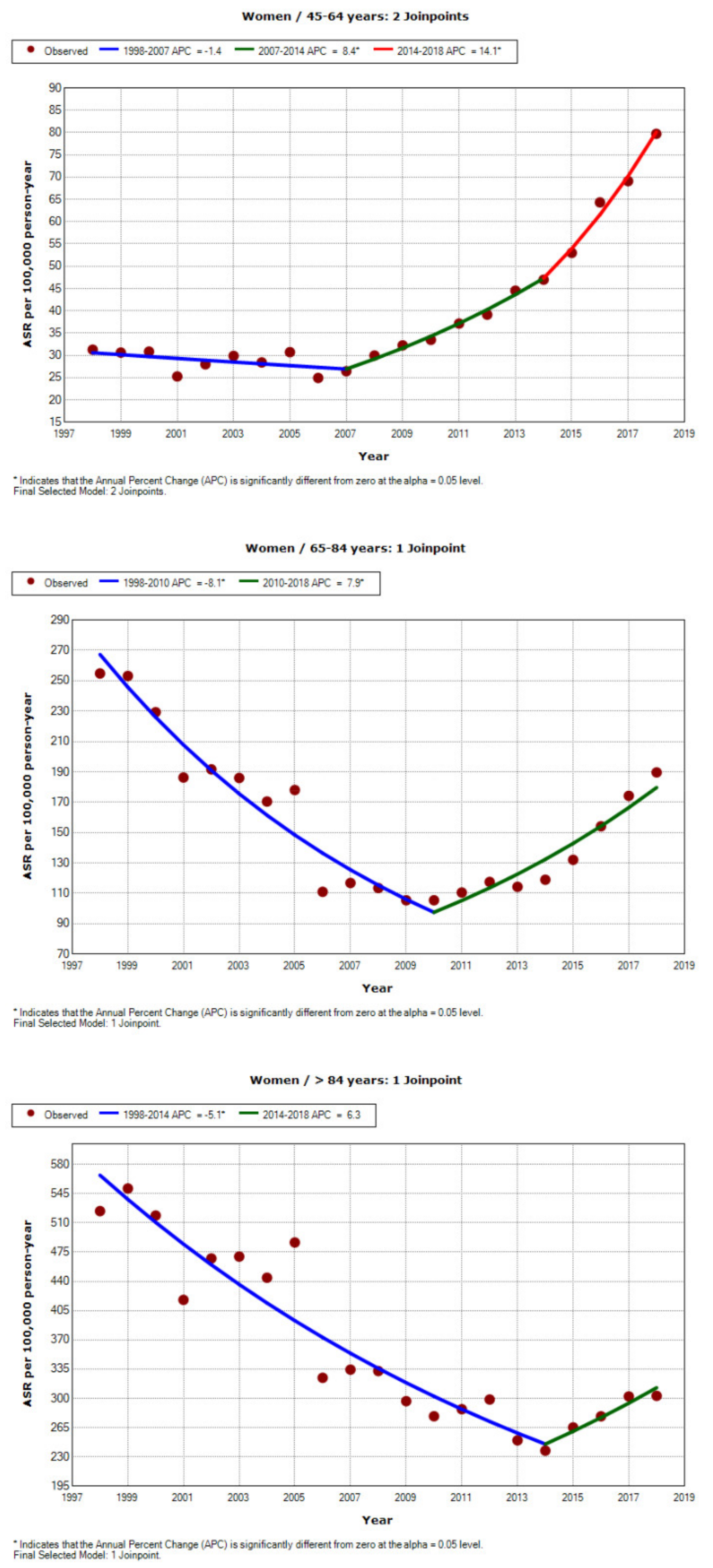
| 45–64 years | 1998–2007 | −1.4 | (−2.9, 0.1) | 2007–2014 | 8.4 * | (5.9, 10.9) | 2014–2018 | 14.1 * | (10.4, 17.9) | 4.9 * | (3.8, 6.1) | |||
| 65–84 years | 1998–2010 | −8.1 * | (−9.2, −6.9) | 2010–2018 | 7.9 * | (5.3, 10.7) | −2.0 * | (−3.1, −0.8) | ||||||
| ≥85 years | 1998–2014 | −5.1 * | (−6.0, −4.2) | 2014–2018 | 6.3 | (−1.7, 14.9) | −2.9 * | (−4.5, −1.4) | ||||||
| Men | ||||||||||||||
| Total | 1998–2004 | −0.3 | (−3.1, 2.6) | 2004–2010 | −6.5 * | (−10.0, −2.8) | 2010–2018 | 1.1 | (−0.8, 2.9) | −1.7 * | (−3.1, −0.2) | |||
| 45–64 years | 1998–2004 | −2.7 * | (−4.3, −1.2) | 2004–2007 | −12.0 | (−25.4, 3.8) | 2007–2014 | −3.2 * | (−5.0, −1.3) | 2014–2018 | 5.6 * | (1.7, 9.7) | −2.7 * | (−5.0, −0.4) |
| 65–84 years | 1998–2004 | −0.4 | (−3.1, 2.4) | 2004–2010 | −7.0 * | (−10.4, −3.5) | 2010–2018 | 0.8 | (−1.1, 2.6) | −2.0 * | (−3.4, −0.6) | |||
| ≥85 years | 1998–2004 | 3.3 * | (0.3, 6.4) | 2004–2014 | −1.6 * | (−2.8, −0.4) | 2014–2018 | 5.5 * | (1.3, 9.9) | 1.3 * | (0.0, 2.5) | |||
| Year | Total | 45–64 Years | 65–84 Years | ≥85 Years | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | ASR | 95% CI | n | ASR | 95% CI | n | ASR | 95% CI | n | ASR | 95% CI | |
| 1998 | 12,477 | 83.6 | (82.1, 85.0) | 1420 | 31.3 | (29.6, 32.9) | 8477 | 254.8 | (249.3, 260.2) | 2383 | 524.1 | (503.0, 545.1) |
| 1999 | 12,942 | 83.7 | (82.3, 85.2) | 1398 | 30.6 | (29.0, 32.2) | 8720 | 253.1 | (247.8, 258.4) | 2642 | 551.2 | (530.2, 572.2) |
| 2000 | 12,241 | 77.7 | (76.4, 79.1) | 1390 | 30.8 | (29.2, 32.5) | 8033 | 229.2 | (224.2, 234.3) | 2612 | 518.8 | (498.9, 538.7) |
| 2001 | 10,299 | 63.4 | (62.2, 64.6) | 1155 | 25.3 | (23.8, 26.7) | 6714 | 186.3 | (181.8, 190.7) | 2210 | 417.9 | (400.4, 435.3) |
| 2002 | 11,103 | 67.1 | (65.9, 68.4) | 1282 | 28.0 | (26.5, 29.5) | 7080 | 191.6 | (187.2, 196.1) | 2496 | 467.4 | (449.1, 485.7) |
| 2003 | 11,240 | 66.5 | (65.3, 67.8) | 1403 | 29.9 | (28.3, 31.5) | 7051 | 186.0 | (181.6, 190.3) | 2555 | 469.7 | (451.5, 487.9) |
| 2004 | 10,655 | 61.8 | (60.6, 63.0) | 1381 | 28.4 | (26.9, 29.9) | 6580 | 170.4 | (166.3, 174.6) | 2469 | 444.3 | (426.8, 461.9) |
| 2005 | 11,584 | 65.7 | (64.5, 66.9) | 1565 | 30.7 | (29.2, 32.2) | 6982 | 178.1 | (173.8, 182.3) | 2781 | 486.6 | (468.5, 504.6) |
