
Mental Health and Perceived Access to Care among People Who Inject Drugs in Athens, Greece

 ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
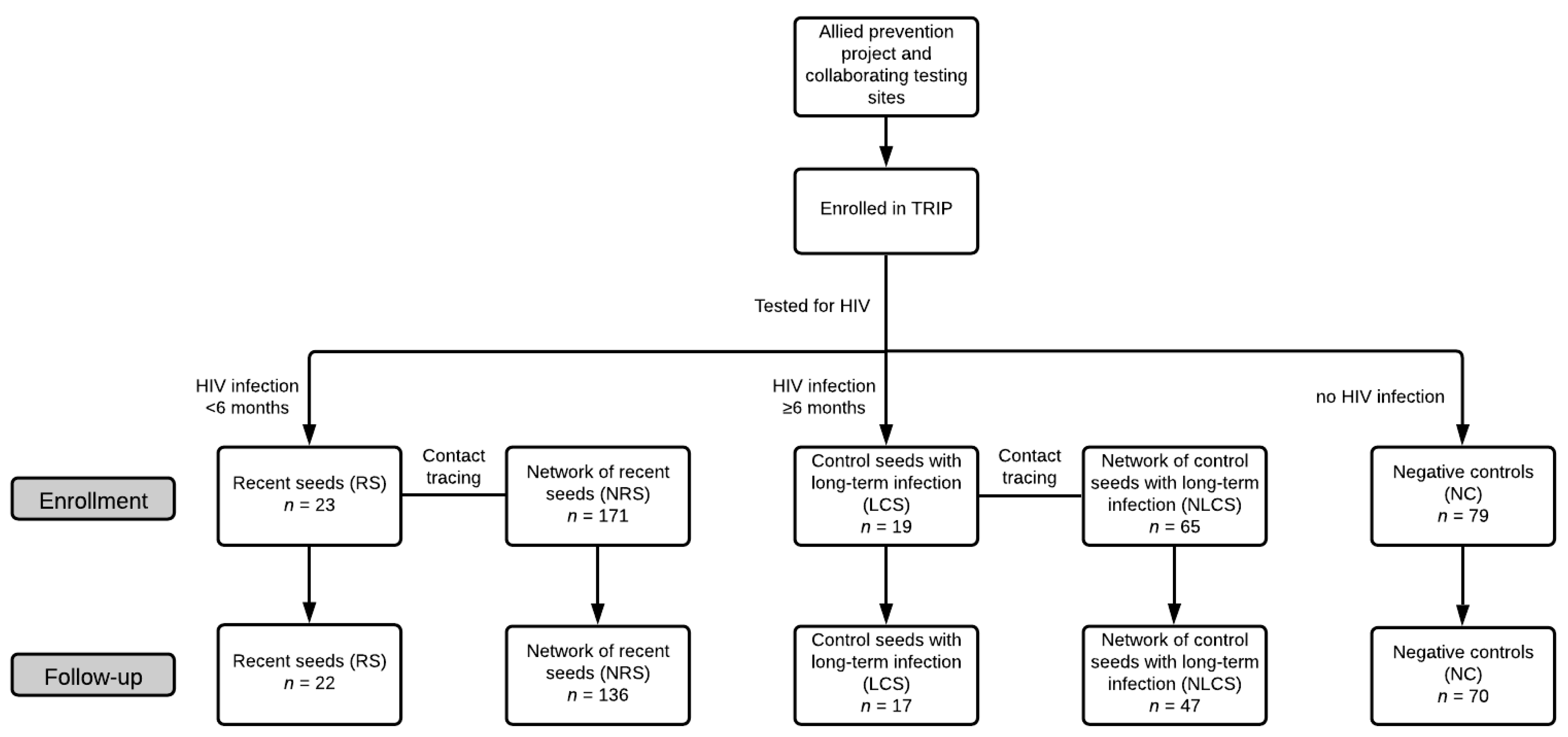
2.2. Participants
2.3. Questionnaire and Measures
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Mental Health
3.3. HIV-Related (for Recent Infection) Stigma and Social Support
3.4. Perceived Access to Care
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colledge, S.; Larney, S.; Peacock, A.; Leung, J.; Hickman, M.; Grebely, J.; Farrell, M.; Degenhardt, L. Depression, post-traumatic stress disorder, suicidality and self-harm among people who inject drugs: A systematic review and meta-analysis. Drug Alcohol. Depend. 2020, 207, 107793. [Google Scholar] [CrossRef]
- Remien, R.H.; Stirratt, M.J.; Nguyen, N.; Robbins, R.N.; Pala, A.N.; Mellins, C.A. Mental health and HIV/AIDS: The need for an integrated response. Aids 2019, 33, 1411–1420. [Google Scholar] [CrossRef]
- Abayomi, O.; Adelufosi, A.; Adebayo, P.; Ighoroje, M.; Ajogbon, D.; Ogunwale, A. HIV risk behavior in persons with severe mental disorders in a psychiatric hospital in Ogun, Nigeria. Ann. Med. Health Sci. Res. 2013, 3, 380–384. [Google Scholar] [CrossRef]
- Bing, E.G.; Burnam, M.A.; Longshore, D.; Fleishman, J.A.; Sherbourne, C.D.; London, A.S.; Turner, B.J.; Eggan, F.; Beckman, R.; Vitiello, B.; et al. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch. Gen. Psychiatry 2001, 58, 721–728. [Google Scholar] [CrossRef]
- National Institute of Mental Health. HIV/AIDS and Mental Health. Available online: https://www.nimh.nih.gov/health/topics/hiv-aids/index.shtml (accessed on 1 December 2020).
- Bhatia, R.; Giordano, T.P. Persons Newly Diagnosed with HIV Infection are at High Risk for Depression and Poor Linkage to Care: Results from the Steps Study. AIDS Behav. 2011, 15, 1161–1170. [Google Scholar] [CrossRef]
- Prasithsirikul, W.; Chongthawonsatid, S.; Ohata, P.J.; Keadpudsa, S.; Klinbuayaem, V.; Rerksirikul, P.; Stephen, J.; Ruxrungtham, K.; Ananworanich, J.; Avihingsanon, A. Depression and anxiety were low amongst virally suppressed, long-term treated HIV- infected individuals enrolled in a public sector antiretroviral program in Thailand. AIDS Care 2017, 29, 299–305. [Google Scholar] [CrossRef]
