Epidemiology and Viral Etiology of Pediatric Immune Thrombocytopenia through Korean Public Health Data Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. HIRA Databases
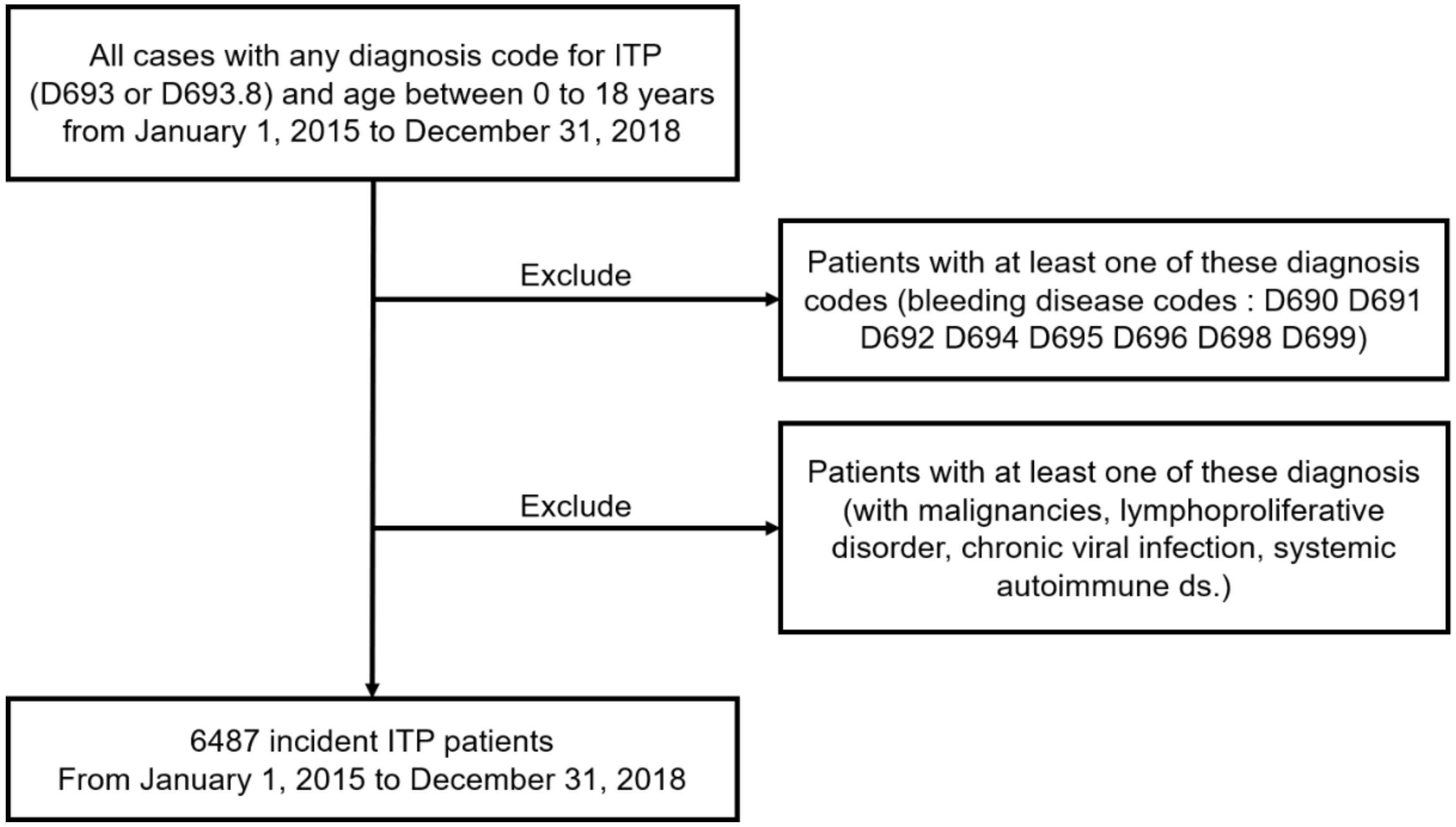
2.2. Study Population
2.3. The Surveillance Data of Virus
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
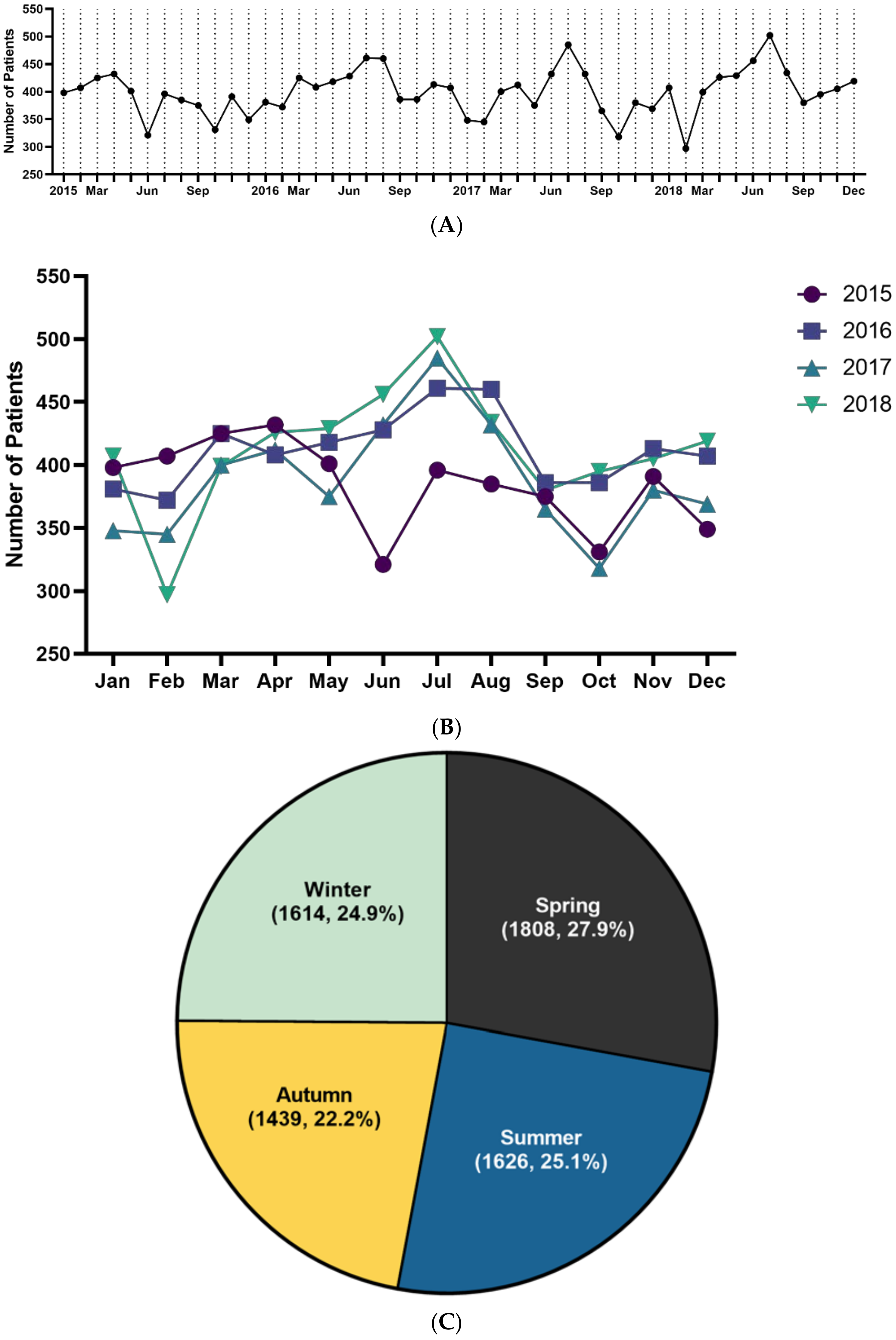
3.2. Trend Analysis of ITP
3.3. Positive Detection Rates of Virus
3.4. Causality between ITP and Virus Prevalence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lilleyman, J.S. Intracranial haemorrhage in idiopathic thrombocytopenic purpura. Paediatric Haematology Forum of the British Society for Haematology. Arch. Dis. Child. 1994, 71, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Bolton-Maggs, P.H.; Moon, I. Assessment of UK practice for management of acute childhood idiopathic thrombocytopenic purpura against published guidelines. Lancet 1997, 350, 620–623. [Google Scholar] [CrossRef]
- Zeller, B.; Helgestad, J.; Hellebostad, M.; Kolmannskog, S.; Nystad, T.; Stensvold, K. Immune thrombocytopenic purpura in childhood in Norway: A prospective, population-based registration. Pediat. Hematol. Oncol. 2000, 17, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, H.; Schmidt, K. The incidence of idiopathic thrombocytopenic purpura in adults increases with age. Blood 1999, 94, 909–913. [Google Scholar] [CrossRef]
- Neylon, A.J.; Saunders, P.W.; Howard, M.R.; Proctor, S.J.; Taylor, P.R.; Northern Region Haematology Group. Clinically significant newly presenting autoimmune thrombocytopenic purpura in adults: A prospective study of a population-based cohort of 245 patients. Br. J. Hematol. 2003, 122, 966–974. [Google Scholar] [CrossRef]
- Abrahamson, P.E.; Hall, S.A.; Feudjo-Tepie, M.; Mitrani-Gold, F.S.; Logie, J. The incidence of idiopathic thrombocytopenic purpura among adults: A population-based study and literature review. Eur. J. Haematol. 2009, 83, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Zeller, B.; Rajantie, J.; Hedlund-Treutiger, I.; Tedgard, U.; Wesenberg, F.; Jonsson, O.G.; Henter, J.I.; Rosthøj, S. Childhood idiopathic thrombocytopenic purpura in the Nordic countries: Epidemiology and predictors of chronic disease. Acta Paediatr. 2005, 94, 178–184. [Google Scholar] [CrossRef]