| 2006 | 7852 | 43.8 | (42.8, 44.8) | 1291 | 24.9 | (23.6, 26.3) | 4421 | 111.0 | (107.7, 114.3) | 1933 | 324.6 | (310.2, 339.1) |
| 2007 | 8415 | 46.1 | (45.1, 47.1) | 1414 | 26.4 | (25.1, 27.8) | 4699 | 116.9 | (113.5, 120.3) | 2056 | 334.4 | (319.9, 348.8) |
| 2008 | 8584 | 46.2 | (45.3, 47.2) | 1648 | 30.0 | (28.5, 31.4) | 4576 | 113.5 | (110.1, 116.8) | 2158 | 332.7 | (318.6, 346.7) |
| 2009 | 8348 | 44.2 | (43.2, 45.1) | 1815 | 32.3 | (30.8, 33.7) | 4302 | 105.5 | (102.3, 108.7) | 2019 | 296.6 | (283.7, 309.5) |
| 2010 | 8434 | 43.9 | (42.9, 44.8) | 1919 | 33.5 | (32.0, 35.0) | 4338 | 105.5 | (102.3, 108.7) | 1993 | 278.5 | (266.3, 290.8) |
| 2011 | 9069 | 46.4 | (45.4, 47.4) | 2166 | 37.1 | (35.6, 38.7) | 4584 | 110.6 | (107.3, 113.8) | 2152 | 286.9 | (274.8, 299.1) |
| 2012 | 9715 | 49.0 | (48.0, 50.0) | 2309 | 39.1 | (37.5, 40.7) | 4890 | 117.5 | (114.1, 120.9) | 2345 | 298.6 | (286.5, 310.6) |
| 2013 | 9663 | 48.6 | (47.6, 49.6) | 2670 | 44.5 | (42.8, 46.2) | 4778 | 114.3 | (111.0, 117.6) | 2025 | 249.7 | (238.8, 260.6) |
| 2014 | 9934 | 49.9 | (48.9, 50.9) | 2827 | 47.0 | (45.2, 48.7) | 4946 | 119.0 | (115.6, 122.3) | 2005 | 237.4 | (227.0, 247.8) |
| 2015 | 11,219 | 55.7 | (54.6, 56.7) | 3240 | 53.0 | (51.2, 54.8) | 5501 | 132.1 | (128.5, 135.7) | 2331 | 265.2 | (254.4, 275.9) |
| 2016 | 13,130 | 65.0 | (63.9, 66.2) | 4007 | 64.3 | (62.3, 66.3) | 6370 | 154.1 | (150.3, 158.0) | 2533 | 278.4 | (267.6, 289.3) |
| 2017 | 14,649 | 71.5 | (70.4, 72.7) | 4388 | 69.1 | (67.1, 71.2) | 7243 | 174.2 | (170.2, 178.3) | 2842 | 302.3 | (291.2, 313.4) |
| 2018 | 16,190 | 78.6 | (77.4, 79.9) | 5165 | 79.7 | (77.5, 81.9) | 7868 | 189.6 | (185.4, 193.9) | 2947 | 303.0 | (292.0, 313.9) |
| Year | Total | 45–64 Years | 65–84 Years | >84 Years | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | ASR | 95% CI | n | ASR | 95% CI | n | ASR | 95% CI | n | ASR | 95% CI | |
| 1998 | 54,237 | 505.9 | (501.6, 510.3) | 10,441 | 244.8 | (240.1, 249.5) | 39,043 | 1635.0 | (1618.6, 1651.4) | 4186 | 2065.9 | (2003.3, 2128.5) |
| 1999 | 58,865 | 530.4 | (526.0, 534.8) | 11,382 | 266.5 | (261.6, 271.5) | 42,322 | 1702.8 | (1686.4, 1719.2) | 4541 | 2133.8 | (2071.7, 2195.8) |
| 2000 | 57,118 | 507.9 | (503.6, 512.1) | 10,510 | 249.2 | (244.4, 254.0) | 41,321 | 1629.7 | (1613.9, 1645.6) | 4674 | 2114.9 | (2054.3, 2175.6) |
