
The Vitamin D Role in Preventing Primary Headache in Adult and Pediatric Population

 ,
,  ,
, 

Abstract
1. Introduction
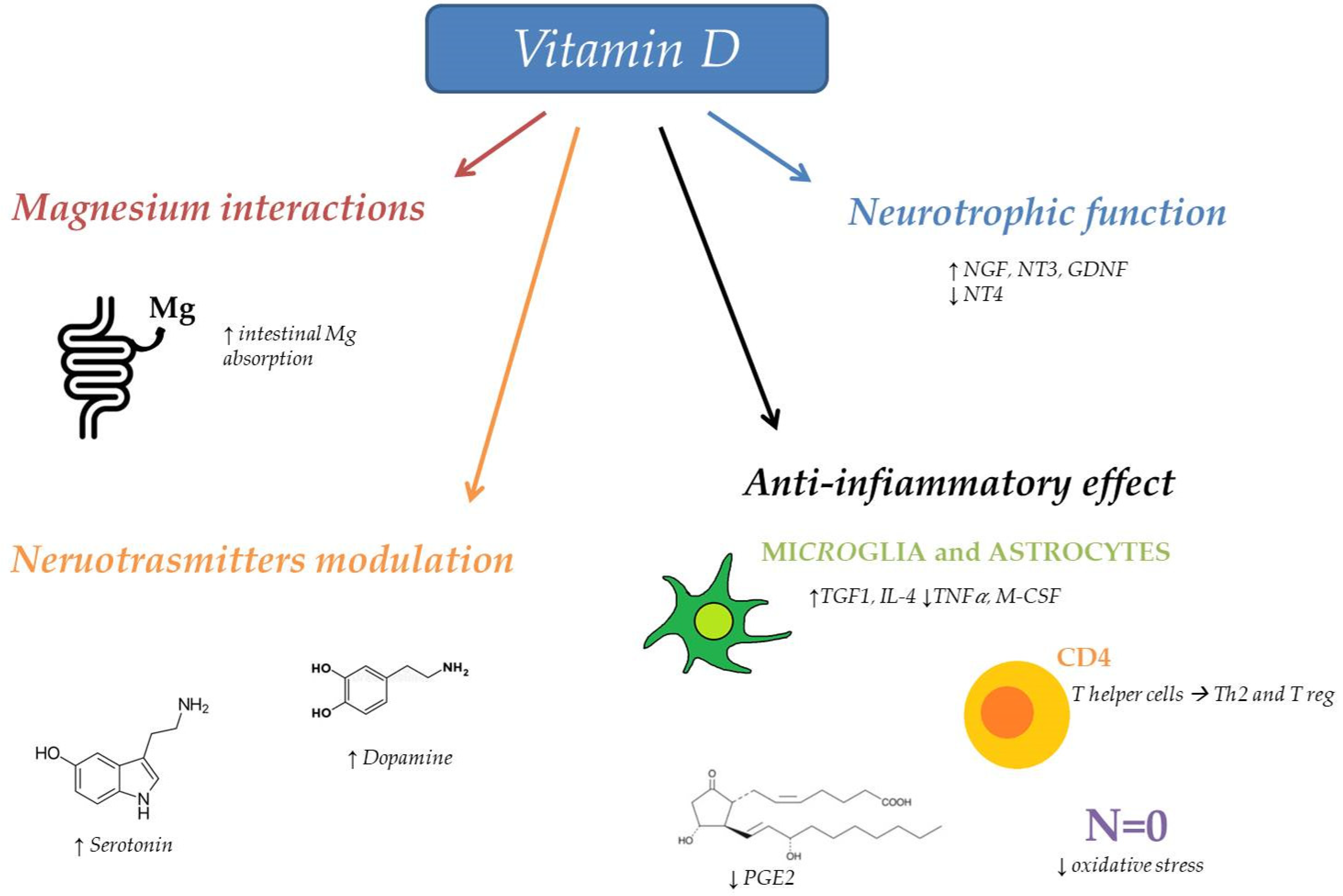
2. Vitamin D and Brain
3. Vitamin D and Headache
4. Vitamin D Prophylaxis in Adult Headache

{kind=link}
| Reference | Study Design | Sample Size (Mean Age) | Type of Headache | Dose of Vitamin D Supplementation | Treatment Duration | Results |
|---|---|---|---|---|---|---|
| Gazerani (2019) [67] | Randomized, double-blind, placebo-controlled, parallel | 48 (45.5 y) | Migraine | 100 μg/day | 196 days | Decreased migraine frequency, no effect on severity, pressure pain thresholds, or temporal summation. |
| Mottaghi (2015) [62] | Randomized, double-blind placebo-controlled | 65 (Group 1 32.7 ± 10.6 y; Group 2 33.9 ± 11.6 y) | Migraine | 50,000 IU/week | 10 weeks | Decreased headache frequency and mean headache diary results, no effect on severity and duration of headache. |
| Buettner (2015) [68] | Randomized, placebo-controlled | 57 (40 y) | Episodic migraine | 1000 IU twice per day (+ simvastatin 20 mg/twice per day) | 24 weeks | Decreased number of migraine days |
| Ghorbani (2020) [69] | Randomized double-blind placebo-controlled trial | 80 (Group1 37 y; Group 2 38 y) | Episodic migraine | 2000 IU/day | 12 weeks | Significantly lower headache days per month, reduced attacks duration, less severe headaches and lower analgesics use/month |
| Ghorbani (2020) [71] | Randomized double-blind placebo-controlled trial | 80 (Group1 37 y; Group 2 38 y) | Episodic migraine | 2000 IU/day | 16 weeks | CGRP level appeared to be significantly lower following vitamin D supplementation. Improved headache characteristics and disability |
| Ghorbani (2021) [72] | Randomized double-blind placebo-controlled trial | 80 (Group1 37 y; Group 2 38 y) | Episodic migraine | 2000 IU/day | 12 weeks | Enhanced Th17/Treg related cytokines balance in episodic migraineurs. |
| Yilmaz (2016) [73] | Pre-post | 29 (36.9 y) | Headache | 50,000 IU/weekly + calcium of 1000 mg/day | 3 months | Decreased headache severity and frequency. |
| Knutsen (2014) [74] | Randomized double-blinded placebo-controlled parallel-group | 158 (35–40 y) | Headache | Group 1: 25 g/day Group 2: 10 g/day | 16 weeks | No effect on occurrence, anatomical localization, and degree of pain parameters or headache frequency. |
| Rist (2021) [75] | Randomized, double-blind, placebo-controlled trial | 1032 (65.6 y) | Migraine | 2000 IU/day or marine n-3 fatty acid (1 g/d) | 5.3 years (median) | No changes in migraine frequency or severity based on self-report |
| Batcheller (2014) [78] | Prospective | — | Cluster headache | 10,000 IU/day | 30 days | Decreased frequency, severity, and duration of headache in 80% of patients. |
5. Vitamin D Profilaxis in Pediatric Headache