- Chen, M.H.; Su, T.P.; Chen, T.J.; Cheng, J.Y.; Wei, H.T.; Bai, Y.M. Identification of psychiatric disorders among human immunodeficiency virus-infected individuals in Taiwan, a nine-year nationwide population-based study. AIDS Care 2012, 24, 1543–1549. [Google Scholar] [CrossRef]
- Leserman, J. Role of Depression, Stress, and Trauma in HIV Disease Progression. Psychosom. Med. 2008, 70, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Nel, A.; Kagee, A. The relationship between depression, anxiety and medication adherence among patients receiving antiretroviral treatment in South Africa. AIDS Care Psychol. Socio-Med. Asp. AIDS/HIV 2013, 25, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Gutmann, M.; Andrew, F. Mental Health and HIV/AIDS; USAID’s AIDS Support and Technical Assistance Resources, AIDSTAR-One, Task Order 1: Arlington, VA, USA, 2009. [Google Scholar]
- Alfonso, V.; Geller, J.; Bermbach, N.; Drummond, A.; Montaner, J.S.G. Becoming a “treatment success”: What helps and what hinders patients from achieving and sustaining undetectable viral loads. AIDS Patient Care STDS 2006, 20, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Nyblade, L.; MacQuarrie, K. Can We Measure HIV/AIDS-Related Stigma and Discrimination? Current Knowledge about Quantifying Stigma in Developing Countries. 2006. Available online: https://www.icrw.org/publications/can-we-measure-hivaids-related-stigma-and-discrimination/ (accessed on 22 February 2021).
- Spicer, N.; Bogdan, D.; Brugha, R.; Harmer, A.; Murzalieva, G.; Semigina, T. ’It’ s risky to walk in the city with syringes’: Understanding access to HIV / AIDS services for injecting drug users in the former Soviet Union countries of Ukraine and Kyrgyzstan. Glob. Health 2011, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Terlikbayeva, A.; Zhussupov, B.; Primbetova, S.; Gilbert, L.; Atabekov, N.; Giyasova, G.; Ruziev, M.; Soliev, A.; Saliev, D.; El-Bassel, N. Access to HIV counseling and testing among people who inject drugs in Central Asia: Strategies for improving access and linkages to treatment and care. Drug Alcohol. Depend. 2013, 132, S61–S64. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. HIV Treatment as Prevention. Available online: https://www.cdc.gov/hiv/risk/art/index.html (accessed on 1 December 2020).
