
Embryological Development and Topographic Anatomy of Pelvic Compartments—Surgical Relevance for Pelvic Lymphonodectomy

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Lymphonodectomy
1.2. Pelvic Compartments
2. Methods
2.1. Selection of Pelvic Malignancies
2.2. Dissection of Anatomical Specimens
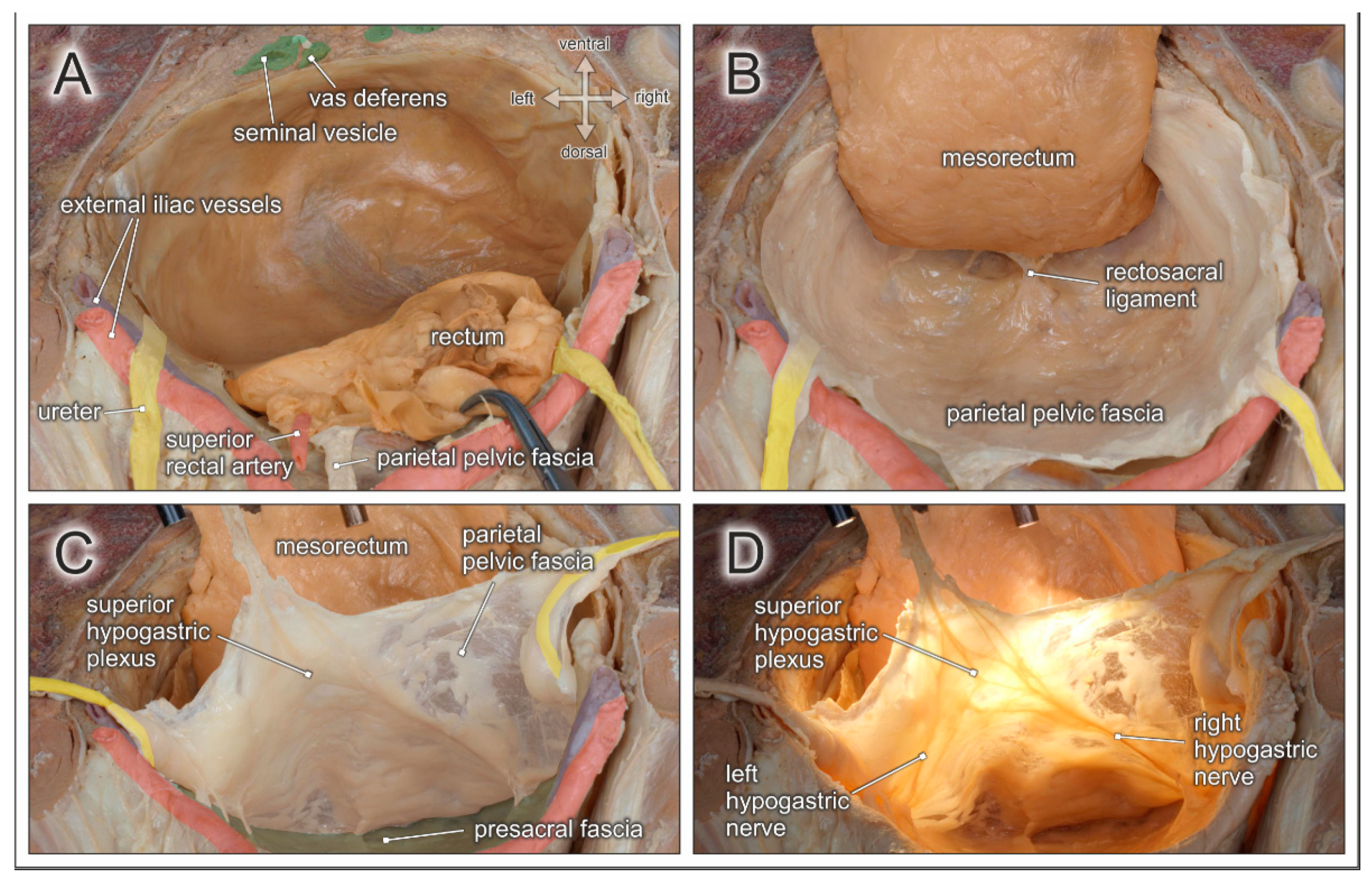
3. Posterior Pelvic Compartment
3.1. Embryology
3.2. Surgery
3.3. Anatomy
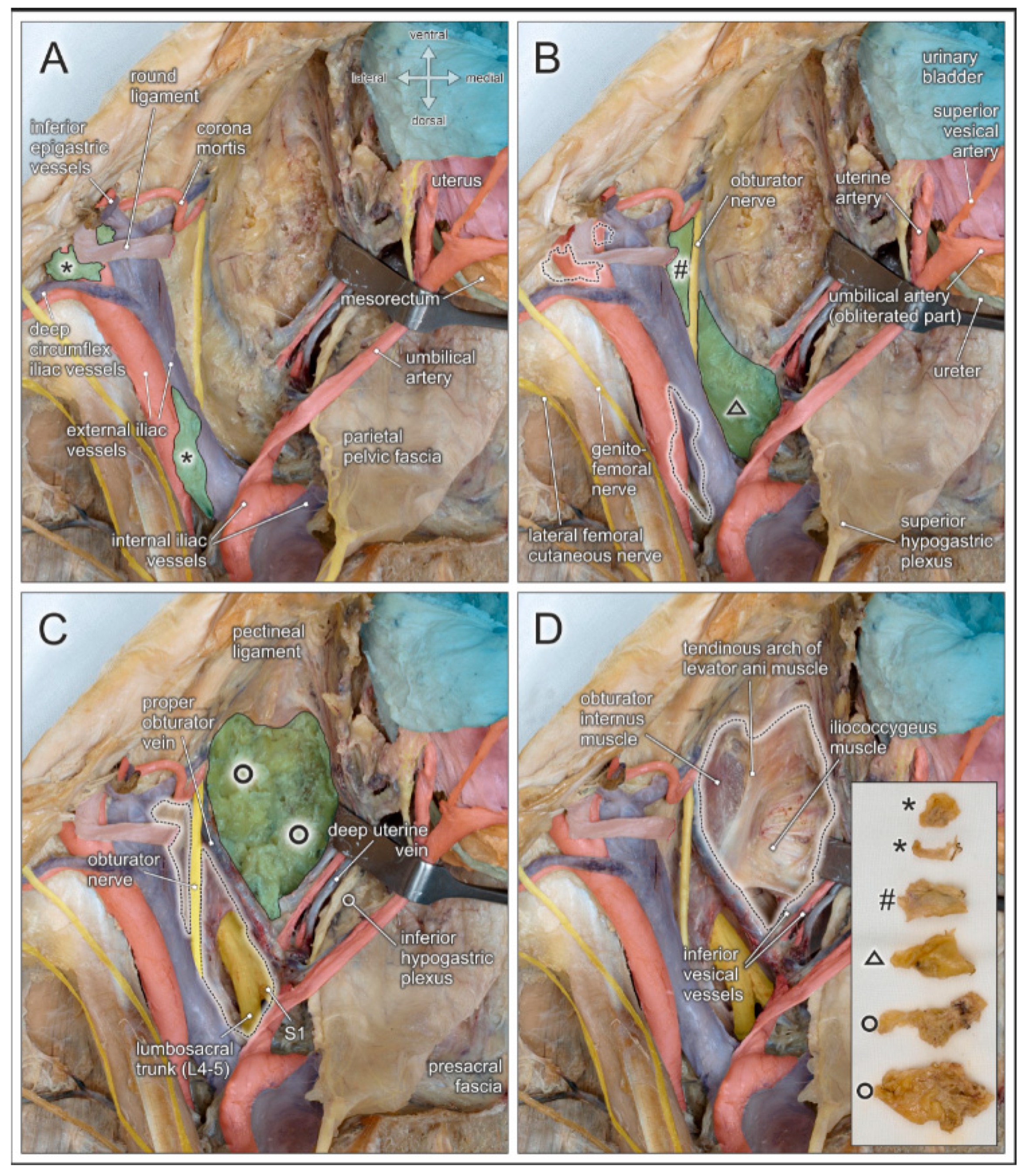
4. Middle (Female) Pelvic Compartment
4.1. Embryology
4.2. Surgery
4.3. Anatomy
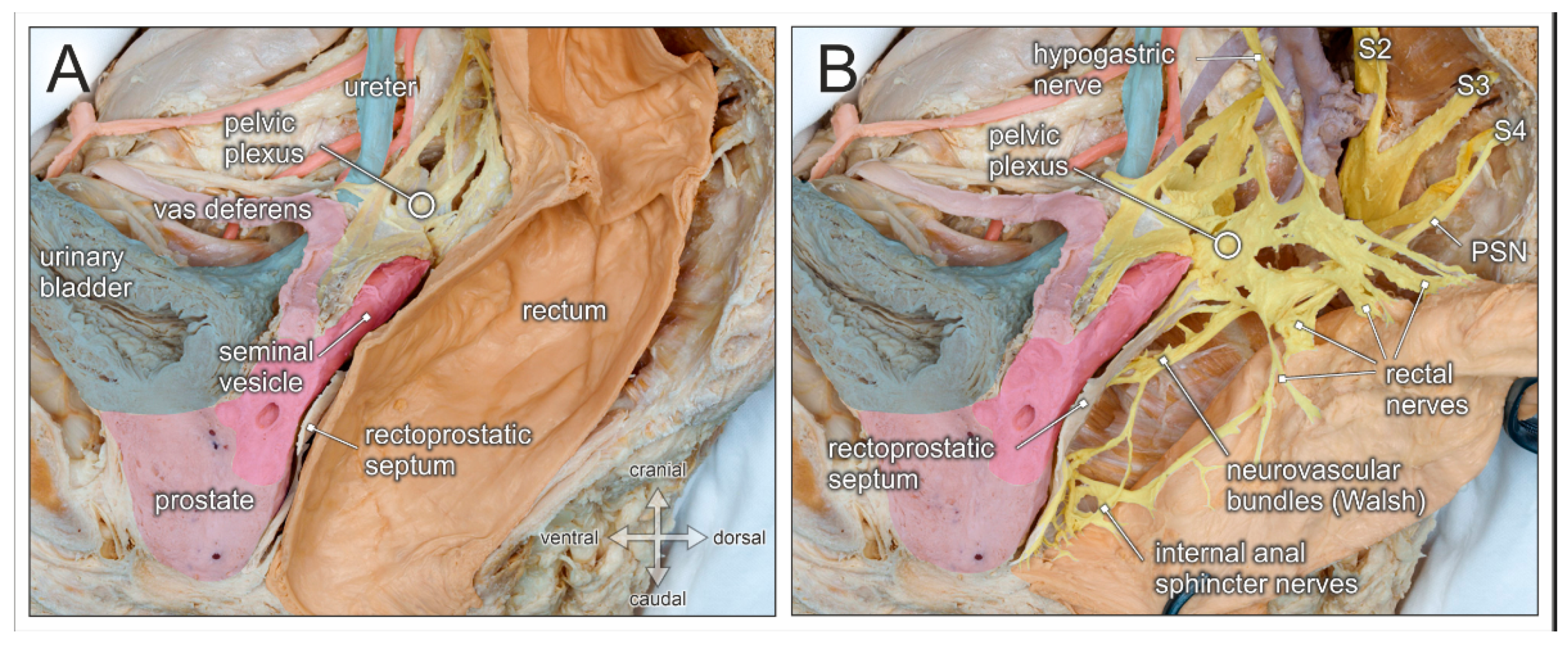
5. Ventral (Male) Pelvic Compartment
5.1. Embryology
5.2. Surgery
5.3. Anatomy
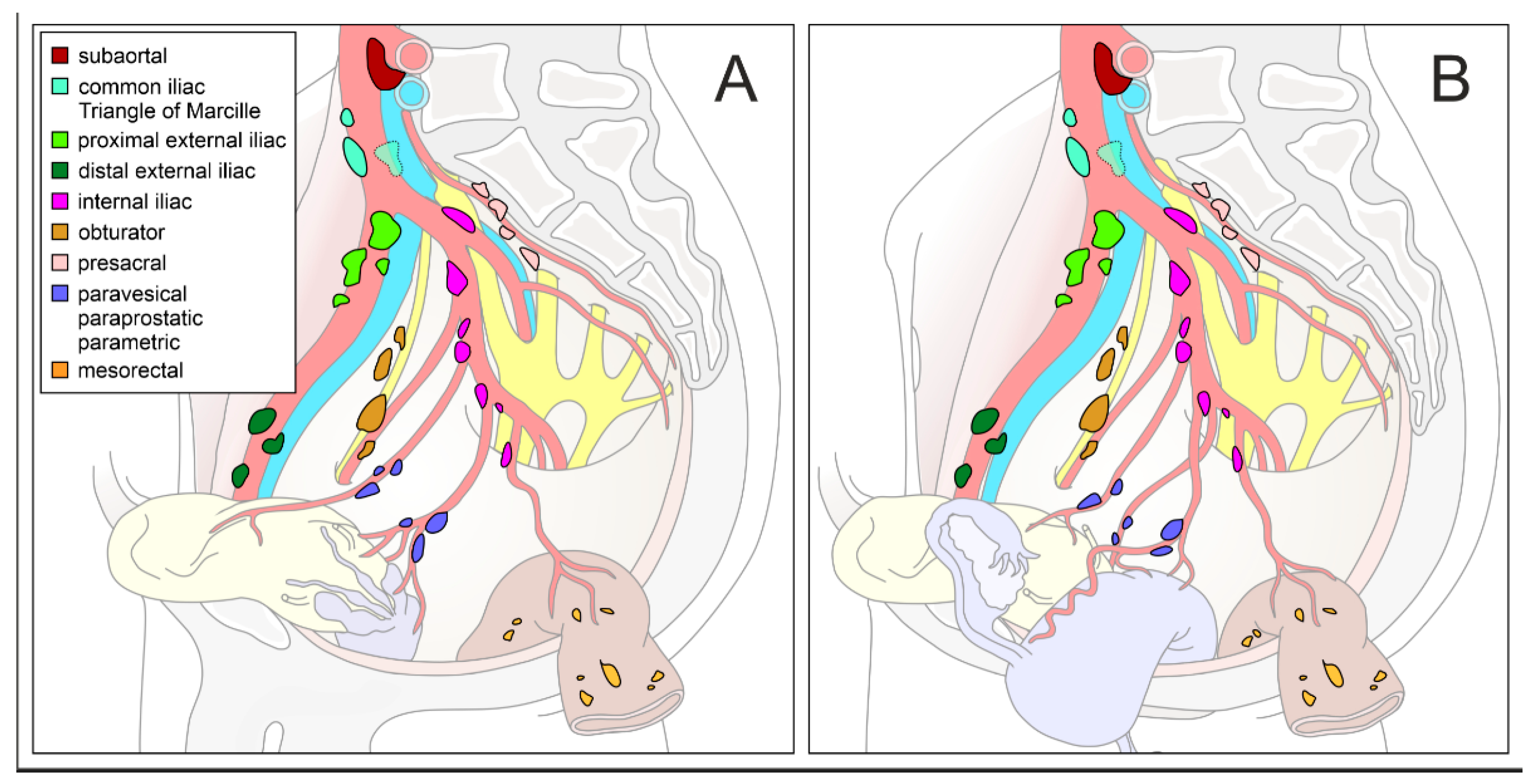
6. Lymph Nodes and Lymphatic Vessels
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cibula, D.; Abu-Rustum, N.R. Pelvic lymphadenectomy in cervical cancer--surgical anatomy and proposal for a new classification system. Gynecol. Oncol. 2010, 116, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Stillwell, A.P.; Ho, Y.-H.; Veitch, C. Systematic review of prognostic factors related to overall survival in patients with stage IV colorectal cancer and unresectable metastases. World J. Surg. 2011, 35, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Lehnert, T.; Herfarth, C. Principles and value of lymph node excision in colorectal carcinoma. Der Chir. Z. Fur Alle Geb. Der Oper. Medizen 1996, 67, 889–899. [Google Scholar]
- Committee on Classification of Regional Lymph Nodes of Japan Society of Clinical Oncology Classification of regional lymph nodes in Japan. Classification of regional lymph nodes in Japan. Int. J. Clin. Oncol. 2003, 8, 248–275. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, H.; Aigner, F.; Ludwikowski, B.; Reinstadler-Zankl, S.; Illig, R.; Urbas, D.; Schwarzer, C.; Longato, S. Epithelial and muscular regionalization of the human developing anorectum. Anat. Rec. 2007, 290, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Knol, J.; Keller, D.S. Total Mesorectal Excision Technique-Past, Present, and Future. Clin. Colon Rectal Surg. 2020, 33, 134–143. [Google Scholar] [CrossRef]