- Yong, M.; Schoonen, W.M.; Li, L.; Kanas, G.; Coalson, J.; Mowat, F.; Fryzek, J.; Kaye, J.A. Epidemiology of paediatric immune thrombocytopenia in the General Practice Research Database. Br. J. Haematol. 2010, 149, 855–864. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, J.H.; Lee, H.; Kang, B.; Kim, J.W.; Kim, S.H.; Lee, J.O.; Kim, J.W.; Kim, Y.J.; Lee, K.W.; et al. Epidemiology and management of primary immune thrombocytopenia: A nationwide population-based study in Korea. Thromb. Res. 2017, 155, 86–91. [Google Scholar] [CrossRef]
- Kim, T.O.; Despotovic, J.; Lambert, M.P. Eltrombopag for use in children with immune thrombocytopenia. Blood Adv. 2018, 2, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Kuhne, T. Diagnosis and management of immune thrombocytopenia in childhood. Hamostaseologie 2017, 37, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Nagamine, T.; Ohtuka, T.; Takehara, K.; Arai, T.; Takagi, H.; Mori, M. Thrombocytopenia associated with hepatitis C viral infection. J. Hepatol. 1996, 24, 135–140. [Google Scholar] [CrossRef]
- Rand, M.L.; Wright, J.F. Virus-associated idiopathic thrombocytopenic purpura. Transfus. Sci. 1998, 19, 253–259. [Google Scholar] [CrossRef]
- Yan, M.; Zhang, Y.; Yang, F.; Ji, L.; Wang, M.; Wang, W. Comparative study between chronic immune thrombocytopenia patients and healthy population on Epstein–Barr virus infection status by polymerase chain reaction. Exp. Rev. Hematol. 2020, 13, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Veneri, D.; Lippi, G. Thrombocytopenia and infections. Exp. Rev. Hematol. 2017, 10, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Justiz Vaillant, A.A.; Gupta, N. ITP–Immune Thrombocytopenic Purpura; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kim, D.S. Introduction, health of the health care system in Korea. Soc. Work Public Health 2010, 25, 127–141. [Google Scholar] [CrossRef]
- Kim, D.S. Special issue on the national health care system of South Korea. Soc. Work Public Health 2010, 25, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of Health Insurance Review and Assessment Service National Patient Samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef]
- Rodeghiero, F.; Stasi, R.; Gernsheimer, T.; Michel, M.; Provan, D.; Arnold, D.M.; Bussel, J.B.; Cines, D.B.; Chong, B.H.; Cooper, N.; et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children, report from an international working group. Blood 2009, 113, 2386–2393. [Google Scholar] [CrossRef]
- Granger, C.W.J. Investigating causal relations by econometric models and cross–spectral methods. Econometrica 1969, 37, 424. [Google Scholar] [CrossRef]
