
Importance of Preoperative Screening Strategies for Coronavirus Disease 2019 in Patients Undergoing Cesarean Sections: A Retrospective, Large Single-Center, Observational Cohort Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
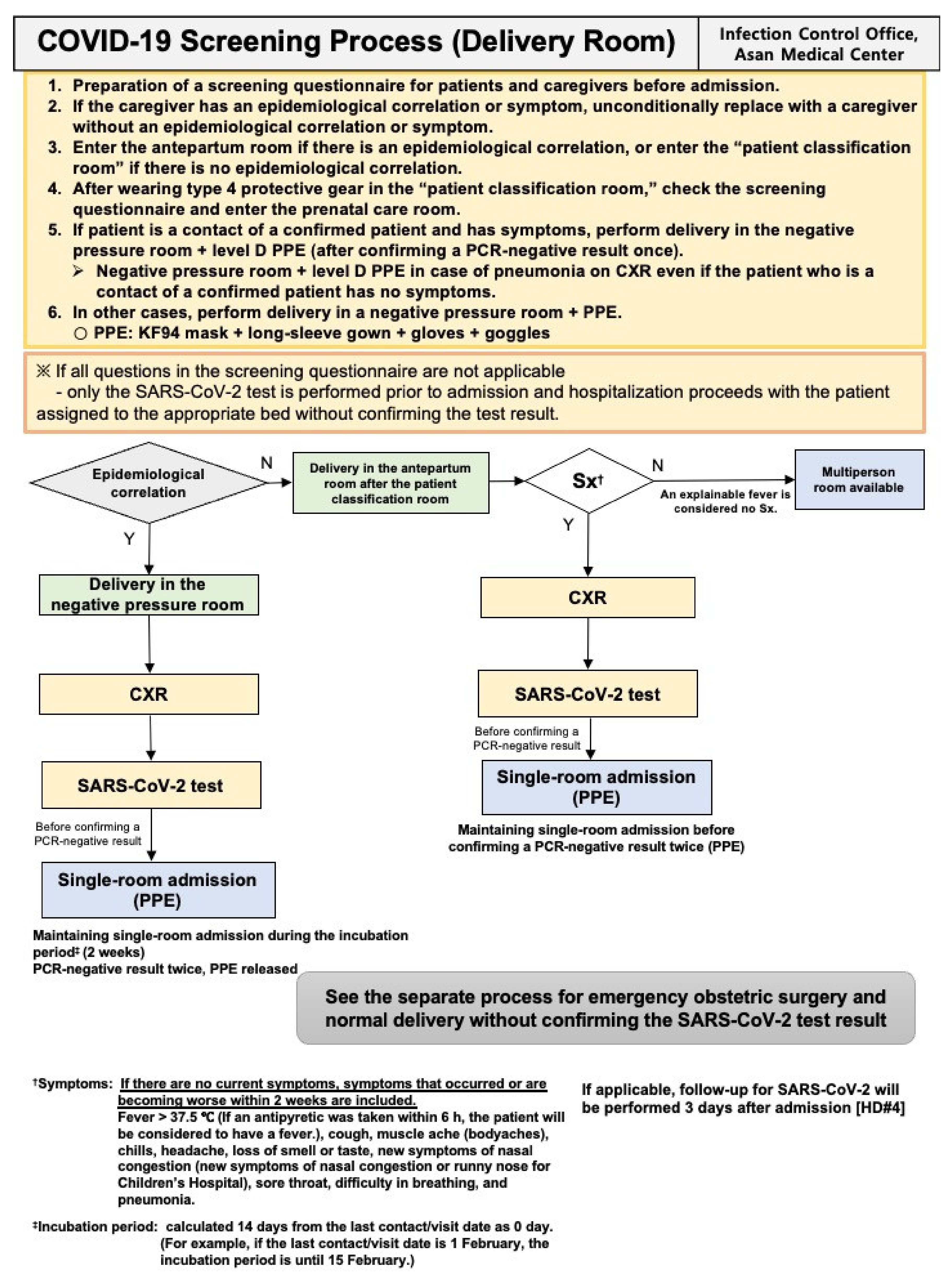
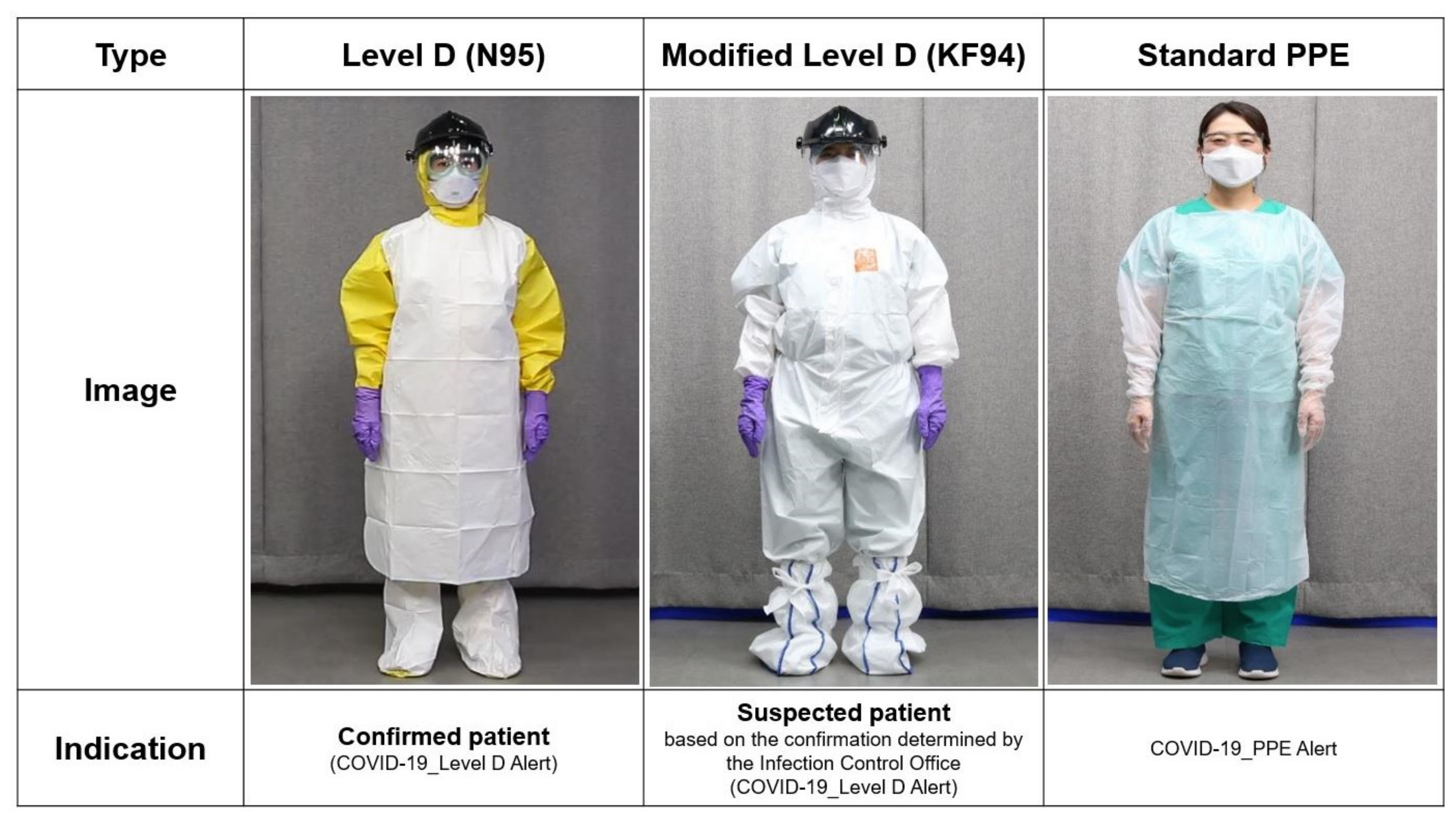
2.3. Preoperative SARS-CoV-2 Screening Process
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef]
- Pang, J.; Wang, M.X.; Ang, I.Y.H.; Tan, S.H.X.; Lewis, R.F.; Chen, J.I.-P.; Gutierrez, R.A.; Gwee, S.X.W.; Chua, P.E.Y.; Yang, Q.; et al. Potential rapid diagnostics, vaccine and therapeutics for 2019 novel coronavirus (2019-nCoV): A systematic review. J. Clin. Med. 2020, 9, 623. [Google Scholar] [CrossRef]
- Korean Society of Epidemiology. Report on the epidemiological features of Coronavirus disease 2019 (COVID-19) outbreak in the Republic of Korea from 19 January to 2 March 2020. J. Korean Med. Sci. 2020, 35, e112. [Google Scholar]
- Hojaij, F.C.; Chinelatto, L.A.; Boog, G.H.P.; Kasmirski, J.A.; Lopes, J.V.Z.; Sacramento, F.M. Surgical practice in the current COVID-19 pandemic: A rapid systematic review. Clinics 2020, 75, e1923. [Google Scholar] [CrossRef] [PubMed]
- Heller, G.; Bauer, E.; Schill, S.; Thomas, T.; Louwen, F.; Wolff, F.; Misselwitz, B.; Schmidt, S.; Veit, C. Decision-to-delivery time and perinatal complications in emergency cesarean section. Dtsch. Aerzteblatt Int. 2017, 114, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Central Disaster Management Headquarters and Korean Central Disease Control Headquarters. 2020. Latest Updates. Available online: http://ncov.mohw.go.kr/en/bdBoardList.do (accessed on 8 January 2021).