- Heald, R.J. A new approach to rectal cancer. Br. J. Hosp. Med. 1979, 22, 277–281. [Google Scholar]
- Memon, M.A.; Awaiz, A.; Yunus, R.M.; Memon, B.; Khan, S. Meta-analysis of histopathological outcomes of laparoscopic assisted rectal resection (LARR) vs open rectal resection (ORR) for carcinoma. Am. J. Surg. 2018, 216, 1004–1015. [Google Scholar] [CrossRef]
- Chen, Y.T.; Kiu, K.T.; Yen, M.H.; Chang, T.C. Comparison of the short-term outcomes in lower rectal cancer using three different surgical techniques: Transanal total mesorectal excision (TME), laparoscopic TME, and open TME. Asian J. Surg. 2019, 42, 674–680. [Google Scholar] [CrossRef]
- Aselmann, H.; Kersebaum, J.N.; Bernsmeier, A.; Beckmann, J.H.; Möller, T.; Egberts, J.H.; Schafmayer, C.; Röcken, C.; Becker, T. Robotic-assisted total mesorectal excision (TME) for rectal cancer results in a significantly higher quality of TME specimen compared to the laparoscopic approach—report of a single-center experience. Int. J. Colorectal Dis. 2018, 33, 1575–1581. [Google Scholar] [CrossRef]
- Hol, J.C.; van Oostendorp, S.E.; Tuynman, J.B.; Sietses, C. Long-term oncological results after transanal total mesorectal excision for rectal carcinoma. Tech. Coloproctol. 2019, 23, 903–911. [Google Scholar] [CrossRef]
- Kiyomatsu, T.; Ishihara, S.; Murono, K.; Otani, K.; Yasuda, K.; Nishikawa, T.; Tanaka, T.; Hata, K.; Kawai, K.; Nozawa, H.; et al. Anatomy of the middle rectal artery: A review of the historical literature. Surg. Today 2017, 47, 14–19. [Google Scholar] [CrossRef]
- Kusters, M.; Uehara, K.; van de Velde, C.J.H.; Moriya, Y. Is There Any Reason to Still Consider Lateral Lymph Node Dissection in Rectal Cancer? Rationale and Technique. Clin. Colon Rectal Surg. 2017, 30, 346–356. [Google Scholar] [PubMed]
