
High Agreement between Barrett Universal II Calculations with and without Utilization of Optional Biometry Parameters

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Visual-Basic Software for Applications Code
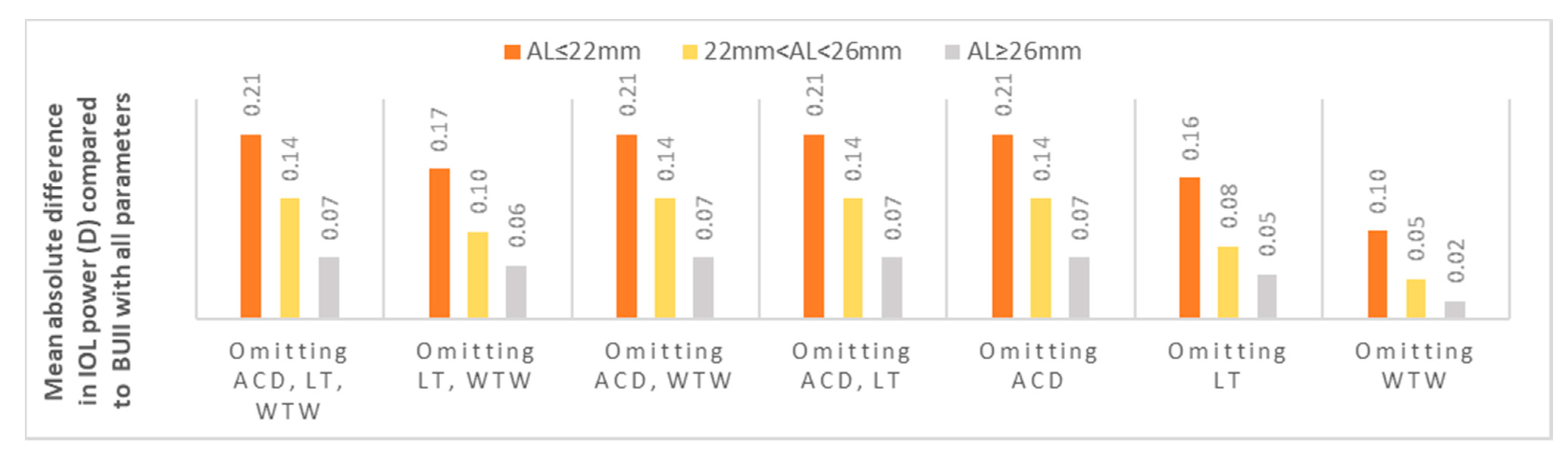
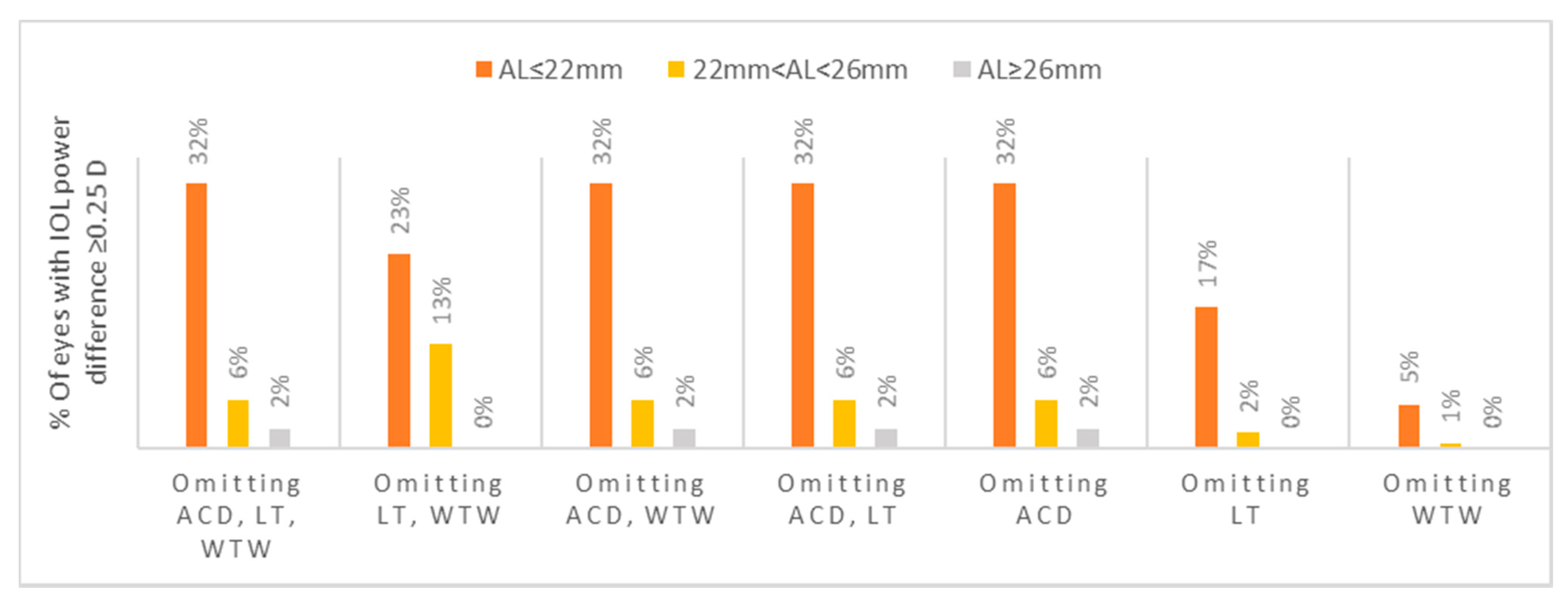
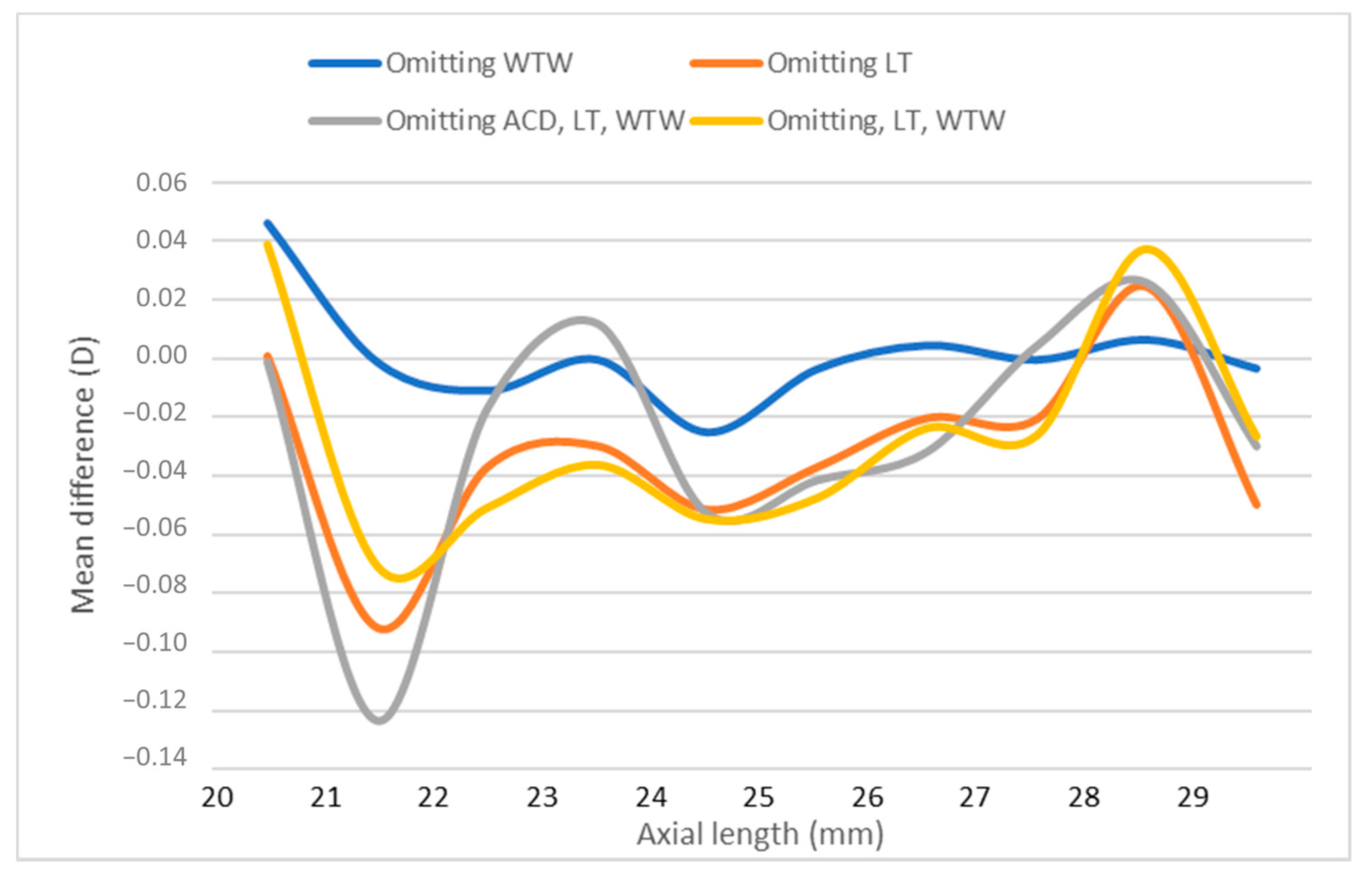
2.3. Axial Length Sub-Analysis
2.4. Power Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Agreement between Partial and Full Biometry Data in Eyes with Short, Intermediate and Long Axial Length
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colin, J.; El Kebir, S.; Eydoux, E.; Hoang-Xuan, T.; Rozot, P.; Weiser, M. Assessment of patient satisfaction with outcomes of and ophthalmic care for cataract surgery. J. Cataract. Refract. Surg. 2010, 36, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Pager, C.K. Expectations and Outcomes in Cataract Surgery: A Prospective Test of 2 Models of Satisfaction. Arch. Ophthalmol. 2004, 122, 1788–1792. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.S.; Chee, Y.E.; Haddadin, R.I.; Veldman, P.B.; Borboli-Gerogiannis, S.; Brauner, S.C.; Chang, K.K.; Chen, S.H.; Gardiner, M.F.; Greenstein, S.H.; et al. Achieving Target Refraction after Cataract Surgery. Ophthalmology 2014, 121, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Melles, R.B.; Holladay, J.T.; Chang, W.J. Accuracy of Intraocular Lens Calculation Formulas. Ophthalmology 