
The Definition, Assessment, and Prevalence of (Human Assumed) Central Sensitisation in Patients with Chronic Low Back Pain: A Systematic Review

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Eligibility Criteria
2.3. Study Screening
2.4. Risk of Bias Appraisal
2.5. Data Extraction
2.5.1. Study Descriptives
2.5.2. Definitions of Human Assumed Central Sensitisation
2.5.3. Assessment of Human Assumed Central Sensitisation
2.5.4. Clinimetrics of Human Assumed Central Sensitisation Assessment Methods
2.5.5. Prevalence of Human Assumed Central Sensitisation
2.6. Data Synthesis
3. Results
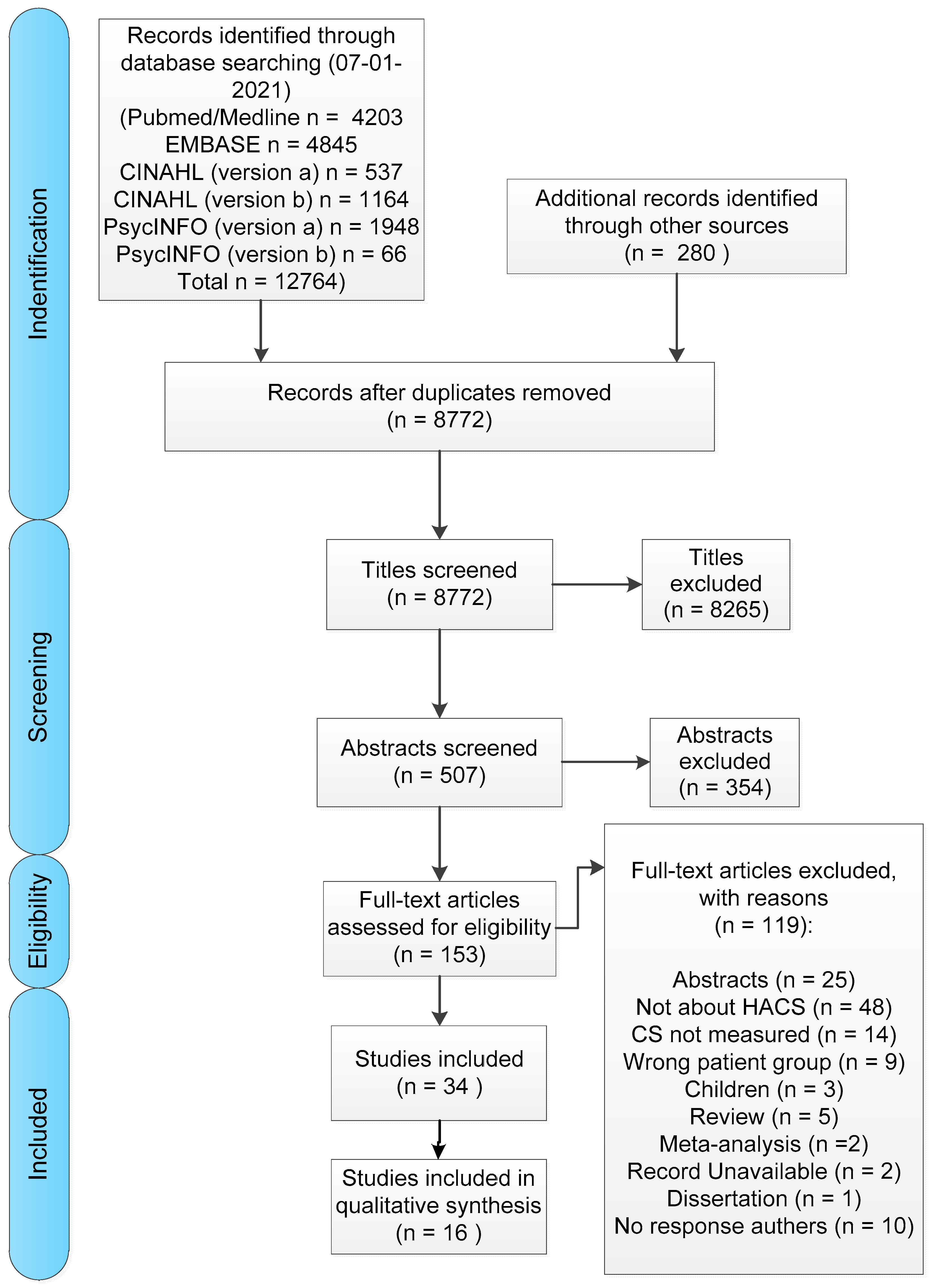
3.1. Study Characteristics
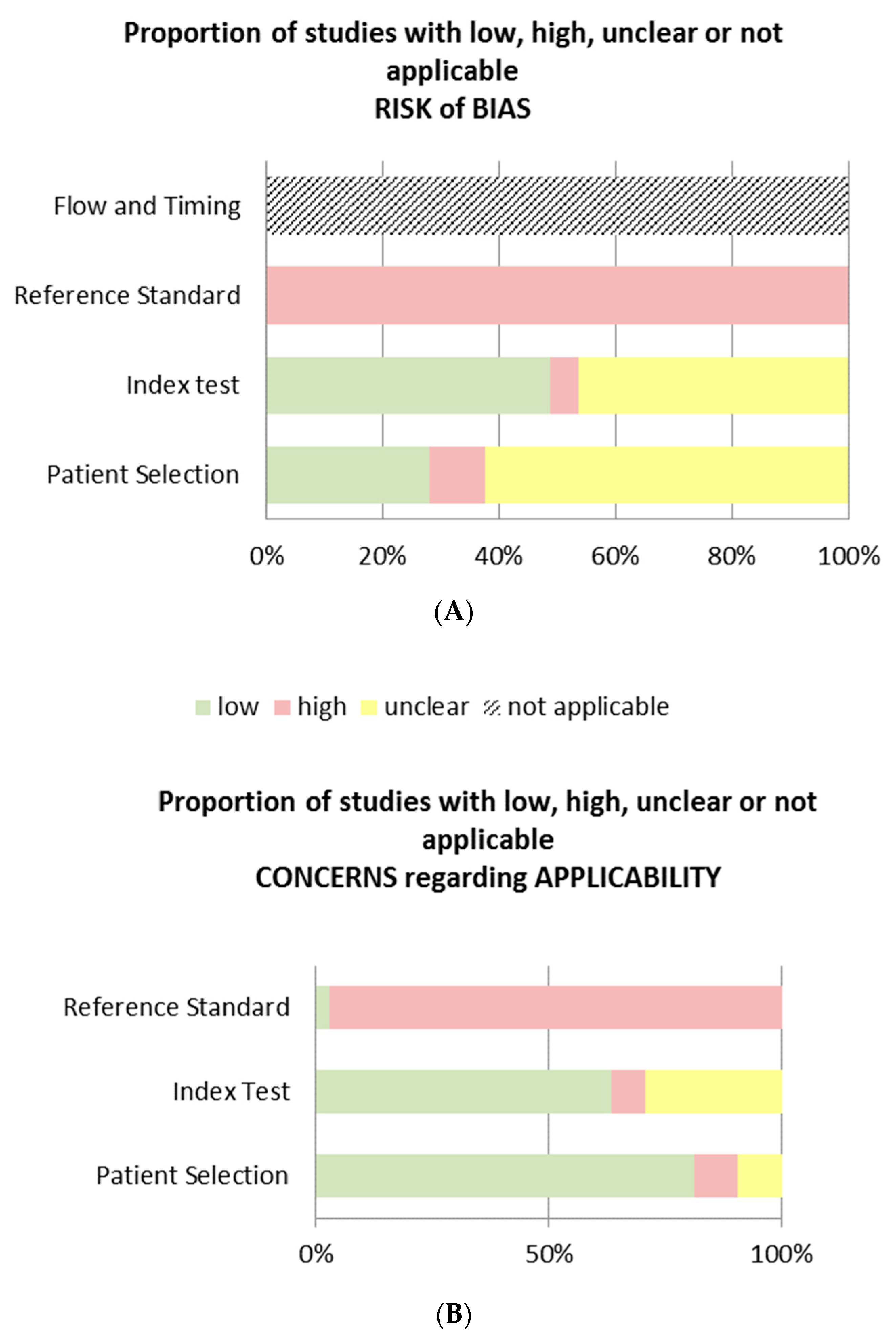
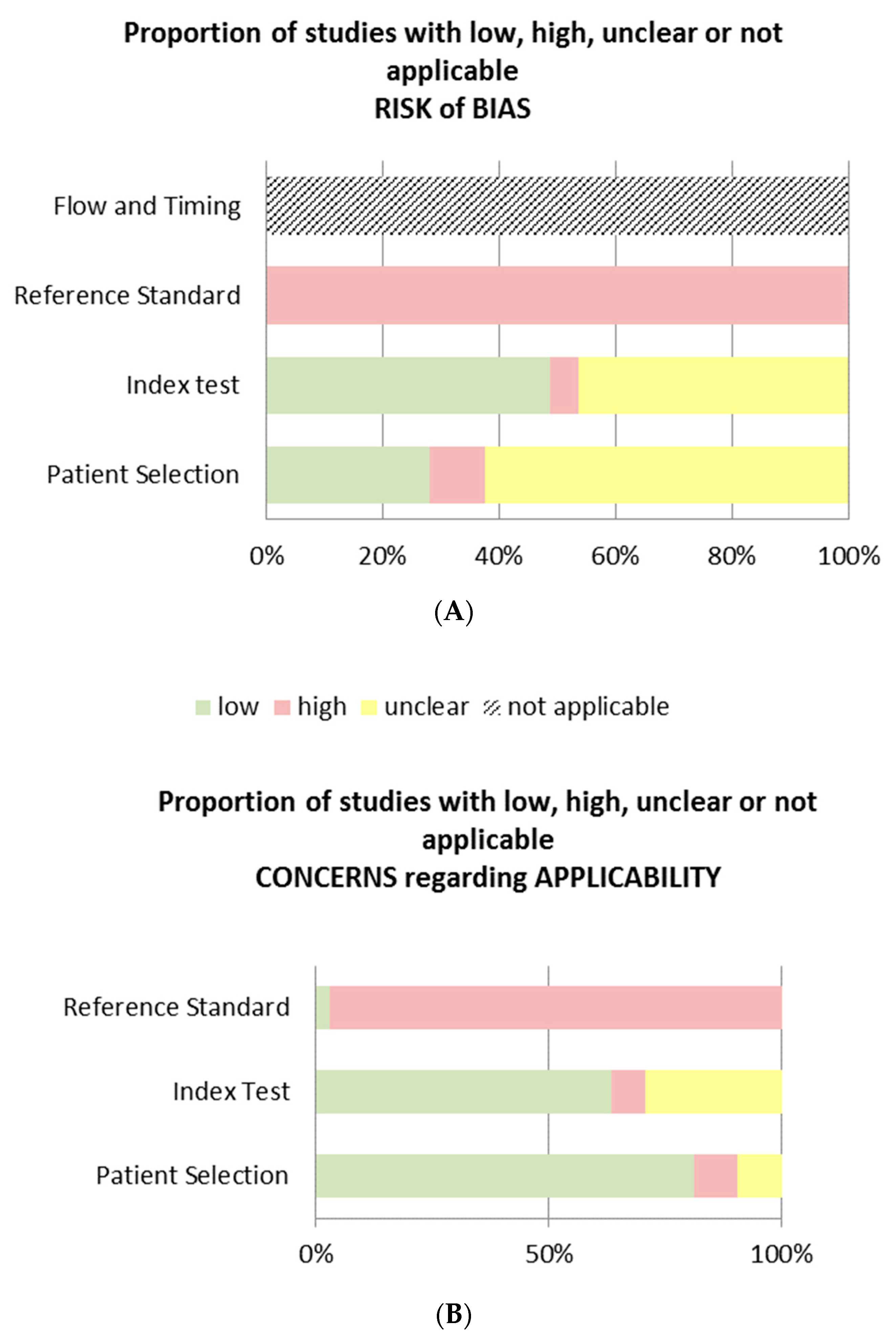
3.2. Risk of Bias
3.3. Definition of Human Assumed Central Sensitisation
3.4. Assessment of Human Assumed Central Sensitisation
3.4.1. Questionnaires
3.4.2. QST Measures
3.5. Clinimetrics of Human Assumed Central Sensitisation Methods
3.6. Estimation of the Prevalence of Human Assumed Central Sensitisation
4. Discussion
4.1. Definition of Human Assumed Central Sensitisation
4.2. Methods for Assessing Human Assumed Central Sensitisation
4.3. Clinimetrics of Human Assumed Central Sensitisation Assessment Methods
4.4. The Estimated Prevalence of Human Assumed Central Sensitisation
4.5. Limitations
4.6. Gold Standard
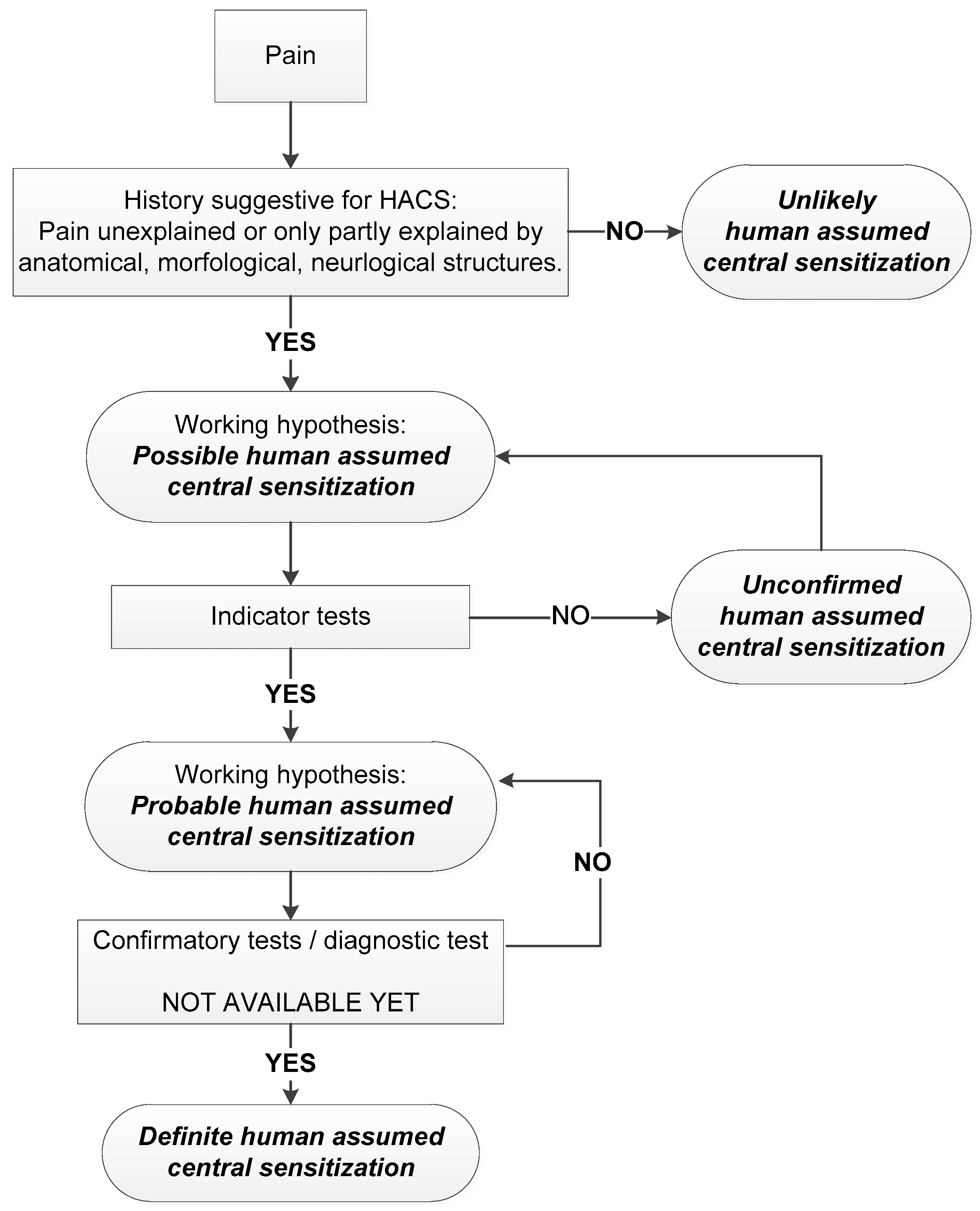
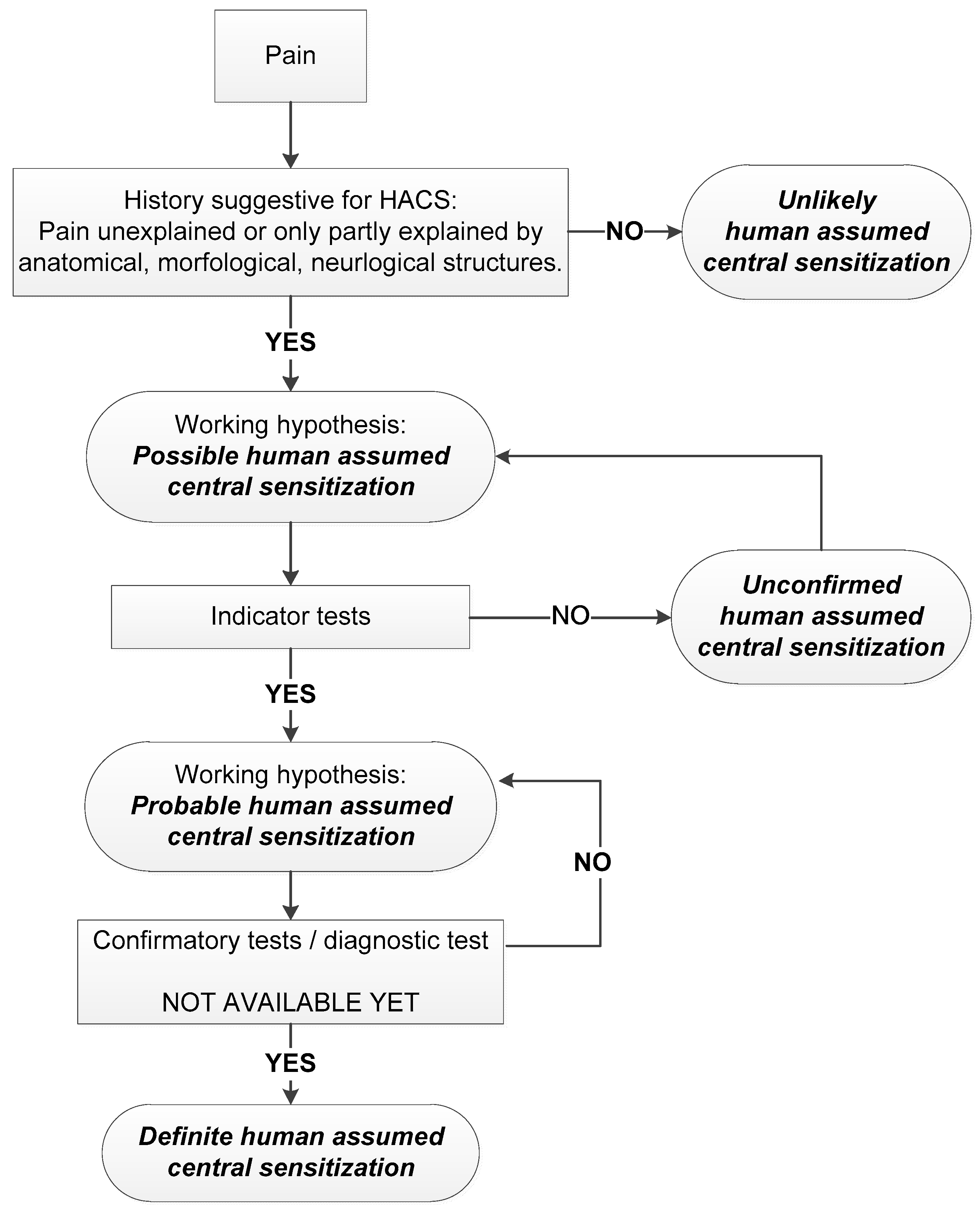
4.7. A Grading System for Human Assumed Central Sensitisation
4.8. Limitations Initial Grading System
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica 2015, 49, 73. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Bütikofer, L.; Andersen, O.K.; Heini, P.; Arendt-Nielsen, L.; Jüni, P.; Curatolo, M. Cold pain hypersensitivity predicts trajectories of pain and disability after low back surgery: A prospective cohort study. Pain 2021, 162, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Schliessbach, J.; Siegenthaler, A.; Bütikofer, L.; Vuilleumier, P.; Jüni, P.; Stamer, U.; Arendt-Nielsen, L.; Curatolo, M. Predicting drug efficacy in chronic low back pain by quantitative sensory tests. Eur. J. Pain 2018, 22, 973–988. [Google Scholar] [CrossRef]
- Loeser, J.D.; Treede, R.-D. The Kyoto protocol of IASP Basic Pain Terminology. Pain 2008, 137, 473–477. [Google Scholar] [CrossRef]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.-A.; Rice, A.S.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef]
- Petersen, K.K.; Olesen, A.E.; Simonsen, O.; Arendt-Nielsen, L. Mechanistic pain profiling as a tool to predict the efficacy of 3-week nonsteroidal anti-inflammatory drugs plus paracetamol in patients with painful knee osteoarthritis. Pain 2019, 160, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Petersen, K.K.; Vaegter, H.B.; Stubhaug, A.; Wolff, A.; Scammell, B.E.; Arendt-Nielsen, L.; Larsen, D.B. The predictive value of quantitative sensory testing: A systematic review on chronic postoperative pain and the analgesic effect of pharmacological therapies in patients with chronic pain. Pain 2021, 162, 31–44. [Google Scholar] [CrossRef]
