
Mortality and Medical Complications of Subtrochanteric Fracture Fixation

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Patients and Methods
Statistical Analysis
3. Results
3.1. Patient Demographics and Mechanism of Injury
3.2. Hospital Stay
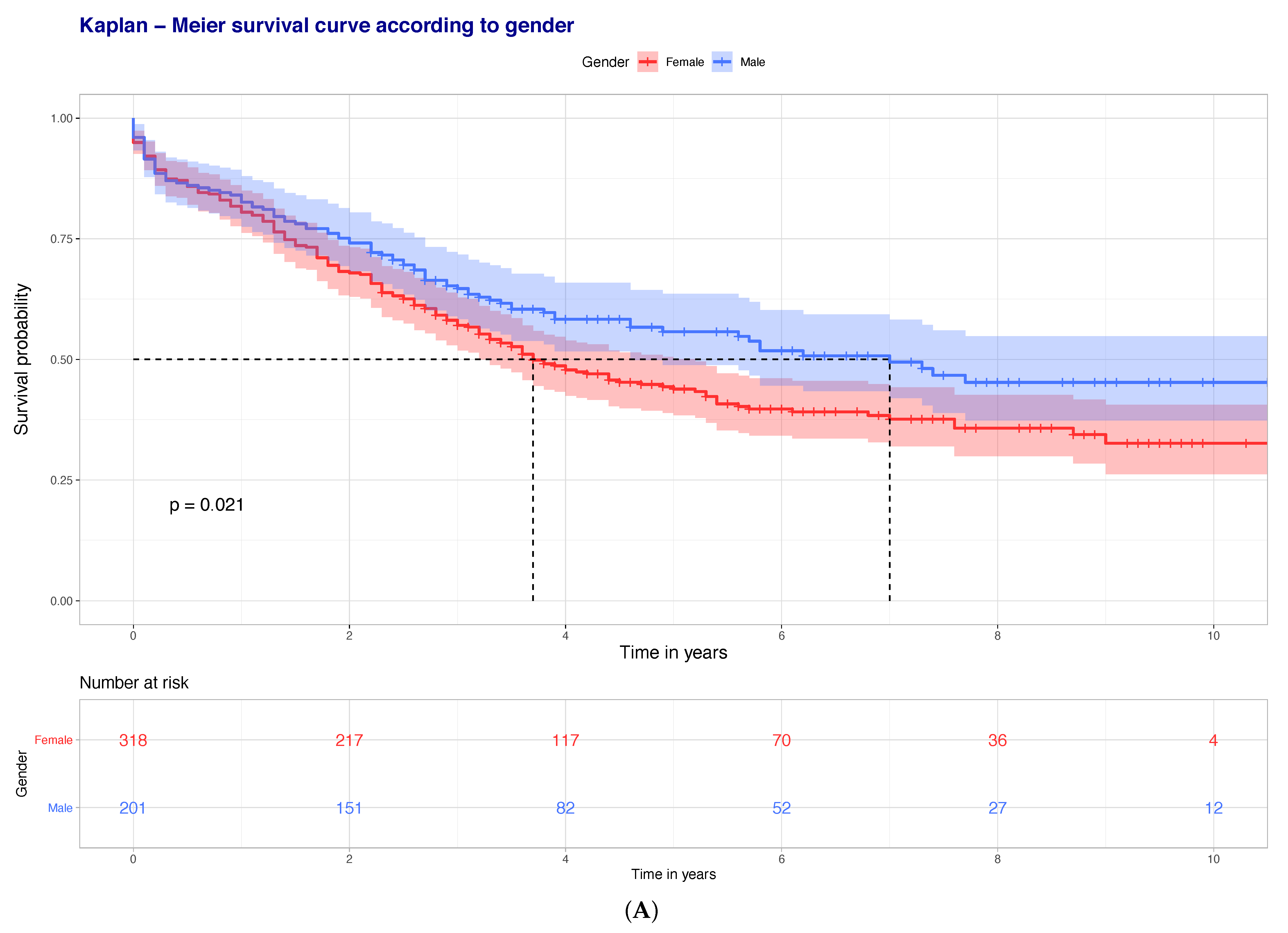
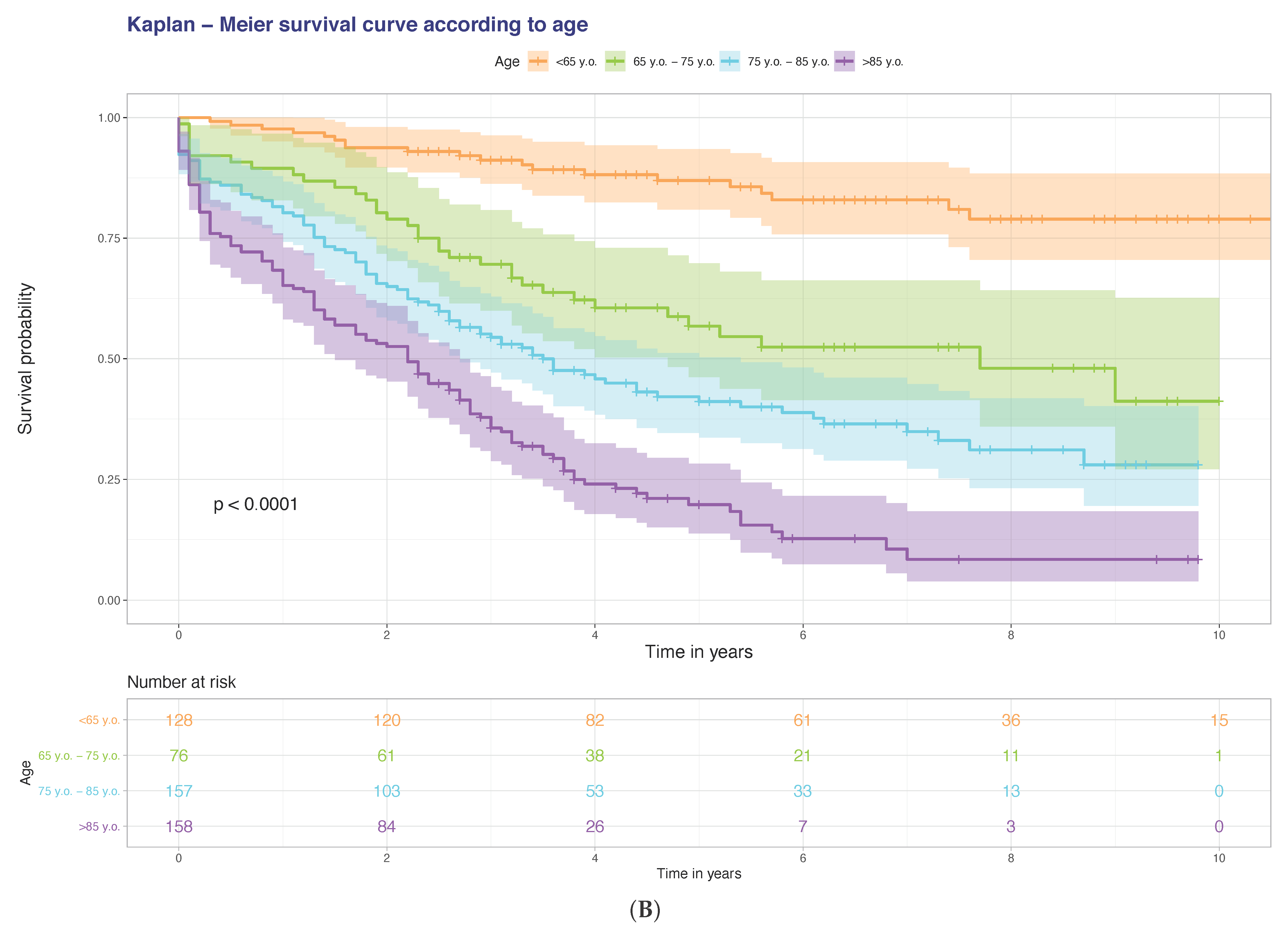
3.3. Mortality
3.4. Venous Thromboembolism
3.5. Myocardial Infarction/Cerebrovascular Accidents
3.6. Hospital Acquired Pneumonia
3.7. Post-Operative Delirium
3.8. Weekend Effect
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Demographics | All Patients | Alive | Deceased | p-value | |
| Total number | 519 | 429 | 90 | - | |
| Age (years) | 73.26 (19.47) | 70.74 (20.13) | 85.27 (8.99) | <0.001 | |
| Age < 65 | 128 | 125 (29.1%) | 3 (3.3%) | <0.001 | |
| Age 65–<75 | 76 | 68(15.9%) | 8 (8.9%) | 0.125 | |
| Age ≥ 75 | 315 | 236 (55.0%) | 79 (87.8%) | <0.001 | |
| Gender | Female | 318 | 260 (60.6%) | 58 (64.4%) | 0.575 |
| Male | 201 | 169 (39.4%) | 32 (35.6%) | ||
| Injury Characteristics | All Patients | Alive | Deceased | p-value | |
| Mechanism of Injury | Low energy | 430 | 344 (80.2%) | 86 (95.5%) | 0.001 |
| High energy | 89 | 85 (19.8%) | 4 (4.5%) | ||
| Isolated | 435 | 356 (83.0%) | 79 (87.8%) | 0.334 | |
| ISS > 16 | 35 | 34 (7.9%) | 1 (1.1%) | 0.046 | |
| Side | Left | 272 | 219 (51.0%) | 53 (58.9%) | 0.216 |
| Right | 247 | 210 (49.0%) | 37 (41.1%) | ||
| Open fracture | 7 | 7 (1.6%) | 0 (0.0%) | 0.473 | |
| Medical Comorbidities | All Patients | Alive | Deceased | p-value | |
