
Apheresis Efficacy and Tolerance in the Setting of HLA-Incompatible Kidney Transplantation

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Endpoints
2.3. Procedures
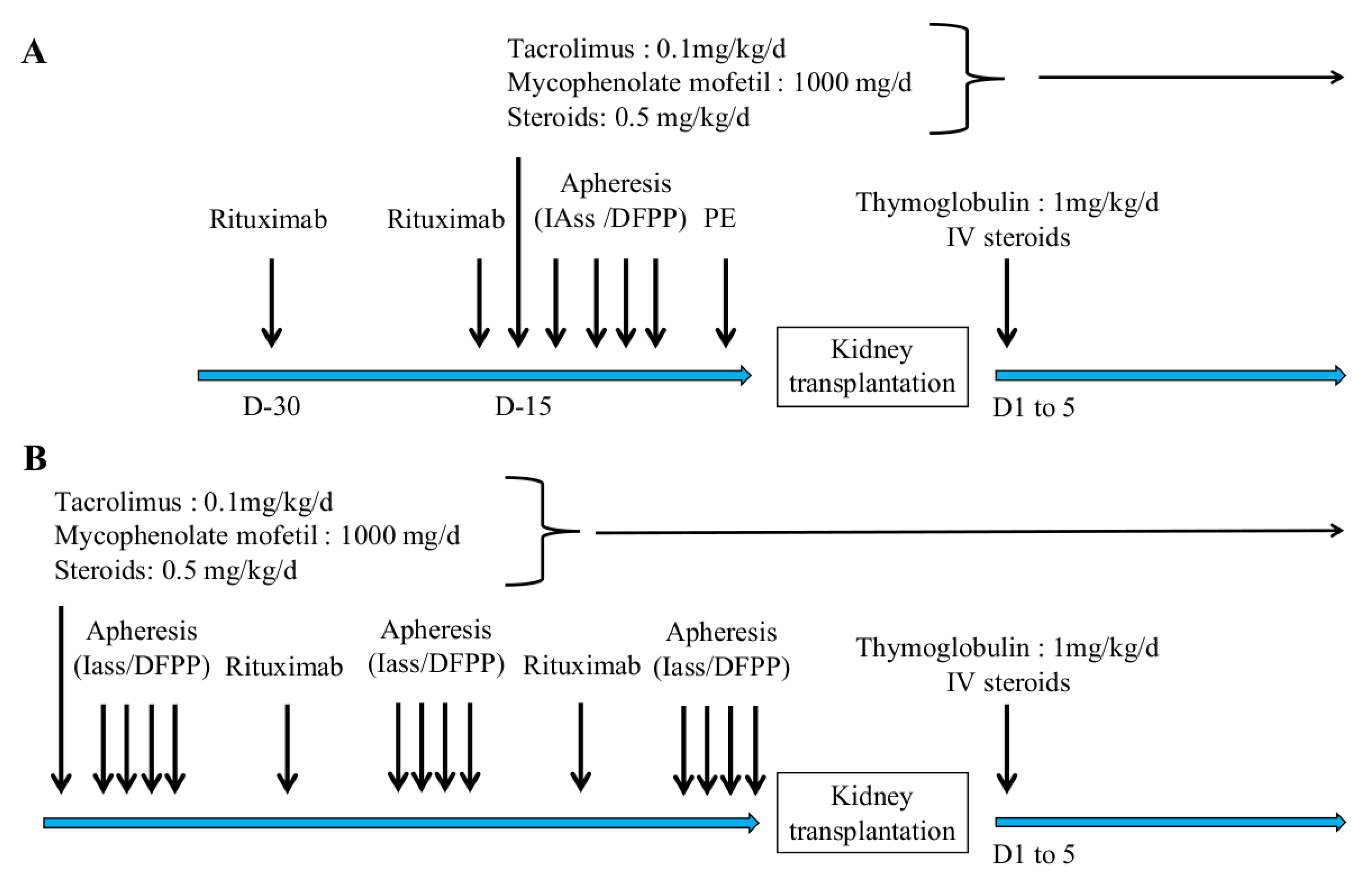
2.4. Desensitization Protocol
2.5. Statistical Analyses
3. Results
3.1. Study Population
3.2. Characteristics of Apheresis for HLAi Kidney Transplantation
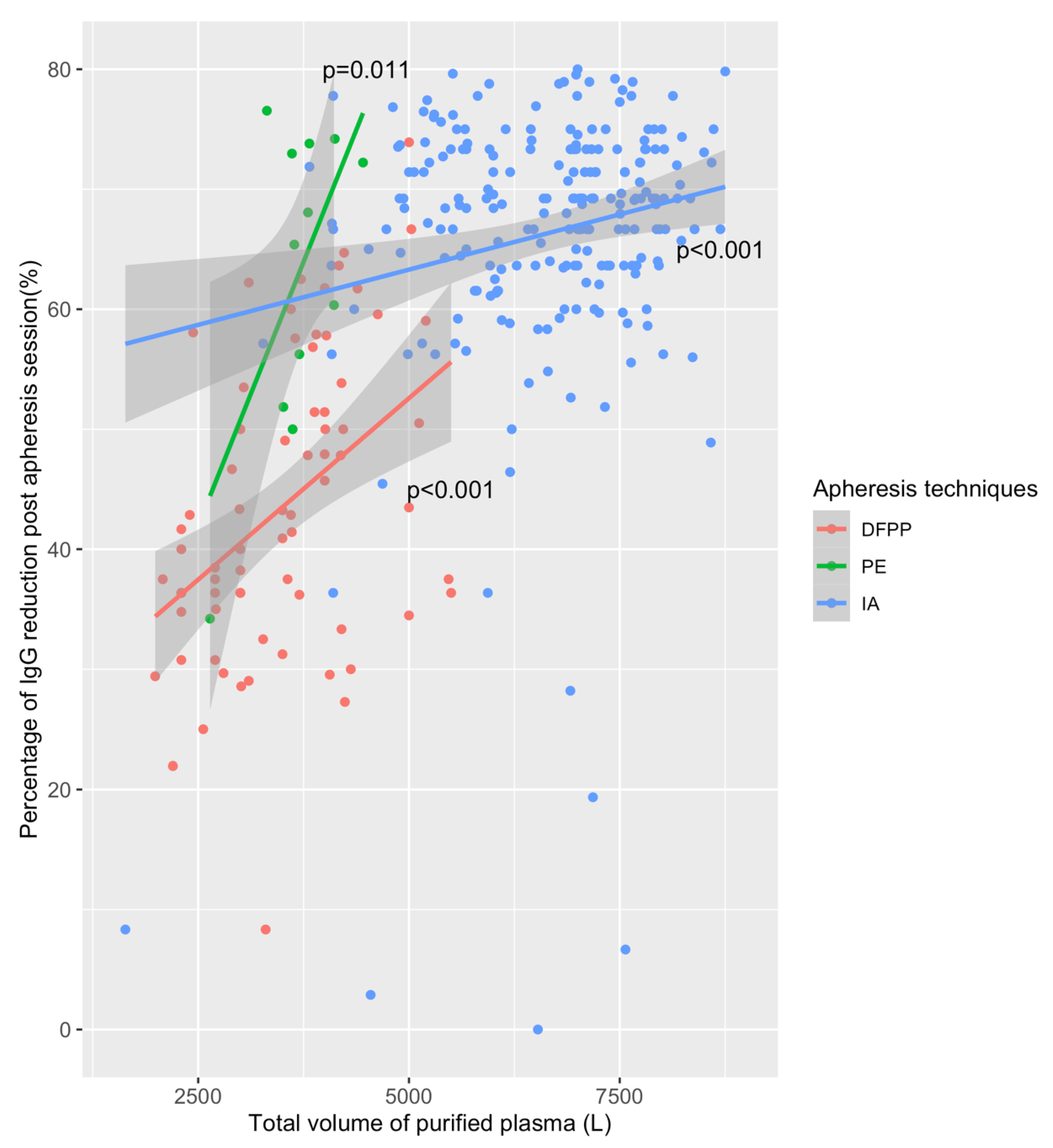
3.3. Efficacy of Apheresis and Access to Kidney Transplantation
3.4. Apheresis Tolerance
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef]
- Malvezzi, P.; Jouve, T.; Noble, J.; Rostaing, L. Desensitization in the Setting of HLA-Incompatible Kidney Transplant. Exp. Clin. Transpl. 2018, 16, 367–375. [Google Scholar]
- Pruthi, R.; Hilton, R.; Pankhurst, L.; Mamode, N.; Hudson, A.; Roderick, P.; Ravanan, R. UK Renal Registry 16th Annual Report: Chapter 4 Demography of Patients Waitlisted for Renal Transplantation in the UK: National and Centre-Specific Analyses. Nephron Clin. Pract. 2013, 125, 81–98. [Google Scholar] [CrossRef]
- Claas, F.H.J.; Witvliet, M.D.; Duquesnoy, R.J.; Persijn, G.G.; Doxiadis, I.I.N. The Acceptable Mismatch Program as a Fast Tool for Highly Sensitized Patients Awaiting a Cadaveric Kidney Transplantation: Short Waiting Time and Excellent Graft Outcome. Transplant. J. 2004, 78, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Gridelli, B.; Remuzzi, G. Strategies for Making More Organs Available for Transplantation. N. Engl. J. Med. 2000, 343, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Orandi, B.J.; Montgomery, R.A.; Segev, D.L. Kidney Transplants from HLA-Incompatible Live Donors and Survival. N. Engl. J. Med. 2016, 375, 288–289. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Suberbielle-Boissel, C.; Zuber, J.; Anglicheau, D.; Timsit, M.-O.; Martinez, F.; Thervet, E.; Bruneval, P.; Charron, D.; Hill, G.S.; et al. Combined Posttransplant Prophylactic IVIg/Anti-CD 20/Plasmapheresis in Kidney Recipients with Preformed Donor-Specific Antibodies: A Pilot Study. Transplantation 2010, 89, 1403–1410. [Google Scholar] [CrossRef]
- Defendi, F.; Malvezzi, P.; Eskandary, F.; Cesbron, J.-Y.; Rostaing, L.; Böhmig, G.A.; Dumestre-Pérard, C. Effects of Immunoadsorption Combined with Membrane Filtration on Complement Markers-Results of a Randomized, Controlled, Crossover Study. Transpl. Int. 2019, 32, 876–883. [Google Scholar] [CrossRef]
