
Apolipoprotein ɛ4 Status and Brain Structure 12 Months after Mild Traumatic Injury: Brain Age Prediction Using Brain Morphometry and Diffusion Tensor Imaging

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Participants and Procedure
2.3. Biospecimen and Genotyping Procedures
2.4. MRI Processing
2.5. Brain-Age Prediction
2.6. Statistical Analyses
2.7. Demographic and Clinical Assessment
3. Results
3.1. Comparison Groups, Demographics, and Injury-Related Variables
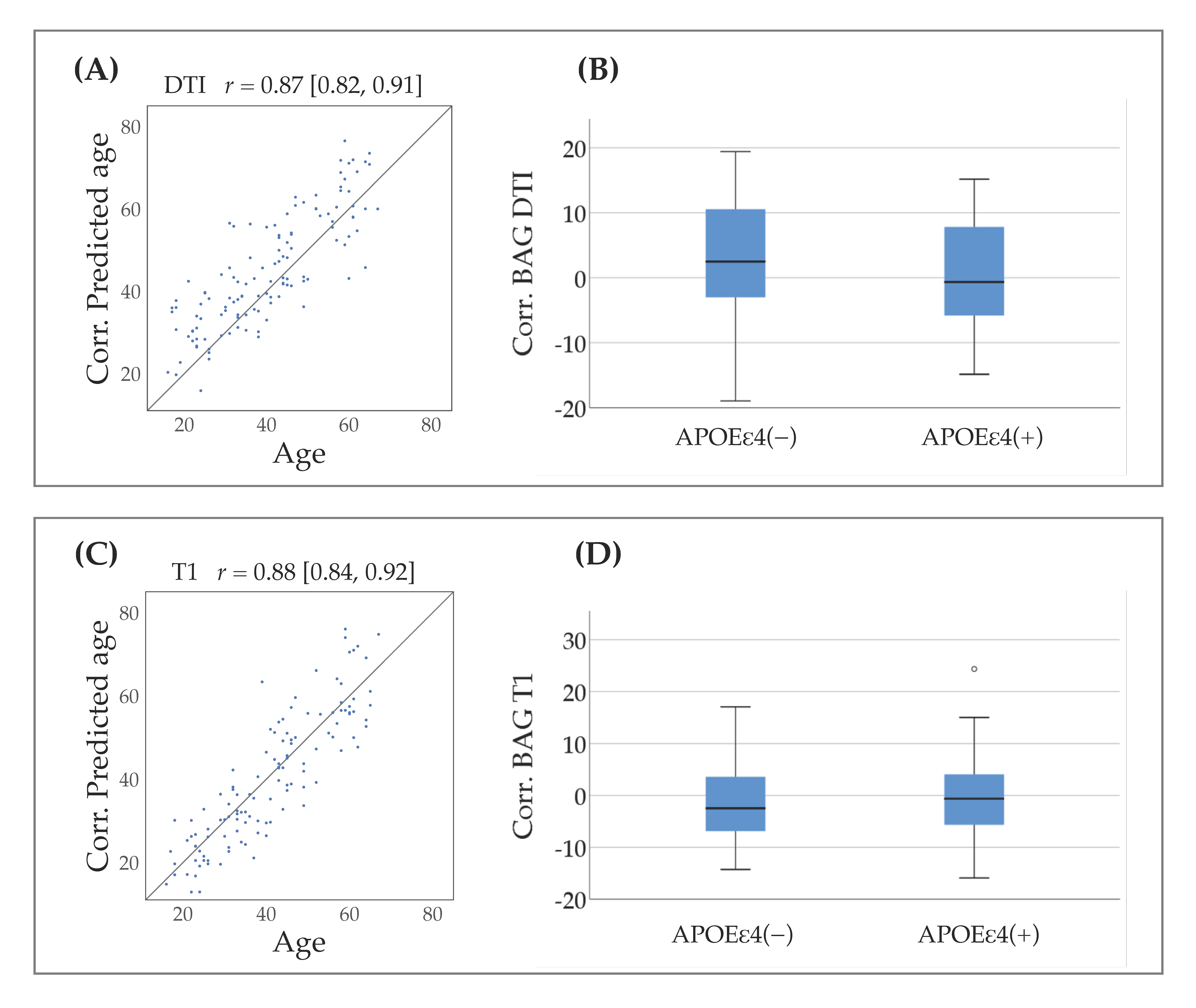
3.2. Brain-Age Prediction
3.3. Association between APOE Status and Brain-Age Gap
3.4. Association between APOE Status and Brain Morphometry
3.5. Association between APOE and DTI Measures
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dikmen, S.; Machamer, J.; Fann, J.R.; Temkin, N.R. Rates of symptom reporting following traumatic brain injury. J. Int. Neuropsychol. Soc. 2010, 16, 401–411. [Google Scholar] [CrossRef]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastis, R.; von Steinbügel, N. A Multidimensional Approach to Post-concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef]
- Sigurdardottir, S.; Andelic, N.; Roe, C.; Jerstad, T.; Schanke, A.K. Post-concussion symptoms after traumatic brain injury at 3 and 12 months post-injury: A prospective study. Brain Inj. 2009, 23, 489–497. [Google Scholar] [CrossRef]
- Finnoff, J.T.; Jelsing, E.J.; Smith, J. Biomarkers, genetics, and risk factors for concussion. J. Inj. Funct. Rehabil. 2011, 3 (Suppl. 2), S452–S459. [Google Scholar] [CrossRef]
- Bartzokis, G.; Lu, P.H.; Geschwind, D.H.; Edwards, N.; Mintz, J.; Cummings, J.L. Apolipoprotein E genotype and age-related myelin breakdown in healthy individuals: Implications for cognitive decline and dementia. Arch. Gen. Psychiatry 2006, 63, 63–72. [Google Scholar] [CrossRef]
- Samatovicz, R.A. Genetics and brain injury: Apolipoprotein E. J. Head Trauma Rehabil. 2000, 15, 869–874. [Google Scholar] [CrossRef]
- Mahley, R.W.; Huang, Y. Apolipoprotein e sets the stage: Response to injury triggers neuropathology. Neuron 2012, 76, 871–885. [Google Scholar] [CrossRef]
- Van Den Heuvel, C.; Thornton, E.; Vink, R. Traumatic brain injury and Alzheimer’s disease: A review. Prog. Brain Res. 2007, 161, 303–316. [Google Scholar]
- Liberman, J.N.; Stewart, W.F.; Wesnes, K.; Troncoso, J. Apolipoprotein E epsilon 4 and short-term recovery from predominantly mild brain injury. Neurology 2002, 58, 1038–1044. [Google Scholar] [CrossRef]
- Mueller, S.G.; Weiner, M.W. Selective effect of age, Apo e4, and Alzheimer’s disease on hippocampal subfields. Hippocampus 2009, 19, 558–564. [Google Scholar] [CrossRef]
- Lenihan, M.W.; Jordan, B.D. The clinical presentation of chronic traumatic encephalopathy. Curr. Neurol. Neurosci. Rep. 2015, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, J.A.; Roberts, G.W.; Graham, D.I. Apolipoprotein E epsilon 4 allele is associated with deposition of amyloid beta-protein following head injury. Nat. Med. 1995, 1, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.P.; Logue, M.W.; Sadeh, N.; Spielberg, J.M.; Verfaellie, M.; Hayes, S.M.; Reagan, A.; Salat, D.H.; Wolf, E.J.; McGlinchey, R.E.; et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain J. Neurol. 2017, 140, 813–825. [Google Scholar] [CrossRef] [PubMed]
- Carroll, L.J.; Cassidy, J.D.; Peloso, P.M.; Borg, J.; von Holst, H.; Holm, L.; Paniak, C.; Pépin, M. Prognosis for mild traumatic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 2004, 14 (Suppl. 43), 84–105. [Google Scholar] [CrossRef]
- Godbolt, A.K.; Cancelliere, C.; Hincapié, C.A.; Marras, C.; Boyle, E.; Kristman, V.L.; Coronado, V.G.; Cassidy, J.D. Systematic review of the risk of dementia and chronic cognitive impairment after mild traumatic brain injury: Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch. Phys. Med. Rehabil. 2014, 95 (Suppl. 3), S245–S256. [Google Scholar] [CrossRef]