- Rodger, A.J.; Cambiano, V.; Phillips, A.N.; Bruun, T.; Raben, D.; Lundgren, J.; Vernazza, P.; Collins, S.; Degen, O.; Corbelli, G.M.; et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): Final results of a multicentre, prospective, observational study. Lancet 2019, 393, 2428–2438. [Google Scholar] [CrossRef]
- Frasquilho, D.; Matos, M.G.; Salonna, F.; Guerreiro, D.; Storti, C.C.; Gaspar, T.; Caldas-de-almeida, J.M. Mental health outcomes in times of economic recession: A systematic literature review. BMC Public Health 2016, 16, 115. [Google Scholar] [CrossRef]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; MacKenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Nikolopoulos, G.K.; Sypsa, V.; Bonovas, S.; Paraskevis, D.; Malliori-Minerva, M.; Hatzakis, A.; Friedman, S.R. Big Events in Greece and HIV Infection among People Who Inject Drugs. Subst. Use Misuse 2015, 50, 825–838. [Google Scholar] [CrossRef]
- Paraskevis, D.; Nikolopoulos, G.; Fotiou, A.; Tsiara, C.; Paraskeva, D.; Sypsa, V.; Lazanas, M.; Gargalianos, P.; Psichogiou, M.; Skoutelis, A.; et al. Economic recession and emergence of an HIV-1 outbreak among drug injectors in Athens metropolitan area: A longitudinal study. PLoS ONE 2013, 8, e78941. [Google Scholar] [CrossRef] [PubMed]
- Nikolopoulos, G.; Pavlitina, E.; Muth, S.S.Q.; Schneider, J.; Psichogiou, M.; Williams, L.L.D.; Paraskevis, D.; Sypsa, V.; Magiorkinis, G.; Smyrnov, P.; et al. A network intervention that locates and intervenes with recently HIV-infected persons: The Transmission Reduction Intervention Project (TRIP). Sci. Rep. 2016, 6, 38100. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.R.; Downing, M.J.; Smyrnov, P.; Nikolopoulos, G.; Schneider, J.A.; Livak, B.; Magiorkinis, G.; Slobodianyk, L.; Vasylyeva, T.I.; Paraskevis, D.; et al. Socially-Integrated Transdisciplinary HIV Prevention. AIDS Behav. 2014, 18, 1821–1834. [Google Scholar] [CrossRef] [PubMed]
- Psichogiou, M.; Giallouros, G.; Pantavou, K.; Pavlitina, E.; Papadopoulou, M.; Williams, L.D.; Hadjikou, A.; Kakalou, E.; Skoutelis, A.; Protopapas, K.; et al. Identifying, linking, and treating people who inject drugs and were recently infected with HIV in the context of a network-based intervention. AIDS Care 2019, 31, 1376–1383. [Google Scholar] [CrossRef]
- Hatzakis, A.; Sypsa, V.; Paraskevis, D.; Nikolopoulos, G.; Tsiara, C.; Micha, K.; Panopoulos, A.; Malliori, M.; Psichogiou, M.; Pharris, A.; et al. Design and baseline findings of a large-scale rapid response to an HIV outbreak in people who inject drugs in Athens, Greece: The ARISTOTLE programme. Addiction 2015, 110, 1453–1467. [Google Scholar] [CrossRef]
- Veit, C.T.; Ware, J.E. The structure of psychological distress and well-being in general populations. J. Consult. Clin. Psychol. 1983, 51, 730–742. [Google Scholar] [CrossRef]
