
SARS-CoV-2 Infection: Modulator of Pulmonary Embolism Paradigm

 , and
, and 
Abstract
1. Introduction
2. Incidence
3. Risk Factors
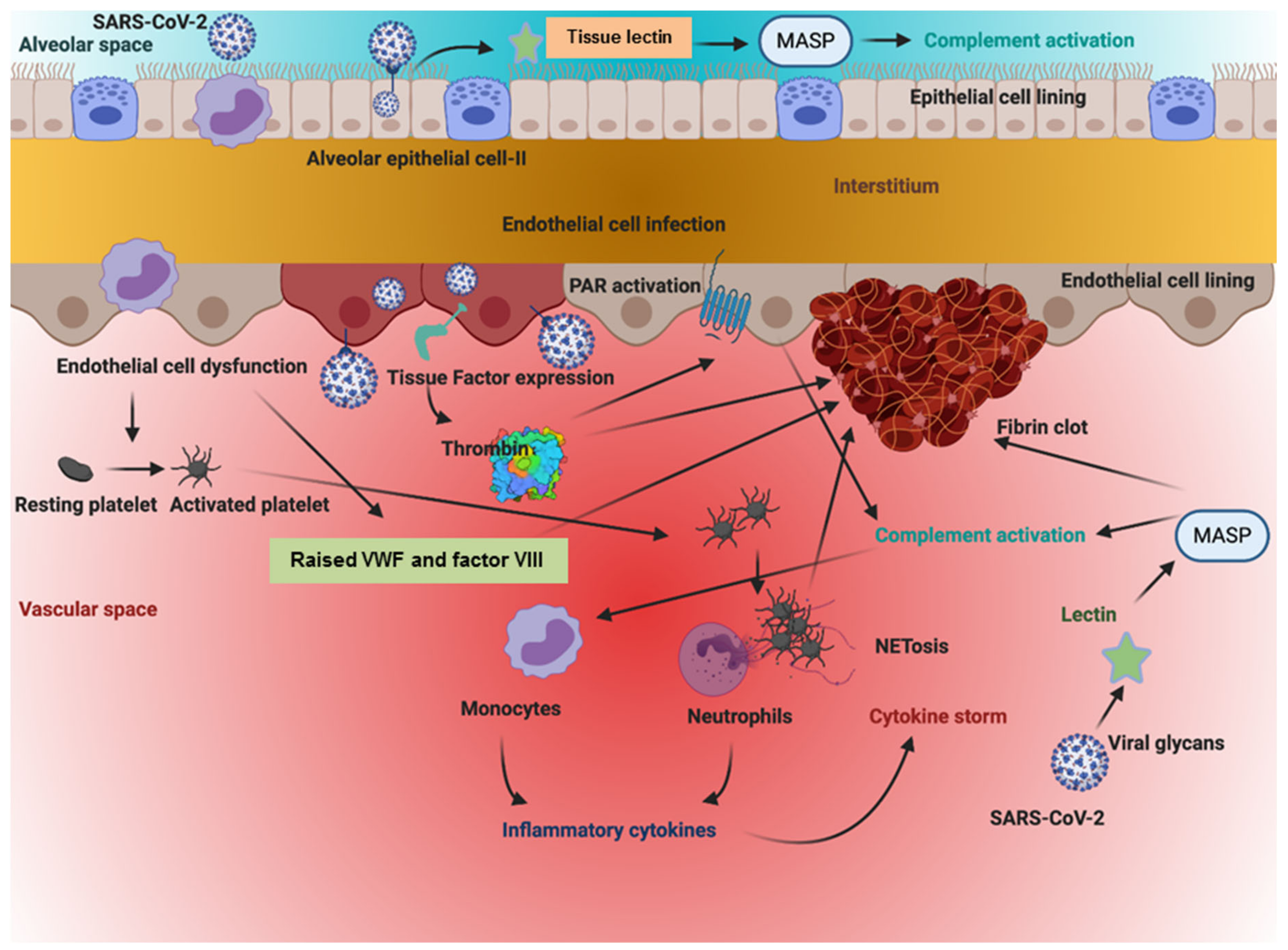
4. Virus-Inflected Pathophysiology
5. Diagnosis
6. Prophylactic and Therapeutic Interventions
7. Post-COVID-19 Thromboprophylaxis
8. Mortality
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Worku, B.; Gulkarov, I.; Girardi, L.N.; Salemi, A. Pulmonary embolectomy in the treatment of submassive and massive pulmonary embolism. Cardiology 2014, 129, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Giordano, N.J.; Jansson, P.S.; Young, M.N.; Hagan, K.A.; Kabrhel, C. Epidemiology, Pathophysiology, Stratification, and Natural History of Pulmonary Embolism. Tech. Vasc. Interv. Radiol. 2017, 20, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Essien, E.O.; Rali, P.; Mathai, S.C. Pulmonary Embolism. Med. Clin. N. Am. 2019, 103, 549–564. [Google Scholar] [CrossRef] [PubMed]
- Grimnes, G.; Isaksen, T.; Tichelaar, Y.I.G.V.; Braekkan, S.K.; Hansen, J.-B. Acute infection as a trigger for incident venous thromboembolism: Results from a population-based case-crossover study. Res. Pr. Thromb. Haemost. 2018, 2, 85–92. [Google Scholar] [CrossRef]
- Matthews, J.C.; McLaughlin, V. Acute right ventricular failure in the setting of acute pulmonary embolism or chronic pulmonary hypertension: A detailed review of the pathophysiology, diagnosis, and management. Curr. Cardiol. Rev. 2008, 4, 49–59. [Google Scholar] [CrossRef]
- Astuti, I.; Ysrafil. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response. Diabetes Metab. Syndr. 2020, 14, 407–412. [Google Scholar] [CrossRef]
- Kashani, K.B. Hypoxia in COVID-19: Sign of Severity or Cause for Poor Outcomes. Mayo Clin. Proc. 2020, 95, 1094–1096. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef]
- Lorenzo, C.; Francesca, B.; Francesco, P.; Elena, C.; Luca, S.; Paolo, S. Acutepulmonary embolism in COVID-19 related hypercoagulability. J. Thromb. Thrombolysis 2020, 50, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.C.; Xue, J.; Sharma, A. Pulmonary Embolism: Epidemiology, Patient Presentation, Diagnosis, and Treatment. J. Radiol. Nurs. 2019, 38, 112–118. [Google Scholar] [CrossRef]
- Turetz, M.; Sideris, A.T.; Friedman, O.A.; Triphathi, N.; Horowitz, J.M. Epidemiology, Pathophysiology, and Natural History of Pulmonary Embolism. Semin. Interv. Radiol. 2018, 35, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Incidence of Pulmonary Embolism in ED Patients During the COVID-19 Pandemic. Available online: https://www.jwatch.org/na52640/2020/10/14/incidence-pulmonary-embolism-ed-patients-during-covid-19 (accessed on 11 December 2020).