| ASA | 1 | 48 | 48 (11.2%) | 0 (0.0%) | <0.001 |
| 2 | 134 | 126 (29.4%) | 8 (8.9%) | ||
| 3 | 257 | 204 (47.6%) | 53 (58.9%) | ||
| 4 | 80 | 51 (11.9%) | 29 (32.2%) | ||
| Charlson comorbidity score | 5.07 (3.01) | 4.65 (3.00) | 7.07 (2.12) | <0.001 | |
| Charlson comorbidity score ≥ 6 | 239 | 163 (38.0%) | 69 (76.7%) | <0.001 | |
| Diabetes | 69 | 56 (13.1%) | 13 (14.4%) | 0.855 | |
| Steroids | 21 | 17 (4.0%) | 4 (4.4%) | 1 | |
| Malignancy | 103 | 80 (18.6%) | 23 (25.6%) | 0.178 | |
| Dementia | 120 | 72 (16.8%) | 48 (53.3%) | <0.001 | |
| Hypoalbuminaemia | 335 | 240 (63.8%) | 77 (91.7%) | <0.001 | |
| Osteoporosis | All Patients | Alive | Deceased | p-value | |
| Bisphosphonates pre-admission | 87 | 76 (17.7%) | 11 (12.2%) | 0.266 | |
| Bisphosphonates on discharge | 127 | 113 (26.3%) | 14 (24.1%) | 0.842 | |
| Calcium/Vitamin D pre-admission | 149 | 122 (28.4%) | 27 (30.0%) | 0.865 | |
| Calcium/Vitamin D on discharge | 239 | 204 (47.6%) | 35 (60.3%) | 0.091 | |
| Vitamin D loading on admission | 82 | 70 (16.3%) | 12 (20.7%) | 0.517 | |
| Fragility Fractures Before | 83 | 83 (19.4%) | 27 (30.0%) | 0.036 | |
| Fragility Fractures After | 37 | 78 (18.2%) | 5 (5.6%) | 0.005 | |
| Social History | All Patients | Alive | Deceased | p-value | |
| Smoking | 103 | 92 (21.4%) | 11 (12.2%) | 0.064 | |
| Alcohol >10 units/week | 96 | 87 (20.3%) | 9 (10.0%) | 0.033 | |
| Pre-operative Mobility | 0.007 | ||||
| Independent | 271 | 237 (55.2%) | 34 (37.8%) | ||
| Stick(s)/Crutch(es) | 90 | 66 (15.4%) | 24 (26.7%) | ||
