
Prolonged Mechanical Ventilation in Patients with Deep-Seated Intracerebral Hemorrhage: Risk Factors and Clinical Implications

 ,
, 
 , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Admission Characteristics in Deep-Seated ICH Patients
3.3. ICU Admission Parameters
3.4. Impact of PMV on Length of Stay/Outcome/Mortality
3.5. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hemphill, J.C., 3rd; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Tuhrim, S.; Broderick, J.P.; Batjer, H.H.; Hondo, H.; Hanley, D.F. Spontaneous intracerebral hemorrhage. N. Engl. J. Med. 2001, 344, 1450–1460. [Google Scholar] [CrossRef]
- Hemphill, J.C., 3rd; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef]
- Mc Lernon, S.; Werring, D.; Terry, L. Clinicians’ Perceptions of the Appropriateness of Neurocritical Care for Patients with Spontaneous Intracerebral Hemorrhage (ICH): A Qualitative Study. Neurocrit. Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Morawo, A.O.; Gilmore, E.J. Critical Care Management of Intracerebral Hemorrhage. Semin Neurol. 2016, 36, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Mayer, S.A.; Rincon, F. Treatment of intracerebral haemorrhage. Lancet Neurol. 2005, 4, 662–672. [Google Scholar] [CrossRef]
- Huttner, H.B.; Kohrmann, M.; Berger, C.; Georgiadis, D.; Schwab, S. Predictive factors for tracheostomy in neurocritical care patients with spontaneous supratentorial hemorrhage. Cerebrovasc. Dis. 2006, 21, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, M.; Mincu, R.I.; Lortz, J.; Horacek, M.; Koch, A.; Pizanis, N.; Kamler, M.; Rassaf, T.; Luedike, P. Prolonged mechanical ventilation after left ventricular assist device implantation: Risk factors and clinical implications. ESC Heart Fail. 2019, 6, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Haviland, K.; Tan, K.S.; Schwenk, N.; Pillai, M.V.; Stover, D.E.; Downey, R.J. Outcomes after long-term mechanical ventilation of cancer patients. BMC Palliat. Care 2020, 19, 42. [Google Scholar] [CrossRef]
- Saber, H.; Palla, M.; Kazemlou, S.; Navi, B.B.; Yoo, A.J.; Simonsen, C.Z.; Sandio, A.; Rajah, G.; Khatibi, K.; Liebeskind, D.S.; et al. Prevalence, Predictors, and Outcomes of Prolonged Mechanical Ventilation After Endovascular Stroke Therapy. Neurocrit. Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Schuss, P.; Lehmann, F.; Schäfer, N.; Bode, C.; Scharnböck, E.; Schaub, C.; Heimann, M.; Potthoff, A.L.; Weller, J.; Güresir, E.; et al. Postoperative Prolonged Mechanical Ventilation in Patients with Newly Diagnosed Glioblastoma—An Unrecognized Prognostic Factor. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef]