- Mehta, K.M.; Ott, A.; Kalmijn, S.; Slooter, A.J.; van Duijn, C.M.; Hofman, A.; Breteler, M.M. Head trauma and risk of dementia and Alzheimer’s disease: The Rotterdam Study. Neurology 1999, 53, 1959–1962. [Google Scholar] [CrossRef]
- Graves, A.B.; White, E.; Koepsell, T.D.; Reifler, B.V.; van Belle, G.; Larson, E.B.; Raskind, M. The association between head trauma and Alzheimer’s disease. Am. J. Epidemiol. 1990, 131, 491–501. [Google Scholar] [CrossRef]
- Schofield, P.W.; Tang, M.; Marder, K.; Bell, K.; Dooneief, G.; Chun, M.; Sano, M.; Stern, Y.; Mayeux, R. Alzheimer’s disease after remote head injury: An incidence study. J. Neurol. Neurosurg. Psych. 1997, 62, 119–124. [Google Scholar] [CrossRef]
- Helmes, E.; Østbye, T.; Steenhuis, R.E. Incremental contribution of reported previous head injury to the prediction of diagnosis and cognitive functioning in older adults. Brain Inj. 2011, 25, 338–347. [Google Scholar] [CrossRef]
- Yue, J.K.; Robinson, C.K.; Burke, J.F.; Winkler, E.A.; Deng, H.; Cnossen, M.C.; Lingsma, H.F.; Ferguson, A.R.; McAllister, T.W.; Rosand, J.; et al. Apolipoprotein E epsilon 4 (APOE-ε4) genotype is associated with decreased 6-month verbal memory performance after mild traumatic brain injury. Brain Behav. 2017, 7, e00791. [Google Scholar] [CrossRef]
- Beck, D.; de Lange, A.G.; Maximov, I.I.; Richard, G.; Andreassen, O.A.; Nordvik, J.E.; Westlye, L.T. White matter microstructure across the adult lifespan: A mixed longitudinal and cross-sectional study using advanced diffusion models and brain-age prediction. NeuroImage 2020, 224, 117441. [Google Scholar] [CrossRef] [PubMed]
- Westlye, L.T.; Walhovd, K.B.; Dale, A.M.; Bjørnerud, A.; Due-Tønnessen, P.; Engvig, A.; Grydeland, H.; Tamnes, C.K.; Ostby, Y.; Fjell, A.M. Life-span changes of the human brain white matter: Diffusion tensor imaging (DTI) and volumetry. Cereb Cortex 2010, 20, 2055–2068. [Google Scholar] [CrossRef] [PubMed]
- Westlye, L.T.; Reinvang, I.; Rootwelt, H.; Espeseth, T. Effects of APOE on brain white matter microstructure in healthy adults. Neurology 2012, 79, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.R.; Logue, M.W.; Wolf, E.J.; Hayes, J.P.; Salat, D.H.; Fortier, C.B.; Fonda, J.R.; McGlinchey, R.E.; Milberg, W.P.; Miller, M.W. Close-Range Blast Exposure Is Associated with Altered White Matter Integrity in Apolipoprotein ɛ4 Carriers. J. Neurotrauma 2019, 36, 3264–3273. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.H.; Franke, K. Predicting Age Using Neuroimaging: Innovative Brain Ageing Biomarkers. Trends Neurosci. 2017, 40, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.H.; Poudel, R.P.K.; Tsagkrasoulis, D.; Caan, M.W.A.; Steves, C.; Spector, T.D.; Montana, G. Predicting brain age with deep learning from raw imaging data results in a reliable and heritable biomarker. NeuroImage 2017, 163, 115–124. [Google Scholar] [CrossRef]
- James, H.; Cole, K.F.; Cherbuin, N. Biomarkers of Human Aging; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Smith, S.M.; Elliott, L.T.; Alfaro-Almagro, F.; McCarthy, P.; Nichols, T.E.; Douaud, G.; Miller, K.L. Brain aging comprises many modes of structural and functional change with distinct genetic and biophysical associations. eLife 2020, 9, e52677. [Google Scholar] [CrossRef]
- Cole, J.H. Multimodality neuroimaging brain-age in UK biobank: Relationship to biomedical, lifestyle, and cognitive factors. Neurobiol. Aging. 2020, 92, 34–42. [Google Scholar] [CrossRef]