| Frame | 133 | 108 (25.2%) | 25 (27.8%) | ||
| Wheelchair/Hoisted | 25 | 18 (4.2%) | 7 (7.8%) | ||
| Frequent falls | 146 | 108 (25.2%) | 38 (42.2%) | 0.001 | |
| Operation Characteristics | All Patients | Alive | Deceased | p-value | |
| Operation in less than 48 h | 415 | 343 (80.0%) | 72 (80.0%) | 0.871 | |
| Simultaneous procedures | 36 | 34 (7.9%) | 2 (2.2%) | 0.088 | |
| Use of cerclage wires | 63 | 56 (13.1%) | 7 (7.8%) | 0.224 | |
| Surgical time (min) ** | 111.84 (45.60) | 112.66 (45.90) | 107.89 (44.20) | 0.37 | |
| Anaesthetic time (min) *** | 48.30 (21.93) | 48.39 (22.46) | 47.92 (19.29) | 0.855 | |
| Time from induction to recovery (min) | 178.87 (50.59) | 180.04 (50.54) | 173.3 (50.78) | 0.254 | |
| Level of First Surgeon | 0.961 | ||||
| Registrar | 309 | 255 (59.7%) | 54 (60.7%) | ||
| Consultant | 207 | 172 (40.3%) | 35 (39.3%) | ||
| Level of Senior Surgeon Present | 286 | 234 (54.8%) | 52 (58.4%) | 0.611 | |
| Registrar | 230 | 193 (45.2%) | 37 (41.6%) | ||
| Consultant | |||||
| Complications | All Patients | Alive | Deceased | p-value | |
| Nail Related Complications * | 95 | 89 (20.7%) | 6 (6.7%) | 0.003 | |
| Failure at lag screw junction | 22 | 21 (4.9%) | 1 (1.1%) | 0.183 | |
| Self-dynamisation | 22 | 21 (4.9%) | 1 (1.1%) | 0.183 | |
| Cut-out | 13 | 13 (3.0%) | 0 (0.0%) | 0.193 | |
| Non-union | 77 | 73 (17.0%) | 4 (4.4%) | 0.005 | |
| Peri-implant fracture | 13 | 11 (2.6%) | 2 (2.2%) | 1 | |
| HAP/CAP | 95 | 61 (14.2%) | 34 (37.8%) | <0.001 | |
| UTI | 75 | 59 (13.8%) | 16 (17.8%) | 0.411 | |