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. COVID-19, SARS and MERS: Are they closely related? Clin. Microbiol. Infect. 2020, 26, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Fu, J.-B.; Li, K.-F.; Liu, J.-N.; Wang, H.-L.; Liu, L.-J.; Chen, Y.; Zhang, Y.-L.; Liu, S.-L.; Tang, A.; et al. Transmission of COVID-19 in the terminal stages of the incubation period: A familial cluster. Int. J. Infect. Dis. 2020, 96, 452–453. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1–5. [Google Scholar] [CrossRef]
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or moderate Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation and treatment coronavirus (COVID-19). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kim, H.; Hong, H.; Yoon, S.H. Diagnostic performance of CT and reverse transcriptase polymerase chain reaction for Coronavirus disease 2019: A meta-analysis. Radiology 2020, 296, E145–E155. [Google Scholar] [CrossRef] [PubMed]
- Winichakoon, P.; Chaiwarith, R.; Liwsrisakun, C.; Salee, P.; Goonna, A.; Limsukon, A.; Kaewpoowat, Q. Negative nasopharyngeal and oropharyngeal swabs do not rule out COVID-19. J. Clin. Microbiol. 2020, 58, e00297-20. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting diagnostic tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef]
- Liu, W.; Wang, Q.; Zhang, Q.; Chen, L.; Chen, J.; Zhang, B.; Lu, Y.; Wang, S.; Xia, L.; Huang, L. Coronavirus disease 2019 (COVID-19) during pregnancy: A case series. Preprints 2020, 2020020373. [Google Scholar]
- Chambers, C.D.; Krogstad, P.; Bertrand, K.; Contreras, D.; Bode, L.; Tobin, N.; Aldrovandi, G.J.M. Evaluation of SARS-CoV-2 in breastmilk from 18 infected women. JAMA 2020, 324, 1347–1348. [Google Scholar] [CrossRef] [PubMed]
- Shaoshuai, W.; Lili, G.; Ling, C.; Weiyong, L.; Yong, C.; Jingyi, Z.; Ling, F. A case report of neonatal COVID-19 infection in China. Clin. Infect. Dis. 2020, 71, 853–857. [Google Scholar]