- Roncon, L.; Zuin, M.; Barco, S.; Valerio, L.; Zuliani, G.; Zonzin, P.; Konstantinides, S.V. Incidence of acute pulmonary embolism in COVID-19 patients: Systematic review and meta-analysis. Eur. J. Intern. Med. 2020, 17, S0953–S6205. [Google Scholar]
- COVID-19. Available online: https://www.hematology.org/covid (accessed on 12 October 2020).
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. 2020, 26, 107602962093814. [Google Scholar] [CrossRef]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary Embolism in Patients With COVID-19. Circ. 2020, 142, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Hauguel-Moreau, M.; El Hajjam, M.; De Baynast, Q.; Vieillard-Baron, A.; Lot, A.-S.; Chinet, T.; Mustafic, H.; Bégué, C.; Carlier, R.Y.; Geri, G.; et al. Occurrence of pulmonary embolism related to COVID-19. J. Thromb. Thrombolysis 2020, 6, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bompard, F.; Monnier, H.; Saab, I.; Tordjman, M.; Abdoul, H.; Fournier, L.; Sanchez, O.; Lorut, C.; Chassagnon, G.; Revel, M.P. Pulmonary embolism in patients with COVID-19pneumonia. Eur. Respir J. 2020, 30, 2001365. [Google Scholar] [CrossRef] [PubMed]
- Mestre-Gómez, B.; Lorente-Ramos, R.M.; Rogado, J.; Franco-Moreno, A.; Obispo, B.; Salazar-Chiriboga, D.; Saez-Vaquero, T.; Torres-Macho, J.; Abad-Motos, A.; Cortina-Camarero, C.; et al. Infanta Leonor Thrombosis Research Group. Incidence of pulmonary embolism in non-critically ill COVID-19 patients. Predicting factors for a challenging diagnosis. J. Thromb. Thrombolysis 2020, 29, 1–7. [Google Scholar]
- Benito, N.; Filella, D.; Mateo, J.; Fortuna, A.M.; Gutierrez-Alliende, J.E.; Hernandez, N.; Gimenez, A.M.; Pomar, V.; Castellvi, I.; Corominas, H.; et al. Pulmonary Thrombosis or Embolism in a Large Cohort of Hospitalized Patients with Covid-19. Front. Med. 2020, 7, 557. [Google Scholar] [CrossRef]
- Liao, S.-C.; Shao, S.-C.; Chen, Y.-T.; Chen, Y.-C.; Hung, M.-J. Incidence and mortality of pulmonary embolism in COVID-19: A systematic review and meta-analysis. Crit. Care 2020, 24, 464. [Google Scholar] [CrossRef]
- Piroth, L.; Cottenet, J.; Mariet, A.-S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: A nationwide, population-based retrospective cohort study. Lancet Respir. Med. 2020, 17, 251–259. [Google Scholar]
- Jiménez, D.; García-Sanchez, A.; Rali, P.; Muriel, A.; Bikdeli, B.; Ruiz-Artacho, P.; Le Mao, R.; Rodríguez, C.; Hunt, B.J.; Monreal, M. Incidence of VTE and Bleeding Among Hospitalized Patients with Coronavirus Disease 2019. Chest 2020, 17, 1182–1196. [Google Scholar]
- Zhang, R.; Ni, L.; Di, X.; Wang, X.; Ma, B.; Niu, S.; Liu, C. Systematic review and meta-analysis of the prevalence of venous thromboembolic events in novel coronavirus disease-2019 patients. J. Vasc. Surgery Venous Lymphat. Disord. 2021, 9, 289–298. [Google Scholar]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.-P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 15, 203557. [Google Scholar]
- Abate, S.M.; Ali, S.A.; Mantfardo, B.; Basu, B. Rate of Intensive Care Unit admission and outcomes among patients with coronavirus: A systematic review and Meta-analysis. PLoS ONE 2020, 15, e0235653. [Google Scholar] [CrossRef]
- Boonyawat, K.; Chantrathammachart, P.; Numthavaj, P.; Nanthatanti, N.; Phusanti, S.; Phuphuakrat, A.; Niparuck, P.; Angchaisuksiri, P. Incidence of thromboembolism in patients with COVID-19: A systematic review and meta-analysis. Thromb. J. 2020, 23, 34. [Google Scholar] [CrossRef]
- Artifoni, M.; Danic, G.; Gautier, G.; Gicquel, P.; Boutoille, D.; Raffi, F.; Neel, A.; Lecomte, R. Systematic assessment of venous thromboembolism in COVID-19 patients receiving thromboprophylaxis: Incidence and role of D-dimer as predictive factors. J. Thromb. Thrombolysis 2020, 50, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.D.; Sacco, C.; Bertuzzi, A.; et al. Humanitas COVID-19 Task Force. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Grillet, F.; Behr, J.; Calame, P.; Aubry, S.; Delabrousse, E. Acute Pulmonary Embolism Associated with COVID-19 Pneumonia Detected with Pulmonary CT Angiography. Radiology 2020, 296, E186–E188. [Google Scholar] [CrossRef]
- Leonard-Lorant, I.; Delabranche, X.; Séverac, F.; Helms, J.; Pauzet, C.; Collange, O.; Schneider, F.; Labani, A.; Bilbault, P.; Molière, S.; et al. Acute Pulmonary Embolism in Patients with COVID-19 at CT Angiography and Relationship to d-Dimer Levels. Radiology 2020, 296, E189–E191. [Google Scholar] [CrossRef]