- Hessington, A.; Tsitsopoulos, P.P.; Fahlstrom, A.; Marklund, N. Favorable clinical outcome following surgical evacuation of deep-seated and lobar supratentorial intracerebral hemorrhage: A retrospective single-center analysis of 123 cases. Acta Neurochir. (Wien) 2018, 160, 1737–1747. [Google Scholar] [CrossRef]
- Seung, W.B.; Jeong, J.H.; Kim, Y.G. Trajectories for Freehand-Guided Aspiration of Deep-Seated Spontaneous Intracerebral Hemorrhage. World Neurosurg. 2020, 133, e551–e557. [Google Scholar] [CrossRef]
- Rasras, S.; Safari, H.; Zeinali, M.; Jahangiri, M. Decompressive hemicraniectomy without clot evacuation in supratentorial deep-seated intracerebral hemorrhage. Clin. Neurol. Neurosurg. 2018, 174, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kothari, R.U.; Brott, T.; Broderick, J.P.; Barsan, W.G.; Sauerbeck, L.R.; Zuccarello, M.; Khoury, J. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996, 27, 1304–1305. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef] [PubMed]
- Schuss, P.; Hadjiathanasiou, A.; Brandecker, S.; Güresir, Á.; Vatter, H.; Güresir, E. Elevated C-reactive protein and white blood cell count at admission predict functional outcome after non-aneurysmal subarachnoid hemorrhage. J. Neurol. 2018, 265, 2944–2948. [Google Scholar] [CrossRef] [PubMed]
- Fung, C.; Murek, M.; Z’Graggen, W.J.; Krähenbühl, A.K.; Gautschi, O.P.; Schucht, P.; Gralla, J.; Schaller, K.; Arnold, M.; Fischer, U.; et al. Decompressive hemicraniectomy in patients with supratentorial intracerebral hemorrhage. Stroke 2012, 43, 3207–3211. [Google Scholar] [CrossRef]
- Safatli, D.A.; Gunther, A.; Schlattmann, P.; Schwarz, F.; Kalff, R.; Ewald, C. Predictors of 30-day mortality in patients with spontaneous primary intracerebral hemorrhage. Surg. Neurol. Int. 2016, 7, S510–S517. [Google Scholar] [CrossRef] [PubMed]
- Zahuranec, D.B.; Lisabeth, L.D.; Sanchez, B.N.; Smith, M.A.; Brown, D.L.; Garcia, N.M.; Skolarus, L.E.; Meurer, W.J.; Burke, J.F.; Adelman, E.E.; et al. Intracerebral hemorrhage mortality is not changing despite declining incidence. Neurology 2014, 82, 2180–2186. [Google Scholar] [CrossRef]
- Braksick, S.A.; Hemphill, J.C., 3rd; Mandrekar, J.; Wijdicks, E.F.M.; Fugate, J.E. Application of the FOUR Score in Intracerebral Hemorrhage Risk Analysis. J. Stroke Cerebrovasc. Dis. 2018, 27, 1565–1569. [Google Scholar] [CrossRef] [PubMed]
- Gregorio, T.; Pipa, S.; Cavaleiro, P.; Atanasio, G.; Albuquerque, I.; Castro Chaves, P.; Azevedo, L. Original Intracerebral Hemorrhage Score for the Prediction of Short-Term Mortality in Cerebral Hemorrhage: Systematic Review and Meta-Analysis. Crit. Care Med. 2019, 47, 857–864. [Google Scholar] [CrossRef]
