
Oxidative Stress Reduction by Midazolam Premedication during Oocyte Retrieval Procedure: Pilot Study


 and
and 
Abstract
1. Introduction
2. Experimental Section
2.1. Patients and Experimental Procedure
2.2. Total Oxidative Capacity
2.3. Total Antioxidative Capacity
2.4. Total Glutathione Levels
2.5. Catalase Activity
2.6. Statistical Analyses
3. Results
3.1. Patients
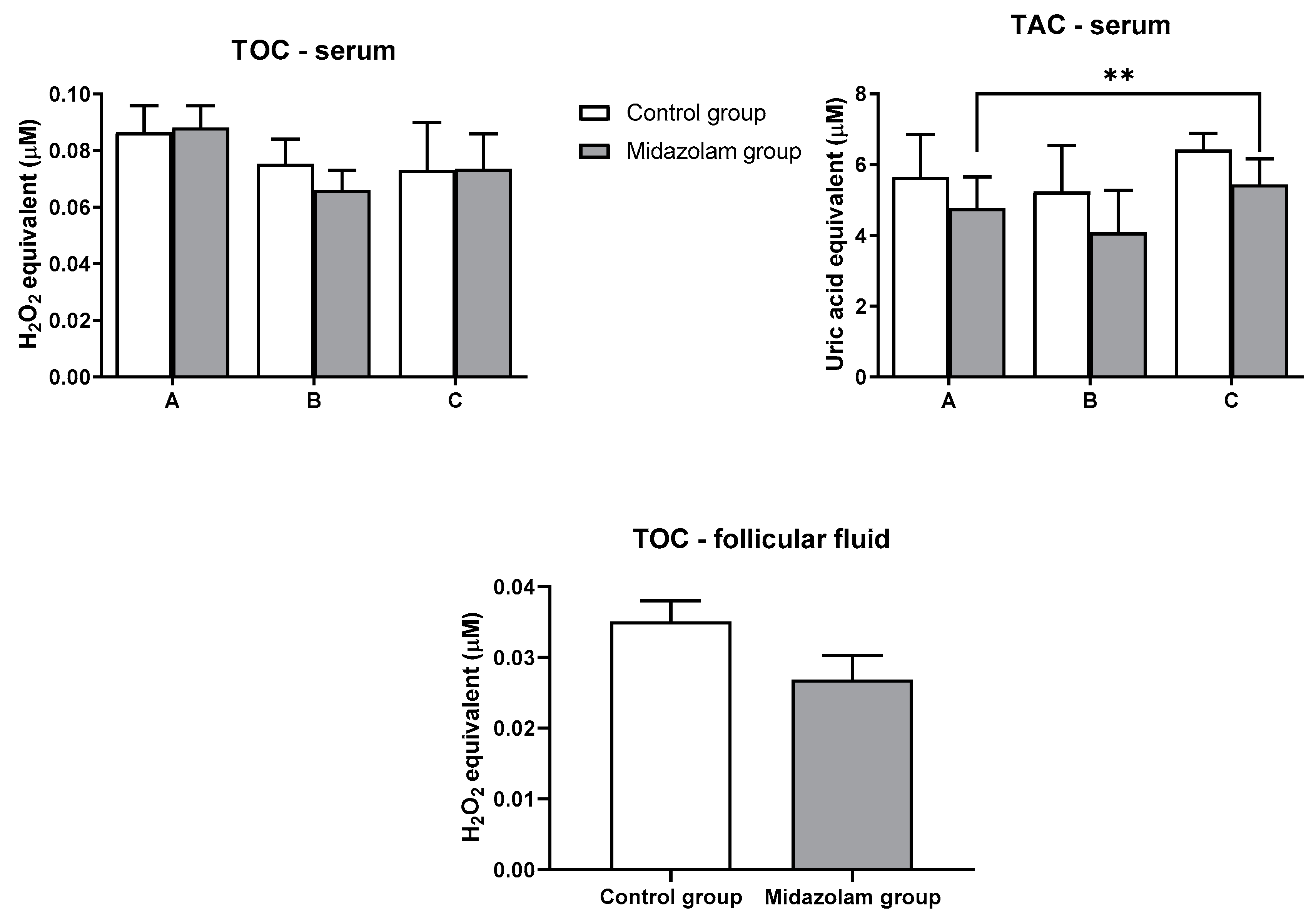
3.2. Total Oxidant and Antioxidant Capacities
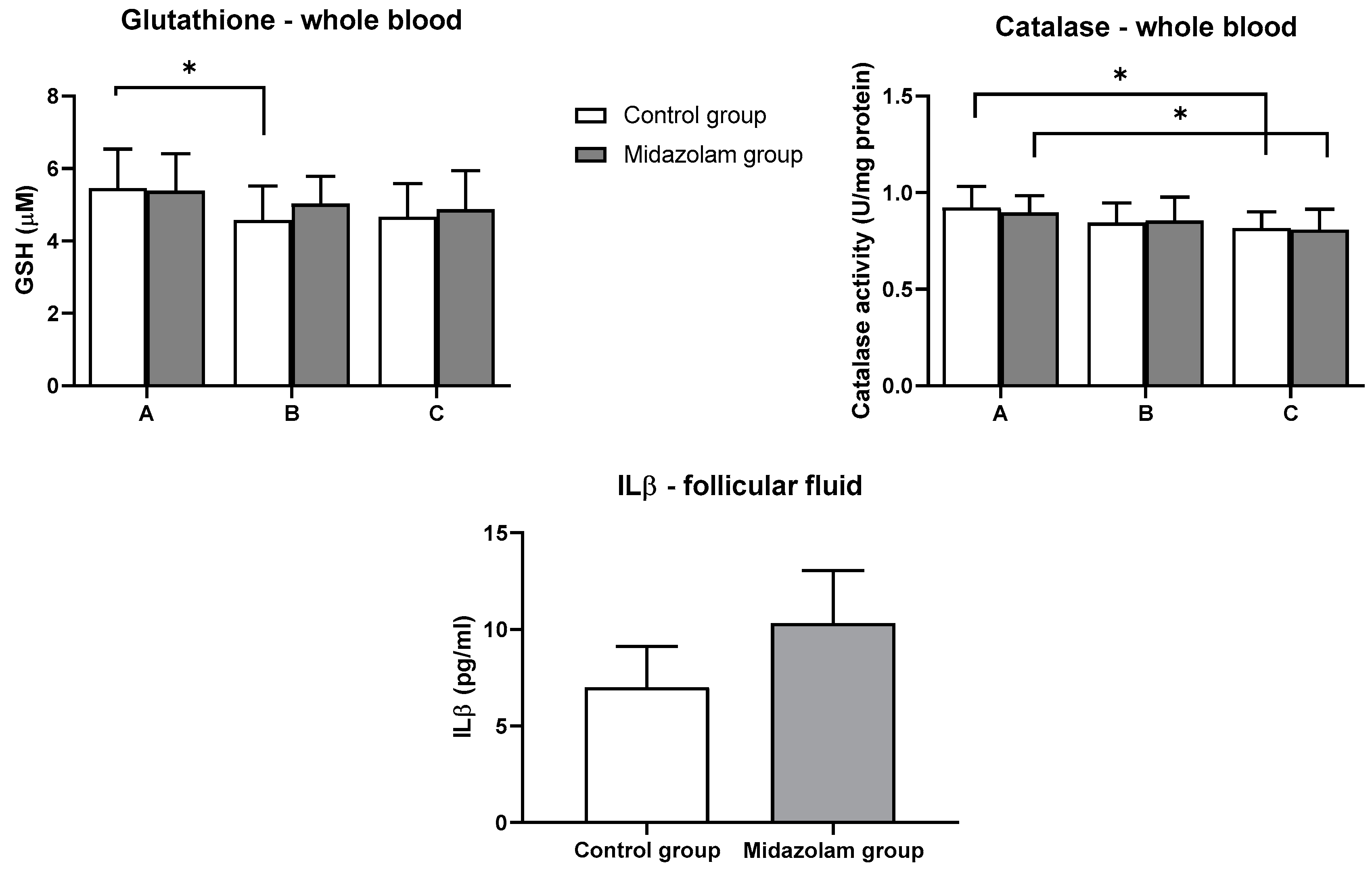
3.3. GSH Levels and Catalase Activity
3.4. Positive Outcome—Follow-Up
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boivin, J.; Bunting, L.; Collins, J.A.; Nygren, K.G. International estimates of infertility prevalence and treatment-seeking: Potential need and demand for infertility medical care. Hum. Reprod. 2007, 22, 1506–1512. [Google Scholar] [CrossRef]
- Amato, P.; Daar, J.; Francis, L.; Klipstein, S.; Ball, D.; Rinaudo, P.; Rajovic, A.; Palmore, M.; Tipton, S.; Coutifaris, C.; et al. Ethics in embryo research: A position statement by the ASRM Ethics in Embryo Research Task Force and the ASRM Ethics Committee. Fertil. Steril. 2020, 113, 270–294. [Google Scholar] [CrossRef] [PubMed]
- Boivin, J.; Griffiths, E.; Venetis, C.A. Emotional distress in infertile women and failure of assisted reproductive technologies: Meta-analysis of prospective psychosocial studies. BMJ 2011, 342, d223. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, A.; Panayotidis, C.; Amso, N.; Marci, R.; Matorras, R.; Onofriescu, M.; Turp, A.B.; Vandekerckhove, F.; Veleva, Z.; Vermeulen, N.; et al. Recommendations for good practice in ultrasound: Oocyte pick up. Hum. Reprod. Open 2019, 2019, hoz025. [Google Scholar] [PubMed]
- Klonoff-Cohen, H.; Chu, E.; Natarajan, L.; Sieber, W. A prospective study of stress among women undergoing in vitro fertilization or gamete intrafallopian transfer. Fertil. Steril. 2001, 76, 675–687. [Google Scholar] [CrossRef]
- Demyttenaere, K.; Nijs, P.; Evers-Kiebooms, G.; Koninckx, P.R. Coping, ineffectiveness of coping and the psychoendocrinological stress responses during in-vitro fertilization. J. Psychosom. Res. 1991, 35, 231–243. [Google Scholar] [CrossRef]