- Llitjos, J.; Leclerc, M.; Chochois, C.; Monsallier, J.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Thomas, W.; Varley, J.; Johnston, A.; Symington, E.; Robinson, M.; Sheares, K.; Lavinio, A.; Besser, M. Thrombotic complications of patients admitted to intensive care with COVID-19 at a teaching hospital in the United Kingdom. Thromb. Res. 2020, 191, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, S.; Coppens, M.; Van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severa, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Hékimian, G.; Lebreton, G.; Bréchot, N.; Luyt, C.-E.; Schmidt, M.; Combes, A. Severe pulmonary embolism in COVID-19 patients: A call for increased awareness. Crit. Care 2020, 24, 274. [Google Scholar] [CrossRef]
- Galeano-Valle, F.; Oblitas, C.M.; Ferreiro-Mazón, M.M.; Alonso-Muñoz, J.; Del Toro-Cervera, J.; di Natale, M.; Demelo-Rodríguez, P. Antiphospholipid antibodies are not elevated in patients with severe COVID-19 pneumonia and venous thromboembolism. Thromb. Res. 2020, 192, 113–115. [Google Scholar] [CrossRef]
- Soumagne, T.; Lascarrou, J.-B.; Hraiech, S.; Horlait, G.; Higny, J.; D’Hondt, A.; Grimaldi, D.; Gaudry, S.; Courcelle, R.; Carbutti, G.; et al. Factors Associated with Pulmonary Embolism Among Coronavirus Disease 2019 Acute Respiratory Distress Syndrome: A Multicenter Study Among 375 Patients. Crit. Care Explor. 2020, 2, e0166. [Google Scholar] [CrossRef]
- Fraissé, M.; Logre, E.; Pajot, O.; Mentec, H.; Plantefève, G.; Contou, D. Thrombotic and hemorrhagic events in critically ill COVID-19 patients: A French monocenter retrospective study. Crit. Care 2020, 2, 275. [Google Scholar] [CrossRef]
- Freund, Y.; Drogrey, M.; Miró, O.; Marra, A.; Féral-Pierssens, A.L.; Penaloza, A.; Hernandez, B.A.L.; Beaune, S.; Gorlicki, J.; Vaittinada, A.P.; et al. Improving emergency care fhu Collaborators. Association Between Pulmonary Embolism and COVID-19 in Emergency Department Patients Undergoing Computed Tomography Pulmonary Angiogram: The PEPCOV International Retrospective Study. Acad. Emerg. Med. 2020, 30, 811–820. [Google Scholar] [CrossRef]
- Chen, J.; Wang, X.; Zhang, S.; Lin, B.; Wu, X.; Wang, Y.; Wang, X.; Yang, M.; Sun, J.; Xie, Y. Characteristics of Acute Pulmonary Embolism in Patients With COVID-19 Associated Pneumonia from the City of Wuhan. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620936772. [Google Scholar] [CrossRef]
- Longchamp, A.; Longchamp, J.; Manzocchi-Besson, S.; Whiting, L.; Haller, C.; Jeanneret, S.; Godio, M.; Garcia Martinez, J.J.; Bonjour, T.; Caillat, M.; et al. Venous thromboembolism in critically Ill patients with COVID-19: Results of a screening study for deep vein thrombosis. Res. Pract. Thromb. Haemost. 2020, 30, 842–847. [Google Scholar] [CrossRef]
- Whyte, M.B.; Kelly, P.A.; Gonzalez, E.; Arya, R.; Roberts, L.N. Pulmonary embolism in hospitalised patients with COVID-19. Thromb. Res. 2020, 195, 95–99. [Google Scholar] [CrossRef]
- Marone, E.M.; Bonalumi, G.; Curci, R.; Arzini, A.; Chierico, S.; Marazzi, G.; Diaco, D.A.; Rossini, R.; Boschini, S.; Rinaldi, L.F. Characteristics of Venous Thromboembolism in COVID-19 Patients: A Multicenter Experience from Northern Italy. Ann. Vasc. Surg. 2020, 68, 83–87. [Google Scholar] [CrossRef]
- Fauvel, C.; Weizman, O.; Trimaille, A.; Mika, D.; Pommier, T.; Pace, N.; Douair, A.; Barbin, E.; Fraix, A.; Bouchot, O.; et al. Critical Covid-19 France Investigators. Pulmonary embolism in COVID-19patients: A French multicentre cohort study. Eur. Heart J. 2020, 41, 3058–3068. [Google Scholar] [CrossRef] [PubMed]
- Van den Heuvel, F.M.A.; Vos, J.L.; Koop, Y.; Van Dijk, A.P.J.; Duijnhouwer, A.L.; De Mast, Q.; Van De Veerdonk, F.L.; Bosch, F.; Kok, B.; Netea, M.G.; et al. Cardiac function in relation to myocardial injury in hospitalised patients with COVID-19. Neth. Hear. J. 2020, 28, 410–417. [Google Scholar] [CrossRef]
- Faggiano, P.; Bonelli, A.; Paris, S.; Milesi, G.; Bisegna, S.; Bernardi, N.; Curnis, A.; Agricola, E.; Maroldi, R. Acute pulmonary embolism in COVID-19 disease: Preliminary report on seven patients. Int. J. Cardiol. 2020, 313, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Gervaise, A.; Bouzad, C.; Peroux, E.; Helissey, C. Acute pulmonary embolism in non-hospitalized COVID-19 patients referred to CTPA by emergency department. Eur. Radiol. 2020, 30, 6170–6177. [Google Scholar] [CrossRef] [PubMed]
- Trimaille, A.; Curtiaud, A.; Marchandot, B.; Matsushita, K.; Sato, C.; Leonard-Lorant, I.; Sattler, L.; Grunebaum, L.; Ohana, M.; Von Hunolstein, J.-J.; et al. Venous thromboembolism in non-critically ill patients with COVID-19 infection. Thromb. Res. 2020, 193, 166–169. [Google Scholar] [CrossRef]
- News, Coronavirus: Covid-19 has Killed More People than SARS and MERS Combined, Despite Lower Case Fatality Rate. Available online: https://www.bmj.com/content/368/bmj.m641 (accessed on 15 January 2020).