2018, 125, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Cooke, D.L.; Cooke, T.L. Comparison of 9 intraocular lens power calculation formulas. J. Cataract. Refract. Surg. 2016, 42, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Reitblat, O.; Levy, A.; Kleinmann, G.; Lerman, T.T.; Assia, E.I. Intraocular lens power calculation for eyes with high and low average keratometry readings: Comparison between various formulas. J. Cataract. Refract. Surg. 2017, 43, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.V.; Hodge, C.; Sutton, G.; Lawless, M.; Contributors to the Vision Eye Institute IOL Outcomes Registry. Comparison of Hill-radial basis function, Barrett Universal and current third generation formulas for the calculation of intraocular lens power during cataract surgery. Clin. Exp. Ophthalmol. 2017, 46, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Shajari, M.; Kolb, C.M.; Petermann, K.; Böhm, M.; Herzog, M.; De’Lorenzo, N.; Schönbrunn, S.; Kohnen, T. Comparison of 9 modern intraocular lens power calculation formulas for a quadrifocal intraocular lens. J. Cataract. Refract. Surg. 2018, 44, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.X.; Van Heerden, A.; Atik, A.; Petsoglou, C. Intraocular lens power formula accuracy: Comparison of 7 formulas. J. Cataract. Refract. Surg. 2016, 42, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Muniz Castro, H.; Tai, A.X.; Sampson, S.J.; Wade, M.; Farid, M.; Garg, S. Accuracy of Intraocular Lens Power Calculation Using Anterior Chamber Depth from Two Devices with Barrett Universal II Formula. J. Ophthalmol. 2019, 2019, 8172615. [Google Scholar] [CrossRef] [PubMed]