- Shin, B.-H.; Everly, M.J.; Zhang, H.; Choi, J.; Vo, A.; Zhang, X.; Huang, E.; Jordan, S.C.; Toyoda, M. Impact of Tocilizumab (Anti-IL-6R) Treatment on Immunoglobulins and Anti-HLA Antibodies in Kidney Transplant Patients with Chronic Antibody-Mediated Rejection. Transplantation 2020, 104, 856–863. [Google Scholar] [CrossRef]
- Sokolov, A.A.; Solovyev, A.G. Russian Pioneers of Therapeutic Hemapheresis and Extracorporeal Hemocorrection: 100-Year Anniversary of the World’s First Successful Plasmapheresis. Ther. Apher. Dial. 2014, 18, 117–121. [Google Scholar] [CrossRef]
- Salvadori, M.; Tsalouchos, A. Therapeutic Apheresis in Kidney Transplantation: An Updated Review. World J. Transpl. 2019, 9, 103–122. [Google Scholar] [CrossRef]
- Sapir-Pichhadze, R.; Tinckam, K.J.; Laupacis, A.; Logan, A.G.; Beyene, J.; Kim, S.J. Immune Sensitization and Mortality in Wait-Listed Kidney Transplant Candidates. J. Am. Soc. Nephrol. 2016, 27, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Choi, J.; Toyoda, M.; Vo, A.; Peng, A.; Jordan, S.C. Desensitization: Overcoming the Immunologic Barriers to Transplantation. J. Immunol. Res. 2017, 2017, 6804678. [Google Scholar] [CrossRef]
- Cardella, C.J.; Sutton, D.; Uldall, P.R.; Deveber, G.A. Intensive plasma exchange and renal-transplant rejection. Lancet 1977, 309, 264. [Google Scholar] [CrossRef]
- Stegall, M.D.; Gloor, J.; Winters, J.L.; Moore, S.B.; Degoey, S. A Comparison of Plasmapheresis versus High-Dose IVIG Desensitization in Renal Allograft Recipients with High Levels of Donor Specific Alloantibody. Am. J. Transpl. 2006, 6, 346–351. [Google Scholar] [CrossRef]
- Kaplan, A.A. Toward the Rational Prescription of Therapeutic Plasma Exchange: The Kinetics of Immunoglobulin Removal. Semin. Dial. 1992, 5, 227–229. [Google Scholar] [CrossRef]
- Hafer, C.; Golla, P.; Gericke, M.; Eden, G.; Beutel, G.; Schmidt, J.J.; Schmidt, B.M.W.; De Reys, S.; Kielstein, J.T. Membrane versus Centrifuge-Based Therapeutic Plasma Exchange: A Randomized Prospective Crossover Study. Int. Urol. Nephrol. 2016, 48, 133–138. [Google Scholar] [CrossRef]