- Brummett, C.; Clauw, D.; Harris, R.; Harte, S.; Hassett, A.; Williams, D. We agree with the need for a new term but disagree with the proposed terms. Pain 2016, 157, 2876. [Google Scholar] [CrossRef]
- Trouvin, A.-P.; Perrot, S. New concepts of pain. Best Pract. Res. Clin. Rheumatol. 2019, 33, 101415. [Google Scholar] [CrossRef]
- Roussel, N.A.; Nijs, J.; Meeus, M.; Mylius, V.; Fayt, C.; Oostendorp, R. Central Sensitization and Altered Central Pain Processing in Chronic Low Back Pain: Fact or Myth? Clin. J. Pain 2013, 29, 625–638. [Google Scholar] [CrossRef] [Green Version]
- Rifbjerg-Madsen, S.; Christensen, A.W.; Boesen, M.; Christensen, R.; Danneskiold-Samsøe, B.; Bliddal, H.; Dreyer, L.; Locht, H.; Amris, K. The course of pain hypersensitivity according to painDETECT in patients with rheumatoid arthritis initiating treatment: Results from the prospective FRAME-cohort study. Arthritis Res. Ther. 2018, 20, 105. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Rey, R.; Argoff, C. When to consider ‘mixed pain’? The right questions can make a difference! Curr. Med. Res. Opin. 2020, 36, 2037–2046. [Google Scholar] [CrossRef]
- Woolf, C.J. Evidence for a central component of post-injury pain hypersensitivity. Nature 1983, 306, 686–688. [Google Scholar] [CrossRef]
- Woolf, C.J. Pain: Moving from symptom control toward mechanism-specific pharmacologic management. Ann. Intern. Med. 2004, 140, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Harte, S.E.; Harris, R.E.; Clauw, D.J. The neurobiology of central sensitization. J. Appl. Biobehav. Res. 2018, 23, e12137. [Google Scholar] [CrossRef] [Green Version]
- Bailly, F.; Cantagrel, A.; Bertin, P.; Perrot, S.; Thomas, T.; Lansaman, T.; Grange, L.; Wendling, D.; Dovico, C.; Trouvin, A.-P. Part of pain labelled neuropathic in rheumatic disease might be rather nociplastic. RMD Open 2020, 6, e001326. [Google Scholar] [CrossRef]
- Brooks, J.; Tracey, I. The insula: A multidimensional integration site for pain. Pain 2007, 128, 1–2. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y.; Lindquist, M.A.; Roy, M.; Woo, C.-W.; Kross, E. An fMRI-based neurologic signature of physical pain. N. Engl. J. Med. 2013, 368, 1388–1397. [Google Scholar] [CrossRef] [Green Version]