- Williamson, J.S.; Quyn, A.J.; Sagar, P.M. Rectal cancer lateral pelvic sidewall lymph nodes: A review of controversies and management. Br. J. Surg. 2020, 107, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Heald, R.J. The “Holy Plane” of rectal surgery. J. R. Soc. Med. 1988, 81, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Stelzner, S.; Heinze, T.; Nikolouzakis, T.K.; Mees, S.T.; Witzigmann, H.; Wedel, T. Perirectal Fascial Anatomy. Dis. Colon Rectum. 2021, 64, 91–102. [Google Scholar] [CrossRef]
- Stelzner, S.; Böttner, M.; Kupsch, J.; Kneist, W.; Quirke, P.; West, N.P.; Witzigmann, H.; Wedel, T. Internal anal sphincter nerves—A macroanatomical and microscopic description of the extrinsic autonomic nerve supply of the internal anal sphincter. Colorectal Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2018, 20, O7–O16. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M. Cancer permeates locally within ontogenetic compartments: Clinical evidence and implications for cancer surgery. Future Oncol. 2012, 8, 29–36. [Google Scholar] [CrossRef]
- Höckel, M.; Horn, L.C.; Manthey, N.; Braumann, U.D.; Wolf, U.; Teichmann, G.; Frauenschläger, K.; Dornhöfer, N.; Einenkel, J. Resection of the embryologically defined uterovaginal (Müllerian) compartment and pelvic control in patients with cervical cancer: A prospective analysis. Lancet Oncol. 2009, 10, 683–692. [Google Scholar] [CrossRef]
- Chiantera, V.; Vizzielli, G.; Lucidi, A.; Gallotta, V.; Petrillo, M.; Legge, F.; Fagotti, A.; Sehouli, J.; Scambia, G.; Muallem, M.Z. Laparoscopic radical hysterectomy in cervical cancer as total mesometrial resection (L-TMMR): A multicentric experience. Gynecol. Oncol. 2015, 139, 47–51. [Google Scholar] [CrossRef]