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stovner, L.J.; Hagen, K.; Jensen, R.; Katsarava, Z.; Lipton, R.; Scher, A.; Steiner, T.; Zwart, J.A. The global burden of headache: A documentation of headache prevalence and disability worldwide. Cephalalgia 2007, 27, 193–210. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef]
- Genizi, J.; Srugo, I.; Kerem, N.C. The cross-ethnic variations in the prevalence of headache and other somatic complaints among adolescents in Northern Israel. J. Headache Pain 2013, 14, 21. [Google Scholar] [CrossRef]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Stewart, W.F.; Wood, G.C.; Manack, A.; Varon, S.F.; Buse, D.C.; Lipton, R.B. Employment and work impact of chronic migraine and episodic migraine. J. Occup. Environ. Med. 2010, 52, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Torres-Ferrus, M.; Vila-Sala, C.; Quintana, M.; Ajanovic, S.; Gallardo, V.J.; Gomez, J.B.; Alvarez-Sabin, J.; Macaya, A.; Pozo-Rosich, P. Headache, comorbidities and lifestyle in an adolescent population (The TEENs Study). Cephalalgia 2019, 39, 91–99. [Google Scholar] [CrossRef]
- Verrotti, A.; Di Fonzo, A.; Penta, L.; Agostinelli, S.; Parisi, P. Obesity and headache/migraine: The importance of weight reduction through lifestyle modifications. BioMed Res. Int. 2014, 2014, 420858. [Google Scholar] [CrossRef] [PubMed]
- Orr, S.L. The Evidence for the Role of Nutraceuticals in the Management of Pediatric Migraine: A Review. Curr. Pain Headache Rep. 2018, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, F.; Saba, A.; Zucchi, R. An Update on Vitamin D Metabolism. Int. J. Mol. Sci. 2020, 21, 6573. [Google Scholar] [CrossRef] [PubMed]
- Nowaczewska, M.; Wiciński, M.; Osiński, S.; Kaźmierczak, H. The Role of Vitamin D in Primary Headache-from Potential Mechanism to Treatment. Nutrients 2020, 12, 243. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani, Z.; Togha, M.; Rafiee, P.; Ahmadi, Z.S.; Rasekh Magham, R.; Haghighi, S.; Razeghi Jahromi, S.; Mahmoudi, M. Vitamin D in migraine headache: A comprehensive review on literature. Neurol. Sci. 2019, 40, 2459–2477. [Google Scholar] [CrossRef]
- Anjum, I.; Jaffery, S.S.; Fayyaz, M.; Samoo, Z.; Anjum, S. The Role of Vitamin D in Brain Health: A Mini Literature Review. Cureus 2018, 10, e2960. [Google Scholar] [CrossRef]
- Jeon, S.M.; Shin, E.A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2018, 50, 1–14. [Google Scholar] [CrossRef]
- Łukaszyk, E.; Bień-Barkowska, K.; Bień, B. Cognitive Functioning of Geriatric Patients: Is Hypovitaminosis D the Next Marker of Cognitive Dysfunction and Dementia? Nutrients 2018, 10, 1104. [Google Scholar] [CrossRef] [PubMed]