- Martin, A.I.; Rao, G. COVID-19: A Potential Risk Factor for Acute Pulmonary Embolism. Methodist. Debakey Cardiovasc. J 2020, 16, 155–157. [Google Scholar]
- García-Ortega, A.; Oscullo, G.; Calvillo, P.; López-Reyes, R.; Méndez, R.; Gómez-Olivas, J.D.; Bekki, A.; Fonfría, C.; Trilles-Olaso, L.; Zaldívar, E.; et al. Incidence, risk factors, and thrombotic load of pulmonary embolism in patients hospitalized for COVID-19 infection. J. Infect. 2021, 82, 261–269. [Google Scholar] [CrossRef]
- Danzi, G.B.; Loffi, M.; Galeazzi, G.; Gherbesi, E. Acute pulmonary embolism and COVID-19 pneumonia: A random association? Eur. Hear. J. 2020, 41, 1858. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Cormier, P.; Patel, P.Y.; Hadied, M.O.; Bhargava, P.; Khanna, K.; Nadig, J.; Keimig, T.; Spizarny, D.; Reeser, N.; et al. Acute Pulmonary Embolism and COVID-19. Radiology 2020, 297, 201955. [Google Scholar] [CrossRef]
- Sanfilippo, F.; La Rosa, V.; Oliveri, F.; Astuto, M. Convalescent plasma for COVID-19: The risk of pulmonary embolism should not be underestimated! Crit. Care 2020, 28, 531. [Google Scholar] [CrossRef]
- Kowalewski, M.; Fina, D.; Słomka, A.; Raffa, G.M.; Martucci, G.; Coco, V.L.; De Piero, M.E.; Ranucci, M.; Suwalski, P.; Lorusso, R. COVID-19 and ECMO: The interplay between coagulation and inflammation—A narrative review. Crit. Care 2020, 24, 205. [Google Scholar] [CrossRef] [PubMed]
- Von Bahr, V.; E Millar, J.; Malfertheiner, M.V.; Ki, K.K.; Passmore, M.R.; Bartnikowski, N.; A Redd, M.; Cavaye, M.; Suen, J.Y.; McAuley, D.F.; et al. Mesenchymal stem cells may ameliorate inflammation in an ex vivo model of extracorporeal membrane oxygenation. Perfusion 2019, 34, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Riedel, M. Acute pulmonary embolism 1: Pathophysiology, clinical presentation, and diagnosis. Heart 2001, 85, 229–240. [Google Scholar] [CrossRef]
- Ciceri, F.; Castagna, A.; Rovere-Querini, P.; De Cobelli, F.; Ruggeri, A.; Galli, L.; Conte, C.; De Lorenzo, R.; Poli, A.; Ambrosio, A.; et al. Early predictors of clinical outcomes of COVID-19 outbreak in Milan, Italy. Clin. Immunol. 2020, 217, 108509. [Google Scholar] [CrossRef] [PubMed]
- Manne, B.K.; Denorme, F.; Middleton, E.A.; Portier, I.; Rowley, J.W.; Stubben, C.J.; Petrey, A.C.; Tolley, N.D.; Guo, L.; Cody, M.J.; et al. Platelet gene expression and function in patients with COVID-19. Blood 2020, 136, 1317–1329. [Google Scholar] [CrossRef]
- Teuwen, L.-A.; Geldhof, V.; Pasut, A.; Carmeliet, P. COVID-19: The vasculature unleashed. Nat. Rev. Immunol. 2020, 20, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.-H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Hottz, E.D.; Azevedo-Quintanilha, I.G.; Palhinha, L.; Teixeira, L.; Barreto, E.A.; Pão, C.R.R.; Righy, C.; Franco, S.; Souza, T.M.L.; Kurtz, P.; et al. Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19. Blood 2020, 136, 1330–1341. [Google Scholar] [CrossRef]
- Wang, J.; Li, Q.; Yin, Y.; Zhang, Y.; Cao, Y.; Lin, X.; Huang, L.; Hoffmann, D.; Lu, M.; Qiu, Y. Excessive Neutrophils and Neutrophil Extracellular Traps in COVID-19. Front. Immunol. 2020, 18, 2063. [Google Scholar] [CrossRef] [PubMed]
- Middleton, E.A.; He, X.Y.; Denorme, F.; Campbell, R.A.; Ng, D.; Salvatore, S.P.; Mostyka, M.; Baxter-Stoltzfus, A.; Borczuk, A.C.; Loda, M.; et al. Neutrophil extracellular traps contribute to immunothrombosis in COVID-19 acute respiratory distress syndrome. Blood 2020, 3, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Amraei, R.; Rahimi, N. COVID19, Renin-Angiotensin System and Endothelial Dysfunction. Cells 2020, 9, 1652. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 16, 271–280.e8. [Google Scholar] [CrossRef]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection. Eur. J. Intern. Med. 2020, 76, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Garvin, M.R.; Alvarez, C.; Miller, J.I.; Prates, E.T.; Walker, A.M.; Amos, B.K.; Mast, A.E.; Justice, A.; Aronow, B.; Jacobson, D.A. A mechanistic model and therapeutic interventions for COVID-19 involving a RAS-mediated bradykinin storm. eLife 2020, 9, e59177. [Google Scholar] [CrossRef] [PubMed]
- Schmaier, A.H. The contact activation and kallikrein/kinin systems: Pathophysiologic and physiologic activities. J. Thromb. Haemost. 2016, 14, 28–39. [Google Scholar] [CrossRef]
- Stavrou, E.X.; Fang, C.; Merkulova, A.; Alhalabi, O.; Grobe, N.; Antoniak, S.; Mackman, N.; Schmaier, A.H. Reduced thrombosis in Klkb1-/- mice is mediated by increased Mas receptor, prostacyclin, Sirt1, and KLF4 and decreased tissue factor. Blood 2015, 22, 710–719. [Google Scholar] [CrossRef]
- Sinha, P.; Matthay, M.A.; Calfee, C.S. Is a “Cytokine Storm” Relevant to COVID-19? JAMA Intern. Med. 2020, 1, 1152–1154. [Google Scholar] [CrossRef]