- de Lange, A.G.; Anatürk, M.; Suri, S.; Kaufmann, T.; Cole, J.H.; Griffanti, L.; Zsoldos, E.; Jensen, D.E.A.; Filippini, N.; Singh-Manoux, A.; et al. Multimodal brain-age prediction and cardiovascular risk: The Whitehall II MRI sub-study. NeuroImage 2020, 222, 117292. [Google Scholar] [CrossRef]
- Kaufmann, T.; van der Meer, D.; Doan, N.T.; Schwarz, E.; Lund, M.J.; Agartz, I.; Alnæs, D.; Barch, D.M.; Baur-Streubel, R.; Bertolino, A.; et al. Common brain disorders are associated with heritable patterns of apparent aging of the brain. Nat. Neurosci. 2019, 22, 1617–1623. [Google Scholar] [CrossRef]
- Han, L.K.M.; Dinga, R.; Hahn, T.; Ching, C.R.K.; Eyler, L.T.; Aftanas, L.; Aghajani, M.; Aleman, A.; Baune, B.T.; Berger, K.; et al. Brain aging in major depressive disorder: Results from the ENIGMA major depressive disorder working group. Mol. Psychiatry 2020, 1–16. [Google Scholar] [CrossRef]
- Cole, J.H.; Marioni, R.E.; Harris, S.E.; Deary, I.J. Brain age and other bodily ‘ages’: Implications for neuropsychiatry. Mol. Psychiatry 2019, 24, 266–281. [Google Scholar] [CrossRef]
- Cole, D.J.; Raffel, J.; Friede, D.T.; Eshaghi, D.A.; Brownlee, D.F.W.J.; Chard, D.D.; Stefano., N.D.; Enzinger, C.; Pirpamer, L.; Filippi, M.; et al. Longitudinal Assessment of Multiple Sclerosis with the Brain-Age Paradigm. Ann. Neurol. 2020, 88, 93–105. [Google Scholar] [CrossRef]
- Cole, J.H.; Leech, R.; Sharp, D.J. Prediction of brain age suggests accelerated atrophy after traumatic brain injury. Ann. Neurol. 2015, 77, 571–581. [Google Scholar] [CrossRef]
- Mild Traumatic Brain Injury Committee; American Congress of Rehabilitation Medicine; Group HIISI. Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 1993, 8, 86–87. [Google Scholar] [CrossRef]
- Hellstrøm, T.; Westlye, L.T.; Server, A.; Løvstad, M.; Brunborg, C.; Lund, M.J.; Nordhøy, W.; Andreassen, O.A.; Andelic, N. Volumetric and morphometric MRI findings in patients with mild traumatic brain injury. Brain Inj. 2016, 30, 1683–1691. [Google Scholar] [CrossRef]
- Hellstrøm, T.; Westlye, L.T.; Sigurdardottir, S.; Brunborg, C.; Soberg, H.L.; Holthe, Ø.; Server, A.; Lund, M.J.; Andreassen, O.A.; Andelic, N. Longitudinal changes in brain morphology from 4 weeks to 12 months after mild traumatic brain injury: Associations with cognitive functions and clinical variables. Brain Inj. 2017, 31, 674–685. [Google Scholar]
- Hellstrøm, T.; Westlye, L.T.; Kaufmann, T.; Trung Doan, N.; Søberg, H.L.; Sigurdardottir, S.; Nordhøy, W.; Helseth, E.; Andreassen, O.A.; Andelic, N. White matter microstructure is associated with functional, cognitive and emotional symptoms 12 months after mild traumatic brain injury. Sci. Rep. 2017, 7, 13795. [Google Scholar] [CrossRef]
- Untergasser, A.; Cutcutache, I.; Koressaar, T.; Ye, J.; Faircloth, B.C.; Remm, M.; Rozen, S.G. Primer3—New capabilities and interfaces. Nucleic Acids Res. 2012, 40, e115. [Google Scholar] [CrossRef]
- Jenkinson, M.; Beckmann, C.F.; Behrens, T.E.; Woolrich, M.W.; Smith, S.M. FSL. NeuroImage 2012, 62, 782–790. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. NeuroImage 2006, 31, 1487–1505. [Google Scholar] [CrossRef] [PubMed]
- Song, S.K.; Sun, S.W.; Ramsbottom, M.J.; Chang, C.; Russell, J.; Cross, A.H. Dysmyelination revealed through MRI as increased radial (but unchanged axial) diffusion of water. NeuroImage 2002, 17, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Sexton, C.E.; Kalu, U.G.; Filippini, N.; Mackay, C.E.; Ebmeier, K.P. A meta-analysis of diffusion tensor imaging in mild cognitive impairment and Alzheimer’s disease. Neurobiol. Aging 2011, 32, 2322.e5–2322.e18. [Google Scholar] [CrossRef] [PubMed]
- Richard, G.; Kolskår, K.; Sanders, A.M.; Kaufmann, T.; Petersen, A.; Doan, N.T.; Sánches, J.M.; Alnæs, D.; Ulrichsen, K.M.; Dørum, E.S.; et al. Assessing distinct patterns of cognitive aging using tissue-specific brain age prediction based on diffusion tensor imaging and brain morphometry. PeerJ 2018, 6, e5908. [Google Scholar] [CrossRef] [PubMed]