- Hiller, A.L.; Murchison, C.F.; Lobb, B.M.; O’Connor, S.; O’Connor, M.; Quinn, J.F. A randomized, controlled pilot study of the effects of vitamin D supplementation on balance in Parkinson’s disease: Does age matter? PLoS ONE 2018, 13, e0203637. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Souberbielle, J.C. Vitamin D and multiple sclerosis: An update. Mult. Scler. Relat. Disord. 2017, 14, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Bivona, G.; Gambino, C.M.; Iacolino, G.; Ciaccio, M. Vitamin D and the nervous system. Neurol. Res. 2019, 41, 827–835. [Google Scholar] [CrossRef]
- Cui, X.; Gooch, H.; Petty, A.; McGrath, J.J.; Eyles, D. Vitamin D and the brain: Genomic and non-genomic actions. Mol. Cell. Endocrinol. 2017, 453, 131–143. [Google Scholar] [CrossRef]
- Eyles, D.W.; Burne, T.H.; McGrath, J.J. Vitamin D, effects on brain development, adult brain function and the links between low levels of vitamin D and neuropsychiatric disease. Front. Neuroendocrinol. 2013, 34, 47–64. [Google Scholar] [CrossRef] [PubMed]
- Gezen-Ak, D.; Dursun, E.; Yilmazer, S. The Effect of Vitamin D Treatment On Nerve Growth Factor (NGF) Release From Hippocampal Neurons. Noro Psikiyatr. Ars. 2014, 51, 157–162. [Google Scholar] [CrossRef]
- Carlberg, C. Genome-wide (over)view on the actions of vitamin D. Front. Physiol. 2014, 5, 167. [Google Scholar] [CrossRef]
- Cui, X.; McGrath, J.J.; Burne, T.H.; Mackay-Sim, A.; Eyles, D.W. Maternal vitamin D depletion alters neurogenesis in the developing rat brain. Int. J. Dev. Neurosci. 2007, 25, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.; Brown, J.; Mackay-Sim, A.; McGrath, J.; Feron, F. Vitamin D3 and brain development. Neuroscience 2003, 118, 641–653. [Google Scholar] [CrossRef]
- Brewer, L.D.; Thibault, V.; Chen, K.C.; Langub, M.C.; Landfield, P.W.; Porter, N.M. Vitamin D hormone confers neuroprotection in parallel with downregulation of L-type calcium channel expression in hippocampal neurons. J. Neurosci. 2001, 21, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Langub, M.C.; Herman, J.P.; Malluche, H.H.; Koszewski, N.J. Evidence of functional vitamin D receptors in rat hippocampus. Neuroscience 2001, 104, 49–56. [Google Scholar] [CrossRef]
- Glaser, S.D.; Veenstra, T.D.; Jirikowski, G.F.; Prüfer, K. Distribution of 1,25-dihydroxyvitamin D3 receptor immunoreactivity in the rat olfactory system. Cell. Mol. Neurobiol. 1999, 19, 613–624. [Google Scholar] [CrossRef]
- Cui, X.; Pelekanos, M.; Liu, P.Y.; Burne, T.H.; McGrath, J.J.; Eyles, D.W. The vitamin D receptor in dopamine neurons; its presence in human substantia nigra and its ontogenesis in rat midbrain. Neuroscience 2013, 236, 77–87. [Google Scholar] [CrossRef]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the vitamin D receptor and 1 alpha-hydroxylase in human brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef]