- Moulis, G.; Palmaro, A.; Montastruc, J.L.; Godeau, B.; Lapeyre–Mestre, M.; Sailler, L. Epidemiology of incident immune thrombocytopenia, a nationwide population–based study in France. Blood 2014, 124, 3308–3315. [Google Scholar] [CrossRef] [PubMed]
- Kurata, Y.; Fujimura, K.; Kuwana, M.; Tomiyama, Y.; Murata, M. Epidemiology of primary immune thrombocytopenia in children and adults in Japan, a population–based study and literature review. Intern. J. Hematol. 2011, 93, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Nugent, D.J. Childhood immune thrombocytopenic purpura. Blood Rev. 2002, 16, 27–29. [Google Scholar] [CrossRef]
- Morse, E.E.; Zinkham, W.H.; Jackson, D.P. Thrombocytopenic purpura following rubella infection in children and adults. Arch. Intern. Med. 1966, 117, 573–579. [Google Scholar] [CrossRef]
- Hsiao, C.C. Epstein–Barr virus associated with immune thrombocytopenic purpura in childhood, a retrospective study. J. Paediatr. Child. Health. 2000, 36, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.C.; Kelley, P.K.; Hogrefe, W.R.; McClain, K.L. Childhood idiopathic thrombocytopenic purpura, association with human parvovirus B19 infection. Am. J. Pediatr. Hematol. Oncol. 1994, 16, 314–319. [Google Scholar]
- Pokhrel, S.D.; Persons, D.L.; Aljitawi, O.S. RSV-related thrombocytopenia associated with transient cytogenetic abnormalities in a recipient of umbilical cord blood transplantation. Case Rep. Hematol. 2016, 2016, 8628507. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Tuncer, H. A case of primary refractory immune thrombocytopenia, challenges in choice of therapies. Case Rep. Hematol. 2018, 2018, 8207017. [Google Scholar] [CrossRef]
- Tsao, H.S.; Chason, H.M.; Fearon, D.M. Immune Thrombocytopenia (ITP) in a pediatric patient positive for SARS–CoV–2. Pediatrics 2020, 146, e20201419. [Google Scholar] [CrossRef]
- Kaneko, H.; Ohkawara, Y.; Nomura, K.; Horiike, S.; Taniwaki, M. Relapse of idiopathic thrombocytopenic purpura caused by influenza A virus infection, a case report. J. Infect. Chemother. 2004, 10, 364–366. [Google Scholar] [CrossRef]
- Lee, C.Y.; Wu, M.C.; Chen, P.Y.; Chou, T.Y.; Chan, Y.J. Acute immune thrombocytopenic purpura in an adolescent with 2009 novel H1N1 influenza A virus infection. J. Chin. Med. Assoc. 2011, 74, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Kang, S.; Kang, J.H.; Ma, S.H. A case of acute idiopathic thrombocytopenic purpura following Influenza B virus infection. Pediatr. Infect. Vaccine 2015, 22, 117–120. [Google Scholar] [CrossRef]