- VanderVeen, D.K.; Nizam, A.; Lynn, M.J.; Bothun, E.D.; McClatchey, S.K.; Weakley, D.R.; DuBois, L.G.; Lambert, S.R.; Infant Aphakia Treatment Study Group. Predictability of intraocular lens calculation and early refractive status: The Infant Aphakia Treatment Study. Arch. Ophthalmol. 2012, 130, 293–299. [Google Scholar] [CrossRef]
- Turnbull, A.M.J.; Barrett, G.D. Using the first-eye prediction error in cataract surgery to refine the refractive outcome of the second eye. J. Cataract. Refract. Surg. 2019, 45, 1239–1245. [Google Scholar] [CrossRef]
- Connell, B.; Kane, J.X. Comparison of the Kane formula with existing formulas for intraocular lens power selection. BMJ Open Ophthalmol. 2019, 4, e000251. [Google Scholar] [CrossRef] [PubMed]
- Moshirfar, M.; Buckner, B.; Ronquillo, Y.C.; Hofstedt, D. Biometry in cataract surgery: A review of the current literature. Curr. Opin. Ophthalmol. 2019, 30, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Sheard, R. Optimising biometry for best outcomes in cataract surgery. Eye 2013, 28, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Maharana, P.K.; Singhi, S.; Aron, N.; Patil, M. Descemet stripping automated endothelial keratoplasty. Indian J. Ophthalmol. 2017, 65, 198–209. [Google Scholar] [CrossRef]