- Richard, G.; Kolskår, K.; Ulrichsen, K.M.; Kaufmann, T.; Alnæs, D.; Sanders, A.M.; Dørum, E.S.; Sánches, J.M.; Petersen, A.; Ihle-Hansen, H.; et al. Brain age prediction in stroke patients: Highly reliable but limited sensitivity to cognitive performance and response to cognitive training. NeuroImage Clin. 2020, 25, 102159. [Google Scholar] [CrossRef] [PubMed]
- Shafto, M.A.; Tyler, L.K.; Dixon, M.; Taylor, J.R.; Rowe, J.B.; Cusack, R.; Calder, A.J.; Marslen-Wilson, W.D.; Duncan, J.; Dalgleish, T.; et al. The Cambridge Centre for Ageing and Neuroscience (Cam-CAN) study protocol: A cross-sectional, lifespan, multidisciplinary examination of healthy cognitive ageing. BMC Neurol. 2014, 14, 204. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.R.; Williams, N.; Cusack, R.; Auer, T.; Shafto, M.A.; Dixon, M.; Tyler, L.K.; Cam-CAN; Henson, R.N. The Cambridge Centre for Ageing and Neuroscience (Cam-CAN) data repository: Structural and functional MRI, MEG, and cognitive data from a cross-sectional adult lifespan sample. NeuroImage 2017, 144, 262–269. [Google Scholar] [CrossRef]
- Chen Tianqi, G.C. XGBoost: A Scalable Tree Boosting System. ACM Digit. Libr. 2016, 785–794. [Google Scholar] [CrossRef]
- de Lange, A.G.; Cole, J.H. Commentary: Correction procedures in brain-age prediction. NeuroImage Clin. 2020, 26, 102229. [Google Scholar] [CrossRef]
- Smith, S.M.; Vidaurre, D.; Alfaro-Almagro, F.; Nichols, T.E.; Miller, K.L. Estimation of brain age delta from brain imaging. NeuroImage 2019, 200, 528–539. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Wilson, J.T.; Pettigrew, L.E.; Teasdale, G.M. Structured interviews for the Glasgow Outcome Scale and the extended Glasgow Outcome Scale: Guidelines for their use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef] [PubMed]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.; Wade, D.T. The Rivermead Post Concussion Symptoms Questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Li, L.; Bao, Y.; He, S.; Wang, G.; Guan, Y.; Ma, D.; Wu, R.; Wang, P.; Huang, X.; Tao, S.; et al. The Association Between Apolipoprotein E and Functional Outcome After Traumatic Brain Injury: A Meta-Analysis. Medicine 2015, 94, e2028. [Google Scholar] [CrossRef]
- Harris, T.C.; de Rooij, R.; Kuhl, E. The Shrinking Brain: Cerebral Atrophy Following Traumatic Brain Injury. Ann. Biomed. Eng. 2019, 47, 1941–1959. [Google Scholar] [CrossRef]
- Wightman, D.P.; Jansen, I.E.; Savage, J.E.; Shadrin, A.A.; Bahrami, S.; Rongve, A.; Børte, S.; Winsvold, B.S.; Drange, O.K.; Martinsen, A.E.; et al. Largest GWAS (N=1,126,563) of Alzheimer’s Disease Implicates Microglia and Immune Cells. medRxiv 2020. [Google Scholar] [CrossRef]
- Blasco, M.A. Telomeres and human disease: Ageing, cancer and beyond. Nat. Rev. Genet. 2005, 6, 611–622. [Google Scholar] [CrossRef]
- Symons, G.F.; Clough, M.; O’Brien, W.T.; Ernest, J.; Salberg, S.; Costello, D.; Sun, M.; Brady, R.D.; McDonald, S.J.; Wright, D.K.; et al. Shortened telomeres and serum protein biomarker abnormalities in collision sport atheletes regardless of concussion history and sex. J. Concussion 2020, 4, 1–11. [Google Scholar] [CrossRef]
- Li, X.; Ploner, A.; Wang, Y.; Magnusson, P.K.; Reynolds, C.; Finkel, D.; Pedersen, N.L.; Jylhävä, J.; Hägg, S. Longitudinal trajectories, correlations and mortality associations of nine biological ages across 20-years follow-up. eLife 2020, 9, e51507. [Google Scholar] [CrossRef] [PubMed]