- Sanchez, A.P.; Cunard, R.; Ward, D.M. The Selective Therapeutic Apheresis Procedures. J. Clin. Apher. 2013, 28, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Böhmig, G.A.; Wahrmann, M.; Regele, H.; Exner, M.; Robl, B.; Derfler, K.; Soliman, T.; Bauer, P.; Müllner, M.; Druml, W. Immunoadsorption in Severe C4d-Positive Acute Kidney Allograft Rejection: A Randomized Controlled Trial. Am. J. Transpl. 2007, 7, 117–121. [Google Scholar] [CrossRef]
- Palmer, A.; Taube, D.; Welsh, K.; Bewick, M.; Gjorstrup, P.; Thick, M. Removal of Anti-HLA Antibodies by Extracorporeal Immunoadsorption to Enable Renal Transplantation. Lancet 1989, 1, 10–12. [Google Scholar] [CrossRef]
- Rostaing, L.; Congy, N.; Aarnink, A.; Maggioni, S.; Allal, A.; Sallusto, F.; Game, X.; Kamar, N. Efficacy of Immunoadsorption to Reduce Donor-Specific Alloantibodies in Kidney-Transplant Candidates. Exp. Clin. Transpl. 2015, 13 (Suppl. 1), 201–206. [Google Scholar]
- Ronspeck, W.; Brinckmann, R.; Egner, R.; Gebauer, F.; Winkler, D.; Jekow, P.; Wallukat, G.; Muller, J.; Kunze, R. Peptide Based Adsorbers for Therapeutic Immunoadsorption. Ther. Dial. 2003, 7, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Belàk, M.; Borberg, H.; Jimenez, C.; Oette, K. Technical and Clinical Experience with Protein a Immunoadsorption Columns. Transfus. Sci. 1994, 15, 419–422. [Google Scholar] [CrossRef]
- Lorenz, M.; Regele, H.; Schillinger, M.; Kletzmayr, J.; Haidbauer, B.; Derfler, K.; Druml, W.; Böhmig, G.A. Peritransplant Immunoadsorption: A Strategy Enabling Transplantation in Highly Sensitized Crossmatch-Positive Cadaveric Kidney Allograft Recipients. Transplantation 2005, 79, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.; Lowe, D.; Hathaway, M.; Lam, F.T.; Kashi, H.; Tan, L.C.; Imray, C.; Fletcher, S.; Chen, K.; Krishnan, N.; et al. Double Filtration Plasmapheresis in Antibody-Incompatible Kidney Transplantation. Ther. Apher. Dial. 2010, 14, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tang, Z.; Chen, D.; Gong, D.; Ji, D.; Liu, Z. Comparison of Double Filtration Plasmapheresis with Immunoadsorption Therapy in Patients with Anti-Glomerular Basement Membrane Nephritis. BMC Nephrol. 2014, 15, 128. [Google Scholar] [CrossRef]