- Williams, L.D.; Korobchuk, A.; Pavlitina, E.; Nikolopoulos, G.K.; Skaathun, B.; Schneider, J.; Kostaki, E.G.; Smyrnov, P.; Vasylyeva, T.I.; Psichogiou, M.; et al. Experiences of stigma and support reported by participants in a network intervention to reduce HIV transmission in Athens, Greece; Odessa, Ukraine; and Chicago, Illinois. AIDS Behav. 2019, 23, 1210–1224. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, W.E.; Hays, R.D.; Williams, K.W.; Beck, K.C.; Dixon, W.J.; Shapiro, M.F. Access to medical care and health-related quality of life for low-income persons with symptomatic human immunodeficiency virus. Med. Care 1995, 33, 739–754. [Google Scholar] [CrossRef] [PubMed]
- Morrison, M.F.; Petitto, J.M.; Ten Have, T.; Gettes, D.R.; Chiappini, M.S.; Weber, A.L.; Brinker-Spence, P.; Bauer, R.M.; Douglas, S.D.; Evans, D.L. Depressive and anxiety disorders in women with HIV infection. Am. J. Psychiatry 2002, 159, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Schadé, A.; van Grootheest, G.; Smit, J.H. HIV-infected mental health patients: Characteristics and comparison with HIV-infected patients from the general population and non-infected mental health patients. BMC Psychiatry 2013, 13, 35. [Google Scholar] [CrossRef]
- Arseniou, S.; Arvaniti, A.; Samakouri, M. HIV infection and depression. Psychiatry Clin. Neurosci. 2014, 68, 96–109. [Google Scholar] [CrossRef]
- Ciesla, J.A.; Roberts, J.E. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am. J. Psychiatry 2001, 158, 725–730. [Google Scholar] [CrossRef]
- Li, Y.; Hershow, R.; Irwanto, I.P.; Setiawan, M.; Levy, J. Factors Associated with Symptoms of Depression among Injection Drug Users Receiving Antiretroviral Treatment in Indonesia. J. AIDS Clin. Res. 2014, 5, 1–15. [Google Scholar] [CrossRef]
- Benoit, A.C.; Light, L.; Burchell, A.N.; Gardner, S.; Rourke, S.B. Demographic and clinical factors correlating with high levels of psychological distress in HIV-positive women living in Ontario, Canada. AIDS Care 2014, 26, 37–41. [Google Scholar] [CrossRef]
- Dombrowski, J.C.; Simoni, J.M.; Katz, D.A.; Golden, M.R. Barriers to HIV Care and Treatment Among Participants in a Public Health HIV Care Relinkage Program. AIDS Patient Care STDS 2015, 29, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, D.; Taket, A.; Smith, P. Action research in health promotion. Health Educ. J. 2003, 62, 5–22. [Google Scholar] [CrossRef]
- Santos, A.M.S.; Novo, R.F. Mental Health Inventory: Sensitivity and Specificity of the Portuguese Version of the MHI-38 and MHI-5. Psychol. Rep. 2020, 123, 1452–1469. [Google Scholar] [CrossRef]
- Australian Mental Health Outcomes and Classification Network. In Mental Health Inventory Training Manual; NSW Institute of Psychiatry: Sydney, Australia, 2005; pp. 1–21.
- Gholizadeh Shamasbi, S.; Barkin, J.L.; Ghanbari-Homayi, S.; Eyvazzadeh, O.; Mirghafourvand, M. The Relationship between Maternal Functioning and Mental Health after Childbirth in Iranian Women. Int. J. Environ. Res. Public Health 2020, 17, 1558. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Socio-Demographic Characteristics | Participant Group | ||||||
|---|---|---|---|---|---|---|---|
| Total | RS | NRS | LCS | NLCS | NC | ||
