
An MRI-Based Radiomic Prognostic Index Predicts Poor Outcome and Specific Genetic Alterations in Endometrial Cancer

 , and
, and
Abstract
1. Introduction
2. Experimental Section
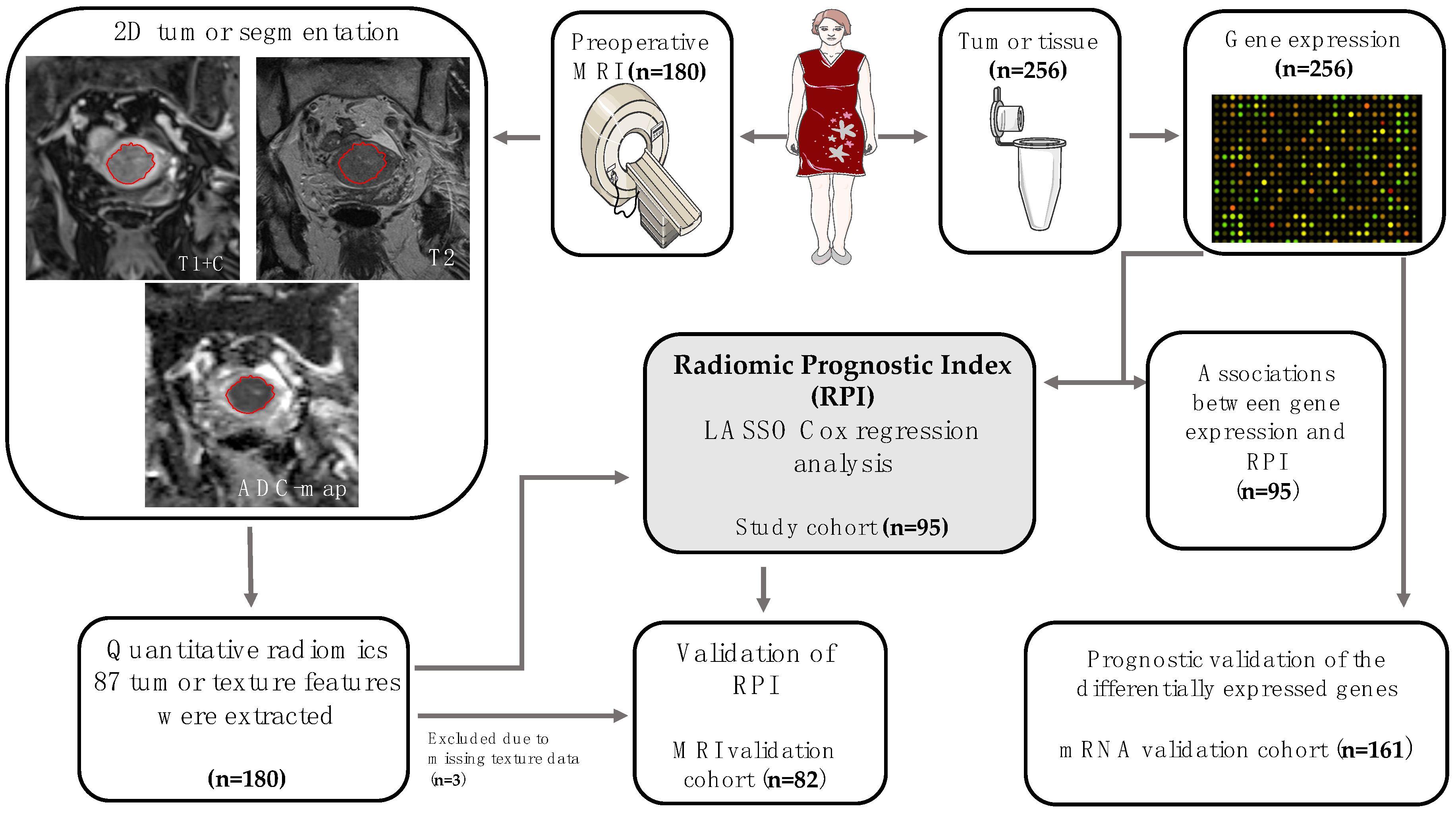
2.1. Patient Samples and Patient Cohorts
2.2. MR Imaging and Texture Analysis
2.3. Gene Expression Analyses
2.4. Model Development and Statistical Analysis
3. Results
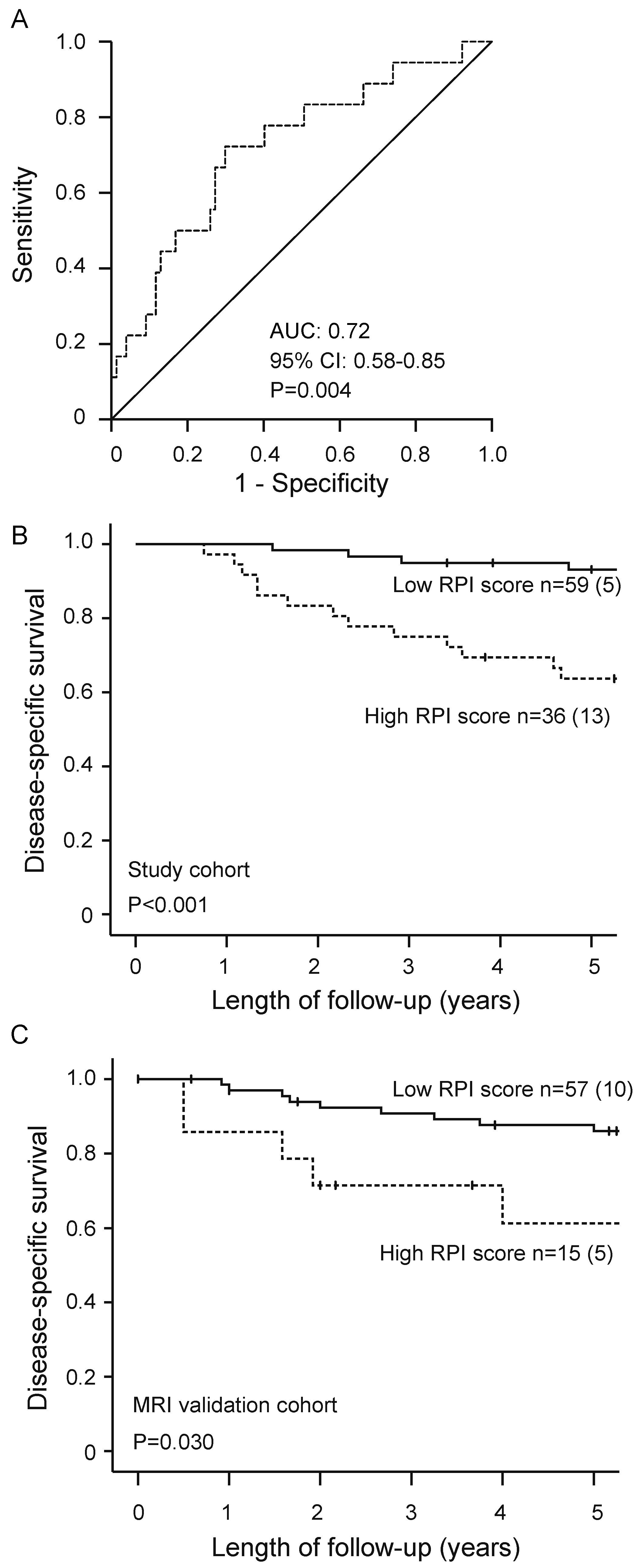
3.1. High Radiomic Prognostic Index Predicts Poor Outcome and Aggressive Clinicopathological Features in Endometrial Cancer
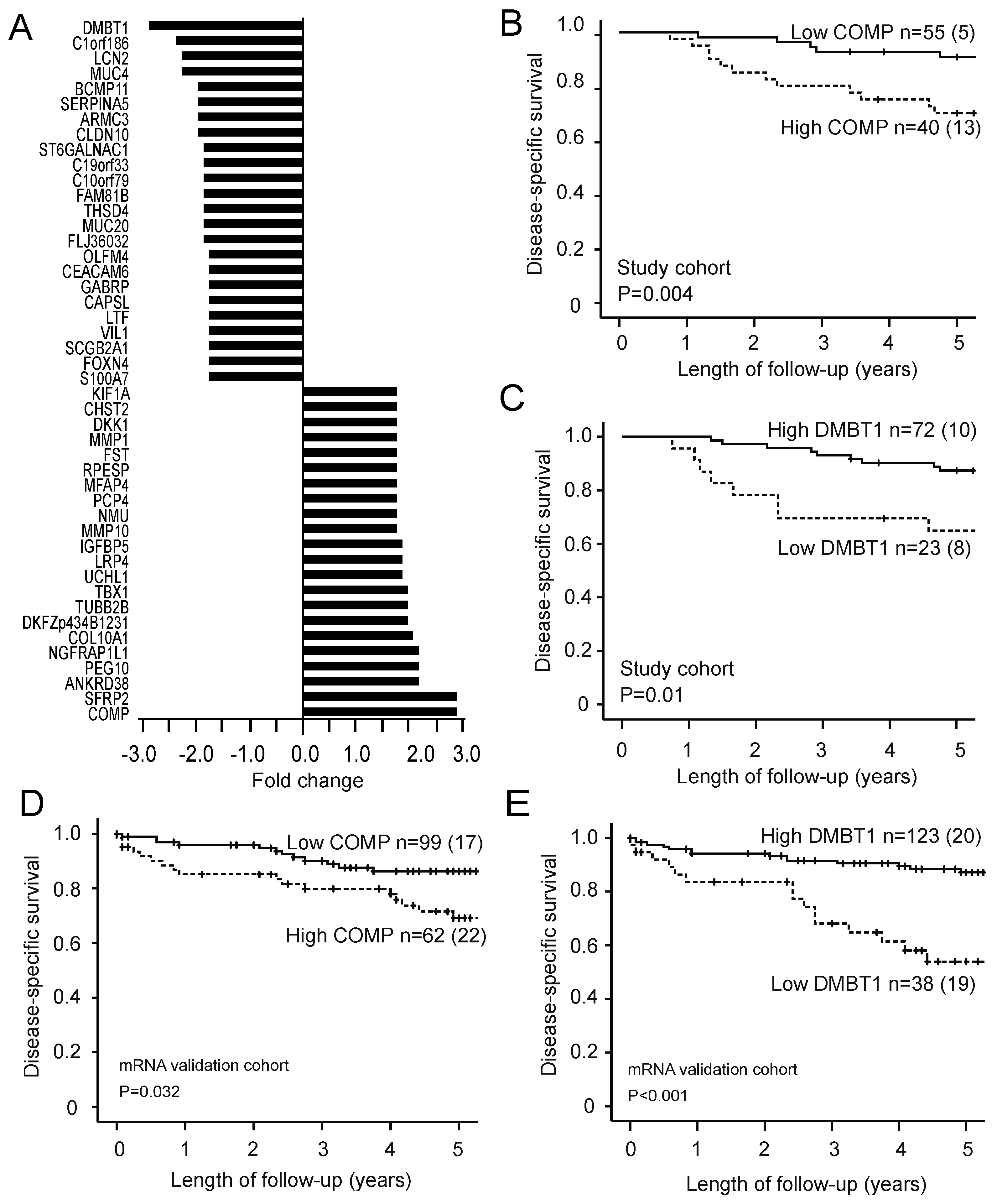
3.2. High RPI Identifies Potential Prognostic Genes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Mirza, M.R.; Koskas, M.; Creutzberg, C.L. Cancer of the corpus uteri. Int. J. Gynecol. Obstet. 2018, 143, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Salvesen, H.B.; Haldorsen, I.S.; Trovik, J. Markers for individualised therapy in endometrial carcinoma. Lancet Oncol. 2012, 13, e353–e361. [Google Scholar] [CrossRef]
- Murali, R.; Soslow, R.A.; Weigelt, B. Classification of endometrial carcinoma: More than two types. Lancet Oncol. 2014, 15, e268–e278. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Haldorsen, I.S.; Salvesen, H.B. What Is the Best Preoperative Imaging for Endometrial Cancer? Curr. Oncol. Rep. 2016, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Jun, W.; Cong, W.; Xianxin, X.; Daqing, J. Meta-Analysis of Quantitative Dynamic Contrast-Enhanced MRI for the Assessment of Neoadjuvant Chemotherapy in Breast Cancer. Am. Surg. 2019, 85, 645–653. [Google Scholar] [CrossRef]
- Haldorsen, I.H.; Lura, N.; Blaakær, J.; Fischerova, D.; Werner, H.M.J. What Is the Role of Imaging at Primary Diagnostic Work-Up in Uterine Cervical Cancer? Curr. Oncol. Rep. 2019, 21, 77. [Google Scholar] [CrossRef]