- Boivin, J.; Takefman, J.E. Stress level across stages of in vitro fertilization in subsequently pregnant and nonpregnant women. Fertil. Steril. 1995, 64, 802–810. [Google Scholar] [CrossRef]
- Csemiczky, G.; Landgten, B.-M.; Collins, A. The influence of stress and state anxiety on the outcome of IVF-treatment: Psychological and endocrinological assessment of Swedish women entering IVF-treatment. Acta Obstet. Gynecol. Scand. 2000, 79, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.H.Y. Anxiolytic premedication reduces preoperative anxiety and pain during oocyte retrieval. A randomized double-blinded placebo-controlled trial. Hum. Reprod. 2002, 17, 1233–1238. [Google Scholar] [CrossRef][Green Version]
- An, Y.; Sun, Z.; Li, L.; Zhang, Y.; Ji, H. Relationship between psychological stress and reproductive outcome in women undergoing in vitro fertilization treatment: Psychological and neurohormonal assessment. J. Assist. Reprod. Genet. 2012, 30, 35–41. [Google Scholar] [CrossRef]
- Aimagambetova, G.; Issanov, A.; Terzic, S.; Bapayeva, G.; Ukybassova, T.; Baikoshkarova, S.; Aldiyarova, A.; Shauyen, F.; Terzic, M. The effect of psychological distress on IVF outcomes: Reality or speculations? PLoS ONE 2020, 15, e0242024. [Google Scholar] [CrossRef]
- Tola, E.N. The effect of anesthetic agents for oocyte pick-up on in vitro fertilization outcome: A retrospective study in a tertiary center. Taiwan J. Obstet. Gynecol. 2019, 58, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Gejervall, A.L.; Stener-Victorin, E.; Cerne, A.; Borg, K.; Bergh, C. Pain aspects in oocyte aspiration for IVF. Reprod. Biomed. Online 2007, 14, 184–190. [Google Scholar] [CrossRef]
- Hadimioglu, N.; Aydogdu Titiz, T.; Dosemeci, L.; Erman, M. Comparison of various sedation regimens for transvaginal oocyte retrieval. Fertil. Steril. 2002, 78, 648–649. [Google Scholar] [CrossRef]
- Sies, H.; Cadenas, E. Oxidative stress: Damage to intact cells and organs. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 1985, 311, 617–631. [Google Scholar]