- Di Battista, A.P.; Churchill, N.; Rhind, S.G.; Richards, D.; Hutchison, M.G. The relationship between symptom burden and systemic inflammation differs between male and female athletes following concussion. BMC Immunol. 2020, 21, 11. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W.T.; Symons, G.F.; Bain, J.; Major, B.P.; Costello, D.M.; Sun, M.; Kimpton, J.S.; Chen, Z.; Brady, R.D.; Mychasiuk, R.; et al. Elevated serum interleukin-1β levels in male, but not female, collision sport athletes with a concussion history. J. Neurotrauma 2020. [Google Scholar] [CrossRef] [PubMed]
- Major, B.P.; McDonald, S.J.; O’Brien, W.T.; Symons, G.F.; Clough, M.; Costello, D.; Sun, M.; Brady, R.D.; Mccullough, J.; Aniceto, R.; et al. Serum Protein Biomarker Findings Reflective of Oxidative Stress and Vascular Abnormalities in Male, but Not Female, Collision Sport Athletes. Front. Neurol. 2020, 11, 549624. [Google Scholar] [CrossRef]
- Povlishock, J.T.; Becker, D.P.; Miller, J.D.; Jenkins, L.W.; Dietrich, W.D. The morphopathologic substrates of concussion? Acta Neuropathol. 1979, 47, 1–11. [Google Scholar] [CrossRef]
- Browne, K.D.; Chen, X.H.; Meaney, D.F.; Smith, D.H. Mild traumatic brain injury and diffuse axonal injury in swine. J. Neurotrauma 2011, 28, 1747–1755. [Google Scholar] [CrossRef]
- Garman, R.H.; Jenkins, L.W.; Switzer, R.C., 3rd; Bauman, R.A.; Tong, L.C.; Swauger, P.V.; Parks, S.A.; Ritzel, D.V.; Dixon, C.E.; Clark, R.S.B.; et al. Blast exposure in rats with body shielding is characterized primarily by diffuse axonal injury. J. Neurotrauma 2011, 28, 947–959. [Google Scholar] [CrossRef]
- Delano-Wood, L.; Bangen, K.J.; Sorg, S.F.; Clark, A.L.; Schiehser, D.M.; Luc, N.; Bondi, M.W.; Werhane, M.; Kim, R.T.; Bigler, E.D. Brainstem white matter integrity is related to loss of consciousness and postconcussive symptomatology in veterans with chronic mild to moderate traumatic brain injury. Brain Imaging Behav. 2015, 9, 500–512. [Google Scholar] [CrossRef]
- Iseki, E.; Matsushita, M.; Kosaka, K.; Kondo, H.; Ishii, T.; Amano, N. Distribution and morphology of brain stem plaques in Alzheimer’s disease. Acta Neuropathol. 1989, 78, 131–136. [Google Scholar] [CrossRef]
- Taylor, W.D.; Hsu, E.; Krishnan, K.R.; MacFall, J.R. Diffusion tensor imaging: Background, potential, and utility in psychiatric research. Biol. Psychiatry 2004, 55, 201–207. [Google Scholar] [CrossRef]
- Bramlett, H.M.; Dietrich, W.D. Progressive damage after brain and spinal cord injury: Pathomechanisms and treatment strategies. Prog. Brain Res. 2007, 161, 125–141. [Google Scholar] [PubMed]
- Sharp, D.J.; Ham, T.E. Investigating white matter injury after mild traumatic brain injury. Curr. Opin. Neurol. 2011, 24, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Bigler, E.D. Neuropsychological results and neuropathological findings at autopsy in a case of mild traumatic brain injury. J. Int. Neuropsychol. Soc. JINS 2004, 10, 794–806. [Google Scholar] [CrossRef] [PubMed]
- Scott, G.; Ramlackhansingh, A.F.; Edison, P.; Hellyer, P.; Cole, J.; Veronese, M.; Leech, R.; Greenwood, R.J.; Turkheimer, F.E.; Gentleman, S.M.; et al. Amyloid pathology and axonal injury after brain trauma. Neurology 2016, 86, 821–828. [Google Scholar] [CrossRef]
- Choo, I.H.; Lee, D.Y.; Oh, J.S.; Lee, J.S.; Lee, D.S.; Song, I.C.; Youn, J.C.; Kim, S.G.; Kim, K.W.; Jhoo, J.H.; et al. Posterior cingulate cortex atrophy and regional cingulum disruption in mild cognitive impairment and Alzheimer’s disease. Neurobiol. Aging. 2010, 31, 772–779. [Google Scholar] [CrossRef]
- Firbank, M.J.; Blamire, A.M.; Krishnan, M.S.; Teodorczuk, A.; English, P.; Gholkar, A.; Harrison, R.; O’Brien, J.T. Atrophy is associated with posterior cingulate white matter disruption in dementia with Lewy bodies and Alzheimer’s disease. NeuroImage 2007, 36, 1–7. [Google Scholar] [CrossRef]