- Boer, C.D.; Dries, L.; Terluin, B.; van der Wouden, J.C.; Blankenstein, A.H.; van Wilgen, C.P.; Lucassen, P.; van der Horst, H.E. Central sensitization in chronic pain and medically unexplained symptom research: A systematic review of definitions, operationalizations and measurement instruments. J. Psychosom. Res. 2019, 117, 32–40. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Morlion, B.; Perrot, S.; Dahan, A.; Dickenson, A.; Kress, H.; Wells, C.; Bouhassira, D.; Mohr Drewes, A. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur. J. Pain 2018, 22, 216–241. [Google Scholar] [CrossRef] [Green Version]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolke, R.; Baron, R.; Maier, C.a.; Tölle, T.; Treede, R.-D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef]
- Caumo, W.; Antunes, L.C.; Elkfury, J.L.; Herbstrith, E.G.; Busanello Sipmann, R.; Souza, A.; Torres, I.L.; Souza Dos Santos, V.; Neblett, R. The Central Sensitization Inventory validated and adapted for a Brazilian population: Psychometric properties and its relationship with brain-derived neurotrophic factor. J. Pain Res. 2017, 10, 2109–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deitos, A.; Dussan-Sarria, J.A.; Souza, A.; Medeiros, L.; Tarrago Mda, G.; Sehn, F.; Chassot, M.; Zanette, S.; Schwertner, A.; Fregni, F.; et al. Clinical Value of Serum Neuroplasticity Mediators in Identifying the Central Sensitivity Syndrome in Patients With Chronic Pain With and Without Structural Pathology. Clin. J. Pain 2015, 31, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Haroutounian, S.; Kamerman, P.; Baron, R.; Bennett, D.L.; Bouhassira, D.; Cruccu, G.; Freeman, R.; Hansson, P.; Nurmikko, T. Neuropathic pain: An updated grading system for research and clinical practice. Pain 2016, 157, 1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treede, R.-D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.; Griffin, J.; Hansson, P.; Hughes, R.; Nurmikko, T.; Serra, J. Neuropathic pain: Redefinition and a grading system for clinical and research purposes. Neurology 2008, 70, 1630–1635. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Jansma, E.P.; Riphagen, I.I.; de Vet, H.C. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual. Life Res. 2009, 18, 1115–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedi, A.; Prinsen, C.; Shah, I.; Buser, Z.; Wang, J.C. Performance properties of health-related measurement instruments in whiplash: Systematic review protocol. Syst. Rev. 2019, 8, 199. [Google Scholar] [CrossRef] [PubMed]
- Chiarotto, A.; Terwee, C.B.; Kamper, S.J.; Boers, M.; Ostelo, R.W. Evidence on the measurement properties of health-related quality of life instruments is largely missing in patients with low back pain: A systematic review. J. Clin. Epidemiol. 2018, 102, 23–37. [Google Scholar] [CrossRef]
- Bramer, W.; Bain, P. Updating search strategies for systematic reviews using EndNote. J. Med. Libr. Assoc. JMLA 2017, 105, 285. [Google Scholar] [CrossRef]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. JMLA 2016, 104, 240. [Google Scholar] [CrossRef] [PubMed]
- Quadas-2. Available online: http://www.quadas.org (accessed on 28 September 2020).