- Kimmig, R.; Wimberger, P.; Buderath, P.; Aktas, B.; Iannaccone, A.; Heubner, M. Definition of compartment-based radical surgery in uterine cancer: Radical hysterectomy in cervical cancer as “total mesometrial resection (TMMR)” by M Höckel translated to robotic surgery (rTMMR). World J. Surg. Oncol. 2013, 11, 1–15. [Google Scholar] [CrossRef]
- Höckel, M.; Horn, L.C.; Fritsch, H. Association between the mesenchymal compartment of uterovaginal organogenesis and local tumour spread in stage IB-IIB cervical carcinoma: A prospective study. Lancet Oncol. 2005, 6, 751–756. [Google Scholar] [CrossRef]
- Höckel, M.; Wolf, B.; Schmidt, K.; Mende, M.; Aktas, B.; Kimmig, R.; Dornhöfer, N.; Horn, L.C. Surgical resection based on ontogenetic cancer field theory for cervical cancer: Mature results from a single-centre, prospective, observational, cohort study. Lancet Oncol. 2019, 20, 1316–1326. [Google Scholar] [CrossRef]
- Höckel, M.; Horn, L.-C.; Tetsch, E.; Einenkel, J. Pattern analysis of regional spread and therapeutic lymph node dissection in cervical cancer based on ontogenetic anatomy. Gynecol. Oncol. 2012, 125, 168–174. [Google Scholar] [CrossRef]
- Ates, M.; Kinaci, E.; Kose, E.; Soyer, V.; Sarici, B.; Cuglan, S.; Korkmaz, F.; Dirican, A. Corona mortis: In vivo anatomical knowledge and the risk of injury in totally extraperitoneal inguinal hernia repair. Hernia 2016, 20, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Sakuragi, N.; Murakami, G.; Konno, Y.; Kaneuchi, M.; Watari, H. Nerve-sparing radical hysterectomy in the precision surgery for cervical cancer. J. Gynecol. Oncol. 2020, 31, e49. [Google Scholar] [CrossRef] [PubMed]
- Osmonov, D.K.; Boller, A.; Aksenov, A.; Naumann, M.; Jünemann, K.P. “intermediate-risk-” und “high-risk-Prostatakarzinompatienten”: Klinische Bedeutung der ausgedehnten Lymphadenektomie. Urol. Ausg. A 2013, 52, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Touijer, K.A.; Ahallal, Y.; Guillonneau, B.D. Indications for and anatomical extent of pelvic lymph node dissection for prostate cancer: Practice patterns of uro-oncologists in North America. Urol. Oncol. 2013, 31, 1517–1521.e1–2. [Google Scholar] [CrossRef] [PubMed]