- Almeras, L.; Eyles, D.; Benech, P.; Laffite, D.; Villard, C.; Patatian, A.; Boucraut, J.; Mackay-Sim, A.; McGrath, J.; Féron, F. Developmental vitamin D deficiency alters brain protein expression in the adult rat: Implications for neuropsychiatric disorders. Proteomics 2007, 7, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Grecksch, G.; Rüthrich, H.; Höllt, V.; Becker, A. Transient prenatal vitamin D deficiency is associated with changes of synaptic plasticity in the dentate gyrus in adult rats. Psychoneuroendocrinology 2009, 1, S258–S264. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Pelekanos, M.; Burne, T.H.; McGrath, J.J.; Eyles, D.W. Maternal vitamin D deficiency alters the expression of genes involved in dopamine specification in the developing rat mesencephalon. Neurosci. Lett. 2010, 486, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Trinko, J.R.; Land, B.B.; Solecki, W.B.; Wickham, R.J.; Tellez, L.A.; Maldonado-Aviles, J.; de Araujo, I.E.; Addy, N.A.; DiLeone, R.J. Vitamin D3: A Role in Dopamine Circuit Regulation, Diet-Induced Obesity, and Drug Consumption. eNeuro 2016, 3, ENEURO 0122-15. [Google Scholar] [CrossRef]
- Jiang, P.; Zhang, L.H.; Cai, H.L.; Li, H.D.; Liu, Y.P.; Tang, M.M.; Dang, R.L.; Zhu, W.Y.; Xue, Y.; He, X. Neurochemical effects of chronic administration of calcitriol in rats. Nutrients 2014, 6, 6048–6059. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Makwana, P.; Rathore, C. Vitamin D deficiency mimicking chronic tension-type headache in children. BMJ Case Rep. 2016, 2, bcr2015213833. [Google Scholar] [CrossRef] [PubMed]
- Donmez, A.; Orun, E.; Sonmez, F.M. Vitamin D status in children with headache: A case-control study. Clin. Nutr. ESPEN 2018, 23, 222–227. [Google Scholar] [CrossRef]
- Kılıç, B.; Kılıç, M. Evaluation of Vitamin D Levels and Response to Therapy of Childhood Migraine. Medicina 2019, 55, 321. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Kumar, M.; Belani, P.; Susvirkar, A.; Ahuja, S. Interrelationships between chronic tension-type headache, musculoskeletal pain, and vitamin D deficiency: Is osteomalacia responsible for both headache and musculoskeletal pain? Ann. Indian Acad. Neurol. 2013, 16, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Mottaghi, T.; Khorvash, F.; Askari, G.; Maracy, M.R.; Ghiasvand, R.; Maghsoudi, Z.; Iraj, B. The relationship between serum levels of vitamin D and migraine. J. Res. Med. Sci. 2013, 18, S66–S70. [Google Scholar]
- Togha, M.; Razeghi Jahromi, S.; Ghorbani, Z.; Martami, F.; Seifishahpar, M. Serum Vitamin D Status in a Group of Migraine Patients Compared With Healthy Controls: A Case-Control Study. Headache 2018, 58, 1530–1540. [Google Scholar] [CrossRef]