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Kincaid, J.C.; Price, K.L.; Jimenez, M.C.; Skljarevski, V. Correlation of vibratory quantitative sensory testing and nerve conduction studies in patients with diabetes. Muscle Nerve Off. J. Am. Assoc. Electrodiagn. Med. 2007, 36, 821–827. [Google Scholar] [CrossRef]
- Miller, L.E. Correlations: Description or inference. J. Agric. Educ. 1994, 35, 5–7. [Google Scholar] [CrossRef] [Green Version]
- Ansuategui Echeita, J.; Dijkhof, M.; Grootenboer, F.; van der Wurff, P.; Killen, V.; Reneman, M.F. A pilot study in the association between Waddell Non-organic Signs and Central Sensitization. Musculoskelet. Sci. Pract. 2020, 49, 102200. [Google Scholar] [CrossRef]
- Ansuategui Echeita, J.; van der Wurff, P.; Killen, V.; Dijkhof, M.F.; Grootenboer, F.M.; Reneman, M.F. Lifting capacity is associated with central sensitization and non-organic signs in patients with chronic back pain. Disabil. Rehabil. 2020, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoyagi, K.; He, J.; Nicol, A.L.; Clauw, D.J.; Kluding, P.M.; Jernigan, S.; Sharma, N.K. A Subgroup of Chronic Low Back Pain Patients with Central Sensitization. Clin. J. Pain 2019, 35, 869–879. [Google Scholar] [CrossRef] [PubMed]
- Aoyagi, K.; Sharma, N.K. Correlation between Central Sensitization and Remote Muscle Performance in Individuals with Chronic Low Back Pain. J. Manip. Physiol. Ther. 2021, 44, 14–24. [Google Scholar] [CrossRef]
- Ashina, S.; Lipton, R.B.; Bendtsen, L.; Hajiyeva, N.; Buse, D.C.; Lyngberg, A.C.; Jensen, R. Increased pain sensitivity in migraine and tension-type headache coexistent with low back pain: A cross-sectional population study. Eur. J Pain 2018, 22, 904–914. [Google Scholar] [CrossRef]
- Bid, D.D.; Soni, C.N.; Yadav, S.A.; Rathod, V.P. A Study on Central Sensitization in Chronic Non-specific Low Back Pain. Indian J. Physiother. Occup. Ther. Int. J. 2017, 11, 165–175. [Google Scholar] [CrossRef]
- Bilika, P.; Neblett, R.; Georgoudis, G.; Dimitriadis, Z.; Fandridis, E.; Strimpakos, N.; Kapreli, E. Cross-cultural Adaptation and Psychometric Properties of the Greek Version of the Central Sensitization Inventory. Pain Pract. 2020, 20, 188–196. [Google Scholar] [CrossRef]
- Chiarotto, A.; Viti, C.; Sulli, A.; Cutolo, M.; Testa, M.; Piscitelli, D. Cross-cultural adaptation and validity of the Italian version of the Central Sensitization Inventory. Musculoskelet. Sci. Pract. 2018, 37, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.R.; Yeowell, G.; Goodwin, P.C. Trait anxiety and sensory processing profile characteristics in patients with non-specific chronic low back pain and central sensitisation—A pilot observational study. J. Bodyw. Mov. 2018, 22, 909–916. [Google Scholar] [CrossRef]
- Clark, J.R.; Nijs, J.; Yeowell, G.; Holmes, P.; Goodwin, P.C. Trait Sensitivity, Anxiety, and Personality Are Predictive of Central Sensitization Symptoms in Patients with Chronic Low Back Pain. Pain Pract. 2019, 19, 800–810. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Roldan-Jimenez, C.; Neblett, R.; Gatchel, R.J. Cross-cultural adaptation and validity of the Spanish central sensitization inventory. Springerplus 2016, 5, 1837. [Google Scholar] [CrossRef] [Green Version]
- Defrin, R.; Devor, M.; Brill, S. Tactile allodynia in patients with lumbar radicular pain (sciatica). Pain 2014, 155, 2551–2559. [Google Scholar] [CrossRef]
- Dixon, E.A.; Benham, G.; Sturgeon, J.A.; Mackey, S.; Johnson, K.A.; Younger, J. Development of the Sensory Hypersensitivity Scale (SHS): A self-report tool for assessing sensitivity to sensory stimuli. J. Behav. Med. 2016, 39, 537–550. [Google Scholar] [CrossRef] [Green Version]
- Hubscher, M.; Moloney, N.; Rebbeck, T.; Traeger, A.; Refshauge, K.M. Contributions of mood, pain catastrophizing, and cold hyperalgesia in acute and chronic low back pain: A comparison with pain-free controls. Clin. J. Pain 2014, 30, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Huysmans, E.; Ickmans, K.; Van Dyck, D.; Nijs, J.; Gidron, Y.; Roussel, N.; Polli, A.; Moens, M.; Goudman, L.; De Kooning, M. Association Between Symptoms of Central Sensitization and Cognitive Behavioral Factors in People With Chronic Nonspecific Low Back Pain: A Cross-sectional Study. J Manip. Physiol. 2018, 41, 92–101. [Google Scholar] [CrossRef]
- Ide, K.; Yasuda, T.; Hasegawa, T.; Yamato, Y.; Yoshida, G.; Banno, T.; Arima, H.; Oe, S.; Mihara, Y.; Ushirozako, H. Evaluation of the Central Sensitization Inventory Score in elderly adults with musculoskeletal examination. Mod. Rheumatol. 2020, 31, 885–889. [Google Scholar] [CrossRef]
- Knezevic, A.; Neblett, R.; Jeremic-Knezevic, M.; Tomasevic-Todorovic, S.; Boskovic, K.; Colovic, P.; Cuesta-Vargas, A. Cross-Cultural Adaptation and Psychometric Validation of the Serbian Version of the Central Sensitization Inventory. Pain Pract. 2018, 18, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, A.; Neblett, R.; Colovic, P.; Jeremic-Knezevic, M.; Bugarski-Ignjatovic, V.; Klasnja, A.; Pantelinac, S.; Pjevic, M. Convergent and Discriminant Validity of the Serbian Version of the Central Sensitization Inventory. Pain Pract. 2020, 20, 724–736. [Google Scholar] [CrossRef] [PubMed]
- Kregel, J.; Vuijk, P.J.; Descheemaeker, F.; Keizer, D.; van der Noord, R.; Nijs, J.; Cagnie, B.; Meeus, M.; van Wilgen, P. The Dutch Central Sensitization Inventory (CSI): Factor Analysis, Discriminative Power, and Test-Retest Reliability. Clin. J. Pain 2016, 32, 624–630. [Google Scholar] [CrossRef]
- Kregel, J.; Schumacher, C.; Dolphens, M.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M.; Coppieters, I. Convergent Validity of the Dutch Central Sensitization Inventory: Associations with Psychophysical Pain Measures, Quality of Life, Disability, and Pain Cognitions in Patients with Chronic Spinal Pain. Pain Pract. 2018, 18, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Leemans, L.; Elma, O.; Nijs, J.; Wideman, T.H.; Siffain, C.; den Bandt, H.; Van Laere, S.; Beckwee, D. Transcutaneous electrical nerve stimulation and heat to reduce pain in a chronic low back pain population: A randomized controlled clinical trial. Braz. J. Phys. 2021, 25, 86–96. [Google Scholar] [CrossRef]
- McKernan, L.C.; Johnson, B.N.; Crofford, L.J.; Lumley, M.A.; Bruehl, S.; Cheavens, J.S. Posttraumatic Stress Symptoms Mediate the Effects of Trauma Exposure on Clinical Indicators of Central Sensitization in Patients With Chronic Pain. Clin. J. Pain 2019, 35, 385–393. [Google Scholar] [CrossRef]
- Mehta, V.; Snidvongs, S.; Ghai, B.; Langford, R.; Wodehouse, T. Characterization of peripheral and central sensitization after dorsal root ganglion intervention in patients with unilateral lumbosacral radicular pain: A prospective pilot study. Br. J. Anaesth. 2017, 118, 924–931. [Google Scholar] [CrossRef] [Green Version]
- Mibu, A.; Nishigami, T.; Tanaka, K.; Manfuku, M.; Yono, S. Difference in the impact of central sensitization on pain-related symptoms between patients with chronic low back pain and knee osteoarthritis. J. Pain Res. 2019, 12, 1757–1765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miki, T.; Nishigami, T.; Takebayashi, T.; Yamauchi, T. Association between central sensitivity syndrome and psychological factors in people with presurgical low back pain: A cross-sectional study. J. Orthop. Sci. 2021, 26, 337–342. [Google Scholar] [CrossRef]