- Leisman, D.E.; Deutschman, C.S.; Legrand, M. Facing, COVID-19 in the ICU: Vascular dysfunction, thrombosis, and dysregulated inflammation. Intensive Care Med. 2020, 46, 1105–1108. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zucoloto, A.Z.; Jenne, C.N. Platelet-Neutrophil Interplay: Insights into Neutrophil Extracellular Trap (NET)-Driven Coagulation in Infection. Front Cardiovasc. Med. 2019, 20, 85. [Google Scholar] [CrossRef] [PubMed]
- Mancini, I.; Baronciani, L.; Artoni, A.; Colpani, P.; Biganzoli, M.; Cozzi, G.; Novembrino, C.; Anzoletti, M.B.; De Zan, V.; Pagliari, M.T.; et al. The ADAMTS13-von Willebrand factor axis in COVID-19 patients. J. Thromb. Haemost. 2021, 19. [Google Scholar] [CrossRef]
- Kyrle, P.A.; Minar, E.; Hirschl, M.; Bialonczyk, C.; Stain, M.; Schneider, B.; Weltermann, A.; Speiser, W.; Lechner, K.; Eichinger, S. High Plasma Levels of Factor VIII and the Risk of Recurrent Venous Thromboembolism. N. Engl. J. Med. 2000, 343, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, X.; Chen, J.; Cai, Y.; Deng, A.; Yang, M. Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br. J. Haematol. 2020, 190, 24–27. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, J.; Laffan, M.A. The relationship between ABO histo-blood group, factor VIII and von Willebrand factor. Transfus. Med. 2001, 11, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Palevsky, H.I. The problems of the clinical and laboratory diagnosis of pulmonary embolism. Semin. Nucl. Med. 1991, 21, 276–280. [Google Scholar] [CrossRef]
- Howard, L. Acute pulmonary embolism. Clin. Med. 2019, 19, 243–247. [Google Scholar] [CrossRef]
- Lavorini, F.; Di Bello, V.; De Rimini, M.L.; Lucignani, G.; Marconi, L.; Palareti, G.; Pesavento, R.; Prisco, D.; Santini, M.; Sverzellati, N.; et al. Diagnosis and treatment of pulmonary embolism: A multidisciplinary approach. Multidiscip. Respir Med. 2013, 19, 75. [Google Scholar] [CrossRef] [PubMed]
- Righini, M.; Robert-Ebadi, H. Diagnosis of acute Pulmonary Embolism. Hamostaseologie 2018, 38, 11–21. [Google Scholar] [CrossRef]
- Adams, E.; Broce, M.; Mousa, A. Proposed Algorithm for Treatment of Pulmonary Embolism in COVID-19 Patients. Ann. Vasc. Surg. 2021, 70, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Rosovsky, R.P.; Grodzin, C.; Channick, R.; Davis, G.A.; Giri, J.S.; Horowitz, J.; Kabrhel, C.; Lookstein, R.; Merli, G.; Morris, T.A.; et al. Diagnosis and Treatment of Pulmonary Embolism During the Coronavirus Disease 2019 Pandemic. Chest 2020, 158, 2590–2601. [Google Scholar] [CrossRef]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef]
- Parks, A.L.; Auerbach, A.D.; Schnipper, J.L.; Anstey, J.E.; Sterken, D.G.; Hecht, T.E.; Fang, M.C.; Vaughn, V.M.; Dunn, A.S.; Linker, A.S.; et al. COVID-19 coagulopathy and thrombosis: Analysis of hospital protocols in response to the rapidly evolving pandemic. Thromb. Res. 2020, 196, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Vidali, S.; Morosetti, D.; Cossu, E.; Luisi, M.L.E.; Pancani, S.; Semeraro, V.; Consales, G. D-dimer as an indicator of prognosis in SARS-CoV-2 infection: A systematic review. ERJ Open Res. 2020, 13, 260–2020. [Google Scholar] [CrossRef] [PubMed]
- Parry, A.H.; Wani, A.H. Pulmonary embolism in coronavirus disease-19 (COVID-19) and use of compression ultrasonography in its optimal management. Thromb. Res. 2020, 192, 36. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, B.; Zhou, J.; Kirkpatrick, J.; Xie, M.; Johri, A.M. Bedside Focused Cardiac Ultrasound in COVID-19 from the Wuhan Epicenter: The Role of Cardiac Point-of-Care Ultrasound, Limited Transthoracic Echocardiography, and Critical Care Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 676–682. [Google Scholar] [CrossRef]
- Dweck, M.R.; Bularga, A.; Hahn, R.T.; Bing, R.; Lee, K.K.; Chapman, A.R.; White, A.; Di Salvo, G.; Sade, L.E.; Pearce, K.; et al. Global evaluation of echocardiography in patients with COVID-19. Eur. Hear. J. Cardiovasc. Imaging 2020, 21, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Scudiero, F.; Silverio, A.; Di Maio, M.; Russo, V.; Citro, R.; Personeni, D.; Cafro, A.; D’Andrea, A.; Attena, E.; Pezzullo, S.; et al. Cov-IT Network. Pulmonary embolism in COVID-19 patients: Prevalence, predictors and clinical outcome. Thromb. Res. 2020, 17, 34–39. [Google Scholar]
- Kostadima, E.; Zakynthinos, E. Pulmonary embolism: Pathophysiology, diagnosis, treatment. Hell. J. Cardiol. 2007, 48, 94–107. [Google Scholar]
- A Systematic Approach for Managing Venous Thromboembolism in Patients with Covid-19. Available online: https://www.isth.org/news/517212 (accessed on 20 January 2020).