- Prakash, S.; Mehta, N.C.; Dabhi, A.S.; Lakhani, O.; Khilari, M.; Shah, N.D. The prevalence of headache may be related with the latitude: A possible role of Vitamin D insufficiency? J. Headache Pain 2010, 11, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Holland, P.R. An Update: Pathophysiology of Migraine. Neurol. Clin. 2019, 37, 651–671. [Google Scholar] [CrossRef]
- Burstein, R.; Noseda, R.; Borsook, D. Migraine: Multiple processes, complex pathophysiology. J. Neurosci. 2015, 35, 6619–6629. [Google Scholar] [CrossRef]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, sensitization, and modulation of pain. Pain 2013, 54, S44–S53. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R. Understanding migraine: Potential role of neurogenic inflammation. Ann. Indian Acad. Neurol. 2016, 19, 175–182. [Google Scholar] [CrossRef]
- Qubty, W.; Patniyot, I. Migraine Pathophysiology. Pediatr. Neurol. 2020, 107, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Burstein, R.; Kainz, V.; Jakubowski, M.; Strassman, A.M. Mast cell degranulation activates a pain pathway underlying migraine headache. Pain 2007, 130, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Dolati, S.; Rikhtegar, R.; Mehdizadeh, A.; Yousefi, M. The Role of Magnesium in Pathophysiology and Migraine Treatment. Biol. Trace Elem. Res. 2020, 196, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Gross, E.C.; Lisicki, M.; Fischer, D.; Sándor, P.S.; Schoenen, J. The metabolic face of migraine-from pathophysiology to treatment. Nat. Rev. Neurol. 2019, 15, 627–643. [Google Scholar] [CrossRef]
- Hoffmann, J.; Charles, A. Glutamate and Its Receptors as Therapeutic Targets for Migraine. Neurotherapeutics 2018, 15, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, M.; Puri, V.; Puri, S. Serotonin and CGRP in migraine. Ann. Neurosci. 2012, 19, 88–94. [Google Scholar] [CrossRef] [PubMed]
- May, A.; Burstein, R. Hypothalamic regulation of headache and migraine. Cephalalgia 2019, 39, 1710–1719. [Google Scholar] [CrossRef]
- Mier, R.W.; Dhadwal, S. Primary Headaches. Dent. Clin. N. Am. 2018, 62, 611–628. [Google Scholar] [CrossRef] [PubMed]
- Jay, G.W.; Barkin, R.L. Primary Headache Disorders-Part 2: Tension-type headache and medication overuse headache. Dis. Mon. 2017, 63, 342–367. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, J.C.A.; Viganò, A.; Alekseeva, A.; Alieva, E.; Arruda, R.; De Luca, C.; D’Ettore, N.; Frattale, I.; Kurnukhina, M.; Macerola, N.; et al. European Headache Federation School of Advanced Studies (EHF-SAS). The fifth cranial nerve in headaches. J. Headache Pain 2020, 21, 65. [Google Scholar] [CrossRef] [PubMed]
- De Tommaso, M.; Fernández-de-Las-Penas, C. Tension Type Headache. Curr. Rheumatol. Rev. 2016, 12, 127–139. [Google Scholar] [CrossRef]
- Ashina, S.; Bendtsen, L.; Ashina, M. Pathophysiology of tension-type headache. Curr. Pain Headache Rep. 2005, 9, 415–422. [Google Scholar] [CrossRef]