- Muller, M.; Limacher, A.; Agten, C.A.; Treichel, F.; Heini, P.; Seidel, U.; Andersen, O.K.; Arendt-Nielsen, L.; Juni, P.; Curatolo, M. Can quantitative sensory tests predict failed back surgery? A prospective cohort study. Eur. J. Anaesthesiol. 2019, 36, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.; Hartzell, M.M.; Williams, M.; Bevers, K.R.; Mayer, T.G.; Gatchel, R.J. Use of the Central Sensitization Inventory (CSI) as a treatment outcome measure for patients with chronic spinal pain disorder in a functional restoration program. Spine J. 2017, 17, 1819–1829. [Google Scholar] [CrossRef]
- Noord, R.; van der Paap, D.; van Wilgen, C.P. Convergent validity and clinically relevant categories for the Dutch Central Sensitization Inventory in patients with chronic pain. J. Appl. Biobehav. Res. 2018, 23, e12119. [Google Scholar] [CrossRef]
- Serrano-Ibáñez, E.R.; Esteve, R.; Ramírez-Maestre, C.; Ruiz-Párraga, G.T.; López-Martínez, A.E. Chronic pain in the time of COVID-19: Stress aftermath and central sensitization. Br. J. Health Psychol. 2021, 26, 544–552. [Google Scholar] [CrossRef]
- Sharma, S.; Jha, J.; Pathak, A.; Neblett, R. Translation, cross-cultural adaptation, and measurement properties of the Nepali version of the central sensitization inventory (CSI). BMC Neurol. 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Smart, K.M.; Blake, C.; Staines, A.; Doody, C. Self-reported pain severity, quality of life, disability, anxiety and depression in patients classified with ‘nociceptive’, ‘peripheral neuropathic’ and ‘central sensitisation’ pain. The discriminant validity of mechanisms-based classifications of low back (+/−leg) pain. Man. Ther. 2012, 17, 119–125. [Google Scholar] [CrossRef]
- Tesarz, J.; Gerhardt, A.; Leisner, S.; Janke, S.; Treede, R.D.; Eich, W. Distinct quantitative sensory testing profiles in nonspecific chronic back pain subjects with and without psychological trauma. Pain 2015, 156, 577–586. [Google Scholar] [CrossRef]
- Tesarz, J.; Eich, W.; Treede, R.D.; Gerhardt, A. Altered pressure pain thresholds and increased wind-up in adult patients with chronic back pain with a history of childhood maltreatment: A quantitative sensory testing study. Pain 2016, 157, 1799–1809. [Google Scholar] [CrossRef]
- Katz, J.N.; Stock, S.R.; Evanoff, B.A.; Rempel, D.; Moore, J.S.; Franzblau, A.; Gray, R.H. Classification criteria and severity assessment in work-associated upper extremity disorders: Methods matter. Am. J. Ind. Med. 2000, 38, 369–372. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use, 3rd ed.; Oxford University Press: Oxford, MS, USA, 2003. [Google Scholar]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Man. Ther. 2010, 15, 135–141. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitizationuncovering the relation between pain and plasticity. Anesthesiol. J. Am. Soc. Anesthesiol. 2007, 106, 864–867. [Google Scholar]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clauw, D.J. Diagnosing and treating chronic musculoskeletal pain based on the underlying mechanism (s). Best Pract. Res. Clin. Rheumatol. 2015, 29, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Torres-Cueco, R.; van Wilgen, P.; Lluch Girbés, E.; Struyf, F.; Roussel, N.; Van Oosterwijck, J.; Daenen, L.; Kuppens, K.; Vanderweeen, L. Applying modern pain neuroscience in clinical practice: Criteria for the classification of central sensitization pain. Pain Physician 2014, 17, 447–457. [Google Scholar] [CrossRef]
- Nijs, J.; Apeldoorn, A.; Hallegraeff, H.; Clark, J.; Smeets, R.; Malfliet, A.; Girbes, E.L.; De Kooning, M.; Ickmans, K. Low back pain: Guidelines for the clinical classification of predominant neuropathic, nociceptive, or central sensitization pain. Pain Physician 2015, 18, E333–E345. [Google Scholar] [CrossRef]
- Yoon, M.-S.; Manack, A.; Schramm, S.; Fritsche, G.; Obermann, M.; Diener, H.-C.; Moebus, S.; Katsarava, Z. Chronic migraine and chronic tension-type headache are associated with concomitant low back pain: Results of the German Headache Consortium study. Pain 2013, 154, 484–492. [Google Scholar] [CrossRef]
- Meyer, R.A.; Campbell, J.N.; Raja, S.N. Peripheral Neural Mechanisms of Nociception; Churchill Livingstone: Edinburgh, UK, 1995; Volume 3. [Google Scholar]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Kindler, L.L.; Bennett, R.M.; Jones, K.D. Central sensitivity syndromes: Mounting pathophysiologic evidence to link fibromyalgia with other common chronic pain disorders. Pain Manag. Nurs. 2011, 12, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinricher, M.; Tavares, I.; Leith, J.; Lumb, B. Descending control of nociception: Specificity, recruitment and plasticity. Brain Res. Rev. 2009, 60, 214–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, S.N.; Campbell, J.N.; Meyer, R.A. Evidence for different mechanisms of primary and secondary hyperalgesia following heat injury to the glabrous skin. Brain 1984, 107, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Torebjörk, H.; Lundberg, L.; LaMotte, R. Central changes in processing of mechanoreceptive input in capsaicin-induced secondary hyperalgesia in humans. J. Physiol. 1992, 448, 765–780. [Google Scholar] [CrossRef]
- Kaya, S.; Hermans, L.; Willems, T.; Roussel, N.; Meeus, M. Central sensitization in urogynecological chronic pelvic pain: A systematic literature review. Pain Physician 2013, 16, 291–308. [Google Scholar] [CrossRef]
- Lluch, E.; Torres, R.; Nijs, J.; Van Oosterwijck, J. Evidence for central sensitization in patients with osteoarthritis pain: A systematic literature review. Eur. J. Pain 2014, 18, 1367–1375. [Google Scholar] [CrossRef]
- Wang, D.; Couture, R.; Hong, Y. Activated microglia in the spinal cord underlies diabetic neuropathic pain. Eur. J. Pharmacol. 2014, 728, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Batheja, S.; Nields, J.A.; Landa, A.; Fallon, B.A. Post-treatment lyme syndrome and central sensitization. J. Neuropsychiatry Clin. Neurosci. 2013, 25, 176–186. [Google Scholar] [CrossRef] [Green Version]
- Ji, R.-R.; Kohno, T.; Moore, K.A.; Woolf, C.J. Central sensitization and LTP: Do pain and memory share similar mechanisms? Trends Neurosci. 2003, 26, 696–705. [Google Scholar] [CrossRef]
- Salter, M.W. Cellular neuroplasticity mechanisms mediating pain persistence. J. Orofac. Pain 2004, 18, 4. [Google Scholar]
- Yunus, M.B. Fibromyalgia and overlapping disorders: The unifying concept of central sensitivity syndromes. Semin. Arthritis Rheum. 2007, 36, 339–356. [Google Scholar] [CrossRef]
- Nijs, J.; Meeus, M.; Van Oosterwijck, J.; Roussel, N.; De Kooning, M.; Ickmans, K.; Matic, M. Treatment of central sensitization in patients with ‘unexplained’chronic pain: What options do we have? Expert Opin. Pharmacother. 2011, 12, 1087–1098. [Google Scholar] [CrossRef]
- Staud, R.; Craggs, J.G.; Robinson, M.E.; Perlstein, W.M.; Price, D.D. Brain activity related to temporal summation of C-fiber evoked pain. Pain 2007, 129, 130–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeus, M.; Nijs, J.; Van de Wauwer, N.; Toeback, L.; Truijen, S. Diffuse noxious inhibitory control is delayed in chronic fatigue syndrome: An experimental study. Pain 2008, 139, 439–448. [Google Scholar] [CrossRef]
- Meeus, M.; Nijs, J. Central sensitization: A biopsychosocial explanation for chronic widespread pain in patients with fibromyalgia and chronic fatigue syndrome. Clin. Rheumatol. 2007, 26, 465–473. [Google Scholar] [CrossRef] [Green Version]
- International Association for the Study of Pain. IASP Taxonomy. Available online: http://www.iasp-pain.org/Taxonomy (accessed on 2 December 2020).