| Wound infection | Superficial | 18 | 16 (3.7%) | 2 (2.2%) | 0.409 |
| Deep | 15 | 14 (3.3%) | 1 (1.1%) | ||
| CKD Stage pre-operatively | <0.001 | ||||
| Mild | 355 | 308 (73.2%) | 47 (54.0%) | ||
| Moderate/Severe | 153 | 113 (26.8%) | 40 (46.0%) | ||
| CKD Stage post-operatively | <0.001 | ||||
| Mild | 364 | 317 (76.0%) | 47 (54.0%) | ||
| Moderate/Severe | 140 | 100 (24.0%) | 40 (46.0%) | ||
| Pre-operative Transfusion | 44 | 36 (8.4%) | 8 (9.0%) | 1 | |
| Post-operative Transfusion(48 h) | 12 | 208 (48.6%) | 60 (67.4%) | 0.001 | |
| Post-operative Transfusion (total) | 330 | 264 (61.7%) | 66 (74.2%) | 0.035 | |
| Hb Drop (g/L) | 45.83 (18.46) | 45.56 (18.11) | 47.11 (20.06) | 0.477 | |
| VTE | No | 101 | 82 (82.8%) | 19 (90.5%) | 0.671 |
| DVT | 11 | 10 (10.1%) | 1 (4.8%) | ||
| PE | 8 | 7 (7.1%) | 1 (4.8%) | ||
| Hospital stay/Mortality | All Patients | Alive | Deceased | p-value | |
| HDU/ICU stay | 60 | 44 (10.3%) | 16 (17.8%) | 0.065 | |
| Total length of hospital stay (days) | 22.92 (19.08) | 22.5 (18.75) | 24.93 (20.60) | 0.271 | |
| Weekend admission | 169 (33.3%) | 133 (31.0%) | 36 (40.0%) | 0.125 | |
| Died within 30 days | 28 (31.1%) | 0 (0.0%) | 28 (31.1%) | <0.001 | |
References
- Coates, S.; Tanna, P.; Scott-Allen, E. Overview of the UK Population: August 2019; Office for National Statistics: Newport, UK, 2019. [Google Scholar]
- Colby, S.; Ortman, J.M. Projections of the Size and Composition of the US Population: 2014 to 2060; US Department of Commerce, Economics and Statistics Administration: Washington, DC, USA, 2015.