- Wei, D.Y.; Yuan Ong, J.J.; Goadsby, P.J. Cluster Headache: Epidemiology, Pathophysiology, Clinical Features, and Diagnosis. Ann. Indian Acad. Neurol. 2018, 21, S3–S8. [Google Scholar] [CrossRef]
- Helde-Frankling, M.; Björkhem-Bergman, L. Vitamin D in Pain Management. Int. J. Mol. Sci. 2017, 18, 2170. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. Vitamin D and immune function: An overview. Proc. Nutr. Soc. 2012, 71, 50–61. [Google Scholar] [CrossRef]
- Liu, X.; Nelson, A.; Wang, X.; Farid, M.; Gunji, Y.; Ikari, J.; Iwasawa, S.; Basma, H.; Feghali-Bostwick, C.; Rennard, S.I. Vitamin D modulates prostaglandin E2 synthesis and degradation in human lung fibroblasts. Am. J. Respir. Cell Mol. Biol. 2014, 50, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Garcion, E.; Wion-Barbot, N.; Montero-Menei, C.N.; Berger, F.; Wion, D. New clues about vitamin D functions in the nervous system. Trends Endocrinol. Metab. 2002, 13, 100–105. [Google Scholar] [CrossRef]
- Mottaghi, T.; Askari, G.; Khorvash, F.; Maracy, M.R. Effect of Vitamin D supplementation on symptoms and C-reactive protein in migraine patients. J. Res. Med. Sci. 2015, 20, 477–482. [Google Scholar] [CrossRef]
- Filgueiras, M.S.; Rocha, N.P.; Novaes, J.F.; Bressan, J. Vitamin D status, oxidative stress, and inflammation in children and adolescents: A systematic review. Crit. Rev. Food Sci. Nutr. 2020, 60, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, A.E.; Sarlo, G.L.; Holton, K.F. The Role of Magnesium in Neurological Disorders. Nutrients 2018, 10, 730. [Google Scholar] [CrossRef] [PubMed]
- Shipton, E.A.; Shipton, E.E. Vitamin D and Pain: Vitamin D and Its Role in the Aetiology and Maintenance of Chronic Pain States and Associated Comorbidities. Pain Res. Treat. 2015, 2015, 904967. [Google Scholar] [CrossRef]
- Kaviani, M.; Nikooyeh, B.; Zand, H.; Yaghmaei, P.; Neyestani, T.R. Effects of vitamin D supplementation on depression and some involved neurotransmitters. J. Affect. Disord. 2020, 269, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Gazerani, P.; Fuglsang, R.; Pedersen, J.G.; Sørensen, J.; Kjeldsen, J.L.; Yassin, H.; Nedergaard, B.S. A randomized, double-blinded, placebo-controlled, parallel trial of vitamin D3 supplementation in adult patients with migraine. Curr. Med. Res. Opin. 2019, 35, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Buettner, C.; Nir, R.R.; Bertisch, S.M.; Bernstein, C.; Schain, A.; Mittleman, M.A.; Burstein, R. Simvastatin and vitamin D for migraine prevention: A randomized, controlled trial. Ann. Neurol. 2015, 78, 970–981. [Google Scholar] [CrossRef]