- Magdi, M.; Rahil, A. Severe immune thrombocytopenia complicated by intracerebral haemorrhage associated with coronavirus infection, a case report and literature review. Eur. J. Case Rep. Intern. Med. 2019, 6, 001155. [Google Scholar] [PubMed]
- Zea-Vera, A.F.; Parra, B. Zika virus (ZIKV) infection related with immune thrombocytopenic purpura (ITP) exacerbation and antinuclear antibody positivity. Lupus 2017, 26, 890–892. [Google Scholar] [CrossRef] [PubMed]
- Ai, Q.; Yin, J.; Chen, S.; Qiao, L.; Luo, N. Rotavirus–associated immune thrombocytopenic purpura in children, a retrospective study. Exp. Ther. Med. 2016, 12, 2187–2190. [Google Scholar] [CrossRef][Green Version]
- Yu, J.; Lai, S.; Geng, Q.; Ye, C.; Zhang, Z.; Zheng, Y.; Wang, L.; Duan, Z.; Zhang, J.; Wu, S.; et al. Prevalence of rotavirus and rapid changes in circulating rotavirus strains among children with acute diarrhea in China, 2009–2015. J. Infect. 2019, 78, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.K.; Hwang, S.H.; Nam, H.N.; Han, K.; Kim, B.; Kong, I.; Park, K.; Lee, J. Incidence of intussusception before and after the introduction of rotavirus vaccine in Korea. PLoS ONE 2020, 15, e0238185. [Google Scholar] [CrossRef]
- Burbelo, P.D.; Ching, K.H.; Esper, F.; Iadarola, M.J.; Delwart, E.; Lipkin, W.I.; Kapoor, A. Serological studies confirm the novel astrovirus HMOAstV–C as a highly prevalent human infectious agent. PLoS ONE 2011, 6, e22576. [Google Scholar] [CrossRef]
- Arias, C.F.; DuBois, R.M. The Astrovirus capsid: A review. Viruses 2017, 9, 15. [Google Scholar] [CrossRef]
- Li, J.; Tao, Y.; Tang, M.; Du, B.; Xia, Y.; Mo, X.; Cao, Q. Rapid detection of respiratory organisms with the FilmArray respiratory panel in a large children’s hospital in China. BMC Infect. Dis. 2018, 18, 510. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Lee, J.H.; Kim, Y.K. Laboratory impact of rapid molecular tests used for the detection of respiratory pathogens. Clin. Lab. 2018, 64, 1545–1551. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age Group, n (%) | 0–1 Year | 1.1–5 Years | 5.1–18 Years | Total |
|---|---|---|---|---|
| Total | 2470 (38.1) | 1895 (29.2) | 2122 (32.7) | 6487 (100.0) |
| Male | 1433 (22.1) | 1010 (15.6) | 1087 (16.8) | 3530 (54.4) |