- Townsend, M. The Impact of an Ageing Population on End of Life Care Costs; London School of Economics: London, UK, 2016. [Google Scholar]
- BOAST 1 Version 2—Patients Sustaining a Fragility Hip Fracture. Available online: https://www.boa.ac.uk/resources/knowledge-hub/boast-1-pdf-1.html (accessed on 22 January 2021).
- Panteli, M.; Mauffrey, C.; Giannoudis, P.V. Subtrochanteric fractures: Issues and challenges. Injury 2017, 48, 2023–2026. [Google Scholar] [CrossRef]
- Loizou, C.L.; McNamara, I.; Ahmed, K.; Pryor, G.A.; Parker, M.J. Classification of subtrochanteric femoral fractures. Injury 2010, 41, 739–745. [Google Scholar] [CrossRef]
- Barbosa de Toledo Lourenco, P.R.; Pires, R.E. Subtrochanteric fractures of the femur: Update. Rev. Bras. Ortop 2016, 51, 246–253. [Google Scholar] [CrossRef][Green Version]
- Miller, S.D.; Burkart, B.; Damson, E.; Shrive, N.; Bray, R.C. The effect of the entry hole for an intramedullary nail on the strength of the proximal femur. J. Bone Jt. Surg. Br. Vol. 1993, 75, 202–206. [Google Scholar] [CrossRef]
- NHFD 2018 Annual Report. Available online: https://www.nhfd.co.uk/20/hipfractureR.nsf/docs/2018Report (accessed on 13 August 2019).
- Kannegaard, P.N.; van der Mark, S.; Eiken, P.; Abrahamsen, B. Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing 2010, 39, 203–209. [Google Scholar] [CrossRef]
- Mattisson, L.; Bojan, A.; Enocson, A. Epidemiology, treatment and mortality of trochanteric and subtrochanteric hip fractures: Data from the Swedish fracture register. BMC Musculoskelet Disord 2018, 19, 369. [Google Scholar] [CrossRef]
- Lunde, A.; Tell, G.S.; Pedersen, A.B.; Scheike, T.H.; Apalset, E.M.; Ehrenstein, V.; Sorensen, H.T. The Role of Comorbidity in Mortality After Hip Fracture: A Nationwide Norwegian Study of 38,126 Women With Hip Fracture Matched to a General-Population Comparison Cohort. Am. J. Epidemiol. 2019, 188, 398–407. [Google Scholar] [CrossRef]
- Pedersen, A.B.; Ehrenstein, V.; Szepligeti, S.K.; Lunde, A.; Lagerros, Y.T.; Westerlund, A.; Tell, G.S.; Sorensen, H.T. Thirty-five-year Trends in First-time Hospitalization for Hip Fracture, 1-year Mortality, and the Prognostic Impact of Comorbidity: A Danish Nationwide Cohort Study, 1980–2014. Epidemiology 2017, 28, 898–905. [Google Scholar] [CrossRef]
- Khan, M.A.; Hossain, F.S.; Ahmed, I.; Muthukumar, N.; Mohsen, A. Predictors of early mortality after hip fracture surgery. Int. Orthop. 2013, 37, 2119–2124. [Google Scholar] [CrossRef]
- Jurisson, M.; Raag, M.; Kallikorm, R.; Lember, M.; Uuskula, A. The impact of comorbidities on hip fracture mortality: A retrospective population-based cohort study. Arch. Osteoporos. 2017, 12, 76. [Google Scholar] [CrossRef]
- Chiu, H.C.; Chen, C.M.; Su, T.Y.; Chen, C.H.; Hsieh, H.M.; Hsieh, C.P.; Shen, D.L. Dementia predicted one-year mortality for patients with first hip fracture: A population-based study. Bone Jt. J. 2018, 100-B, 1220–1226. [Google Scholar] [CrossRef]