- Villain, N.; Desgranges, B.; Viader, F.; de la Sayette, V.; Mézenge, F.; Landeau, B.; Landeau, B.; Baron, J.-C.; Eustache, F.; Chételat, G. Relationships between hippocampal atrophy, white matter disruption, and gray matter hypometabolism in Alzheimer’s disease. J. Neurosci. 2008, 28, 6174–61781. [Google Scholar] [CrossRef]
- Zhang, J.; Tian, L.; Zhang, L.; Cheng, R.; Wei, R.; He, F.; Li, J.; Luo, B.; Ye, X. Relationship between white matter integrity and post-traumatic cognitive deficits: A systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 98–107. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Overall | APOEɛ4(−) | APOEɛ4(+) | p-Value |
|---|---|---|---|---|
| (n = 123) | (n = 75) | (n = 48) | ||
| Age years, mean (SD) | 39.3 (14.0) | 40.7 (14.2) | 37.3 (13.6) | 0.19 |
| Gender (n, %) | ||||
| - male | 75 (61) | 45 (60) | 30 (62) | 0.78 |
| - female | 48 (39) | 30 (40) | 18 (38) | |
| Education (years) | 14.7 (2.8) | 14.9 (2.5) | 14.3 (3.3) | 0.33 |
| Mechanism of injury (n, %) | ||||
| - Traffic accidents | 52 (42) | 31 (41) | 21(43) | 0.63 |
| - Falls | 46 (37) | 31 (41) | 15 (31) | |
| - Violence | 13 (11) | 7 (10) | 6 (13) | |
| - Other | 12 (10) | 6 (8) | 6 (13) | |
| GCS | ||||
| 13 | 6 (5) | 4 (5) | 2 (4) | 0.55 |
| 14 | 29 (24) | 20(27) | 9 (19) | |
| 15 | 88 (71) | 51(68) | 37(77) | |
| LOC (n, %) | ||||
| - no | 25 (20) | 18 (24) | 7 (15) | 0.21 |
| - yes/unknown | 98 (80) | 57 (76) | 41(85) | |
| PTA (n, %) | ||||
| - no amnesia | 12 (10) | 9 (12) | 3 (6) | 0.29 |
| - yes/unknown | 111 (90) | 66 (88) | 45(94) | |
| Complicated | ||||
| -no | 67 (54) | 41 (55) | 26 (54) | 0.96 |
| - yes | 56 (46) | 34 (45) | 22 (46) | |
| Coil (n, %) | ||||
| -HNS | 37 (30) | 20 (27) | 17 (35) | 0.3 |
| -8HRBRAIN | 86 (70) | 55 (73) | 31 (65) |
| Variables | Overall (n = 123) | APOEɛ4(−) (n = 75) | APOEɛ4 (+) (n = 48) | p-Value |
|---|---|---|---|---|
| RPQ total | ||||
| Mean (SD) | 13.12 (13.81) | 12.23 (13.54) | 14.52 (14.26) | 0.38 |
| GOSE | ||||
| Mean (SD) | 7.20 (.82) | 7.21 (.84) | 7.19 (.79) | 0.86 |
| PHQ 9 | ||||
| Mean (SD) | 6.50 (5.16) | 6.23 (4.83) | 6.94 (5.66) | 0.47 |
| Model Performance—Training Sample (Cam-CAN) | ||||||
| Model | R2 | RMSE | MAE | R2nestedCV | RMSEnestedCV | MAEnestedCV |
| DTI | 0.82 ± 0.03 | 7.81 ± 0.48 | 6.17 ± 0.40 | 0.82 ± 0.03 | 7.75 ± 0.62 | 6.13 ± 0.52 |
| T1 | 0.81 ± 0.03 | 7.97 ± 0.50 | 6.26 ± 0.42 | 0.81 ± 0.02 | 8.07 ± 0.29 | 6.39 ± 0.21 |
| Model Performance—Test Sample (MTBI) | ||||||
| Model | R2 | RMSE | MAE | R2 corr | RMSE corr | MAE corr |
| DTI | 0.58 | 11.89 | 9.76 | 0.76 | 9.01 | 7.48 |
| T1 | 0.56 | 10.35 | 8.63 | 0.78 | 7.65 | 6.20 |
| Brain Age Gap | Comparison Groups | |||
|---|---|---|---|---|
| APOE-ɛ4(−) vs. APOE-ɛ4(+) | ||||
| B | SE | p-Value | R2 | |
| T1w-based: | 0.054 | |||
| -APOE ɛ4 | 0.790 | 1.404 | 0.58 | |
| -Age (per year) | 0.032 | 0.050 | 0.52 | |
| -Sex | 1.791 | 1.424 | 0.21 | |
| -Head coil | −3.328 | 1.508 | 0.03 | |
| DTI-based: | 0.119 | |||
| -APOE ɛ4 | −2.564 | 1.563 | 0.1 | |
| -Age (per year) | 0.131 | 0.056 | 0.02 | |
| -Sex | −3.614 | 1.586 | 0.02 | |
| -Head Coil | −3.425 | 1.679 | 0.04 | |
| ROI | APOE-ɛ4(−) (n = 75) | APOE-ɛ4(+) (n = 48) | p-Value | ||
|---|---|---|---|---|---|
| Mean mm3 | SD mm3 | Mean mm3 | SD mm3 | ||
| Total ICV | 1.584767 | 152.613 | 1.571603 | 150.490 | 0.64 |
| Total gray volume | 662.282 | 66.495 | 664.349 | 64.095 | 0.87 |
| Cortex volume | 491.343 | 51.833 | 492.455 | 47.444 | 0.91 |
| L Accumbens area | 645 | 137 | 688 | 135 | 0.09 |
| R Accumbens area | 649 | 125 | 636 | 131 | 0.59 |
| L Amygdala | 1597 | 233 | 1607 | 195 | 0.81 |
| R Amygdala | 1843 | 249 | 1852 | 240 | 0.84 |
| Brainstem | 21,267 | 2108 | 20.485 | 2514 | 0.06 |
| L Caudate | 3815 | 573 | 3954 | 517 | 0.18 |
| R Caudate | 3999 | 629 | 4195 | 568 | 0.08 |
| CC-posterior | 990 | 147 | 982 | 168 | 0.78 |