- Srivannaboon, S.; Chirapapaisan, C.; Chirapapaisan, N.; Lertsuwanroj, B.; Chongchareon, M. Accuracy of Holladay 2 formula using IOLMaster parameters in the absence of lens thickness value. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 2563–2567. [Google Scholar] [CrossRef]
- Olsen, T. Calculation of intraocular lens power: A review. Acta Ophthalmol. Scand. 2007, 85, 472–485. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | AL (mm) | K1 (D) | K2 (D) | ACD (mm) | LT (mm) | WTW (mm) | |
|---|---|---|---|---|---|---|---|
| Mean | 65.16 | 23.75 | 43.63 | 44.86 | 3.15 | 4.48 | 11.86 |
| SD | 17.38 | 1.88 | 2.03 | 2.07 | 0.48 | 0.49 | 0.50 |
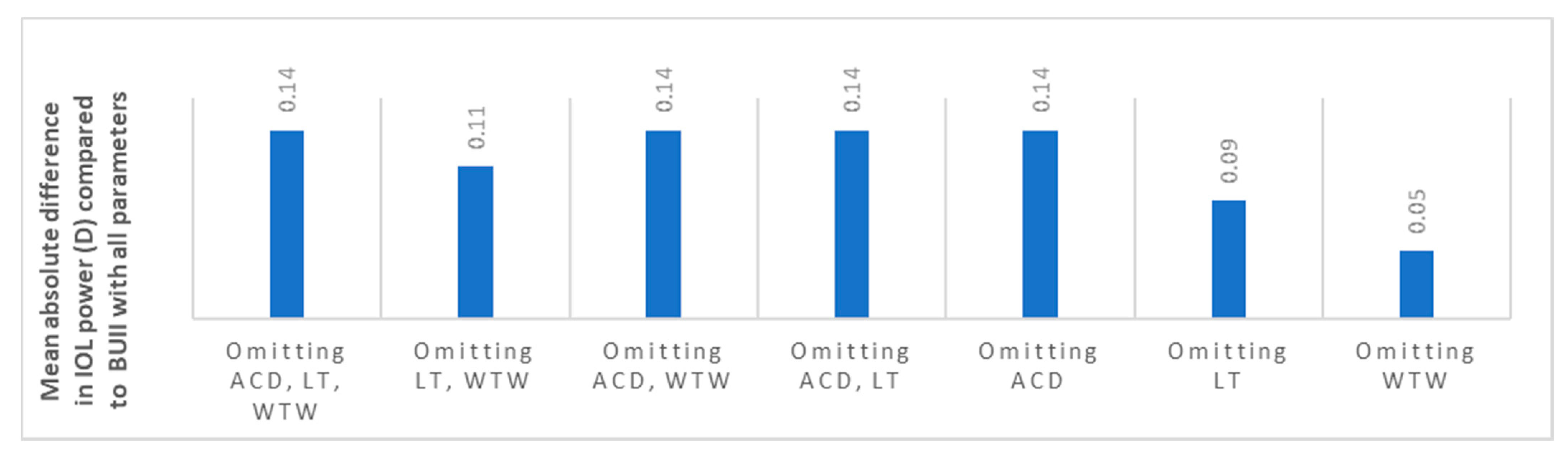
| Parameters Used | Mean Difference between Partial Biometry and All BUII Parameters (SD); CI; p-Value | Mean Absolute Difference between Partial Biometry and All BUII Parameters (SD); CI; p-Value |
|---|---|---|
| All BUII parameters | NA | NA |
| AL, K | 0.03 (0.18); 0.01–0.05; <0.001 | 0.14 (0.12); 0.13–0.15; <0.001 |
| AL, K, ACD | 0.04 (0.13); 0.03–0.05; <0.001 | 0.11 (0.09); 0.10–0.11; <0.001 |
| AL, K, LT | 0.03 (0.18); 0.01–0.05; < 0.001 | 0.14 (0.12); 0.13–0.15; <0.001 |
| AL, K, WTW | 0.03 (0.18); 0.01–0.05; <0.001 | 0.14 (0.12); 0.13–0.15; <0.001 |
| AL, K, LT, WTW | 0.03 (0.18); 0.01–0.05; <0.001 | 0.14 (0.12); 0.13–0.15; <0.001 |
| AL, K, ACD, WTW | 0.04 (0.12); 0.03–0.05; <0.001 | 0.09 (0.08); 0.08–0.10; <0.001 |