| Total | 292 | 22 (7.5%) | 136 (46.6%) | 17 (5.8%) | 47 (16.1%) | 70 (24.0%) | |
| Sex | Males | 231 (79.1%) | 17 (77.3%) | 106 (77.9%) | 14 (82.4%) | 37 (78.7%) | 57 (81.4%) |
| Females | 61 (20.9%) | 5 (22.7%) | 30 (22.1%) | 3 (4.9%) | 10 (21.3%) | 13 (18.6%) | |
| Age [years, median (interquartile range)] | 35 (31–41) | 39.5 (31–44) | 35 (30–39) | 36 (32–40) | 34 (31–37) | 36 (32–45) | |
| Nationality | Greek | 269 (92.1) | 20 (90.9%) | 123 (90.4%) | 15 (88.2%) | 42 (89.4%) | 69 (98.6%) |
| Non-Greek | 23 (7.9%) | 2 (9.1%) | 13 (9.6%) | 2 (11.8%) | 5 (10.6%) | 1 (1.4%) | |
| Permanent residence | Locals (living in Athens since birth) | 169 (57.9%) | 12 (54.6%) | 76 (55.9%) | 10 (58.8%) | 22 (46.8%) | 49 (70%) |
| Non-locals | 123 (42.1%) | 10 (45.4%) | 60 (44.1%). | 7 (41.2%) | 25 (53.2%) | 21 (30.0%) | |
| Education | Up to high school | 250 (85.6%) | 19 (86.4%) | 115 (84.6%) | 15 (88.2%) | 39 (83.0%) | 62 (88.6%) |
| Post-high school | 42 (14.4%) | 3 (13.6%) | 21 (15.4%) | 2 (11.8%) | 8 (11.4%) | 8 (11.4%) | |
| Homelessness | Homeless | 39 (13.4%) | 2 (9.1%) | 24 (17.8%) | 2 (11.8%) | 9 (19.2%) | 2 (2.9%) |
| Non-homeless | 252 (86.6%) | 20 (90.9%) | 111 (82.2%) | 15 (88.2%) | 38 (80.9%) | 68 (97.1%) | |
| Employment | Unemployed/unable to work | 232 (79.4%) | 19 (86.4%) | 113 (83.1%) | 15 (88.2%) | 35 (74.5%) | 50 (71.4%) |
| Employed | 60 (20.6%) | 3 (13.6%) | 23 (16.9%) | 2 (77.8%) | 12 (25.5%) | 20 (28.6%) | |
| Injected drugs (past 6 months) | Injected drugs | 211 (72.3%) | 18 (81.8%) | 107 (78.7%) | 13 (76.5%) | 38 (80.9%) | 35 (50.0%) |
| Non-injected drugs | 81 (27.7%) | 4 (18.2%) | 29 (21.3%) | 4 (23.5%) | 9 (19.1%) | 35 (50.0%) | |
| Duration of drug injection [years, median (interquartile range)] | 14 (8–18) | 13.5 (4–19) | 13 (7–18) | 12 (7–16) | 13.5 (8–15.5) | 15 (9–21) | |
| Drug/alcohol treatment at enrollment | On treatment | 156 (53.4%) | 15 (68.2%) | 68 (50%) | 12 (70.6%) | 19 (40.4%) | 42 (60.0%) |
| Without treatment | 136 (46.9%) | 7 (31.8%) | 68 (50%) | 5 (29.4%) | 28 (59.6%) | 28 (40%) | |
| Sexual orientation | Heterosexuals | 284 (97.3%) | 21 (95.5%) | 133 (97.8%) | 16 (94.1%) | 46 (97.9%) | 68 (97.1%) |
| Non-heterosexuals | 8 (2.7%) | 1 (4.5%) | 3 (2.2%) | 1 (5.9%) | 1 (2.1%) | 2 (2.9%) | |
| Socio-Demographic Characteristics | HIV Status | ||
|---|---|---|---|
| Positive | Negative | ||
| Total | 122 | 170 | |
| Sex | Males | 94 (77.1%) | 137 (80.6%) |
| Females | 28 (22.9%) | 33 (19.4%) | |
| Age [years, median (interquartile range)] | 34 (30–40) | 35 (32–41) | |
| Nationality | Greek | 108 (88.5%) | 161 (94.7%) |
| Non-Greek | 14 (11.5%) | 9 (5.3%) | |
| Permanent residence | Local (living in Athens since birth) | 64 (52.5%) | 105 (61.8%) |
| Non-locals | 58 (47.5%) | 65 (38.2%) | |
| Education | Up to high school | 107 (87.7%) | 143 (84.1%) |
| Post-high school | 15 (12.3%) | 27 (15.9%) | |
| Homelessness | Homeless | 23 (19.0%) | 16 (9.4%) |
| Non-homeless | 98 (81%) | 154 (90.6%) | |
| Employment | Unemployed/unable to work | 106 (86.9%) | 126 (74.1%) |