- Zeng, L.; Xia, S.; Yuan, W.; Yan, K.; Xiao, F.; Shao, J.; Zhou, W. Neonatal early-onset infection with SARS-CoV-2 in 33 neonates born to mothers with COVID-19 in Wuhan, China. JAMA Pediatrics 2020, 174, 722–725. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Emergency (n = 79) | Elective (n = 217) | Total (n = 296) | |
|---|---|---|---|
| Age, years (SD) | 34 (4) | 36 (4) | 35 (4) |
| BMI, kg/m2 (IQR) | 26.4 (24.6–28.3) | 26.7 (24.4–28.8) | 26.6 (24.4–28.7) |
| Gestational age, days (SD) | 254 (28) | 266 (11) | 263 (18) |
| Diagnosis, n (%) | |||
| Previous cesarean section | 7 (8.9%) | 53 (24.4%) | 60 (20.3%) |
| Cephalopelvic disproportion | 11 (13.9%) | 37 (17.1%) | 48 (16.2%) |
| Multifetal pregnancy | 6 (7.6%) | 36 (16.6%) | 42 (14.2%) |
| Known fetal anomaly | 7 (8.9%) | 19 (8.8%) | 26 (8.8%) |
| Placenta previa | 3 (3.8%) | 20 (9.2%) | 23 (7.8%) |
| Malpresentation | 5 (6.3%) | 13 (6.0%) | 18 (6.1%) |
| Failed induction of labor | 16 (20.3%) | 1 (0.5%) | 17 (5.7%) |
| Fetal distress | 6 (7.6%) | 2 (0.9%) | 8 (2.7%) |
| Preeclampsia | 4 (5.1%) | 4 (1.8%) | 8 (2.7%) |
| Anesthetic methods, n (%) | |||
| GA | 12 (15.2%) | 8 (3.7%) | 20 (6.8%) |
| SA | 22 (27.8%) | 13 (6.0%) | 35 (11.8%) |
| CSEA | 45 (57.0%) | 196 (90.3%) | 241 (81.4%) |
| ASA classification, n (%) | |||
| 2 | 73 (92.4%) | 212 (97.7%) | 285 (96.3%) |
| 3 | 6 (7.6%) | 5 (2.3%) | 11 (3.7%) |
| Duration of anesthesia, min (SD) | 63.6 (11.9) | 68.8 (25.9) | 67.4 (23.1) |
| Duration of operation, min (SD) | 41.8 (10.0) | 47.0 (41.2) | 45.6 (35.7) |
| Emergency (n = 79) | Elective (n = 217) | Total (n = 296) | ||
|---|---|---|---|---|
| Epidemiological correlation, n (%) | 4 (5.1%) | 0 | 4 (1.4%) | |
| Contact with a confirmed patient, n (%) | 0 | 0 | 0 | |
| Symptoms on the questionnaire, n (%) | ||||
