
Intravenous Immunoglobulin Treatment in Kawasaki Disease Decreases the Incidence of Myopia



Abstract
1. Introduction
2. Materials and Methods
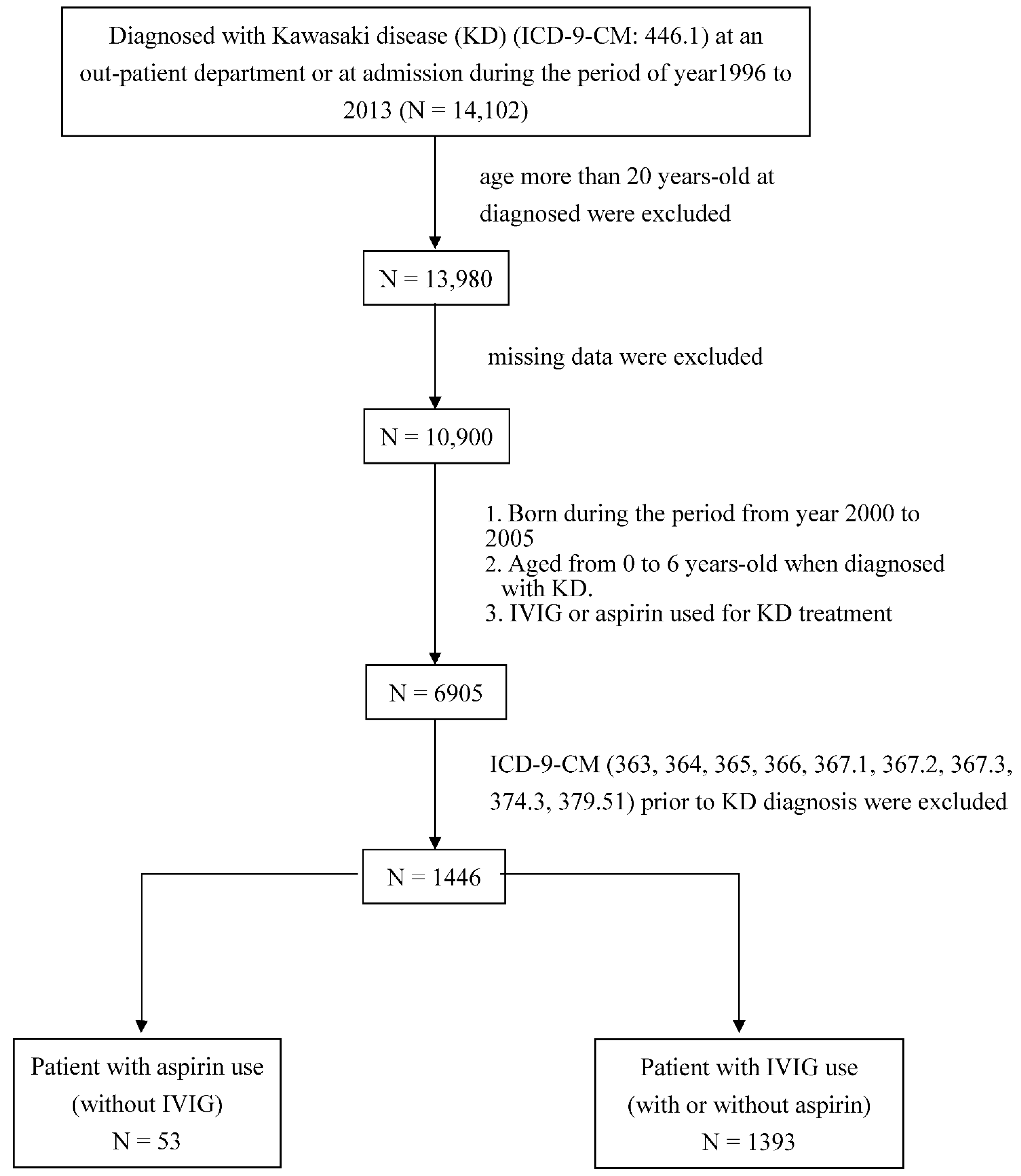
2.1. Subjects
2.2. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Ding, B.Y.; Shih, Y.F.; Lin, L.L.K.; Hsiao, C.K.; Wang, I.J. Myopia among schoolchildren in East Asia and Singapore. Surv. Ophthalmol. 2017, 62, 677–697. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Ohno-Matsui, K.; Saw, S.M. Myopia. Lancet 2012, 379, 1739–1748. [Google Scholar] [CrossRef]
- Metlapally, R.; Wildsoet, C.F. Scleral Mechanisms Underlying Ocular Growth and Myopia. Prog. Mol. Biol. Transl. Sci. 2015, 134, 241–248. [Google Scholar] [PubMed]
- Lin, H.J.; Wei, C.C.; Chang, C.Y.; Chen, T.H.; Hsu, Y.A.; Hsieh, Y.C. Role of Chronic Inflammation in Myopia Progression: Clinical Evidence and Experimental Validation. EBioMedicine 2016, 10, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Kosaki, F.; Okawa, S.; Shigematsu, I.; Yanagawa, H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics 1974, 54, 271–276. [Google Scholar]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.-C. Preventing coronary artery lesions in Kawasaki disease. Biomed. J. 2017, 40, 141–146. [Google Scholar] [CrossRef]
- Nakamura, Y.; Aso, E.; Yashiro, M.; Tsuboi, S.; Kojo, T.; Aoyama, Y. Mortality among Japanese with a history of Kawasaki disease: Results at the end of 2009. J. Epidemiol. 2013, 23, 429–434. [Google Scholar] [CrossRef]
- Nakamura, Y.; Yashiro, M.; Uehara, R.; Oki, I.; Kayaba, K.; Yanagawa, H. Increasing incidence of Kawasaki disease in Japan: Nationwide survey. Pediatrics Int. Off. J. Jpn. Pediatric Soc. 2008, 50, 287–290. [Google Scholar] [CrossRef]
- Lue, H.C.; Chen, L.R.; Lin, M.T.; Chang, L.Y.; Wang, J.K.; Lee, C.Y. Estimation of the incidence of Kawasaki disease in Taiwan. A comparison of two data sources: Nationwide hospital survey and national health insurance claims. Pediatrics Neonatol. 2014, 55, 97–100. [Google Scholar] [CrossRef]
- Huang, Y.H.; Lin, K.M.; Ho, S.C.; Yan, J.H.; Lo, M.H.; Kuo, H.C. Increased Incidence of Kawasaki Disease in Taiwan in Recent Years: A 15 Years Nationwide Population-Based Cohort Study. Front. Pediatr. 2019, 7, 121. [Google Scholar] [CrossRef] [PubMed]
- Holman, R.C.; Belay, E.D.; Christensen, K.Y.; Folkema, A.M.; Steiner, C.A.; Schonberger, L.B. Hospitalizations for Kawasaki syndrome among children in the United States, 1997–2007. Pediatric Infect. Dis. J. 2010, 29, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, K.S.; Weng, K.P.; Lin, C.C.; Huang, T.C.; Lee, C.L.; Huang, S.M. Treatment of acute Kawasaki disease: Aspirin’s role in the febrile stage revisited. Pediatrics 2004, 114, e689–e693. [Google Scholar] [CrossRef]