- Munoz Venturelli, P.; Wang, X.; Zahuranec, D.B.; Lavados, P.M.; Stapf, C.; Lindley, R.; Delcourt, C.; Chalmers, J.; Anderson, C.S.; Robinson, T.G.; et al. Withdrawal of active treatment after intracerebral haemorrhage in the INTERACT2 study. Age Ageing 2017, 46, 329–332. [Google Scholar] [CrossRef]
- Sahgal, S.; Yande, A.; Thompson, B.B.; Chen, E.P.; Fagerlin, A.; Morgenstern, L.B.; Zahuranec, D.B. Surrogate Satisfaction with Decision Making After Intracerebral Hemorrhage. Neurocrit. Care 2020. [Google Scholar] [CrossRef]
- Simmons, B.B.; Parks, S.M. Intracerebral hemorrhage for the palliative care provider: What you need to know. J. Palliat. Med. 2008, 11, 1336–1339. [Google Scholar] [CrossRef] [PubMed]
- Weimer, J.M.; Nowacki, A.S.; Frontera, J.A. Withdrawal of Life-Sustaining Therapy in Patients with Intracranial Hemorrhage: Self-Fulfilling Prophecy or Accurate Prediction of Outcome? Crit. Care Med. 2016, 44, 1161–1172. [Google Scholar] [CrossRef]
- Aboussouan, L.S.; Lattin, C.D.; Kline, J.L. Determinants of long-term mortality after prolonged mechanical ventilation. Lung 2008, 186, 299–306. [Google Scholar] [CrossRef]
- Jang, C.S.; Wang, J.D. Predicting Mortality and Life Expectancy in Patients under Prolonged Mechanical Ventilation and Maintenance Dialysis. J. Palliat. Med. 2020, 23, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Toffart, A.C.; Timsit, J.F. Is prolonged mechanical ventilation of cancer patients futile? Crit. Care 2013, 17, 189. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.M.; Broderick, J.; Hennerici, M.; Brun, N.C.; Diringer, M.N.; Mayer, S.A.; Begtrup, K.; Steiner, T. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology 2006, 66, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Suarez, J.I.; Parekh, P.D.; Bhardwaj, A. Prediction and timing of tracheostomy in patients with infratentorial lesions requiring mechanical ventilatory support. Crit. Care Med. 2000, 28, 1383–1387. [Google Scholar] [CrossRef]
- Bösel, J.; Schiller, P.; Hook, Y.; Andes, M.; Neumann, J.O.; Poli, S.; Amiri, H.; Schonenberger, S.; Peng, Z.; Unterberg, A.; et al. Stroke-related Early Tracheostomy versus Prolonged Orotracheal Intubation in Neurocritical Care Trial (SETPOINT): A randomized pilot trial. Stroke 2013, 44, 21–28. [Google Scholar] [CrossRef]


{kind=link}
| Patients without PMV (n = 52) | Patients with PMV (n = 42) | ||
|---|---|---|---|
| Mean age (years) | 65 ± 16 | 64 ± 11 | n.s. |
| female sex | 21 (%) | 12 (%) | n.s. |
| pre-existing hypertension | 41 (%) | 37 (%) | n.s. |
| diabetes mellitus | 5 (10%) | 7 (17%) | n.s. |
| previous stroke | 9 (%) | 8 (%) | n.s. |