- Gurland, H.J.; Lysaght, M.J.; Samtleben, W.; Schmidt, B. Comparative Evaluation of Filters Used in Membrane Plasmapheresis. Nephron 1984, 36, 173–182. [Google Scholar] [CrossRef]
- Huestis, D.W. Mortality in Therapeutic Haemapheresis. Lancet 1983, 1, 1043. [Google Scholar] [CrossRef]
- Biesenbach, P.; Eskandary, F.; Ay, C.; Wiegele, M.; Derfler, K.; Schaden, E.; Haslacher, H.; Oberbauer, R.; Böhmig, G.A. Effect of Combined Treatment with Immunoadsorption and Membrane Filtration on Plasma Coagulation—Results of a Randomized Controlled Crossover Study. J. Clin. Apher. 2016, 31, 29–37. [Google Scholar] [CrossRef]
- Keller, A.J.; Chirnside, A.; Urbaniak, S.J. Coagulation Abnormalities Produced by Plasma Exchange on the Cell Separator with Special Reference to Fibrinogen and Platelet Levels. Br. J. Haematol. 1979, 42, 593–603. [Google Scholar] [CrossRef]
- Sutton, D.M.; Nair, R.C.; Rock, G. Complications of Plasma Exchange. Transfusion 1989, 29, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Siami, G.A.; Siami, F.S. Membrane Plasmapheresis in the United States: A Review over the Last 20 Years. Ther. Apher. 2001, 5, 315–320. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Desensitization with Living Donors | Desensitization with a Total of Deceased Donors | Total | p-Value | |
|---|---|---|---|---|
| N = 18 | N = 27 | N = 45 | ||
| Age at inclusion (years) | 53.6 ± 15 | 51.9 ± 12 | 52.6 ± 13 | 0.84 |
| Male/Female gender ratio | 7/11 | 13/14 | 20/25 | 0.54 |
| Body Mass index (Kg/m2) | 24.5 ± 3 | 24.2 ± 4 | 24.3 ± 4 | 0.54 |
| History of previous transplantation—N (%) | 6 (35.3) | 17 (77.3) | 23 (59) | 0.02 |
| Pre-emptive kidney trans—N (%) | 1 (5.9) | 0 (0) | 1 (2.6) | 0.25 |
| Time on dialysis (months) | 17 ± 15 | 150 ± 114 | 92 ± 108 | <0.001 |
| cPRA (%) | 65 ± 35 | 96 ± 5 | 84 ± 26 | <0.001 |
| >1 class I DSA—N (%) | 11 (65) | 16 (59) | 27 (60) | 0.09 |
| >1 class II DSA—N (%) | 12 (66.6) | 13 (48) | 25 (55.5) | 0.01 |
| Number of class I | 17 KT | 22 KT | 39 KT | 0.31 |
| Missmatch—N (%) | ||||
| 1 | 1 (5.8) | 0 (0) | 1 (2.5) | |
| 2 | 7 (41) | 6 (27) | 13 (33.3) | |
| 3 | 8 (47) | 9 (41) | 17 (43.5) | |
| 4 | 1 (5.8) | 5 (22.7) | 6 (15.3) | |
| Number of class II | 0.93 | |||
| Missmatch—N (%) | ||||
| 0 | 3 (17.6) | 3 (13.6) | 6 (15.3) | |