- Ohno, S.; Miyajima, T.; Higuchi, M.; Yoshida, A.; Matsuda, H.; Saheki, Y. Ocular manifestations of Kawasaki’s disease (mucocutaneous lymph node syndrome). Am. J. Ophthalmol. 1982, 93, 713–717. [Google Scholar] [CrossRef]
- Lee, K.J.; Kim, H.J.; Kim, M.J.; Yoon, J.H.; Lee, E.J.; Lee, J.Y. Usefulness of anterior uveitis as an additional tool for diagnosing incomplete Kawasaki disease. Korean J. Pediatrics 2016, 59, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Kung, Y.J.; Wei, C.C.; Chen, L.A.; Chen, J.Y.; Chang, C.Y.; Lin, C.J. Kawasaki Disease Increases the Incidence of Myopia. BioMed Res. Int. 2017, 2017, 2657913. [Google Scholar] [CrossRef]
- Abe, J.; Ebata, R.; Jibiki, T.; Yasukawa, K.; Saito, H.; Terai, M. Elevated granulocyte colony-stimulating factor levels predict treatment failure in patients with Kawasaki disease. J. Allergy Clin. Immunol. 2008, 122, 1008–1013.e8. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C.; Chang, W.C.; Wang, L.J.; Li, S.C.; Chang, W.P. Association of Attention deficit hyperactivity disorder and Kawasaki disease: A nationwide population-based cohort study. Epidemiol. Psychiatr. Sci. 2016, 25, 573–580. [Google Scholar] [CrossRef]
- Fledelius, H.C. Is myopia getting more frequent? A cross-sectional study of 1416 Danes aged 16 years+. Acta Ophthalmol. 1983, 61, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Tarczy-Hornoch, K.; Ying-Lai, M.; Varma, R. Myopic refractive error in adult Latinos: The Los Angeles Latino Eye Study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1845–1852. [Google Scholar] [CrossRef]
- Wei, C.C.; Kung, Y.J.; Chen, C.S.; Chang, C.Y.; Lin, C.J.; Tien, P.T. Allergic Conjunctivitis-induced Retinal Inflammation Promotes Myopia Progression. EBioMedicine 2018, 28, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.P.; Papadia, M.; Neri, P. Myopia and inflammation. J. Ophthalmic Vis. Res. 2011, 6, 270–283. [Google Scholar]
- Neri, P.; Lettieri, M.; Fortuna, C.; Manoni, M.; Giovannini, A. Inflammatory choroidal neovascularization. Middle East Afr. J. Ophthalmol. 2009, 16, 245–251. [Google Scholar] [PubMed]
- Newburger, J.W.; Takahashi, M.; Burns, J.C.; Beiser, A.S.; Chung, K.J.; Duffy, C.E. The treatment of Kawasaki syndrome with intravenous gamma globulin. N. Engl. J. Med. 1986, 315, 341–347. [Google Scholar] [CrossRef]
- Yuan, J.; Wu, S.; Wang, Y.; Pan, S.; Wang, P.; Cheng, L. Inflammatory cytokines in highly myopic eyes. Sci. Rep. 2019, 9, 3517. [Google Scholar] [CrossRef] [PubMed]