- Coppola, A.; Tagliaferri, A.; Rivolta, G.F.; Quintavalle, G.; Franchini, M. Confronting COVID-19: Issues in Hemophilia and Congenital Bleeding Disorders. Semin. Thromb. Hemost. 2020, 46, 819–822. [Google Scholar] [PubMed]
- ESC Guidance for the Diagnosis and Management of CV Disease during the COVID-19 Pandemic. Available online: https://www.escardio.org/Education/COVID-19-and-Cardiology/ESC-COVID-19-Guidance (accessed on 17 January 2021).
- Hosseini, A.; Bahramnezhad, F. Pulmonary embolism in patients with COVID-19 and its treatment based on low-molecular-weight heparin. Sao Paulo Med J. 2020, 138, 349–351. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Kipshidze, N.; Dangas, G.; White, C.J.; Kipshidze, N.; Siddiqui, F.; Lattimer, C.R.; Carter, C.A.; Fareed, J. Viral Coagulopathy in Patients With COVID-19: Treatment and Care. Clin. Appl. Thromb. 2020, 26, 1076029620936776. [Google Scholar] [CrossRef] [PubMed]
- Tersalvi, G.; Vicenzi, M.; Calabretta, D.; Biasco, L.; Pedrazzini, G.; Winterton, D. Elevated Troponin in Patients with Coronavirus Disease 2019: Possible Mechanisms. J. Card. Fail 2020, 26, 470–475. [Google Scholar] [CrossRef]
- Cohoon, K.P.; Mahé, G.; Tafur, A.J.; Spyropoulos, A.C. Emergence of institutional antithrombotic protocols for coronavirus 2019. Res. Pr. Thromb. Haemost. 2020, 4, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Riker, R.R.; May, T.L.; Fraser, G.L.; Gagnon, D.J.; Bandara, M.; Zemrak, W.R.; Seder, D.B. Heparin-induced thrombocytopenia with thrombosis in COVID-19 adult respiratory distress syndrome. Res. Pr. Thromb. Haemost. 2020, 4, 936–941. [Google Scholar] [CrossRef]
- Obi, A.T.; Barnes, G.D.; Wakefield, T.W.; Brown, S.; Eliason, J.L.; Arndt, E.; Henke, P.K. Practical diagnosis and treatment of suspected venous thromboembolism during COVID-19 pandemic. J. Vasc. Surgery: Venous Lymphat. Disord. 2020, 8, 526–534. [Google Scholar] [CrossRef]
- Tacquard, C.; Mansour, A.; Godon, A.; Godet, J.; Poissy, J.; Garrigue, D.; Kipnis, E.; Hamada, S.R.; Mertes, P.M.; Steib, A.; et al. Impact of high dose prophylactic anticoagulation in critically ill patients with COVID-19 pneumonia. Chest 2021, 16. (In Press)
- Bikdeli, B.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Farrokhpour, M.; Bakhshandeh, H.; Sezavar, H.; Dabbagh, A.; Beigmohammadi, M.T.; Payandemehr, P.; et al. Intermediate versus standard-dose prophylactic anticoagulation and statin therapy versus placebo in critically-ill patients with COVID-19: Rationale and design of the INSPIRATION/INSPIRATION-S studies. Thromb. Res. 2020, 196, 382–394. [Google Scholar] [CrossRef]
- Kosior, D.A.; Undas, A.; Kopeć, G.; Hryniewiecki, T.; Torbicki, A.; Mularek-Kubzdela, T.; Windyga, J.; Pruszczyk, P. Guidance for anticoagulation management in venous thromboembolism during the coronavirus disease 2019 (COVID-19) pandemic in Poland: An expert opinion of the Section on Pulmonary Circulation of the Polish Cardiac Society. Kardiologia Polska 2020, 25, 642–646. [Google Scholar] [CrossRef]
- Sakr, Y.; Giovini, M.; Leone, M.; Pizzilli, G.; Kortgen, A.; Bauer, M.; Tonetti, T.; Duclos, G.; Zieleskiewicz, L.; Buschbeck, S.; et al. Pulmonary embolism in patients with coronavirus disease-2019 (COVID-19) pneumonia, a narrative review. Ann. Intensive Care 2020, 16, 124. [Google Scholar] [CrossRef]
- Moores, L.K.; Tritschler, T.; Brosnahan, S.; Carrier, M.; Collen, J.F.; Doerschug, K.; Holley, A.B.; Jimenez, D.; Le Gal, G.; Rali, P.; et al. Prevention, Diagnosis, and Treatment of VTE in Patients with Coronavirus Disease 2019. Chest 2020, 158, 1143–1163. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. Global COVID-19 Thrombosis Collaborative Group, Endorsed by the ISTH, NATF, ESVM, and the IUA, Supported by the ESC Working Group on Pulmonary Circulation and Right Ventricular Function. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol 2020, 16, 2950–2973. [Google Scholar]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D. The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS); The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Respir J. 2019, 9, 1901647. [Google Scholar]
- Philippe, J.; Cordeanu, E.-M.; Leimbach, M.-B.; Greciano, S.; Younes, W. Acute pulmonary embolism and systemic thrombolysis in the era of COVID-19 global pandemic 2020: A case series of seven patients admitted to a regional hospital in the French epidemic cluster. Eur. Hear. J. Case Rep. 2021, 5, 522. [Google Scholar] [CrossRef] [PubMed]
- Scudiero, F.; Pitì, A.; Keim, R.; Parodi, G. Acute pulmonary embolism in COVID-19 patient: A case report of free-floating right heart thrombus successfully treated with fibrinolysis. Eur. Hear. J. Case Rep. 2021, 5, ytaa388. [Google Scholar] [CrossRef]