| 1 | 3 (17.6) | 5 (22.7) | 8 (20.5) | |
| 2 | 7 (41) | 8 (36.3) | 15 (38.4) | |
| 3 | 2 (11.7) | 3 (13.6) | 5 (12.8) | |
| 4 | 2 (11.7) | 1 (4.5) | 3 (7.7) | |
| Mean number of PE sessions | 2 ± 1 | 1 ± 1 | 1 ± 1 | 0.04 |
| Mean number of DFPP sessions | 3 ± 3 | 2 ± 3 | 2 ± 3 | 0.61 |
| Mean number of IA sessions | 6 ± 7 | 22 ± 17 | 16 ± 15 | <0.001 |
| Trough tacrolimus level (ng/mL) at inclusion | 4.9 ± 0.5 | 9.8 ± 5.8 | 8.5 ± 5.5 | 0.02 |
| DFPP (N = 107) | PE (N = 54) | IA (N = 720) | Total (N = 881) | p-Value | |
|---|---|---|---|---|---|
| Duration of session (hours). Median [IQ] | 2 (1.8–2.3) | 1.7 (1.5–2.0) | 3.5 (2.9–4.0) | 3.2 (2.6–3.9) | <0.01 |
| Treated plasma volume (L). Median [IQ] | 3675 (3000–4200) | 4200 (2564–3685) | 6641 (5520–7523) | 6035 (4803–7286) | <0.01 |
| Blood flow (mL/min) Mean ± SD | 146 ± 14 | 63 ± 38 | 54 ± 7 | 65 ± 32 | <0.01 |
| Substitution volume (L) Mean ± SD | 259 ± 224 | 2857 ± 750 | 104 ± 53 | 295 ± 717 | <0.01 |
| Substitution fluid N (%) | <0.01 | ||||
| – Albumin 20% | 10 (9.3%) | 0 (0%) | 720 (100%) | 730 (83%) | |
| – Albumin 20% + saline serum | 88 (82.2%) | 0 (0%) | 0 (0%) | 88 (10%) | |
| – Albumin 4% | 9 (8.4%) | 20 (37%) | 0 (0%) | 29 (3.2%) | |
| – FFP | 0 (0%) | 34 (63.0%) | 0 (0%) | 34 (3.9%) |
| DSA Class I | DSA Class II | |||
| Univariate p-Value | Multivariate p-Value | Univariate p-Value | Multivariate p-Value | |
| Volume of treated plasma | 0.01 | 0.03 | 0.07 | 0.37 |
| Technique of apheresis | 0.20 | 0.60 (IA) | 0.02 (PE) | <0.01 (PE) |
| (IA and PE vs. DFPP) | 0.01 (IA) | <0.01 (IA) | ||
| Duration of session | 0.89 | - | 0.10 | - |
| Maximum MFI of DSA | 0.39 | 0.19 | <0.01 | <0.01 |
| DSA Class I | DSA Class II | |||
|---|---|---|---|---|
| Univariate p-Value | Multivariate p-Value | Univariate p-Value | Multivariate p-Value | |
| Volume of treated Plasma | 0.24 | 0.04 | 0.06 | 0.02 |
| Technique of apheresis | 0.86 (PE) | 0.83 (PE) | 0.22 (PE) | 0.18 (PE) |
| (IA and PE vs. DFPP) | 0.11 (IA) | 0.03 (IA) | 0.76 (IA) | 0.38 (IA) |
| Delay between sessions | 0.42 | - | 0.49 | |
| Duration of session | 0.92 | - | 0.78 | - |
| DFPP (N = 107) | PE (N = 54) | IA (N = 720) | Total (N = 881) | p-Value | |
|---|---|---|---|---|---|