- Schliessbach, J.; Siegenthaler, A.; Streitberger, K.; Eichenberger, U.; Nüesch, E.; Jüni, P.; Arendt-Nielsen, L.; Curatolo, M. The prevalence of widespread central hypersensitivity in chronic pain patients. Eur. J. Pain 2013, 17, 1502–1510. [Google Scholar] [CrossRef]
- Baranauskas, G.; Nistri, A. Sensitization of pain pathways in the spinal cord: Cellular mechanisms. Prog. Neurobiol. 1998, 54, 349–365. [Google Scholar] [CrossRef]
- Maixner, W.; Fillingim, R.; Sigurdsson, A.; Kincaid, S.; Silva, S. Sensitivity of patients with painful temporomandibular disorders to experimentally evoked pain: Evidence for altered temporal summation of pain. Pain 1998, 76, 71–81. [Google Scholar] [CrossRef]
- Wilgen, C.P.v.; Konopka, K.; Keizer, D.; Zwerver, J.; Dekker, R. Do patients with chronic patellar tendinopathy have an altered somatosensory profile?–A Quantitative Sensory Testing (QST) study. Scand. J. Med. Sci. Sports 2013, 23, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.M.; Turk, D.C. Psychosocial factors and central sensitivity syndromes. Curr. Rheumatol. Rev. 2015, 11, 96–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costigan, M.; Scholz, J.; Woolf, C.J. Neuropathic pain: A maladaptive response of the nervous system to damage. Annu. Rev. Neurosci. 2009, 32, 1–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brummett, C.M.; Bakshi, R.R.; Goesling, J.; Leung, D.; Moser, S.E.; Zollars, J.W.; Williams, D.A.; Clauw, D.J.; Hassett, A.L. Preliminary validation of the michigan body map (MBM). Pain 2016, 157, 1205. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, R.H.; Turk, D.C.; Revicki, D.A.; Harding, G.; Coyne, K.S.; Peirce-Sandner, S.; Bhagwat, D.; Everton, D.; Burke, L.B.; Cowan, P. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain 2009, 144, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Trudeau, J.J.; Benson, C.; Biondi, D.M.; Katz, N.P.; Kim, M. Validation of the Short-form McGill Pain Questionnaire-2 (SF-MPQ-2) in acute low back pain. J. Pain 2015, 16, 357–366. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: A modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, D.L.; Kemp, H.I.; Ridout, D.; Yarnitsky, D.; Rice, A.S. Reliability of conditioned pain modulation: A systematic review. Pain 2016, 157, 2410. [Google Scholar] [CrossRef]
- Lewis, G.N.; Rice, D.A.; McNair, P.J. Conditioned pain modulation in populations with chronic pain: A systematic review and meta-analysis. J. Pain 2012, 13, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Lahousse, A.; Kapreli, E.; Bilika, P.; Saraçoğlu, İ.; Malfliet, A.; Coppieters, I.; De Baets, L.; Leysen, L.; Roose, E. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. J. Clin. Med. 2021, 10, 3203. [Google Scholar] [CrossRef]
- Neblett, R. The central sensitization inventory: A user’s manual. J. Appl. Biobehav. Res. 2018, 23, e12123. [Google Scholar] [CrossRef]
- Scerbo, T.; Colasurdo, J.; Dunn, S.; Unger, J.; Nijs, J.; Cook, C. Measurement properties of the central sensitization inventory: A systematic review. Pain Pract. 2018, 18, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Coronado, R.A.; George, S.Z. The Central Sensitization Inventory and Pain Sensitivity Questionnaire: An exploration of construct validity and associations with widespread pain sensitivity among individuals with shoulder pain. Musculoskelet. Sci. Pract. 2018, 36, 61–67. [Google Scholar] [CrossRef] [PubMed]
- McPhee, M.E.; Graven-Nielsen, T. Recurrent low back pain patients demonstrate facilitated pronociceptive mechanisms when in pain, and impaired antinociceptive mechanisms with and without pain. Pain 2019, 160, 2866–2876. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: http://www3.med.unipmn.it/dispense_ebm/2009-2010/Corso%20Perfezionamento%20EBM_Faggiano/NOS_oxford.pdf (accessed on 19 July 2021).
- Koneru, S.N.; Staelin, R.; Rawe, I.M. Chronic pain intervention using pulsed shortwave therapy: The relationship between pain demographics and central sensitization inventory. Pain Manag. 2019, 9, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Middlebrook, N.; Rushton, A.B.; Heneghan, N.R.; Falla, D. Measures of central sensitisation and their measurement properties in the adult musculoskeletal trauma population: A protocol for a systematic review and data synthesis. BMJ Open 2019, 9, e023204. [Google Scholar] [CrossRef] [PubMed]
- Wilgen, C.P.v.; Vuijk, P.J.; Kregel, J.; Voogt, L.; Meeus, M.; Descheemaeker, F.; Keizer, D.; Nijs, J. Psychological distress and widespread pain contribute to the variance of the central sensitization inventory: A cross-sectional study in patients with chronic pain. Pain Pract. 2018, 18, 239–246. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Cummins, T.M.; Kucharczyk, M.M.; Graven-Nielsen, T.; Bannister, K. Activation of the descending pain modulatory system using cuff pressure algometry: Back translation from man to rat. Eur. J. Pain 2020, 24, 1330–1338. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| 1st Author, Year | Country | nr. of Participants | Age (Mean ± SD/Range/95% CI) | Sex (%Female) | BMI (Mean ± SD/95% CI) | |
|---|---|---|---|---|---|---|
| Ansuategui Echeita, 2020a *,# | [41] | The Netherlands | CLBP: 56 | CLBP: 42.55 ± 13.22 | CLBP: 33 (58.9%) | CLBP: 26.30 ± 4.77 |
| Ansuategui Echeita, 2020b *,# | [42] | The Netherlands | CLBP: 56 | CLBP: 42.55 ± 13.22 | CLBP: 33 (58.9%) | CLBP: 26.30 ± 4.77 |
| Aoyagi, 2019 | [43] | United States of America | CLBP only: 24 CLBP+: 22 Healthy controls: 22 | CLBP only: 42.38 ± 12.37 CLBP+: 43.95 ± 14.00 Healthy controls: 41.15 ± 8.83 | CLBP only: 15 (63%) CLBP+: 17 (77%) Healthy controls: 15 (68%) | CLBP only: 28.76 ± 6.20 CLBP+: 31.34 ± 6.13 Healthy controls: 28.35 ± 8.10 |
| Aoyagi, 2020 | [44] | United States of America | CLBP only: 30 CLBP+: 30 | CLBP only: 42.38 ± 12.37 CLBP+: 41.23 ± 13.81 | CLBP only: 19 (63%) CLBP+: 24 (80%) | CLBP only: 29.58 ± 6.43 CLBP+: 31.18 ± 6.67 |
| Ashina, 2018, # | [45] | Denmark | CLBP: 570 | CLBP: 48.31 ± 0.57 | CLBP: 305 (53.5%) | NR |
| Bid, 2017 | [46] | India | CLBP: 128 Experimental Group (n = 64) Control Group (n = 64) | CLBP: Experimental Group: 41.33 ± 7.27 CLBP: Control Group: 41.12 ± 7.76 | CLBP: Experimental Group: 36 (56.25%) CLBP: Control Group: 42 (65.63%) | CLBP: Experimental Group: 24.88 ± 2.97 CLBP: Control Group: 24.72 ± 2.76 |