- García-Perdomo, H.A.; Correa-Ochoa, J.J.; Contreras-García, R.; Daneshmand, S. Effectiveness of extended pelvic lymphadenectomy in the survival of prostate cancer: A systematic review and meta-analysis. Cent. Eur. J. Urol. 2018, 71, 262–269. [Google Scholar]
- Osmonov, D.K.; Aksenov, A.V.; Boller, A.; Kalz, A.; Heimann, D.; Janssen, I.; Jünemann, K.-P. Extended salvage pelvic lymph node dissection in patients with recurrent prostate cancer. Adv. Urol. 2014, 2014, 321619. [Google Scholar] [CrossRef]
- Osmonov, D.K.; Wang, C.; Hoenle, J.; Aksenov, A.; Hamann, C.; Naumann, C.M.; Juenemann, K.P. Extended lymphadenectomy "step by step" in patients undergoing radical prostatectomy. Urology 2011, 77, 969–974. [Google Scholar] [CrossRef]
- Maderthaner, L.; Furrer, M.A.; Studer, U.E.; Burkhard, F.C.; Thalmann, G.N.; Nguyen, D.P. More extended lymph node dissection template at radical prostatectomy detects metastases in the common iliac region and in the fossa of Marcille. BJU Int. 2018, 121, 725–731. [Google Scholar] [CrossRef]
- Bando, Y.; Hinata, N.; Terakawa, T.; Furukawa, J.; Harada, K.; Nakano, Y.; Fujisawa, M. Diagnostic and therapeutic value of pelvic lymph node dissection in the fossa of Marcille in patients with clinically localized high-risk prostate cancer: Histopathological and molecular analyses. Prostate 2020, 80, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Walsh, P.C. The discovery of the cavernous nerves and development of nerve sparing radical retropubic prostatectomy. J. Urol. 2007, 177, 1632–1635. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.; Francis, K.E.; Solomon, M.J.; Ramsey-Stewart, G.; Austin, K.K.S.; Koh, C. Triangle of Marcille: The anatomical gateway to lateral pelvic exenteration. ANZ J. Surg. 2017, 87, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Benedix, F.; Lippert, H.; Meyer, F. Lymphokutane Fisteln, Chylaszites sowie Chylothorax im Komplikationsspektrum chirurgischer Eingriffe: Ursachen, Diagnostik und Therapie. Zent. Für Chir. 2007, 132, 529–538. [Google Scholar] [CrossRef]