| Pre-post IgA evolution (%) Median [IQ] | −55 (−45; −63) | −48 (−1; −71) | −14 (−7; −21) | −17 (−8; −29) | <0.01 |
| Pre-post IgG evolution (%) Median [IQ] | −40 (−31; −50) | −61 (−46; −73) | −60 (−33; −70) | −56 (−33; −69) | <0.01 |
| Pre-post IgM evolution (%) Median [IQ] | −37 (0; −58) | −51 (60; −75) | −17 (0; −54) | −17 (0; −57) | 0.10 |
| Pre-post Alb evolution (%) Median [IQ] | 1 (14; 2) | 10 (14; −3) | 9 (14; −1) | 9 (15; 0) | 0.73 |
| Pre-post fibrinogen evolution (%) Median [IQ] | −61 (−56; −69) | −33 (−29; −64) | −43 (−22; −57) | −47 (23; −60) | <0.01 |
| Pre-post hemoglobin evolution (%) Median [IQ] | 15 (22; −8) | 2 (10; −2) | 2 (9; −2) | 3 (11; −2) | <0.01 |
| Pre-post leukocytes Evolution (%) Median [IQ] | 65 (96; 33) | 22 (60; 5) | 4 (18; 8) | 8 (27; 6) | <0.01 |
| Pre-post platelet evolution (%) Median [IQ] | 7 (−1; 17) | 14 (2; 21) | 12 (3; 21) | 12 (2; 21) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noble, J.; Metzger, A.; Naciri Bennani, H.; Daligault, M.; Masson, D.; Terrec, F.; Imerzoukene, F.; Bardy, B.; Fiard, G.; Marlu, R.; et al. Apheresis Efficacy and Tolerance in the Setting of HLA-Incompatible Kidney Transplantation. J. Clin. Med. 2021, 10, 1316. https://doi.org/10.3390/jcm10061316
Noble J, Metzger A, Naciri Bennani H, Daligault M, Masson D, Terrec F, Imerzoukene F, Bardy B, Fiard G, Marlu R, et al. Apheresis Efficacy and Tolerance in the Setting of HLA-Incompatible Kidney Transplantation. Journal of Clinical Medicine. 2021; 10(6):1316. https://doi.org/10.3390/jcm10061316
Chicago/Turabian StyleNoble, Johan, Antoine Metzger, Hamza Naciri Bennani, Melanie Daligault, Dominique Masson, Florian Terrec, Farida Imerzoukene, Beatrice Bardy, Gaelle Fiard, Raphael Marlu, and et al. 2021. "Apheresis Efficacy and Tolerance in the Setting of HLA-Incompatible Kidney Transplantation" Journal of Clinical Medicine 10, no. 6: 1316. https://doi.org/10.3390/jcm10061316
APA StyleNoble, J., Metzger, A., Naciri Bennani, H., Daligault, M., Masson, D., Terrec, F., Imerzoukene, F., Bardy, B., Fiard, G., Marlu, R., Chevallier, E., Janbon, B., Malvezzi, P., Rostaing, L., & Jouve, T. (2021). Apheresis Efficacy and Tolerance in the Setting of HLA-Incompatible Kidney Transplantation. Journal of Clinical Medicine, 10(6), 1316. https://doi.org/10.3390/jcm10061316