- Dijkhoff, R.A.; Beets-Tan, R.G.H.; Lambregts, D.M.J.; Beets, G.L.; Maas, M. Value of DCE-MRI for staging and response evaluation in rectal cancer: A systematic review. Eur. J. Radiol. 2017, 95, 155–168. [Google Scholar] [CrossRef]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Ytre-Hauge, S.; Dybvik, J.A.; Lundervold, A.; Salvesen, Ø.; Krakstad, C.; Fasmer, K.E.; Werner, H.M.; Ganeshan, B.; Høivik, E.; Bjørge, L.; et al. Preoperative tumor texture analysis on MRI predicts high-risk disease and reduced survival in endometrial cancer. J. Magn. Reson. Imaging 2018, 48, 1637–1647. [Google Scholar] [CrossRef]
- Chitalia, R.D.; Kontos, D. Role of texture analysis in breast MRI as a cancer biomarker: A review. J. Magn. Reson. Imaging 2019, 49, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Giganti, F.; Tang, L.; Baba, H. Gastric cancer and imaging biomarkers: Part 1—A critical review of DW-MRI and CE-MDCT findings. Eur. Radiol. 2019, 29, 1743–1753. [Google Scholar] [CrossRef] [PubMed]
- Ueno, Y.; Forghani, B.; Forghani, R.; Dohan, A.; Zeng, X.Z.; Chamming’S, F.; Arseneau, J.; Fu, L.; Gilbert, L.; Gallix, B.; et al. Endometrial Carcinoma: MR Imaging-based Texture Model for Preoperative Risk Stratification-A Preliminary Analysis. Radiology 2017, 284, 748–757. [Google Scholar] [CrossRef]
- Zhou, M.; Leung, A.; Echegaray, S.; Gentles, A.; Shrager, J.B.; Jensen, K.C.; Berry, G.J.; Plevritis, S.K.; Rubin, D.L.; Napel, S.; et al. Non-Small Cell Lung Cancer Radiogenomics Map Identifies Relationships between Molecular and Imaging Phenotypes with Prognostic Implications. Radiology 2018, 286, 307–315. [Google Scholar] [CrossRef]
- Yeh, A.C.; Li, H.; Zhu, Y.; Zhang, J.; Khramtsova, G.; Drukker, K.; Edwards, A.; McGregor, S.; Yoshimatsu, T.; Zheng, Y.; et al. Radiogenomics of breast cancer using dynamic contrast enhanced MRI and gene expression profiling. Cancer Imaging 2019, 19, 48. [Google Scholar] [CrossRef]