| AL, K, ACD, LT | 0.00 (0.11); −0.01–0.01; 0.41 | 0.05 (0.09); 0.04–0.06; <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vega, Y.; Gershoni, A.; Achiron, A.; Tuuminen, R.; Weinberger, Y.; Livny, E.; Nahum, Y.; Bahar, I.; Elbaz, U. High Agreement between Barrett Universal II Calculations with and without Utilization of Optional Biometry Parameters. J. Clin. Med. 2021, 10, 542. https://doi.org/10.3390/jcm10030542
Vega Y, Gershoni A, Achiron A, Tuuminen R, Weinberger Y, Livny E, Nahum Y, Bahar I, Elbaz U. High Agreement between Barrett Universal II Calculations with and without Utilization of Optional Biometry Parameters. Journal of Clinical Medicine. 2021; 10(3):542. https://doi.org/10.3390/jcm10030542
Chicago/Turabian StyleVega, Yakov, Assaf Gershoni, Asaf Achiron, Raimo Tuuminen, Yehonatan Weinberger, Eitan Livny, Yoav Nahum, Irit Bahar, and Uri Elbaz. 2021. "High Agreement between Barrett Universal II Calculations with and without Utilization of Optional Biometry Parameters" Journal of Clinical Medicine 10, no. 3: 542. https://doi.org/10.3390/jcm10030542
APA StyleVega, Y., Gershoni, A., Achiron, A., Tuuminen, R., Weinberger, Y., Livny, E., Nahum, Y., Bahar, I., & Elbaz, U. (2021). High Agreement between Barrett Universal II Calculations with and without Utilization of Optional Biometry Parameters. Journal of Clinical Medicine, 10(3), 542. https://doi.org/10.3390/jcm10030542