| CC-mid-posterior | 432 | 91 | 402 | 89 | 0.08 |
| CC-central | 437 | 78 | 414 | 84 | 0.13 |
| CC-mid-anterior | 456 | 94 | 442 | 79 | 0.39 |
| CC-anterior | 905 | 144 | 890 | 141 | 0.58 |
| L Hippocampus | 4555 | 542 | 4480 | 478 | 0.44 |
| R Hippocampus | 4551 | 467 | 4576 | 446 | 0.78 |
| L Pallidum | 1337 | 296 | 1308 | 312 | 0.61 |
| R Pallidum | 1596 | 280 | 1558 | 291 | 0.47 |
| L Putamen | 60,441 | 892 | 6009 | 1009 | 0.84 |
| R Putamen | 5946 | 796 | 6009 | 856 | 0.68 |
| L Thalamus | 8612 | 1183 | 8603 | 1068 | 0.97 |
| R Thalamus | 6983 | 913 | 6975 | 900 | 0.96 |
| L lateral Ventricle | 9760 | 5507 | 10.717 | 6399 | 0.38 |
| R lateral Ventricle | 9068 | 6041 | 8983 | 4994 | 0.93 |
| ROI | APOE-ɛ4(−) (n = 75) | APOE-ɛ4(+) (n = 48) | p-Value | ||
|---|---|---|---|---|---|
| Mean mm | SD mm | Mean mm | SD mm | ||
| L hemisphere, mean | 2.51 | 0.127 | 2.52 | 0.105 | 0.46 |
| R hemisphere, mean | 2.48 | 0.118 | 2.49 | 0.099 | 0.50 |
| L frontal | 2.51 | 0.145 | 2.51 | 0.126 | 0.95 |
| R frontal | 2.43 | 0.124 | 2.44 | 0.115 | 0.85 |
| L temporal | 2.95 | 0.151 | 2.97 | 0.136 | 0.45 |
| R temporal | 2.89 | 0.149 | 2.90 | 0.131 | 0.48 |
| L parietal | 2.29 | 0.132 | 2.30 | 0.139 | 0.67 |
| R parietal | 2.30 | 0.146 | 2.31 | 0.121 | 0.67 |
| L cingulate | 2.58 | 0.175 | 2.62 | 0.201 | 0.21 |
| R cingulate | 2.61 | 0.196 | 2.59 | 0.167 | 0.59 |
| L occipital | 2.04 | 0.111 | 2.05 | 0.100 | 0.55 |
| R occipital | 2.06 | 0.120 | 2.07 | 0.100 | 0.64 |
| L insula | 3.08 | 0.175 | 3.10 | 0.130 | 0.62 |
| R insula | 3.03 | 0.171 | 3.04 | 0.166 | 0.72 |
| ROI | Comparison Groups | |||
|---|---|---|---|---|
| APOE-ɛ4(−) vs. APOE-ɛ44(+) | ||||
| B | SE | p-Value | R2 | |
| Total ICV | −13698 | 23822 | 0.57 | 0.312 |
| Total gray volume | −1932.9 | 5208.5 | 0.71 | 0.825 |
| Cortex volume | −1125.3 | 4541.6 | 0.81 | 0.773 |
| L Accumbens area | 22.527 | 19.780 | 0.26 | 0.428 |
| R Accumbens area | −24.698 | 19.020 | 0.20 | 0.382 |
| L Amygdala | −6.604 | 33.963 | 0.85 | 0.334 |
| R Amygdala | 12.443 | 42.132 | 0.77 | 0.185 |
| Brain Stem | −710.59 | 306.40 | 0.02 | 0.512 |
| L Caudate | 95.763 | 77.147 | 0.22 | 0.468 |
| R Caudate | 135.66 | 83.163 | 0.11 | 0.492 |
| L Hippocampus | −91.780 | 74.287 | 0.22 | 0.434 |
| R Hippocampus | 9.805 | 67.792 | 0.89 | 0.399 |
| L Putamen | −143.81 | 124.25 | 0.25 | 0.516 |
| R Putamen | −53.235 | 97.863 | 0.59 | 0.606 |
| Left Thalamus | 34.182 | 170.03 | 0.84 | 0.384 |
| Right Thalamus | −25.139 | 125.03 | 0.84 | 0.475 |
| CC-posterior | 5.094 | 25.748 | 0.84 | 0.239 |
| CC-mid-poster | −30.256 | 16.590 | 0.07 | 0.089 |
| CC-central | −22.641 | 14.790 | 0.13 | 0.084 |
| CC-mid-anterior | −12.932 | 15.477 | 0.41 | 0.157 |
| CC-anterior | −7.022 | 24.002 | 0.77 | 0.216 |
| L Pallidum | −56.903 | 47.265 | 0.24 | 0.317 |
| R Pallidum | −6.0494 | 41.844 | 0.15 | 0.402 |
| L lateral Ventricle | 1669.5 | 945.24 | 0.08 | 0.287 |
| R lateral Ventricle | 555.08 | 933.86 | 0.55 | 0.246 |
| L hemisphere, mean thick | 0.006 | 0.019 | 0.75 | 0.304 |
| R hemisphere, mean thick | 0.005 | 0.018 | 0.80 | 0.279 |
| L frontal thick | −0.007 | 0.020 | 0.73 | 0.395 |
| R frontal thick | 0.001 | 0.019 | 0.95 | 0.266 |
| L temporal thick | 0.011 | 0.024 | 0.63 | 0.257 |
| R temporal thick | 0.008 | 0.024 | 0.73 | 0.235 |
| L parietal thick | −0.005 | 0.022 | 0.81 | 0.241 |
| R parietal thick | −0.001 | 0.023 | 0.96 | 0.208 |
| L cingulate thick | 0.024 | 0.027 | 0.37 | 0.424 |
| R cingulate thick | −0.029 | 0.028 | 0.30 | 0.351 |
| L occipital thick | 0.004 | 0.019 | 0.82 | 0.129 |
| R occipital thick | 0.002 | 0.020 | 0.94 | 0.129 |
| L insula thick | −0.004 | 0.026 | 0.89 | 0.266 |
| R insula thick | −0.007 | 0.028 | 0.81 | 0.231 |
| ROI | Comparison Groups | |||
|---|---|---|---|---|