- Cabello-Verrugio, C.; Simon, F.; Trollet, C.; Santibañez, J.F. Oxidative Stress in Disease and Aging: Mechanisms and Therapies 2016. Oxid. Med. Cell. Longev. 2017, 2017, 4310469. [Google Scholar] [CrossRef]
- Dutta, S.; Majzoub, A.; Agarwal, A. Oxidative stress and sperm function: A systematic review on evaluation and management. Arab J. Urol. 2019, 17, 87–97. [Google Scholar] [CrossRef]
- Amorini, A.M.; Listorti, I.; Bilotta, G.; Pallisco, R.; Saab, M.W.; Mangione, R.; Manca, B.; Lazzarino, G.; Tavazzi, B.; Lazzarino, G.; et al. Antioxidant-Based Therapies in Male Infertility: Do We Have Sufficient Evidence Supporting Their Effectiveness? Antioxidants 2021, 10, 220. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Gupta, S.; Sharma, R.K. Role of oxidative stress in female reprodution. Reprod. Biol. Endocrinol. 2005, 3, 28. [Google Scholar] [CrossRef]
- Rodríguez-Varela, C.; Labarta, E. Clinical application of antioxidants to improve human oocyte mitochondrial function: A review. Antioxidants 2020, 9, 1197. [Google Scholar] [CrossRef]
- Lampiao, F. Free radicals generation in an in vitro fertilization setting and how to minimize them. World J. Obstet. Gynecol. 2012, 1, 29. [Google Scholar] [CrossRef]
- Tatzber, F.; Griebenow, S.; Wonisch, W.; Winkler, R. Dual method for the determination of peroxidase activity and total peroxides-iodide leads to a significant increase of peroxidase activity in human sera. Anal. Biochem. 2003, 316, 147–153. [Google Scholar] [CrossRef]
- Tietze, F. Enzymic method for quantitative determination of nanogram amounts of total and oxidized glutathione: Applications to mammalian blood and other tissues. Anal. Biochem. 1969, 27, 502–522. [Google Scholar] [CrossRef]
- Góth, L. A simple method for determination of serum catalase activity and revision of reference range. Clin. Chim. Acta. 1991, 196, 143–151. [Google Scholar] [CrossRef]
- Campbell, M.K.; Farrell, S.O. Biochemistry; Brooks/Cole, Cengage Learning: Boston, MA, USA, 2012; ISBN 0840068581. [Google Scholar]
- Sies, H. Biochemistry of Oxidative Stress. Angew. Chemie Int. Ed. Engl. 1986, 25, 1058–1071. [Google Scholar] [CrossRef]