| Bilika, 2020, # | [47] | Greece | CLBP only: 28 Healthy controls: 50 | CLBP only: 49.04 ± 14.811 Healthy controls: 27.90 ± 8.707 | CLBP only: 17 (60.7%) Healthy controls: 25 (50%) | NR |
| Chiarotto 2018, # | [48] | Italy | CLBP only: 76 | CLBP only: 50.9 ± 13.7 | CLBP only: 56 (73.7%) | CLBP only: 24.68 ± 4.30 |
| Clark, 2018 | [49] | New Zealand and United Kingdom | CLBP: 21 | CLBP: 43 (range 20–64) | CLBP: 16 (76%) | NR |
| Clark, 2019, # | [50] | United Kingdom, Ireland and New Zealand | CLBP: 165 | CLBP: 45 ± 12 | CLBP: 126 (76%) | NR |
| Cuesta-Vargas, 2016, # | [51] | Spain | CLBP only: 126 CLBP+: 90 | CLBP only: 52.50 ± 12.61 (10 missing) CLBP+: 57.50 ± 12.28 (6 missing) | CLBP only: 14 (11.1%) (84 missing) CLBP+: 17 (18.9%) (59 missing) | CLBP only: 25.70 ± 4.23 (8 missing) CLBP+: 26.02 ± 3.89 (3 missing) |
| Defrin, 2014 | [52] | Israel | CLBP only: 15 CLBP+: 74 Healthy controls: 22 | CLBP only: Axial CLBP: 64.5 ± 20.7 CLBP+: CLBP with radiation: 65.8 ± 12.9 Healthy controls: 54.2 ± 18.6 | CLBP only: Axial CLBP: 6 (40%) CLBP+: CLBP with radiation: 39 (53%) Healthy controls: 12 (55%) | NR |
| Dixon, 2016 | [53] | United States of America | CLBP: 59 Healthy controls: 44 | CLBP: 40.56 ± 11.32 Healthy controls: 40.26 ± 11.6 | CLBP: 27(46%) (4 missing) Healthy controls: 24(55%) (2 missing) | NR |
| Hubscher, 2014 | [54] | Australia | CLBP: 30 Healthy controls: 30 | CLBP: 30.6 (range 21.8–35.0) Healthy controls: 28.0 (range 21.8–31.0) | CLBP: 15 (50%) Healthy controls: 17(56.7%) | NR |
| Huysmans, 2018 | [55] | Belgium | CLBP only: 38 | CLBP only: 40.76 ± 13.30 | CLBP only: 24 (63.2%) | CLBP only: 24.98 ± 3.16 |
| Ide, 2020, # | [56] | Japan | CLBP only: 46 CLBP+: 206 | CLBP only: 74.33 ± 7.57 CLBP+: 75.95 ± 7.67 | CLBP only: 24 (52.2%) CLBP+: 140 (68.0%) | CLBP only: 22.96 ± 2.74 CLBP+: 22.62 ± 3.16 |
| Knezevic, 2018, # | [57] | Serbia | CLBP only: 157 CLBP+: 74 | CLBP only: 51.59 ± 13.34 CLBP+: 56.65 ± 9.55 | CLBP only: 89 (56.7%) CLBP+: 57(77%) | NR |
| Knezevic, 2020, # | [58] | Serbia | CLBP only: 155 CLBP+: 88 Healthy controls: 146 | CLBP only: 51.74 ± 13.44 CLBP+: 56.77 ± 9.49 Healthy controls: 39.18 ± 14.95 | CLBP only: 83 (53.5%) CLBP+: 66 (75.0%) Healthy controls: 102 (69.9%) | NR |
| Kregel, 2016, # | [59] | The Netherlands and Belgium | CLBP only: 4 CLBP+: 11 | CLBP only: 51.50 ± 15.97 CLBP+: 40.45 ± 9.20 | CLBP only: 3 (75.0%) CLBP+: 8 (72.7%) | NR |
| Kregel, 2018 | [60] | Belgium | CLBP: 54 | CLBP: 41.24 ± 13.04 | CLBP: 31 (57.4%) | NR |
| Leemans, 2020 | [61] | Belgium | CLBP: 50 Experimental (n = 25) Control (n = 25) | CLBP: Experimental: 43.9 ± 12.2 CLBP: Control: 44.7 ± 12.2 | CLBP: Experimental: 13 (52%) CLBP: Control: 14 (56%) | CLBP: Experimental: 26.5 ± 3.8 CLBP: Control: 27.6 ± 5.1 |
| Mayer, 2012 | [25] | United States of America | CLBP only: 44 Healthy controls: 40 | CLBP only: 42.8 ± 10.0 Healthy controls: 21.33 ± 13.6 | CLBP only: 11 (25%) Healthy controls: 31 (77%) | NR |
| McKernan, 2019, # | [62] | United States of America | CLBP only: 38 | CLBP only: 46.75 ± 13.74 | CLBP only: 24 (63.2%) (2 missng) | NR |
| Mehta, 2017 | [63] | United Kingdom | CLBP+: 23 Healthy controls: 21 | CLBP+: 46 Healthy controls: 60 (range 40–81) | CLBP+: 13 (56.5%) Healthy controls: 17 (81.0%) | NR |
| Mibu, 2019 | [64] | Japan | CLBP: 104 | CLBP: 58.4 ± 14.2 | CLBP: 77 (74.0%) | NR |
| Miki, 2020 | [65] | Japan | CLBP: 238 | CLBP: 63.50 ± 16.0 | CLBP: 102 (42.9%) | CLBP: 24.39 ± 4.33 |
| Müller, 2019 | [66] | Switzerland | CLBP: 141 FBSS (n = 44) No FBSS (n = 97) | CLBP: FBSS: 60.7 ± 14.2 CLBP: No FBSS: 61.3 ± 13.7 | CLBP: FBSS: 21 (48%) CLBP: No FBSS: 60 (62%) | CLBP: FBSS: 29.3 ± 4.6 CLBP: No FBSS: 27.8 ± 4.4 |
| Neblett, 2017, # | [67] | United States of America | CLBP only: 322 CLBP+: 323 | CLBP only: 47.27 ± 10.56 CLBP+: 45.96 ± 11.05 | CLBP only: 97 (30.1%) CLBP+: 121 (37.5%) | NR |
| Noord van der, 2018, # | [68] | The Netherlands | CLBP only: 19 CLBP+: 76 | CLBP only: 47.58 ± 15.95 CLBP+: 45.26 ± 13.73 | CLBP only: 10 (52.6%)CLBP+: 49 (64.5%) | NR |
| Serrano-Ibáñez, 2020, # | [69] | Spain | CLBP: 23 | CLBP: 52.48 ± 10.40 | CLBP: 17 (73.9%) | NR |
| Sharma, 2020, # | [70] | Nepal | CLBP only: 22 CLBP+: 27 | CLBP only: 34.36 ± 9.88 CLBP+: 36.22 ± 13.74 | CLBP only: 13 (59.1%) CLBP+: 16 (59.3%) | NR |
| Smart, 2012, # | [71] | Ireland and United Kingdom | CLBP only: 207 CLBP+: 134 | CLBP only: 44.43 ± 14.41 CLBP+: 46.40 ± 13.07 | CLBP only: 118 (57%) CLBP+: 75 (56%) | NR |
| Tesarz, 2015 | [72] | Germany | CLBP: 149 nsCLBP-TE: (n = 56) nsCLBP-W-TE: (n = 93) Healthy controls: 31 | CLBP: nsCLBP-TE: 55.8 (95% CI: 53.1; 58.6) CLBP: nsCLBP-W-TE: 58.2 (95% CI: 56.3; 60.2) Healthy controls: 60.1 (95% CI: 55.7; 64.5) | CLBP: nsCLBP-TE: 42 (75.0%) CLBP: nsCLBP-W-TE: 61 (65.6%) Healthy controls: 18 (58.1%) | CLBP: nsCLBP-TE: 29.0 (95% CI: 27.2; 30.9) CLBP: nsCLBP-W-TE: 28.2 (95% CI: 26.9; 29.5) Healthy controls: 26.8 (95% CI: 25.3; 28.2) |
| Tesarz, 2016 | [73] | Germany | CLBP: 176 Healthy controls: 27 | CLBP: 56.7 ± 10.0 Healthy controls: 57.1 ± 11.7 | CLBP: 128 (72.7%) Healthy controls: 17 (63.0%) | NR |
| 1st Author, Year | Risk of Bias | Applicability Concerns | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Patient Selection | What Index Test | Index Test | Reference Standard | Flow and Timing | Patient Selection | What Index Test | Index Test | Reference Standard | |
| Ansuategui Echeita, 2020a [41] | ☺ | CSI | ☹ | ☹ | N/A | ☺ | CSI |  | ☹ |
| NOS | ☹ | NOS | | ||||||
| Ansuategui Echeita, 2020b [42] | | CSI | | ☹ | N/A | | CSI | ☺ | ☹ |
| Aoyagi, 2019 [43] | | PPT | | ☹ | N/A | ☺ | PPT | ☺ | ☹ |
| CPM | | CPM | ☺ | ||||||
| Aoyagi, 2020 [44] | ☹ | FM survey (WPI & SS) | | ☹ | N/A | ☺ | FM survey (WPI & SS) | ☺ | ☹ |
| Ashina, 2018 [45] | ☺ | TTS | ☺ | ☹ | N/A | ☹ | TTS | | ☹ |
| PPT | ☺ | PPT | | ||||||
| Bid, 2017 [46] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Bilika, 2019 [47] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Chiarotto, 2018 [48] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Clark, 2018 [49] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Clark, 2019 [50] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Cuesta-Vargas, 2016 [51] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Defrin, 2014 [52] | | QST allodynia | ☺ | ☹ | N/A | ☺ | QST allodynia | ☹ | ☹ |