| Employed | 16 (13.1%) | 44 (25.9%) | |
| Injected drugs (past 6 months) | Injected drugs | 108 (88.5%) | 103 (60.6%) |
| Did not inject drugs | 14 (11.5%) | 67 (39.4%) | |
| Duration of drug injection [years, median (Interquartile Range)] | 13.5 (8–18) | 14 (8–19) | |
| Drug/alcohol treatment at enrollment | On treatment | 72 (59.0%) | 84 (49.4%) |
| Without treatment | 50 (41.0%) | 86 (50.6%) | |
| Sexual orientation | Heterosexuals | 117 (95.9%) | 167 (98.2%) |
| Non-heterosexuals | 5 (4.1%) | 3 (1.8%) | |
| Mental Health Subscales | Subscale Range | Participant Group [Mean, (sd)] | HIV Status [Mean, (sd)] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | RS | NRS | LCS | NLCS | NC | Positive | Negative | ||
| Depression (n = 290) | 4 to 23 | 14.1 (4.4) | 12.8 (3.8) | 13.9 (4.4) | 13.6 (4.6) | 14.6 (4.3) | 14.5 (4.5) | 13.9 (4.4) | 14.2 (4.4) |
| Anxiety (n = 290) | 9 to 54 | 32.5 (8.8) | 31.9 (7.6) | 31.7 (8.7) | 29.4 (7.9) | 33.9 (8.7) | 34.0 (9.2) | 31.9 (8.6) | 32.9 (8.9) |
| General Positive Affect (n = 288) | 10 to 60 | 28.6 (10.0) | 30.2 (10.8) | 29.4 (9.9) | 30.8 (10.8) | 26.3 (9.4) | 27.8 (10.3) | 28.7 (10.2) | 28.6 (10.0) |
| A | Mental Health Subscales | |||
|---|---|---|---|---|
| Socio-Demographic Characteristics | Depression | Anxiety | General Positive Affect | |
| Sex (males vs. females) | 0.27 (−0.97, 1.52) | −1.62 (−4.11, 0.86) | −0.05 (−2.91, 2.80) | |
| Age | 0.02 (−0.04, 0.08) | −0.09 (−0.21, 0.04) | −0.01 (−0.16, 0.13) | |
| Nationality (Greek vs. non-Greek) | 0.42 (−1.49, 2.33) | 1.99 (−1.84, 5.81) | 1.47 (−3.02, 5.95) | |
| Permanent residence (locals vs. non-locals) | 0.09 (−0.94, 1.12) | 1.15 (−0.90, 3.21) | 0.69 (−1.67,3.06) | |
| Education (up to high school vs. post-high school) | −0.56 (−2.00, 0.88) | −0.31 (−3.20, 2.57) | 0.21 (−3.58, 3.17) | |
| Homelessness (homeless vs. non-homeless) | 0.87 (−0.63, 2.37) | −0.79 (−3.80, 2.22) | −3.03 (−6.46, 0.39) | |
| Employment (unemployed/unable to work vs. employed) | 1.49 (0.24, 2.74) | 0.08 (−2.44, 2.60) | −1.29 (−4.18, 1.59) | |
| Injected drugs (injected vs. did not inject drugs)(past 6 months) | 0.75 (−0.38, 1.87) | 0.64 (−1.62, 2.90) | −3.21 (−5.77, −0.64) | |
| Duration of drug injection | 0.06 (−0.00, 0.13) | 0.04 (−0.09, 0.18) | −0.06 (−0.21, 0.09) | |
| Drug/alcohol treatment at enrolment (on treatment vs. without treatment) | 0.88 (−0.13, 1.89) | 0.38 (−1.65, 2.41) | −1.25 (−3.59, 1.08) | |
| Sexual orientation (heterosexuals vs. non-heterosexuals) | 0.20 (−2.89, 3.29) | −3.50 (−9.68, 2.69) | −1.39 (−8.49, 5.70) | |
| HIV status (HIV-positive vs. HIV-negative) | −0.29 (−1.32, 0.74) | −1.00 (−3.06, 1.05) | 0.13 (−2.25, 2.50) | |
| Participant group (vs. LCS) | RS | −0.87 (−3.66, 1.91) | 2.50 (−3.05, 8.04) | −0.57 (−7.05, 5.92) |
| NRS | 0.30 (−1.92, 2.52) | 2.24 (−2.18, 6.67) | −1.36 (−6.58, 3.86) | |
| NLCS | 0.91 (−1.53, 3.35) | 4.48 (−0.38, 9.34) | −4.40 (−10.13, 1.33) | |
| NC | 0.84 (−1.49, 3.17) | 4.59 (−0.06, 9.23) | −2.98 (−8.44, 2.49) | |
| B | ||||
| Mental Health Subscales | ||||