| Female | 1037 (16.0) | 885 (13.6) | 1035 (15.9) | 2957 (45.6) |
| Male to female ratio | 1.4 | 1.1 | 1.1 | 1.2 |
| Incidence rate | 145.4 | 25.7 | 7.9 | 18.1 |
| 0–1 Year | 1.1–5 Year | <5 Year | 5.1–18 Year | |
|---|---|---|---|---|
| HAdV | 0.532 | 0.881 | 0.831 | 0.353 |
| HPIV | 0.619 | 0.560 | 0.992 | 0.869 |
| HRSV | 0.696 | 0.918 | 0.772 | 0.030 |
| IFV | 0.599 | 0.924 | 0.782 | 0.996 |
| HCoV | 0.522 | 0.764 | 0.564 | 0.065 |
| HRV | 0.052 | 0.469 | 0.475 | 0.312 |
| HBoV | 0.493 | 0.489 | 0.960 | 0.887 |
| HMPV | 0.082 | 0.891 | 0.396 | 0.202 |
| Rotavirus | 0.208 | 0.085 | 0.035 | 0.837 |
| Norovirus | 0.832 | 0.571 | 0.873 | 0.079 |
| Adenovirus | 0.385 | 0.486 | 0.319 | 0.482 |
| Astrovirus | 0.646 | 0.871 | 0.169 | 0.029 |
| 0–1 Year | 1.1–5 Year | <5 Year | 5.1–18 Year | |
|---|---|---|---|---|
| HAdV | 0.638 | 0.893 | 0.947 | 0.411 |
| HPIV | 0.885 | 0.840 | 0.836 | 0.997 |
| HRSV | 0.885 | 0.426 | 0.517 | 0.063 |
| IFV | 0.472 | 0.350 | 0.871 | 0.242 |
| HCoV | 0.133 | 0.766 | 0.251 | 0.241 |
| HRV | 0.015 | 0.708 | 0.274 | 0.370 |
| HBoV | 0.706 | 0.369 | 0.513 | 0.995 |
| HMPV | 0.114 | 0.176 | 0.090 | 0.487 |
| Rotavirus | 0.050 | 0.093 | 0.031 | 0.877 |
| Norovirus | 0.065 | 0.972 | 0.375 | 0.314 |
| Adenovirus | 0.518 | 0.266 | 0.503 | 0.212 |
| Astrovirus | 0.104 | 0.761 | 0.493 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, J.H.; Kim, Y.K.; Min, S.H.; Kim, S.W.; Lee, Y.H.; Lee, J.M. Epidemiology and Viral Etiology of Pediatric Immune Thrombocytopenia through Korean Public Health Data Analysis. J. Clin. Med. 2021, 10, 1356. https://doi.org/10.3390/jcm10071356
Lim JH, Kim YK, Min SH, Kim SW, Lee YH, Lee JM. Epidemiology and Viral Etiology of Pediatric Immune Thrombocytopenia through Korean Public Health Data Analysis. Journal of Clinical Medicine. 2021; 10(7):1356. https://doi.org/10.3390/jcm10071356
Chicago/Turabian StyleLim, Jae Hee, Yu Kyeong Kim, So Hyeon Min, Sang Won Kim, Young Hwan Lee, and Jae Min Lee. 2021. "Epidemiology and Viral Etiology of Pediatric Immune Thrombocytopenia through Korean Public Health Data Analysis" Journal of Clinical Medicine 10, no. 7: 1356. https://doi.org/10.3390/jcm10071356
APA StyleLim, J. H., Kim, Y. K., Min, S. H., Kim, S. W., Lee, Y. H., & Lee, J. M. (2021). Epidemiology and Viral Etiology of Pediatric Immune Thrombocytopenia through Korean Public Health Data Analysis. Journal of Clinical Medicine, 10(7), 1356. https://doi.org/10.3390/jcm10071356