- Baiocchi, G.; Faloppa, C.C.; Araujo, R.L.C.; Fukazawa, E.M.; Kumagai, L.Y.; Menezes, A.N.O.; Badiglian-Filho, L. Chylous ascites in gynecologic malignancies: Cases report and literature review. Arch. Gynecol. Obstet. 2010, 281, 677–681. [Google Scholar] [CrossRef]
- Höckel, M. Morphogenetic fields of embryonic development in locoregional cancer spread. Lancet Oncol. 2015, 16, e148–e151. [Google Scholar] [CrossRef]
- Van der Putte, S.C. The development of the lymphatic system in man. Adv. Anat. Embryol. Cell Biol. 1975, 51, 3–60. [Google Scholar] [PubMed]
- Yang, X.; Yang, S.; Hu, T.; Gu, C.; Wei, M.; Deng, X.; Wang, Z.; Zhou, Z. What is the role of lateral lymph node dissection in rectal cancer patients with clinically suspected lateral lymph node metastasis after preoperative chemoradiotherapy? A meta-analysis and systematic review. Cancer Med. 2020, 9, 4477–4489. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Fujita, S.; Ota, M.; Mizusawa, J.; Shida, D.; Kanemitsu, Y.; Ito, M.; Shiomi, A.; Komori, K.; Ohue, M.; et al. Long-term follow-up of the randomized trial of mesorectal excision with or without lateral lymph node dissection in rectal cancer (JCOG0212). Br. J. Surg. 2020, 107, 586–594. [Google Scholar] [CrossRef]
- Höckel, M.; Hentschel, B.; Horn, L.C. Association between developmental steps in the organogenesis of the uterine cervix and locoregional progression of cervical cancer: A prospective clinicopathological analysis. Lancet Oncol. 2014, 15, 445–456. [Google Scholar] [CrossRef]