| Depression | - | 1.38 (1.21, 1.55) | −1.47 (−1.68, −1.27) | |
| Anxiety | - | - | −0.55 (−0.67, −0.43) | |
| General positive affect | - | - | - | |
| Crude β (95%CI) | Adjusted β (95%CI) | |||
|---|---|---|---|---|
| Socio-demographic characteristics | Sex (males vs. females) | −0.84 (−2.40, 0.72) | ||
| Age | −0.08 (−0.16, 0.00) | −0.05 (−0.12, 0.03) | ||
| Nationality (Greek vs. non-Greek) | 1.59 (−0.81, 3.99) | |||
| Permanent residence (locals vs. non-locals) | 0.53 (−0.77, 1.84) | |||
| Education (up to high school vs. post-high school) | 0.40 (−1.40, 2.20) | |||
| Homelessness (homeless vs. non-homeless) | −1.41 (−2.44, 1.13) | |||
| Employment (unemployed/unable to work vs employed) | −0.62 (−2.23,0.99) | |||
| Injected drugs (injected vs. did not inject drugs—past 6 months) | −0.27 (−1.70, 1.16) | |||
| Duration of drug injection | −0.02 (−0.11, 0.06) | |||
| Drug/alcohol treatment at enrolment (on treatment vs. without treatment) | 0.80 (−0.49, 2.09) | |||
| Sexual orientation (heterosexuals vs. non-heterosexual) | −2.00 (−5.80, 1.80) | |||
| HIV status (HIV-positive vs. HIV-negative) | 1.49 (0.19, 2.79) | 1.32 (0.11, 2.54) | ||
| Participant group (vs. LCS) | RS | 1.19 (−2.39, 4.77) | ||
| NRS | −0.04 (−2.93, 2.85) | |||
| NLCS | 1.57 (−1.63, 4.76) | |||
| NC | −0.33 (−3.36, 2.70) | |||
| Measures | Mental health (self-reported) | Depression | −0.29 (−0.44, −0.14) | −0.22 (−0.43, 0.00) |
| Anxiety | −0.14 (−0.21, −0.06) | −0.06 (−0.16, 0.03) | ||
| General positive affect | 0.08 (0.01, 0.14) | 0.49 (−0.10, 0.05) | ||
| Stigma and support | HIV-related stigma | −0.47 (−1.33, 0.38) | ||
| HIV-related social support | 0.73 (−0.00, 1.47) | |||
| Perceived access to care at baseline | 0.34 (0.23, 0.45) | 0.33 (0.22, 0.43) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pampaka, D.; Pantavou, K.; Giallouros, G.; Pavlitina, E.; Williams, L.D.; Piovani, D.; Bonovas, S.; Nikolopoulos, G.K. Mental Health and Perceived Access to Care among People Who Inject Drugs in Athens, Greece. J. Clin. Med. 2021, 10, 1181. https://doi.org/10.3390/jcm10061181
Pampaka D, Pantavou K, Giallouros G, Pavlitina E, Williams LD, Piovani D, Bonovas S, Nikolopoulos GK. Mental Health and Perceived Access to Care among People Who Inject Drugs in Athens, Greece. Journal of Clinical Medicine. 2021; 10(6):1181. https://doi.org/10.3390/jcm10061181
Chicago/Turabian StylePampaka, Despina, Katerina Pantavou, George Giallouros, Eirini Pavlitina, Leslie D. Williams, Daniele Piovani, Stefanos Bonovas, and Georgios K. Nikolopoulos. 2021. "Mental Health and Perceived Access to Care among People Who Inject Drugs in Athens, Greece" Journal of Clinical Medicine 10, no. 6: 1181. https://doi.org/10.3390/jcm10061181
APA StylePampaka, D., Pantavou, K., Giallouros, G., Pavlitina, E., Williams, L. D., Piovani, D., Bonovas, S., & Nikolopoulos, G. K. (2021). Mental Health and Perceived Access to Care among People Who Inject Drugs in Athens, Greece. Journal of Clinical Medicine, 10(6), 1181. https://doi.org/10.3390/jcm10061181