- Saha, A.; Harowicz, M.R.; Grimm, L.J.; Kim, C.E.; Ghate, S.V.; Walsh, R.; Mazurowski, M.A. A machine learning approach to radiogenomics of breast cancer: A study of 922 subjects and 529 DCE-MRI features. Br. J. Cancer 2018, 119, 508–516. [Google Scholar] [CrossRef]
- Fan, M.; Xia, P.; Clarke, R.; Wang, Y.; Li, L. Radiogenomic signatures reveal multiscale intratumour heterogeneity associated with biological functions and survival in breast cancer. Nat. Commun. 2020, 11, 4861. [Google Scholar] [CrossRef]
- Beig, N.; Bera, K.; Prasanna, P.; Antunes, J.; Correa, R.; Singh, S.; Bamashmos, A.S.; Ismail, M.; Braman, N.; Verma, R.; et al. Radiogenomic-Based Survival Risk Stratification of Tumor Habitat on Gd-T1w MRI Is Associated with Biological Processes in Glioblastoma. Clin. Cancer Res. 2020, 26, 1866–1876. [Google Scholar] [CrossRef] [PubMed]
- Trovik, J.; Wik, E.; Stefansson, I.M.; Marcickiewicz, J.; Tingulstad, S.; Staff, A.C.; Njolstad, T.S.; Vandenput, I.; Amant, F.; Akslen, L.A.; et al. Stathmin Overexpression Identifies High-Risk Patients and Lymph Node Metastasis in Endometrial Cancer. Clin. Cancer Res. 2011, 17, 3368–3377. [Google Scholar] [CrossRef] [PubMed]
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Krakstad, C.; Trovik, J.; Wik, E.; Engelsen, I.B.; Werner, H.M.J.; Birkeland, E.; Raeder, M.B.; Øyan, A.M.; Stefansson, I.M.; Kalland, K.H.; et al. Loss of GPER identifies new targets for therapy among a subgroup of ERα-positive endometrial cancer patients with poor outcome. Br. J. Cancer 2012, 106, 1682–1688. [Google Scholar] [CrossRef] [PubMed]
- Wik, E.; Ræder, M.B.; Krakstad, C.; Trovik, J.; Birkeland, E.; Hoivik, E.A.; Mjos, S.; Werner, H.M.; Mannelqvist, M.; Stefansson, I.M.; et al. Lack of estrogen receptor-alpha is associated with epithelial-mesenchymal transition and PI3K alterations in endometrial carcinoma. Clin. Cancer Res. 2013, 19, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Halle, M.K.; Tangen, I.L.; Berg, H.F.; Hoivik, E.A.; Mauland, K.K.; Kusonmano, K.; Berg, A.; Hurtado, A.; Kalland, K.H.; Øyan, A.M.; et al. HER2 expression patterns in paired primary and metastatic endometrial cancer lesions. Br. J. Cancer 2018, 118, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Dysvik, B.; Jonassen, I. J-Express: Exploring gene expression data using Java. Bioinformatics 2001, 17, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Tibshirani, R. The lasso method for variable selection in the Cox model. Stat. Med. 1997, 16, 385–395. [Google Scholar] [CrossRef]
- Zhang, H.; Mao, Y.; Chen, X.; Wu, G.; Liu, X.; Zhang, P.; Bai, Y.; Lu, P.; Yao, W.; Wang, Y.; et al. Magnetic resonance imaging radiomics in categorizing ovarian masses and predicting clinical outcome: A preliminary study. Eur. Radiol. 2019, 29, 3358–3371. [Google Scholar] [CrossRef]
- Li, Q.; Xiao, Q.; Li, J.; Duan, S.; Wang, H.; Gu, Y. MRI-Based Radiomic Signature as a Prognostic Biomarker for HER2-Positive Invasive Breast Cancer Treated with NAC. Cancer Manag. Res. 2020, 12, 10603–10613. [Google Scholar]
- Fasmer, K.E.; Hodneland, E.; Dybvik, J.A.; Wagner-Larsen, K.; Trovik, J.; Salvesen, Ø.; Krakstad, C.; Haldorsen, I.H. Whole-Volume Tumor MRI Radiomics for Prognostic Modeling in Endometrial Cancer. J. Magn. Reson. Imaging 2020. [Google Scholar] [CrossRef]
- Winkler, J.; Abisoye-Ogunniyan, A.; Metcalf, K.J.; Werb, Z. Concepts of extracellular matrix remodelling in tumour progression and metastasis. Nat. Commun. 2020, 11, 5120. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Li, Y.; Hu, S.; Chen, Y.; Gao, L.; Liu, D.; Guo, H.; Yang, Y. Clinical significance of matrix metalloproteinase-2 in endometrial cancer. Medicine 2018, 97, e10994. [Google Scholar] [CrossRef]