- Bai, J.; Zhang, P.; Liang, X.; Wu, Z.; Wang, J.; Liang, Y. Association between dementia and mortality in the elderly patients undergoing hip fracture surgery: A meta-analysis. J. Orthop Surg. Res. 2018, 13, 298. [Google Scholar] [CrossRef]
- Roche, J.J.; Wenn, R.T.; Sahota, O.; Moran, C.G. Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: Prospective observational cohort study. BMJ 2005, 331, 1374. [Google Scholar] [CrossRef]
- Edelmuth, S.; Sorio, G.N.; Sprovieri, F.A.A.; Gali, J.C.; Peron, S.F. Comorbidities, clinical intercurrences, and factors associated with mortality in elderly patients admitted for a hip fracture. Rev. Bras. Ortop. 2018, 53, 543–551. [Google Scholar] [CrossRef]
- Bohl, D.D.; Shen, M.R.; Hannon, C.P.; Fillingham, Y.A.; Darrith, B.; Della Valle, C.J. Serum Albumin Predicts Survival and Postoperative Course Following Surgery for Geriatric Hip Fracture. J. Bone Jt. Surg. Am. 2017, 99, 2110–2118. [Google Scholar] [CrossRef]
- Miyanishi, K.; Jingushi, S.; Torisu, T. Mortality after hip fracture in Japan: The role of nutritional status. J. Orthop. Surg. 2010, 18, 265–270. [Google Scholar] [CrossRef]
- Harrison, S.J.; Messner, J.; Leeder, D.J.; Stephenson, J.; Sidhom, S.A. Are Albumin Levels a Good Predictor of Mortality in Elderly Patients with Neck of Femur Fractures? J. Nutr. Health Aging. 2017, 21, 699–703. [Google Scholar] [CrossRef]
- Pimlott, B.J.; Jones, C.A.; Beaupre, L.A.; Johnston, D.W.; Majumdar, S.R. Prognostic impact of pre-operative albumin on short-term mortality and complications in patients with hip fracture. Arch. Gerontol. Geriatr. 2011, 53, 90–94. [Google Scholar] [CrossRef]
- Ryan, S.; Politzer, C.; Fletcher, A.; Bolognesi, M.; Seyler, T. Preoperative Hypoalbuminemia Predicts Poor Short-term Outcomes for Hip Fracture Surgery. Orthopedics 2018, 41, e789–e796. [Google Scholar] [CrossRef]
- Pedersen, A.B.; Ehrenstein, V.; Szepligeti, S.K.; Sorensen, H.T. Excess risk of venous thromboembolism in hip fracture patients and the prognostic impact of comorbidity. Osteoporos. Int. 2017, 28, 3421–3430. [Google Scholar] [CrossRef]
- Shin, W.C.; Lee, S.M.; Suh, K.T. Recent Updates of the Diagnosis and Prevention of Venous Thromboembolism in Patients with a Hip Fracture. Hip. Pelvis. 2017, 29, 159–167. [Google Scholar] [CrossRef]
- Li, Q.; Dai, B.; Xu, J.; Yao, Y.; Song, K.; Zhang, H.; Chen, D.; Jiang, Q. Can patients with femoral neck fracture benefit from preoperative thromboprophylaxis?: A prospective randomized controlled trial. Medicine 2017, 96, e7604. [Google Scholar] [CrossRef]
- Carpintero, P.; Caeiro, J.R.; Carpintero, R.; Morales, A.; Silva, S.; Mesa, M. Complications of hip fractures: A review. World J. Orthop 2014, 5, 402–411. [Google Scholar] [CrossRef]
- Bohsali, F.; Klimpl, D.; Baumgartner, R.; Sieber, F.; Eid, S.M. Effect of Heart Failure With Preserved Ejection Fraction on Perioperative Outcomes in Patients Undergoing Hip Fracture Surgery. J. Am. Acad. Orthop. Surg. 2019. [Google Scholar] [CrossRef]