- Ghorbani, Z.; Togha, M.; Rafiee, P.; Ahmadi, Z.S.; Rasekh Magham, R.; Djalali, M.; Shahemi, S.; Martami, F.; Zareei, M.; Razeghi Jahromi, S.; et al. Vitamin D3 might improve headache characteristics and protect against inflammation in migraine: A randomized clinical trial. Neurol. Sci. 2020, 41, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Lukacs, M.; Tajti, J.; Fulop, F.; Toldi, J.; Edvinsson, L.; Vecsei, L. Migraine, Neurogenic Inflammation, Drug Development-Pharmacochemical Aspects. Curr. Med. Chem. 2017, 24, 3649–3665. [Google Scholar] [CrossRef]
- Ghorbani, Z.; Rafiee, P.; Fotouhi, A.; Haghighi, S.; Rasekh Magham, R.; Ahmadi, Z.S.; Djalali, M.; Zareei, M.; Razeghi Jahromi, S.; Shahemi, S.; et al. The effects of vitamin D supplementation on interictal serum levels of calcitonin gene-related peptide (CGRP) in episodic migraine patients: Post hoc analysis of a randomized double-blind placebo-controlled trial. J. Headache Pain 2020, 21, 22. [Google Scholar] [CrossRef]
- Ghorbani, Z.; Rafiee, P.; Haghighi, S.; Razeghi Jahromi, S.; Djalali, M.; Moradi-Tabriz, H.; Mahmoudi, M.; Togha, M. The effects of vitamin D3 supplementation on TGF-β and IL-17 serum levels in migraineurs: Post hoc analysis of a randomized clinical trial. J. Pharm. Health Care Sci. 2021, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, R.; Salli, A.; Cingoz, H.T.; Kucuksen, S.; Ugurlu, H. Efficacy of vitamin D replacement therapy on patients with chronic nonspecific widespread musculoskeletal pain with vitamin D deficiency. Int. J. Rheum. Dis. 2016, 19, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Knutsen, K.V.; Madar, A.A.; Brekke, M.; Meyer, H.E.; Natvig, B.; Mdala, I.; Lagerløv, P. Effect of vitamin D on musculoskeletal pain and headache: A randomized, double-blind, placebo-controlled trial among adult ethnic minorities in Norway. Pain 2014, 155, 2591–2598. [Google Scholar] [CrossRef] [PubMed]
- Rist, P.M.; Buring, J.E.; Cook, N.R.; Manson, J.E.; Kurth, T. Effect of Vitamin D and/or Marine n-3 Fatty Acid Supplementation on Changes in Migraine Frequency and Severity. Am. J. Med. 2021, 134, 756–762.e5. [Google Scholar] [CrossRef]
- Hoffmann, J.; May, A. Diagnosis, pathophysiology, and management of cluster headache. Lancet Neurol. 2018, 17, 75–83. [Google Scholar] [CrossRef]
- Sohn, J.H.; Chu, M.K.; Park, K.Y.; Ahn, H.Y.; Cho, S.J. Vitamin D deficiency in patients with cluster headache: A preliminary study. J. Headache Pain 2018, 19, 54. [Google Scholar] [CrossRef]
- Batcheller Peter, L. A Survey of Cluster Headache (CH) Sufferers Using Vitamin D3 as a CH Preventative (P1.256). Neurology 2014, 82, 2148. [Google Scholar] [CrossRef]
- U.S. National Library of Medicine. ClinicalTrials.gov. Identifier: NCT04570475. High Dose Vitamin D Plus Multivitamin in the Prevention of Cluster Headache. Available online: https://clinicaltrials.gov/ct2/show/NCT04570475 (accessed on 19 December 2021).