| 2001 | 53,765 | 464.6 | (460.6, 468.7) | 9453 | 220.0 | (215.6, 224.5) | 39,122 | 1497.2 | (1482.2, 1512.1) | 4532 | 1962.9 | (1905.7, 2020.0) |
| 2002 | 59,332 | 503.6 | (499.5, 507.8) | 9766 | 226.6 | (222.1, 231.1) | 43,746 | 1628.0 | (1612.7, 1643.4) | 5180 | 2236.2 | (2175.3, 2297.1) |
| 2003 | 62,286 | 517.2 | (513.0, 521.3) | 10,245 | 231.9 | (227.4, 236.4) | 45,666 | 1655.7 | (1640.5, 1671.0) | 5655 | 2408.2 | (2345.4, 2471.0) |
| 2004 | 59,561 | 487.2 | (483.2, 491.2) | 9618 | 210.1 | (205.9, 214.3) | 43,694 | 1558.9 | (1544.3, 1573.5) | 5632 | 2373.2 | (2311.2, 2435.2) |
| 2005 | 66,537 | 533.7 | (529.5, 537.8) | 10,350 | 214.3 | (210.2, 218.4) | 48,840 | 1711.3 | (1696.1, 1726.5) | 6727 | 2754.8 | (2689.0, 2820.7) |
| 2006 | 47,331 | 371.9 | (368.5, 375.3) | 7159 | 146.1 | (142.7, 149.5) | 34,456 | 1178.0 | (1165.5, 1190.4) | 5252 | 2050.2 | (1994.7, 2105.6) |
| 2007 | 52,204 | 403.1 | (399.6, 406.6) | 7937 | 157.0 | (153.6, 160.5) | 37,537 | 1266.1 | (1253.2, 1278.9) | 6263 | 2314.7 | (2257.4, 2372.1) |
| 2008 | 50,579 | 382.4 | (379.0, 385.8) | 7580 | 145.1 | (141.8, 148.3) | 35,840 | 1189.3 | (1177.0, 1201.7) | 6703 | 2316.7 | (2261.2, 2372.1) |
| 2009 | 49,994 | 368.8 | (365.6, 372.1) | 7717 | 144.6 | (141.3, 147.8) | 34,982 | 1144.2 | (1132.2, 1156.2) | 6760 | 2193.4 | (2141.1, 2245.7) |
| 2010 | 47,808 | 346.5 | (343.4, 349.7) | 7026 | 129.3 | (126.2, 132.3) | 33,502 | 1083.5 | (1071.8, 1095.1) | 6819 | 2078.2 | (2028.9, 2127.5) |
| 2011 | 48,722 | 344.3 | (341.2, 347.4) | 7239 | 131.8 | (128.7, 134.8) | 33,694 | 1064.9 | (1053.5, 1076.3) | 7337 | 2110.0 | (2061.7, 2158.3) |
| 2012 | 50,298 | 349.7 | (346.6, 352.8) | 6996 | 125.3 | (122.3, 128.2) | 34,616 | 1080.1 | (1068.7, 1091.6) | 8311 | 2254.4 | (2206.0, 2302.9) |
| 2013 | 48,269 | 329.3 | (326.3, 332.2) | 6955 | 122.5 | (119.6, 125.4) | 33,007 | 1018.2 | (1007.2, 1029.3) | 7934 | 2063.2 | (2017.8, 2108.7) |
| 2014 | 48,723 | 329.6 | (326.6, 332.5) | 6862 | 120.5 | (117.6, 123.4) | 33,094 | 1018.9 | (1007.8, 1029.9) | 8415 | 2091.6 | (2046.9, 2136.2) |
| 2015 | 51,740 | 344.9 | (341.9, 347.9) | 7320 | 126.9 | (124.0, 129.9) | 34,917 | 1069.0 | (1057.7, 1080.3) | 9179 | 2166.5 | (2122.1, 2210.8) |