- Pedersen, A.B.; Ehrenstein, V.; Szepligeti, S.K.; Sorensen, H.T. Hip Fracture, Comorbidity, and the Risk of Myocardial Infarction and Stroke: A Danish Nationwide Cohort Study, 1995–2015. J. Bone Min. Res. 2017, 32, 2339–2346. [Google Scholar] [CrossRef]
- Karaca, S.; Ayhan, E.; Kesmezacar, H.; Uysal, O. Hip fracture mortality: Is it affected by anesthesia techniques? Anesth. Res. Pr. 2012, 2012, 708754. [Google Scholar] [CrossRef]
- Bohl, D.D.; Sershon, R.A.; Saltzman, B.M.; Darrith, B.; Della Valle, C.J. Incidence, Risk Factors, and Clinical Implications of Pneumonia After Surgery for Geriatric Hip Fracture. J. Arthroplast. 2018, 33, 1552–1556. [Google Scholar] [CrossRef]
- Chang, S.C.; Lai, J.I.; Lu, M.C.; Lin, K.H.; Wang, W.S.; Lo, S.S.; Lai, Y.C. Reduction in the incidence of pneumonia in elderly patients after hip fracture surgery: An inpatient pulmonary rehabilitation program. Medicine 2018, 97, e11845. [Google Scholar] [CrossRef]
- Lawrence, V.A.; Hilsenbeck, S.G.; Noveck, H.; Poses, R.M.; Carson, J.L. Medical complications and outcomes after hip fracture repair. Arch. Intern. Med. 2002, 162, 2053–2057. [Google Scholar] [CrossRef]
- Henderson, C.Y.; Ryan, J.P. Predicting mortality following hip fracture: An analysis of comorbidities and complications. Ir. J. Med. Sci. 2015, 184, 667–671. [Google Scholar] [CrossRef]
- Buss, L.; Mckeever, T.; Nightingale, J.; Akyea, R.; Ollivere, B.; Moppett, I.; Bolton, C. Outcomes post hip fracture for patients with COPD. Eur. Respir. J. 2018, 52, PA4145. [Google Scholar] [CrossRef]
- Lee, P.J.; Shorten, G.D. Delirium after hip fracture surgery. J. Clin. Anesth 2019, 58, 119–120. [Google Scholar] [CrossRef]
- McCusker, J.; Cole, M.; Abrahamowicz, M.; Primeau, F.; Belzile, E. Delirium predicts 12-month mortality. Arch. Intern. Med. 2002, 162, 457–463. [Google Scholar] [CrossRef]
- Gottschalk, A.; Hubbs, J.; Vikani, A.R.; Gottschalk, L.B.; Sieber, F.E. The Impact of Incident Postoperative Delirium on Survival of Elderly Patients After Surgery for Hip Fracture Repair. Anesth. Analg. 2015, 121, 1336–1343. [Google Scholar] [CrossRef]
- Harris, M.J.; Brovman, E.Y.; Urman, R.D. Clinical predictors of postoperative delirium, functional status, and mortality in geriatric patients undergoing non-elective surgery for hip fracture. J. Clin. Anesth. 2019, 58, 61–71. [Google Scholar] [CrossRef]
- Sheikh, H.Q.; Aqil, A.; Hossain, F.S.; Kapoor, H. There is no weekend effect in hip fracture surgery—A comprehensive analysis of outcomes. Surg. J. R. Coll. Surg. Edinb. Irel. 2018, 16, 259–264. [Google Scholar] [CrossRef]
- Boylan, M.R.; Rosenbaum, J.; Adler, A.; Naziri, Q.; Paulino, C.B. Hip Fracture and the Weekend Effect: Does Weekend Admission Affect Patient Outcomes? Am. J. Orthop. 2015, 44, 458–464. [Google Scholar]
- Nijland, L.M.G.; Karres, J.; Simons, A.E.; Ultee, J.M.; Kerkhoffs, G.; Vrouenraets, B.C. The weekend effect for hip fracture surgery. Injury 2017, 48, 1536–1541. [Google Scholar] [CrossRef]


| Demographics | Unadjusted OR (95% CI) | p-value |
| Age ≥ 75 | 5.87 (3.04–11.35) | <0.001 |