- Giri, J.; Sista, A.K.; Weinberg, I.; Kearon, C.; Kumbhani, D.J.; Desai, N.D.; Piazza, G.; Gladwin, M.T.; Chatterjee, S.; Kobayashi, T.; et al. Interventional Therapies for Acute Pulmonary Embolism: Current Status and Principles for the Development of Novel Evidence: A Scientific Statement from the American Heart Association. Circ. 2019, 140, e774–e801. [Google Scholar] [CrossRef]
- Flaczyk, A.; Rosovsky, R.P.; Reed, C.T.; Bankhead-Kendall, B.K.; Bittner, E.A.; Chang, M.G. Comparison of published guidelines for management of coagulopathy and thrombosis in critically ill patients with COVID 19: Implications for clinical practice and future investigations. Crit. Care 2020, 16, 559. [Google Scholar] [CrossRef]
- Greenall, R.; E Davis, R. Intermittent pneumatic compression for venous thromboembolism prevention: A systematic review on factors affecting adherence. BMJ Open 2020, 10, e037036. [Google Scholar] [CrossRef]
- Witt, D.M.; Nieuwlaat, R.; Clark, N.P.; Ansell, J.; Holbrook, A.; Skov, J.; Shehab, N.; Mock, J.; Myers, T.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Optimal management of anticoagulation therapy. Blood Adv. 2018, 2, 3257–3291. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 17 January 2021).
- Antithrombotic Therapy in Patients with COVID-19. Available online: https://www.covid19treatmentguidelines.nih.gov/adjunctive-therapy/antithrombotic-therapy/ (accessed on 13 January 2021).
- Aron, J.A.; Bulteel, A.J.; Clayman, K.A.; Cornett, J.A.; Filtz, K.; Heneghan, L.; Hubbell, K.T.; Huff, R.; Richter, A.J.; Yu, K.; et al. A Role for Telemedicine in Medical Education During the COVID-19 Pandemic. Acad. Med. 2020, 95, e4–e5. [Google Scholar] [CrossRef]
- Vadukul, P.; Sharma, D.S.; Vincent, P. Massive pulmonary embolism following recovery from COVID-19 infection: Inflammation, thrombosis and the role of extended thromboprophylaxis. BMJ Case Rep. 2020, 13, e238168. [Google Scholar] [CrossRef]
- Zhai, Z.; Li, C.; Chen, Y.; Gerotziafas, G.; Zhang, Z.; Wan, J.; Liu, P.; Elalamy, I.; Wang, C. Prevention Treatment of VTE Associated with COVID-19 Infection Consensus Statement Group. Prevention and Treatment of Venous Thromboembolism Associated with Coronavirus Disease 2019 Infection: A Consensus Statement before Guidelines. Thromb. Haemost. 2020, 120, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Patell, R.; Bogue, T.; Koshy, A.; Bindal, P.; Merrill, M.; Aird, W.C.; Bauer, K.A.; Zwicker, J.I. Post discharge thrombosis and hemorrhage in patients with COVID-19. Blood 2020, 136, 1342–1346. [Google Scholar] [CrossRef] [PubMed]
- Mojoli, F.; Mongodi, S.; Orlando, A.; Arisi, E.; Pozzi, M.; Civardi, L.; Tavazzi, G.; Baldanti, F.; Bruno, R.; Iotti, G.A. COVID-19 Pavia Crisis Unit. Our recommendations for acute management of COVID-19. Crit. Care 2020, 8, 207. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Study Design | Mean Age (Years) | Number of Patients | PE Incidence (%) | ICU (%) | Mortality (%) | Thromboprophylaxis | PE Imaging Test | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Artifoni et al. [30] | Retrospective cohort double-center study | 64 | 133 | 10 | 12.78 | 14.28 | Heparin (unspecified) | Low limb venous duplex ultrasonography/CTPA * |
| 2 | Lodigiani et al. [31] | Retrospective single-center | 66 | 388 | 2.8 | 16 | 26 | Low-molecular-weight heparin | Two-point compression ultrasonography |
| 3 | Poissy et al. [18] | Retrospective single-center | 57 | 107 | 20.6 | 20.6 | 14 | Unfractionated heparin or low-molecular-weight heparin | CTPA |
| 4 | Grillet et al. [32] | Retrospective single-center | 66 | 100 | 23 | 39 | NR | NR | CTPA |
| 5 | Leonard-Lorant et al. [33] | Retrospective double-center | 63.5 | 106 | 30.2 | 75 | NR | Low-molecular-weight heparin | CTPA |
| 6 | Llitjos et al. [34] | Retrospective double-center | 68 | 26 | 23.1 | An ICU study | 12 | Low-molecular-weight heparin or unfractionated heparin | Complete duplex ultrasound |
| 7 | Klok et al. [9] | Retrospective multicenter | 64 | 184 | 35.5 | An ICU study | 22 | Low-molecular-weight heparins | CTPA and/or ultrasonography |
| 8 | Thomas et al. [35] | Retrospective single-center | 59 | 63 | 7.9 | An ICUstudy | 16 | Unfractionated heparin/low-molecular-weight heparin | Lower limb ultrasound dopplers/CTPA |
| 9 | Middeldorp et al. [36] | Retrospective single-center | 61 | 198 | 6.6 | 38 | 19 | Low-molecular-weight heparin | CTPA |
| 10 | Helms et al. [37] | Prospective multicenter | 63 | 150 | 16.7 | An ICU study | 9 | Unfractionated heparin/low-molecular-weight heparin | CTPA/abdomen and pelvis CT |