| 2016 | 53,740 | 351.3 | (348.3, 354.3) | 7859 | 132.9 | (130.0, 135.9) | 35,522 | 1075.0 | (1063.7, 1086.2) | 10,027 | 2262.1 | (2217.8, 2306.3) |
| 2017 | 56,347 | 362.8 | (359.8, 365.8) | 8123 | 134.4 | (131.4, 137.3) | 36,684 | 1103.4 | (1092.0, 1114.8) | 11,194 | 2413.0 | (2368.3, 2457.7) |
| 2018 | 60,944 | 384.8 | (381.7, 387.9) | 9551 | 154.6 | (151.5, 157.7) | 38,623 | 1151.9 | (1140.3, 1163.4) | 12,451 | 2563.7 | (2518.7, 2608.8) |
| 45–64 Years N (row %) | 65–84 Years N (row %) | >84 Years N (row %) | Total N | |
|---|---|---|---|---|
| Women 1998 | 1420 (11.6) | 8477 (69.0) | 2383 (19.4) | 12,280 |
| 2010 | 1919 (23.3) | 4338 (52.6) | 1993 (24.2) | 8250 |
| 2018 | 5165 (32.3) | 7868 (49.2) | 2947 (18.4) | 15,980 |
| Men 1998 | 10,441 (19.5) | 39,043 (72.7) | 4186 (7.8) | 53,670 |
| 2010 | 7026 (14.8) | 33,502 (70.8) | 6819 (14.4) | 47,347 |
| 2018 | 9551 (15.8) | 38,623 (63.7) | 12,451 (20.5) | 60,625 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orozco-Beltrán, D.; Arriero-Marin, J.M.; Carratalá-Munuera, C.; Soler-Cataluña, J.J.; Lopez-Pineda, A.; Gil-Guillén, V.F.; Quesada, J.A. Trends in Hospital Admissions for Chronic Obstructive Pulmonary Disease in Men and Women in Spain, 1998 to 2018. J. Clin. Med. 2021, 10, 1529. https://doi.org/10.3390/jcm10071529
Orozco-Beltrán D, Arriero-Marin JM, Carratalá-Munuera C, Soler-Cataluña JJ, Lopez-Pineda A, Gil-Guillén VF, Quesada JA. Trends in Hospital Admissions for Chronic Obstructive Pulmonary Disease in Men and Women in Spain, 1998 to 2018. Journal of Clinical Medicine. 2021; 10(7):1529. https://doi.org/10.3390/jcm10071529
Chicago/Turabian StyleOrozco-Beltrán, Domingo, Juan Manuel Arriero-Marin, Concepción Carratalá-Munuera, Juan J. Soler-Cataluña, Adriana Lopez-Pineda, Vicente F. Gil-Guillén, and Jose A. Quesada. 2021. "Trends in Hospital Admissions for Chronic Obstructive Pulmonary Disease in Men and Women in Spain, 1998 to 2018" Journal of Clinical Medicine 10, no. 7: 1529. https://doi.org/10.3390/jcm10071529
APA StyleOrozco-Beltrán, D., Arriero-Marin, J. M., Carratalá-Munuera, C., Soler-Cataluña, J. J., Lopez-Pineda, A., Gil-Guillén, V. F., & Quesada, J. A. (2021). Trends in Hospital Admissions for Chronic Obstructive Pulmonary Disease in Men and Women in Spain, 1998 to 2018. Journal of Clinical Medicine, 10(7), 1529. https://doi.org/10.3390/jcm10071529