- Fields, G.B. Mechanisms of Action of Novel Drugs Targeting Angiogenesis-Promoting Matrix Metalloproteinases. Front. Immunol. 2019, 10, 1278. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R.; Gautam, S.K.; Cannon, A.; Thompson, C.; Hall, B.R.; Aithal, A.; Banerjee, K.; Jain, M.; Solheim, J.C.; Kumar, S.; et al. Cancer-associated mucins: Role in immune modulation and metastasis. Cancer Metastasis Rev. 2019, 38, 223–236. [Google Scholar] [CrossRef]
- Englund, E.; Bartoschek, M.; Reitsma, B.; Jacobsson, L.; Escudero-Esparza, A.; Orimo, A.; Leandersson, K.; Hagerling, C.; Aspberg, A.; Storm, P.; et al. Cartilage oligomeric matrix protein contributes to the development and metastasis of breast cancer. Oncogene 2016, 35, 5585–5596. [Google Scholar] [CrossRef] [PubMed]
- Nfonsam, V.N.; Nfonsam, L.E.; Chen, D.; Omesiete, P.N.; Cruz, A.; Runyan, R.B.; Jandova, J. COMP Gene Coexpresses With EMT Genes and Is Associated With Poor Survival in Colon Cancer Patients. J. Surg. Res. 2019, 233, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Nfonsam, V.N.; Jecius, H.C.; Janda, J.; Omesiete, P.N.; Elquza, E.; Scott, A.J.; Nfonsam, L.E.; Jandova, J. Cartilage oligomeric matrix protein (COMP) promotes cell proliferation in early-onset colon cancer tumorigenesis. Surg. Endosc. 2019, 34, 3992–3998. [Google Scholar] [CrossRef]
- Braidotti, P.; Nuciforo, P.; Mollenhauer, J.; Poustka, A.; Pellegrini, C.; Moro, A.; Bulfamante, G.; Coggi, G.; Bosari, S.; Pietra, G.G. DMBT1 expression is down-regulated in breast cancer. BMC Cancer 2004, 4, 46. [Google Scholar]
- Du, J.; Guan, M.; Fan, J.; Jiang, H. Loss of DMBT1 expression in human prostate cancer and its correlation with clinical progressive features. Urology 2011, 77, 509.e9–509.e13. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Kim, B.C.; Yeo, H.Y.; Kim, K.-H.; Yoo, B.C.; Park, J.W.; Chang, H.J. Deleted in malignant brain tumor 1 is a novel prognostic marker in colorectal cancer. Oncol. Rep. 2018, 39, 2279–2287. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Study Cohort (n = 95) | MRI Validation Cohort (n = 82) | mRNA Validation Cohort (n = 161) | p-Value * |