- Kimmig, R.; Iannaccone, A.; Buderath, P.; Aktas, B.; Wimberger, P.; Heubner, M. Definition of compartment based radical surgery in uterine cancer-part I: Therapeutic pelvic and periaortic lymphadenectomy by Michael höckel translated to robotic surgery. ISRN Obstet. Gynecol. 2013, 2013, 297921. [Google Scholar] [CrossRef] [PubMed]
- Reiffenstuhl, G. Das Lymphsystem des Weiblichen Genitale; Urband & Schwarzenberg: Amsterdam, The Netherlands, 1957. [Google Scholar]
- Xia, X.; Xu, H.; Wang, Z.; Liu, R.; Hu, T.; Li, S. Analysis of Prognostic Factors Affecting the Outcome of Stage IB-IIB Cervical Cancer Treated by Radical Hysterectomy and Pelvic Lymphadenectomy. Am. J. Clin. Oncol. Cancer Clin. Trials 2016, 39, 604–608. [Google Scholar] [CrossRef]
- Wolf, B.; Ganzer, R.; Stolzenburg, J.U.; Hentschel, B.; Horn, L.C.; Höckel, M. Extended mesometrial resection (EMMR): Surgical approach to the treatment of locally advanced cervical cancer based on the theory of ontogenetic cancer fields. Gynecol. Oncol. 2017, 146, 292–298. [Google Scholar] [CrossRef]
- Höckel, M. Long-Term Experience with (Laterally) Extended Endopelvic Resection (LEER) in Relapsed Pelvic Malignancies. Curr. Oncol. Rep. 2015, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Fossati, N.; Willemse, P.P.M.; Van den Broeck, T.; van den Bergh, R.C.N.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; De Santis, M.; et al. The Benefits and Harms of Different Extents of Lymph Node Dissection During Radical Prostatectomy for Prostate Cancer: A Systematic Review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; van den Bergh, R.C.N.; Gandaglia, G.; Ost, P.; Surcel, C.I.; Sooriakumaran, P.; Montorsi, F.; Graefen, M.; van der Poel, H.; de la Taille, A.; et al. Effect of Extended Pelvic Lymph Node Dissection on Oncologic Outcomes in Patients with D’Amico Intermediate and High Risk Prostate Cancer Treated with Radical Prostatectomy: A Multi-Institutional Study. J. Urol. 2020, 203, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Bandini, M.; Marchioni, M.; Nazzani, S.; Tian, Z.; Pompe, R.S.; Fossati, N.; Briganti, A.; Saad, F.; Shariat, S.F.; et al. Extent of lymph node dissection improves survival in prostate cancer patients treated with radical prostatectomy without lymph node invasion. Prostate 2018, 78, 469–475. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Kinugasa, Y.; Shiomi, A.; Sato, S.; Yamakawa, Y.; Kagawa, H.; Tomioka, H.; Mori, K. Learning curve for robotic-assisted surgery for rectal cancer: Use of the cumulative sum method. Surg. Endosc. 2015, 29, 1679–1685. [Google Scholar] [CrossRef]
- Yuh, B.E.; Ruel, N.H.; Mejia, R.; Wilson, C.M.; Wilson, T.G. Robotic extended pelvic lymphadenectomy for intermediate- and high-risk prostate cancer. Eur. Urol. 2012, 61, 1004–1010. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayer, A.; Heinze, T.; Alkatout, I.; Osmonov, D.; Stelzner, S.; Wedel, T. Embryological Development and Topographic Anatomy of Pelvic Compartments—Surgical Relevance for Pelvic Lymphonodectomy. J. Clin. Med. 2021, 10, 708. https://doi.org/10.3390/jcm10040708
Bayer A, Heinze T, Alkatout I, Osmonov D, Stelzner S, Wedel T. Embryological Development and Topographic Anatomy of Pelvic Compartments—Surgical Relevance for Pelvic Lymphonodectomy. Journal of Clinical Medicine. 2021; 10(4):708. https://doi.org/10.3390/jcm10040708
Chicago/Turabian StyleBayer, Andreas, Tillmann Heinze, Ibrahim Alkatout, Daniar Osmonov, Sigmar Stelzner, and Thilo Wedel. 2021. "Embryological Development and Topographic Anatomy of Pelvic Compartments—Surgical Relevance for Pelvic Lymphonodectomy" Journal of Clinical Medicine 10, no. 4: 708. https://doi.org/10.3390/jcm10040708
APA StyleBayer, A., Heinze, T., Alkatout, I., Osmonov, D., Stelzner, S., & Wedel, T. (2021). Embryological Development and Topographic Anatomy of Pelvic Compartments—Surgical Relevance for Pelvic Lymphonodectomy. Journal of Clinical Medicine, 10(4), 708. https://doi.org/10.3390/jcm10040708