- Tozzi, E.; Boncristiano, A.; Antenucci, A.; Di Loreto, S.; Farello, G. P013. 25(OH)D Level and headache in children sample. J. Headache Pain 2015, 16, A84. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hancı, F.; Kabakuş, N.; Türay, S.; Bala, K.A.; Dilek, M. The role of obesity and vitamin D deficiency in primary headaches in childhood. Acta Neurol. Belg. 2020, 120, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Gallelli, L.; Michniewicz, A.; Cione, E.; Squillace, A.; Colosimo, M.; Pelaia, C.; Fazio, A.; Zampogna, S.; Peltrone, F.; Iannacchero, R.; et al. 25-Hydroxy Vitamin D Detection Using Different Analytic Methods in Patients with Migraine. J. Clin. Med. 2019, 8, 895. [Google Scholar] [CrossRef] [PubMed]
- Onofri, A.; Necozione, S.; Tozzi, E. Complementary and alternative medicine (CAM) in headache of children and adolescents: Open-label Italian study. Clin. Ter. 2020, 171, e393–e398. [Google Scholar] [CrossRef] [PubMed]
- Cayir, A.; Turan, M.I.; Tan, H. Effect of vitamin D therapy in addition to amitriptyline on migraine attacks in pediatric patients. Braz. J. Med. Biol. Res. 2014, 47, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Potrykus, A.; Pilarska, F. The role of vitamin D supply and its impact on headaches in children and teenagers. Eur. J. Paediatr. Neurol. 2013, 17, S81. [Google Scholar] [CrossRef]

| Reference | Study Design | Sample Size (Mean Age) | Type of Headache | Dose of Vitamin D Supplementation | Treatment Duration | Results |
|---|---|---|---|---|---|---|
| Onofri (2020) [83] | Open label study | 99 (6–17 y) | Migraine and TTH | Patients were administered 3 different compounds, one containing vitamin D | — | Reduction of migraine disability and of the use of attack therapy |
| Kilic (2019) [36] | Prospective | 42 (14 y) | Migraine | 2000 UI for 2 months, 600–1000 IU for next 6 months | 8 months | Migraine frequency, duration, severity of attacks and PedMIDAS were significantly improved in treated patients compared with control |
| Cayir (2014) [84] | Prospective | 53 (8–16 y) | Migraine | Group1: amitriptylineGroup2: 400 IU + amitriptylineGroup3: 800 IU + amitriptyline Group4: 5000 IU + amitriptyline | 6 months | Group 2-3-4 reported a decrese in headache frequency |
| Potrykus (2013) [85] | Prospective | 37 | Migraine and TTH | 500–1000–2000–5000 IU based on the initial level of the vitamin D | 6 months | Reduction in headache strenght at 3 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dell’Isola, G.B.; Tulli, E.; Sica, R.; Vinti, V.; Mencaroni, E.; Di Cara, G.; Striano, P.; Verrotti, A. The Vitamin D Role in Preventing Primary Headache in Adult and Pediatric Population. J. Clin. Med. 2021, 10, 5983. https://doi.org/10.3390/jcm10245983
Dell’Isola GB, Tulli E, Sica R, Vinti V, Mencaroni E, Di Cara G, Striano P, Verrotti A. The Vitamin D Role in Preventing Primary Headache in Adult and Pediatric Population. Journal of Clinical Medicine. 2021; 10(24):5983. https://doi.org/10.3390/jcm10245983
Chicago/Turabian StyleDell’Isola, Giovanni Battista, Eleonora Tulli, Rossella Sica, Valerio Vinti, Elisabetta Mencaroni, Giuseppe Di Cara, Pasquale Striano, and Alberto Verrotti. 2021. "The Vitamin D Role in Preventing Primary Headache in Adult and Pediatric Population" Journal of Clinical Medicine 10, no. 24: 5983. https://doi.org/10.3390/jcm10245983
APA StyleDell’Isola, G. B., Tulli, E., Sica, R., Vinti, V., Mencaroni, E., Di Cara, G., Striano, P., & Verrotti, A. (2021). The Vitamin D Role in Preventing Primary Headache in Adult and Pediatric Population. Journal of Clinical Medicine, 10(24), 5983. https://doi.org/10.3390/jcm10245983