| Injury Characteristics | Unadjusted OR (95% CI) | p-value |
| ISS > 16 | 0.13 (0.02–0.97) | 0.046 |
| Patient Co-morbidities | Unadjusted OR (95% CI) | p-value |
| Dementia | 5.67 (3.49–9.21) | <0.001 |
| Pre-operative CKD | 2.32 (1.44–3.72) | <0.001 |
| Post-operative CKD | 2.70 (1.67–4.35) | <0.001 |
| Hypoalbuminaemia | 6.23 (2.80–13.90) | <0.001 |
| CCS ≥ 6 | 5.36 (3.17–9.07) | <0.001 |
| Social History | Unadjusted OR (95% CI) | p-value |
| Alcohol > 10 units/week | 0.44 (0.21–0.90) | 0.026 |
| Osteoporosis | Unadjusted OR (95% CI) | p-value |
| Frequent Falls | 2.17 (1.36–3.48) | 0.001 |
| Pre-injury Fragility Fractures | 1.78 (1.07–2.97) | 0.027 |
| Post-injury Fragility Fractures | 0.26 (0.10–0.67) | 0.005 |
| Osteoporosis | 1.72 (1.04–2.83) | 0.035 |
| Complications | Unadjusted OR (95% CI) | p-value |
| Nail Related Complications * | 0.27 (0.12–0.65) | 0.003 |
| Non-union | 0.23 (0.08–0.64) | 0.005 |
| HAP/CAP | 3.66 (2.21–6.07) | <0.001 |
| Post-Operative Transfusion < 48 h | 2.19 (1.35–3.54) | 0.001 |
| Post-Operative Transfusion (All) | 1.78 (1.07–2.98) | 0.027 |
| OR | Confidence Interval | p-Value | |
|---|---|---|---|
| Albumin (Low) | 4.82 | 2.08–11.19 | p < 0.001 |
| Dementia | 3.99 | 2.27–7.01 | p < 0.001 |
| HAP/CAP | 3.18 | 1.76–5.77 | p < 0.001 |
| CCS > 6 | 2.94 | 1.62–5.35 | p < 0.001 |
| OR | Confidence Interval | p-Value | |
|---|---|---|---|
| CCS 0 to 8 | 1.69 | 1.00–2.84 | p = 0.048 |
| CCS ≥ 9 | 2.02 | 1.03–3.95 | p = 0.040 |
| Asthma/COPD | 2.29 | 1.37–3.82 | p = 0.002 |
| ICU/HDU Stay | 3.25 | 1.77–5.96 | p < 0.001 |
| LOS ≥ 21 days | 8.82 | 1.18–65.80 | p = 0.034 |
| OR | Confidence Interval | p-Value | |
|---|---|---|---|
| Dementia | 3.84 | 1.98–7.44 | p < 0.001 |
| HAP/CAP | 2.21 | 1.09–4.47 | p = 0.028 |
| UTI | 3.29 | 1.66–6.52 | p = 0.001 |
| CKD Stage post-operatively (Moderate/Severe) | 2.02 | 1.07–3.81 | p = 0.030 |
| ICU/HDU Stay | 4.25 | 1.78–10.14 | p = 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panteli, M.; Giannoudi, M.P.; Lodge, C.J.; West, R.M.; Pountos, I.; Giannoudis, P.V. Mortality and Medical Complications of Subtrochanteric Fracture Fixation. J. Clin. Med. 2021, 10, 540. https://doi.org/10.3390/jcm10030540
Panteli M, Giannoudi MP, Lodge CJ, West RM, Pountos I, Giannoudis PV. Mortality and Medical Complications of Subtrochanteric Fracture Fixation. Journal of Clinical Medicine. 2021; 10(3):540. https://doi.org/10.3390/jcm10030540
Chicago/Turabian StylePanteli, Michalis, Marilena P. Giannoudi, Christopher J. Lodge, Robert M. West, Ippokratis Pountos, and Peter V. Giannoudis. 2021. "Mortality and Medical Complications of Subtrochanteric Fracture Fixation" Journal of Clinical Medicine 10, no. 3: 540. https://doi.org/10.3390/jcm10030540
APA StylePanteli, M., Giannoudi, M. P., Lodge, C. J., West, R. M., Pountos, I., & Giannoudis, P. V. (2021). Mortality and Medical Complications of Subtrochanteric Fracture Fixation. Journal of Clinical Medicine, 10(3), 540. https://doi.org/10.3390/jcm10030540