| Fever | 10 (12.7%) | 1 (0.5%) | 11 (3.7%) | |
| Cough | 1 (1.3%) | 1 (0.5%) | 2 (0.7%) | |
| Dyspnea | 0 | 0 | 0 | |
| Chills | 0 | 1 (0.5%) | 1 (0.3%) | |
| Myalgia | 1 (1.3%) | 0 | 1 (0.3%) | |
| Sore throat | 0 | 0 | 0 | |
| New loss of taste or smell | 0 | 0 | 0 | |
| Body temperature, n (%) | ||||
| Day before the cesarean section | < 37.5 °C | 41 (51.9%) | 206 (94.9%) | 247 (83.4%) |
| ≥ 37.5 °C | 6 (7.6%) | 2 (0.9%) | 8 (2.7%) | |
| Morning of the operation day | < 37.5 °C | 72 (91.1%) | 190 (87.6%) | 262 (88.5%) |
| ≥ 37.5 °C | 4 (5.1%) | 0 | 4 (1.4%) | |
| Before entering the operating room | < 37.5 °C | 47 (59.5%) | 107 (49.3%) | 154 (52.0%) |
| ≥ 37.5 °C | 10 (12.7%) | 0 | 10 (3.4%) | |
| Before anesthesia | < 37.5 °C | 70 (88.6%) | 203 (93.5%) | 273 (92.2%) |
| ≥ 37.5 °C | 9 (11.4%) | 9 (4.1%) | 18 (6.1%) | |
| Number of perioperative SARS-CoV-2 tests, n (%) | ||||
| Preoperative | 1 | 69 (87.3%) | 210 (96.8%) | 279 (94.3%) |
| 2 | 5 (6.3%) | 7 (3.2%) | 12 (4.1%) | |
| 3 | 4 (5.1%) | 0 | 4 (1.4%) | |
| 5 | 1 (1.3%) | 0 | 1 (0.3%) | |
| Postoperative | 1 | 5 (6.3%) | 0 | 5 (1.7%) |
| Classification of patients without confirming a negative SARS-CoV-2 result, n (%) | ||||
| 1 | 1 (1.3%) | 0 | 1 (0.3%) | |
| 2 | 3 (3.8%) | 0 | 3 (1.0%) | |
| 3 | 38 (48.1%) | 0 | 38 (12.8%) | |
| Treated in a negative pressure operating room, n (%) | 42 (53.2%) | 0 | 42 (14.2%) | |
| Emergency (n = 90) | Elective (n = 254) | Total (n = 344) | |
|---|---|---|---|
| Birth weight, g (SD) | 2484 (900) | 2922 (572) | 2808 (701) |
| Apgar score, median (IQR) | |||
| 1 min | 8 (6–9) | 8 (8–9) | 8 (8–9) |
| 5 min | 9 (8–9) | 9 (9–9) | 9 (9–9) |
| NICU admission, n (%) | 43 (47.8%) | 52 (20.5%) | 95 (27.6%) |
| NICU negative pressure room admission, n (%) | 4 (4.4%) | 0 | 4 (1.2%) |
| Multifetal pregnancy case, n | |||