| 11 | Hékimian et al. [38] | Retrospective single-center | NA | 51 | 16 | An ICU study | NR | NR | CTPA |
| 12 | Galeano-Valle et al. [39] | Prospective observational single-center | 64.3 | 24 | 45.8 | 3 | NR | NR | CTPA |
| 13 | Bompard et al. [20] | Retrospective double-center | 64 | 135 | 23.7 | 17 | 12 | Heparin (unspecified) | CTPA |
| 14 | Soumagne et al. [40] | Retrospective multicenter | 63.5 | 375 | 15 | An ICU study | NR | Anticoagulant not specified | NR |
| 15 | Fraissé et al. [41] | Retrospective single-center | 61 | 93 | 49 | An ICU study | 41 | Anticoagulant not specified | NR |
| 16 | Freund et al. [42] | Retrospective multicenter | 61. | 3253 | 15 | 0 | NR | NR | CTPA |
| 17 | Chen et al. [43] | Retrospective single-center | 65 | 25 | 40 | NR | 24 | NR | CTPA |
| 18 | Longchamp et al. [44] | Retrospective single-center | 68 | 25 | 20.0 | An ICU study | 20 | Heparin (unspecified) | CTPA/CUS ** |
| 19 | Whyte et al. [45] | Retrospective single-center | 61.5 | 1477 | 37 | 15 | 16 | Unfractionated heparin/low-molecular-weight heparin | CTPA |
| 20 | Marone et al. [46] | Retrospective single-center | NA | 101 | 23.7 | NR | NR | Low-molecular-weight heparin | Duplex ultrasound/CTPA |
| 21 | Fauvel et al. [47] | Retrospective multicenter | 64 | 1240 | 8.3 | 14.9 | 12.2 | Unfractionated heparin/low-molecular-weight heparin | CTPA |
| 22 | Van den Heuvel et al. [48] | Retrospective single-center | 63 | 51 | 18 | 37 | 1 | NR | CTPA |
| 23 | Mestre-Gómez et al. [21] | Retrospective single-center | 65 | 29 | 6.4 | 6.9 | 3.4 | Low-molecular-weight heparin | CTPA |
| 24 | Faggiano et al. [49] | Retrospective single-center | 70.3 | 25 | 7 | NR | 14 | Unfractionated or low-molecular-weight heparin | CTPA |
| 25 | Gervaise et al. [50] | Retrospective single-center | 62.3 | 72 | 18 | 57 | 15 | NR | CTPA |
| 26 | Trimaille et al. [51] | Retrospective single-center | 62.2 | 289 | 14.5 | 72 | 47 | Unfractionated heparin/low-molecular-weight heparin | CTPA |
| Condition of the Patient | Level of Risk for PE | Treatment |
|---|---|---|
| Stable | Mild and moderate risk | Pharmacological prevention is prescribed. LMWH is recommended as first-line treatment, in the absence of contraindication. |
| Traumatic | Mild and moderate risk | Pharmacological prevention is prescribed. LMWH is recommended as first-line treatment, in the absence of contraindication. In case of contraindication for pharmacological thromboprophylaxis, mechanical thromboprophylaxis is preferred. |
| Stable (discharged) | Persistent mild and moderate risk | Prolonged outpatient VTE * prophylaxis care is considered with LMWH ** over DOAC *** use to prevent drug–drug interactions, and/or frequent comorbidities. |
| Acute | Confirmed | Initial parenteral anticoagulation with LMWH or UFH, overlapped with latter vitamin K antagonist therapy. |
| Shock/hypotension | Confirmed | Systemically administered thrombolytics if there is no high risk of bleeding. |
| Acute/cardiopulmonary deterioration | Confirmed | Systemic thrombolytic therapy after an initiation of anticoagulant therapy in the absence of hypotension and a low risk of bleeding. |
| Acute | Confirmed | Systemic thrombolysis for patients eligible for advanced therapy but lack an invasive approach due to limited resources or high risk of viral transmission. |
| Critical (refractory circulatory collapse or cardiac arrest) | Confirmed | ECMO **** in combination with surgical embolectomy or catheter-directed treatment. |
| Stable (outpatient) | Confirmed | Parenteral anticoagulants overlapped with vitamin K antagonists. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akhter, M.S.; Hamali, H.A.; Mobarki, A.A.; Rashid, H.; Oldenburg, J.; Biswas, A. SARS-CoV-2 Infection: Modulator of Pulmonary Embolism Paradigm. J. Clin. Med. 2021, 10, 1064. https://doi.org/10.3390/jcm10051064
Akhter MS, Hamali HA, Mobarki AA, Rashid H, Oldenburg J, Biswas A. SARS-CoV-2 Infection: Modulator of Pulmonary Embolism Paradigm. Journal of Clinical Medicine. 2021; 10(5):1064. https://doi.org/10.3390/jcm10051064
Chicago/Turabian StyleAkhter, Mohammad Suhail, Hassan A. Hamali, Abdullah A. Mobarki, Hina Rashid, Johannes Oldenburg, and Arijit Biswas. 2021. "SARS-CoV-2 Infection: Modulator of Pulmonary Embolism Paradigm" Journal of Clinical Medicine 10, no. 5: 1064. https://doi.org/10.3390/jcm10051064
APA StyleAkhter, M. S., Hamali, H. A., Mobarki, A. A., Rashid, H., Oldenburg, J., & Biswas, A. (2021). SARS-CoV-2 Infection: Modulator of Pulmonary Embolism Paradigm. Journal of Clinical Medicine, 10(5), 1064. https://doi.org/10.3390/jcm10051064