|---|---|---|---|---|
| Age, median (range) years | 68 (41–93) | 66 (41–84) | 66 (38–93) | 0.60 |
| FIGO stage | 0.64 | |||
| I–II | 82 (86%) | 68 (83%) | 122 (76%) | |
| III–IV | 13 (14%) | 14 (17%) | 39 (24%) | |
| Histologic subtype | 0.90 | |||
| Endometrioid | 76 (80%) | 65 (79%) | 127 (79%) | |
| Non-endometrioid | 19 (20%) | 17 (21%) | 34 (21%) | |
| Histologic grade § | 0.58 | |||
| Grade 1 | 34 (45%) | 30 (46%) | 44 (35%) | |
| Grade 2 | 21 (28%) | 24 (37%) | 49 (39%) | |
| Grade 3 | 20 (26%) | 10 (15%) | 30 (24%) | |
| ND | 1 (1%) | 1 (2%) | 3 (2%) | |
| Myometrial invasion | 0.04 | |||
| <50% | 47 (50%) | 52 (63%) | 77 (48%) | |
| ≥50% | 48 (50%) | 28 (34%) | 82 (51%) | |
| ND | 2 (3%) | 2 (1%) | ||
| Lymph node metastases | 0.69 | |||
| No | 76 (81%) | 56 (68%) | 92 (57%) | |
| Yes | 10 (10%) | 9 (11%) | 23 (14%) | |
| ND | 9 (9%) | 17 (21%) | 46 (29%) |
| Study Cohort (n = 95) | MRI Validation Cohort (n = 82) | |||||||
|---|---|---|---|---|---|---|---|---|
| Patients (n) | High RPI (n = 36) | Low RPI (n = 59) | p-Value * | Patients (n) | High RPI (n = 15) | Low RPI (n = 67) | p-Value * | |
| Age | 0.54 | 0.59 | ||||||
| <67 years | 46 | 16 (44%) | 30 (51%) | 44 | 9 (60%) | 35 (52%) | ||
| ≥67 years | 49 | 20 (56%) | 29 (49%) | 38 | 6 (40%) | 32 (48%) | ||
| FIGO stage | 0.06 | 0.03 | ||||||
| I–II | 82 | 28 (78%) | 54 (91%) | 67 | 9 (64%) | 58 (88%) | ||
| III–IV | 13 | 8 (22%) | 5 (9%) | 13 | 5 (36%) | 8 (12%) | ||
| Histologic type | 0.67 | 0.53 | ||||||
| Endometrioid | 76 | 28 (78%) | 48 (81%) | 65 | 11 (73%) | 54 (81%) | ||
| Non-endometrioid | 19 | 8 (22%) | 11 (19%) | 17 | 4 (27%) | 13 (19%) | ||
| Histologic grade § | 0.16 | 0.89 | ||||||
| Grade 1–2 | 55 | 17 (47%) | 38 (64%) | 54 | 10 (67%) | 44 (66%) | ||