- Wojsiat, J.; Korczyński, J.; Borowiecka, M.; Żbikowska, H.M. The role of oxidative stress in female infertility and in vitro fertilization. Postepy Hig. Med. Dosw. 2017, 71, 359–366. [Google Scholar] [CrossRef]
- Harlev, A.; Gupta, S.; Agarwal, A. Targeting oxidative stress to treat endometriosis. Expert Opin. Ther. Targets 2015, 19, 1447–1464. [Google Scholar] [CrossRef]
- Nishihara, T.; Matsumoto, K.; Hosoi, Y.; Morimoto, Y. Evaluation of antioxidant status and oxidative stress markers in follicular fluid for human in vitro fertilization outcome. Reprod. Med. Biol. 2018, 17, 481–486. [Google Scholar] [CrossRef]
- Pasqualotto, E.B.; Agarwal, A.; Sharma, R.K.; Izzo, V.M.; Pinotti, J.A.; Joshi, N.J.; Rose, B.I. Effect of oxidative stress in follicular fluid on the outcome of assisted reproductive procedures. Fertil. Steril. 2004, 81, 973–976. [Google Scholar] [CrossRef]
- Gery, I.; Handschumacher, R.E. Potentiation of the T lymphocyte response to mitogens. Cell. Immunol. 1974, 11, 162–169. [Google Scholar] [CrossRef]
- Masters, S.L.; Simon, A.; Aksentijevich, I.; Kastner, D.L. Horror Autoinflammaticus: The Molecular Pathophysiology of Autoinflammatory Disease. Annu. Rev. Immunol. 2009, 27, 621–668. [Google Scholar] [CrossRef] [PubMed]
- Kreines, F.M.; Nasioudis, D.; Minis, E.; Irani, M.; Witkin, S.S.; Spandorfer, S. IL-1β predicts IVF outcome: A prospective study. J. Assist. Reprod. Genet. 2018, 35, 2031–2035. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Control Group | Midazolam Group | χ2, p |
|---|---|---|---|
| Estradiol | H = 3 N = 23 L = 1 | H = 5 N = 23 L = 3 | 1.230; 0.541 |
| Progesterone | H = 0 N = 10 L = 9 | H = 2 N = 10 L = 8 | 2.035; 0.362 |
| Testosterone | H = 0 N = 21 L = 0 | H = 1 N = 26 L = 0 | 0.794; 0.891 |
| Dehidroxyepiandrostendione-sulfate | H = 1 N = 16 L = 0 | H = 2 N = 17 L = 0 | 0.253; 0.503 |
| thyrotropin | H = 0 N = 24 L = 0 | H = 0 N = 22 L = 0 | - |
| anti-Müllerian hormone | H = 0 N = 23 L = 0 | H = 0 N = 26 L = 0 | - |
| follicle-stimulating hormone | H = 0 N = 24 L = 0 | H = 0 N = 26 L = 0 | - |