- Hirono, K.; Kemmotsu, Y.; Wittkowski, H.; Foell, D.; Saito, K.; Ibuki, K.; Watanabe, K.; Watanabe, S.; Uese, K.; Saji, T.; et al. Infliximab reduces the cytokine-mediated inflammation but does not suppress cellular infiltration of the vessel wall in refractory Kawasaki disease. Pediatr. Res. 2009, 65, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Hyman, L.; Gwiazda, J.; Hussein, M.; Norton, T.T.; Wang, Y.; Marsh-Tootle, W. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch. Ophthalmol. 2005, 123, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.C.; Tsai, C.L.; Wu, H.L.; Yang, Y.H.; Kuo, H.K. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology 2013, 120, 1080–1085. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Patient with Aspirin Use | Patient with IVIG Use | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Follow-up, years (means ± SD) | 3.67 ± 1.34 | 4.00 ± 1.41 | 0.094 | ||
| Gender | |||||
| Male | 27 | 50.94 | 896 | 64.32 | 0.046 * |
| Female | 26 | 49.06 | 497 | 36.68 | |
| Age, years | |||||
| <1 | 14 | 26.42 | 508 | 36.47 | 0.176 |
| 1~3 | 26 | 49.06 | 656 | 47.09 | |
| 4~6 | 13 | 24.53 | 229 | 16.44 | |
| (means ± SD) | 2.00 ± 1.16 | 1.74 ± 1.29 | 0.153 | ||
| Myopia | |||||
| without | 36 | 67.92 | 1083 | 77.75 | 0.093 |
| with | 17 | 32.08 | 310 | 22.25 | |
| Variables | Crude HR (95% CI) | Adjusted HR (95% CI) |
|---|---|---|
| Kawasaki disease | ||
| Aspirinuse | 1.00 | 1.00 |
| IVIG use | 0.59 (0.36~0.96) * | 0.62 (0.38~1.02) |
| Gender | ||
| Boy | 1.00 | 1.00 |
| Girl | 0.62 (0.49~0.79) † | 0.68 (0.53~0.87) ** |
| Age, years | ||
| <1 | 1.00 | 1.00 |
| 1~3 | 1.94 (1.49~2.53) † | 1.89 (1.45~2.47) † |
| 4~6 | 10.94 (7.29~16.42) † | 10.10 (6.71~15.19) † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.-J.; Chuang, M.-N.; Chu, C.-L.; Wu, P.-L.; Ho, S.-C.; Kuo, H.-C. Intravenous Immunoglobulin Treatment in Kawasaki Disease Decreases the Incidence of Myopia. J. Clin. Med. 2021, 10, 1381. https://doi.org/10.3390/jcm10071381
Yu H-J, Chuang M-N, Chu C-L, Wu P-L, Ho S-C, Kuo H-C. Intravenous Immunoglobulin Treatment in Kawasaki Disease Decreases the Incidence of Myopia. Journal of Clinical Medicine. 2021; 10(7):1381. https://doi.org/10.3390/jcm10071381
Chicago/Turabian StyleYu, Hun-Ju, Meng-Ni Chuang, Chiao-Lun Chu, Pei-Lin Wu, Shu-Chen Ho, and Ho-Chang Kuo. 2021. "Intravenous Immunoglobulin Treatment in Kawasaki Disease Decreases the Incidence of Myopia" Journal of Clinical Medicine 10, no. 7: 1381. https://doi.org/10.3390/jcm10071381
APA StyleYu, H.-J., Chuang, M.-N., Chu, C.-L., Wu, P.-L., Ho, S.-C., & Kuo, H.-C. (2021). Intravenous Immunoglobulin Treatment in Kawasaki Disease Decreases the Incidence of Myopia. Journal of Clinical Medicine, 10(7), 1381. https://doi.org/10.3390/jcm10071381