| Twin | 7 | 37 | 44 |
| Triplet | 2 | 0 | 2 |
| Newborn No. | Length of Hospital Stay, Day | Length of ICU Stay, Day | Ventilation Requirements | Healthcare Infection |
|---|---|---|---|---|
| 1 * | 1 | 1 | Yes | No |
| 2 | 3 | 3 | No | No |
| 3 | 4 | 4 | No | No |
| 4 | 17 | 17 | Yes | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-J.; Cho, H.-S.; Lee, M.-Y.; Kim, H.; Choi, W.-J.; Won, H.-S.; Ro, Y.-J.; Choi, I.-C. Importance of Preoperative Screening Strategies for Coronavirus Disease 2019 in Patients Undergoing Cesarean Sections: A Retrospective, Large Single-Center, Observational Cohort Study. J. Clin. Med. 2021, 10, 885. https://doi.org/10.3390/jcm10040885
Kim H-J, Cho H-S, Lee M-Y, Kim H, Choi W-J, Won H-S, Ro Y-J, Choi I-C. Importance of Preoperative Screening Strategies for Coronavirus Disease 2019 in Patients Undergoing Cesarean Sections: A Retrospective, Large Single-Center, Observational Cohort Study. Journal of Clinical Medicine. 2021; 10(4):885. https://doi.org/10.3390/jcm10040885
Chicago/Turabian StyleKim, Ha-Jung, Hyun-Seok Cho, Mi-Young Lee, Hyungtae Kim, Woo-Jong Choi, Hye-Sung Won, Young-Jin Ro, and In-Cheol Choi. 2021. "Importance of Preoperative Screening Strategies for Coronavirus Disease 2019 in Patients Undergoing Cesarean Sections: A Retrospective, Large Single-Center, Observational Cohort Study" Journal of Clinical Medicine 10, no. 4: 885. https://doi.org/10.3390/jcm10040885
APA StyleKim, H.-J., Cho, H.-S., Lee, M.-Y., Kim, H., Choi, W.-J., Won, H.-S., Ro, Y.-J., & Choi, I.-C. (2021). Importance of Preoperative Screening Strategies for Coronavirus Disease 2019 in Patients Undergoing Cesarean Sections: A Retrospective, Large Single-Center, Observational Cohort Study. Journal of Clinical Medicine, 10(4), 885. https://doi.org/10.3390/jcm10040885