| APOE-ɛ4(−) vs. APOE-ɛ4(+) | ||||
| B | SE | p-Value | R2 | |
| FA-ATR L | 0.003 | 0.003 | 0.38 | 0.257 |
| FA-ATR R | 0.003 | 0.003 | 0.32 | 0.253 |
| FA-CG L | 0.001 | 0.004 | 0.87 | 0.317 |
| FA-CG R | 0.000 | 0.004 | 0.93 | 0.200 |
| FA-CING L | −0.011 | 0.005 | 0.03 | 0.214 |
| FA-CING R | −0.011 | 0.004 | 0.01 | 0.222 |
| FA-CST L | 0.001 | 0.003 | 0.83 | 0.253 |
| FA-CST R | −0.002 | 0.003 | 0.61 | 0.289 |
| FA-FMAJ | 0.002 | 0.003 | 0.59 | 0.244 |
| FA-FMIN | 0.004 | 0.004 | 0.26 | 0.430 |
| FA-IFOF L | 0.001 | 0.003 | 0.68 | 0.382 |
| FA-IFOF R | 0.004 | 0.003 | 0.24 | 0.315 |
| FA-ILF L | −0.001 | 0.003 | 0.79 | 0.348 |
| FA-ILF R | −0.001 | 0.003 | 0.86 | 0.274 |
| FA-SLF L | 0.002 | 0.003 | 0.44 | 0.296 |
| FA-SLF R | 0.002 | 0.003 | 0.41 | 0.328 |
| FA-SLFT L | 0.000 | 0.004 | 0.95 | 0.148 |
| FA-SLFT R | 0.002 | 0.003 | 0.60 | 0.277 |
| FA-UF L | 0.002 | 0.003 | 0.54 | 0.209 |
| FA-UF R | 0.004 | 0.003 | 0.18 | 0.206 |
| FA-CCBody | −0.005 | 0.006 | 0.41 | 0.249 |
| FA-CCGenu | 0.004 | 0.005 | 0.41 | 0.346 |
| FA-CCSplenium | 0.002 | 0.004 | 0.64 | 0.196 |
| FA-ws | 0.001 | 0.003 | 0.68 | 0.351 |
| MD-ATR L | 7.319 × 10−6 | 0.000 | 0.24 | 0.133 |
| MD-ATR R | 3.674 × 10−6 | 0.000 | 0.62 | 0.100 |
| MD-CG L | 8.128 × 10−8 | 0.000 | 0.99 | 0.033 |
| MD-CG R | −1.644 × 10−6 | 0.000 | 0.72 | 0.039 |
| MD-CING L | 1.377 × 10−5 | 0.000 | 0.08 | 0.215 |
| MD-CING R | 7.395 × 10−6 | 0.000 | 0.38 | 0.117 |
| MD-CST L | 4.134 × 10−6 | 0.000 | 0.36 | 0.132 |
| MD-CST R | 5.745 × 10−6 | 0.000 | 0.25 | 0.151 |
| MD-FMAJ | 1.775 × 10−7 | 0.000 | 0.97 | 0.362 |
| MD-FMIN | −2.931 × 10−6 | 0.000 | 0.66 | 0.191 |
| MD-IFOF L | −2.129 × 10−6 | 0.000 | 0.66 | 0.063 |
| MD-IFOF R | −5.288 × 10−6 | 0.000 | 0.29 | 0.100 |
| MD-ILF L | −2.673 × 10−6 | 0.000 | 0.60 | 0.060 |
| MD-ILF R | −5.404 × 10−6 | 0.000 | 0.29 | 0.066 |
| MD-SLF L | −7.339 × 10−7 | 0.000 | 0.86 | 0.029 |
| MD-SLF R | −1.968 × 10−6 | 0.000 | 0.65 | 0.051 |
| MD-SLFT L | −2.722 × 10−6 | 0.000 | 0.58 | 0.042 |
| MD-SLFT R | −5.847 × 10−6 | 0.000 | 0.29 | 0.154 |
| MD-UF L | −4.273 × 10−6 | 0.000 | 0.43 | 0.266 |
| MD-UF R | −2.661 × 10−6 | 0.000 | 0.64 | 0.207 |
| MD-CCBody | 5.241 × 10−6 | 0.000 | 0.46 | 0.100 |
| MD-CCGenu | −2.526 × 10−8 | 0.000 | 0.99 | 0.159 |
| MD-CCSplenium | 2.404 × 10−6 | 0.000 | 0.70 | 0.213 |
| MD-ws | 2.734 × 10−7 | 0.000 | 0.95 | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hellstrøm, T.; Andelic, N.; de Lange, A.-M.G.; Helseth, E.; Eiklid, K.; Westlye, L.T. Apolipoprotein ɛ4 Status and Brain Structure 12 Months after Mild Traumatic Injury: Brain Age Prediction Using Brain Morphometry and Diffusion Tensor Imaging. J. Clin. Med. 2021, 10, 418. https://doi.org/10.3390/jcm10030418
Hellstrøm T, Andelic N, de Lange A-MG, Helseth E, Eiklid K, Westlye LT. Apolipoprotein ɛ4 Status and Brain Structure 12 Months after Mild Traumatic Injury: Brain Age Prediction Using Brain Morphometry and Diffusion Tensor Imaging. Journal of Clinical Medicine. 2021; 10(3):418. https://doi.org/10.3390/jcm10030418
Chicago/Turabian StyleHellstrøm, Torgeir, Nada Andelic, Ann-Marie G. de Lange, Eirik Helseth, Kristin Eiklid, and Lars T. Westlye. 2021. "Apolipoprotein ɛ4 Status and Brain Structure 12 Months after Mild Traumatic Injury: Brain Age Prediction Using Brain Morphometry and Diffusion Tensor Imaging" Journal of Clinical Medicine 10, no. 3: 418. https://doi.org/10.3390/jcm10030418
APA StyleHellstrøm, T., Andelic, N., de Lange, A.-M. G., Helseth, E., Eiklid, K., & Westlye, L. T. (2021). Apolipoprotein ɛ4 Status and Brain Structure 12 Months after Mild Traumatic Injury: Brain Age Prediction Using Brain Morphometry and Diffusion Tensor Imaging. Journal of Clinical Medicine, 10(3), 418. https://doi.org/10.3390/jcm10030418