| chronic obstructive pulmonary disease COPD | 3 (6%) | 5 (12%) | n.s. |
| anticoagulant medication prior ictus | 23 (44%) | 17 (41%) | n.s. |
| Patients without PMV (n = 52) | Patients with PMV (n = 42) | Significance | |
|---|---|---|---|
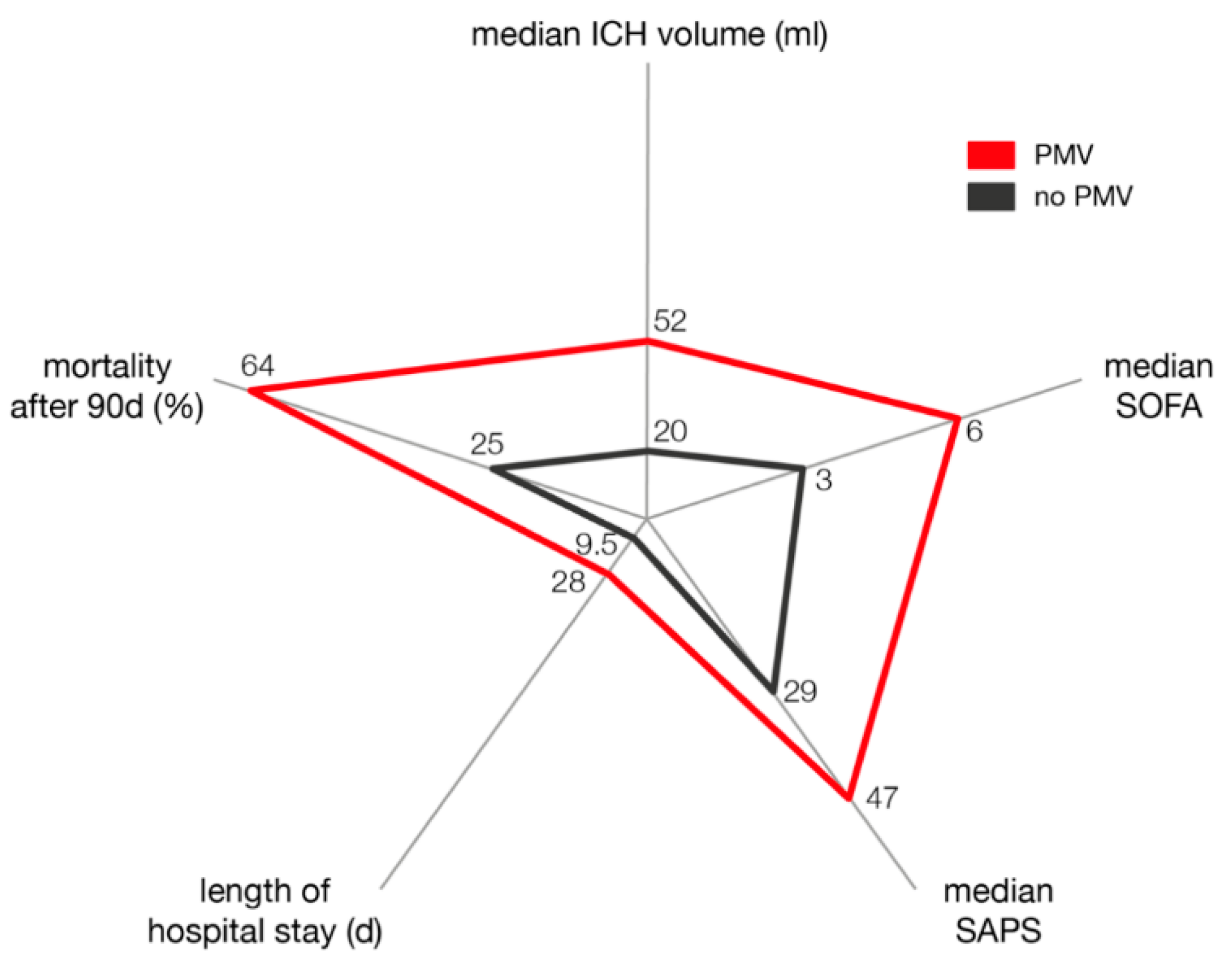
| median ICH volume (IQR, mL) | 20.3 (9.9–39.6) | 51.8 (29.7–93.9) | p < 0.0001 |
| ICH volume > 30 mL | 18 (35%) | 32 (76%) | p < 0.0001, OR 6.0, 95% CI 2.4–15.0 |
| admission GCS > 12 | 28 (54%) | 7 (17%) | p = 0.0002, OR 5.8, 95% CI 2.2–15.5 |
| ICH score > 3 | 6 (12%) | 11 (26%) | n.s. |
| admission CRP > 10 mg/L | 13 (25%) | 11 (26%) | n.s. |
| admission PCT > 0.5 μg/L | 2 (4%) | 7 (17%) | n.s. |
| admission WBC > 12 G/L | 16 (31%) | 19 (45%) | n.s. |
| early AKI | 7 (14%) | 15 (36%) | p = 0.02, OR 3.6, 95% CI 1.3–9.9 |
| admission SAPS score > 30 | 25 (48%) | 35 (83%) | p < 0.0001, OR 5.4, 95% CI 2.0–14.3 |
| admission SOFA score > 5 | 4 (8%) | 24 (57%) | p < 0.0001, OR 16, 95% CI 4.9–52.5 |
| favorable outcome after 3 months (mRS 0–4) | 38 (73%) | 15 (36%) | p < 0.0001, OR 4.9, 95% CI 2.0–11.8 |
| 90 d mortality | 13 (25%) | 27 (64%) | p < 0.0001, OR 5.4, 95% CI 2.2–13.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehmann, F.; Schenk, L.M.; Ilic, I.; Putensen, C.; Hadjiathanasiou, A.; Borger, V.; Zimmermann, J.; Güresir, E.; Vatter, H.; Bode, C.; et al. Prolonged Mechanical Ventilation in Patients with Deep-Seated Intracerebral Hemorrhage: Risk Factors and Clinical Implications. J. Clin. Med. 2021, 10, 1015. https://doi.org/10.3390/jcm10051015
Lehmann F, Schenk LM, Ilic I, Putensen C, Hadjiathanasiou A, Borger V, Zimmermann J, Güresir E, Vatter H, Bode C, et al. Prolonged Mechanical Ventilation in Patients with Deep-Seated Intracerebral Hemorrhage: Risk Factors and Clinical Implications. Journal of Clinical Medicine. 2021; 10(5):1015. https://doi.org/10.3390/jcm10051015
Chicago/Turabian StyleLehmann, Felix, Lorena M. Schenk, Inja Ilic, Christian Putensen, Alexis Hadjiathanasiou, Valeri Borger, Julian Zimmermann, Erdem Güresir, Hartmut Vatter, Christian Bode, and et al. 2021. "Prolonged Mechanical Ventilation in Patients with Deep-Seated Intracerebral Hemorrhage: Risk Factors and Clinical Implications" Journal of Clinical Medicine 10, no. 5: 1015. https://doi.org/10.3390/jcm10051015
APA StyleLehmann, F., Schenk, L. M., Ilic, I., Putensen, C., Hadjiathanasiou, A., Borger, V., Zimmermann, J., Güresir, E., Vatter, H., Bode, C., Schneider, M., & Schuss, P. (2021). Prolonged Mechanical Ventilation in Patients with Deep-Seated Intracerebral Hemorrhage: Risk Factors and Clinical Implications. Journal of Clinical Medicine, 10(5), 1015. https://doi.org/10.3390/jcm10051015