| Grade 3 | 39 | 19 (53%) | 20 (34%) | 27 | 5 (33%) | 22 (33%) | ||
| ND | 1 | 1 (0%) | 1 (2%) | 1 | 0 (0%) | 1 (1%) | ||
| Myometrial invasion | 0.001 | 0.004 | ||||||
| <50% | 52 | 4 (27%) | 48 (72%) | |||||
| ≥50% | 47 | 10 (28%) | 37 (63%) | 28 | 10 (67%) | 18 (27%) | ||
| ND | 48 | 26 (72%) | 22 (37%) | 2 | 1 (6%) | 1 (1%) | ||
| Lymph node metastases | 0.31 | 0.02 | ||||||
| No | 76 | 27 (75%) | 49 (83%) | 56 | 6 (40%) | 50 (75%) | ||
| Yes | 10 | 6 (17%) | 4 (7%) | 9 | 4 (27%) | 5 (7%) | ||
| ND | 9 | 3 (8%) | 6 (10%) | 17 | 5 (33%) | 12 (18%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacob, H.; Dybvik, J.A.; Ytre-Hauge, S.; Fasmer, K.E.; Hoivik, E.A.; Trovik, J.; Krakstad, C.; Haldorsen, I.S. An MRI-Based Radiomic Prognostic Index Predicts Poor Outcome and Specific Genetic Alterations in Endometrial Cancer. J. Clin. Med. 2021, 10, 538. https://doi.org/10.3390/jcm10030538
Jacob H, Dybvik JA, Ytre-Hauge S, Fasmer KE, Hoivik EA, Trovik J, Krakstad C, Haldorsen IS. An MRI-Based Radiomic Prognostic Index Predicts Poor Outcome and Specific Genetic Alterations in Endometrial Cancer. Journal of Clinical Medicine. 2021; 10(3):538. https://doi.org/10.3390/jcm10030538
Chicago/Turabian StyleJacob, Havjin, Julie A. Dybvik, Sigmund Ytre-Hauge, Kristine E. Fasmer, Erling A. Hoivik, Jone Trovik, Camilla Krakstad, and Ingfrid S. Haldorsen. 2021. "An MRI-Based Radiomic Prognostic Index Predicts Poor Outcome and Specific Genetic Alterations in Endometrial Cancer" Journal of Clinical Medicine 10, no. 3: 538. https://doi.org/10.3390/jcm10030538
APA StyleJacob, H., Dybvik, J. A., Ytre-Hauge, S., Fasmer, K. E., Hoivik, E. A., Trovik, J., Krakstad, C., & Haldorsen, I. S. (2021). An MRI-Based Radiomic Prognostic Index Predicts Poor Outcome and Specific Genetic Alterations in Endometrial Cancer. Journal of Clinical Medicine, 10(3), 538. https://doi.org/10.3390/jcm10030538