| luteinizing hormone | H = 4 N = 21 L = 0 | H = 0 N = 27 L = 0 | 4.680; 0.030 |
| Prolactin | H = 3 N = 16 L = 2 | H = 5 N = 17 L = 2 | 0.332; 0.847 |
| BMI | H = 4 N = 23 L = 2 | H = 9 N = 21 L = 1 | 2.281, 0.319 |
| Parameter for | Control Group N = 8 | Midazolam Group N = 3 | χ2, p |
|---|---|---|---|
| Estradiol | H = 1 N = 4 L = 0 | H = 0 N = 3 L = 0 | 0.686; 0.408 |
| Progesterone | H = 0 N = 1 L = 1 | H = 0 N = 2 L = 1 | - |
| Testosterone | H = 0 N = 3 L = 0 | H = 0 N = 2 L = 0 | - |
| Dehidroxyepiandrostendione-sulfate | H = 1 N = 2 L = 0 | H = 0 N = 2 L = 0 | 0.833; 0.361 |
| thyrotropin | H = 0 N = 4 L = 0 | H = 0 N = 3 L = 0 | - |
| anti-Müllerian hormone | H = 3 N = 1 L = 0 | H = 1 N = 1 L = 0 | 0.375; 0.540 |
| follicle-stimulating hormone | H = 0 N = 5 L = 0 | H = 0 N = 3 L = 0 | - |
| luteinizing hormone | H = 1 N = 4 L = 0 | H = 0 N = 3 L = 0 | 0.686; 0.408 |
| Prolactin | H = 1 N = 1 L = 0 | H = 0 N = 3 L = 0 | 1.875; 0.171 |
| BMI | H = 2 N = 4 L = 2 | H = 1 N = 2 L = 0 | 0.000; >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pešić, M.; Kličan-Jaić, K.; Vučić, M.; Kuna, K.; Košec, A.; Čipak Gašparović, A. Oxidative Stress Reduction by Midazolam Premedication during Oocyte Retrieval Procedure: Pilot Study. J. Clin. Med. 2021, 10, 855. https://doi.org/10.3390/jcm10040855
Pešić M, Kličan-Jaić K, Vučić M, Kuna K, Košec A, Čipak Gašparović A. Oxidative Stress Reduction by Midazolam Premedication during Oocyte Retrieval Procedure: Pilot Study. Journal of Clinical Medicine. 2021; 10(4):855. https://doi.org/10.3390/jcm10040855
Chicago/Turabian StylePešić, Maja, Katarina Kličan-Jaić, Marinko Vučić, Krunoslav Kuna, Andro Košec, and Ana Čipak Gašparović. 2021. "Oxidative Stress Reduction by Midazolam Premedication during Oocyte Retrieval Procedure: Pilot Study" Journal of Clinical Medicine 10, no. 4: 855. https://doi.org/10.3390/jcm10040855
APA StylePešić, M., Kličan-Jaić, K., Vučić, M., Kuna, K., Košec, A., & Čipak Gašparović, A. (2021). Oxidative Stress Reduction by Midazolam Premedication during Oocyte Retrieval Procedure: Pilot Study. Journal of Clinical Medicine, 10(4), 855. https://doi.org/10.3390/jcm10040855