| Dixon, 2016 [53] | | SHS | | ☹ | N/A | ☺ | SHS | ☹ | ☹ |
| Hubscher, 2014 [54] | | thermal QST | ☹ | ☹ | N/A | ☺ | thermal QST | | ☹ |
| Huysmans, 2018 [55] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Ide, 2020 [56] | ☹ | CSI | ☺ | ☹ | N/A | ☹ | CSI | ☺ | ☹ |
| Knezevic, 2018 [57] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Knezevic, 2020 [58] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Kregel, 2016 [59] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Kregel, 2018 [60] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| PPT | | PPT | ☺ | ||||||
| CPM | | CPM | ☺ | ||||||
| Leemans, 2020 [61] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Mayer, 2012 [25] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| McKernan, 2019 [62] | | CSI | | ☹ | N/A | | CSI | ☺ | ☹ |
| MBM | | MBM | | ||||||
| MPQ | | MPQ | | ||||||
| Mehta, 2017 [63] | | PPT | | ☹ | N/A | ☺ | PPT | | ☹ |
| CPM | | CPM | | ||||||
| Mibu, 2019 [64] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| PPT | | PPT | | ||||||
| TS | | TS | | ||||||
| Miki, 2020 [65] | | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Müller, 2019 [66] | | QST | | ☹ | N/A | ☺ | QST | | ☹ |
| Neblett, 2017 [67] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Noord, van der, 2018 [68] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Serrano-Ibáñez, 2020 [69] | ☹ | CSI | | ☹ | N/A | ☹ | CSI | ☺ | ☹ |
| Sharma, 2020 [70] | ☺ | CSI | ☺ | ☹ | N/A | ☺ | CSI | ☺ | ☹ |
| Smart,. 2012 [71] | | N/A | ☹ | ☹ | N/A | | N/A | ☹ | ☺ |
| Tesarz, 2015 [72] | | QST | | ☹ | N/A | ☺ | QST | | ☹ |
| Tesarz, 2016 [73] | | QST | | ☹ | N/A | ☺ | QST | | ☹ |
= Unknown, CPM: conditioned pain modulation, CSI: central sensitisation inventory, FM-survey: Fibromyalgia survey, MBM: Michigan Body Map—revised version, MPQ: McGill Pain Questionnaire—short form-revised, N/A: not applicable. NOS: waddle non-organic signs, PPT: pressure pain threshold, QST: quantitative sensory testing, SHS: Sensory Hypersensitivity Scale, SS: symptom severity, TS: temporal summation, TTS: total tenderness score, WPI: widespread pain index.| 1st Author, Year | Definition of HACS or HACS Similar Definition | Reference Definition HACS (1st Author, Year) | Prevalence HACS in Patients with CLBP Stated in the Article | CSI | |
|---|---|---|---|---|---|
| Mean | Prevalence (Cut-Off CSI 40) | ||||
| Ansuategui Echeita, 2020a [41] # | “Central Sensitisation was introduced as a possible pathophysiological mechanism in several chronic pain conditions, including a subgroup of patients with CBP.” | Woolf, 1983 [16] Roussel, 2013 [13] | NR | 34.7 ± 13.1 | 22 out of 56 (39.3%) |
| Ansuategui Echeita, 2020b [42] # | “In a subgroup of patients with chronic pain, pain might not be direct reflection of the presence of a noxious peripheral stimulus (nociceptive pain) nor the nervous system (neuropathic pain), but could be the result of a condition in which the CNS is in a hypersensitive state; central sensitisation.” | Woolf, 2011 [18] | |||
| Aoyagi, 2019 [43] | “Defined as augmented central pain processing.” | Woolf, 2007 [77] Latremoliere, 2009 [78] Woolf, 2011 [18] Clauw, 2015 [79] Nijs, 2014 [80] Roussel, 2013 [13] | NR | NA | NA |
| Aoyagi, 2020 [44] | “Defined as amplified pain processing in the central nervous system.” | Clauw, 2015 [79] Nijs, 2015 [81] Roussel, 2013 [13] | NR | NA | NA |
| Ashina, 2018 [45] # | “Both back pain and primary headache disorders may play a role in the sensitisation of partially overlapping central nociceptive pathways.” | Yoon, 2013 [82] | NR | NA | NA |
| Bid, 2017 [46] | “CS is described by the International Association for the Study of Pain (IASP) as: "Increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input". CS is also defined as "an augmentation of responsiveness of central neurons to input from unimodal and polymodal receptors".” | Loeser, 2008 [7] Meyer, 1995 [83] | Experimental (n = 64): 78.1% Control (n = 64): 64,1% Based on the CSI | Baseline Experimental: 45.68 Control: 37.34 Week 4 Experimental: 23.42 Control: 28.21 Week 8 Experimental: 11.17 Control: 21.17 | 91 out of 128 (71.1%) |
| Bilika, 2020 [47] # | “A phenomenon of hypersensitivity of the central nervous system in patients with chronic pain.” | Roussel, 2013 [13] Woolf, 2011 [18] | NR | 31.79 ± 12.19 | CLBP only: 9 out of 28 (32.14%) CLBP+: 1 out of 23 (4.17%) |
| Chiarotto 2018 [48] # | “an amplification of neural signalling within the central nervous system that elicits pain hypersensitivity” | Woolf, 2011 [18] | NR | 33.93 ± 11.88 | NR |
| Clark, 2018 [49] | “Central sensitisation involves facilitation of peripheral stimulus processing and alterations in descending inhibitory control of nociceptive input to the brain.” | Woolf, 2011 [18] Nijs, 2010 [76] Mayer, 2012 [25] | NR | 46.14 ± 19.39 | 16 out of 21 (76.2%) |
| Clark, 2019 [50] # | “A dysregulation of the central nervous system causing neuronal hyperexcitability, characterized by generalized hypersensitivity of the somatosensory system to both noxious and non-noxious stimuli.” | Nijs, 2010 [76] Mayer, 2012 [25] Neblett, 2013 [84] | NR | 50.10 ± 13.86 | 125 out of 165 (75.8%) |
| Cuesta-Vargas, 2016 [51] # | “CS involves an abnormal increase of pain caused by neuronal hyperexcitability and dysfunction in descending and ascending pathways in the central nervous system.” | Kindler, 2011 [85] Heinricher, 2009 [86] | NR | CLBP only: 22.57 ± 11.37 CLBP+: 25.62 ± 12.22 | CLBP only: 7 out of 107 (6.5%) CLBP+: 7 out of 73 (9.6%) |
| Defrin, 2014 [52] | “Current pain theory holds that sustained peripheral noxious input, whether due to sensitized sensory endings or ectopic pacemaker activity, may secondarily initiate a state of spinal central sensitisation. In this state, afferent input is amplified and activity in low threshold Ab mechanosensitive afferents is rendered painful (Ab pain). A well-known example is secondary hyperalgesia, a region of hypersensibility to light touch (tactile allodynia) on the skin that surrounds the location of a primary noxious input.” | Raja, 1984 [87] Torebjörk, 1992 [88] Woolf, 2011 [18] | CLBP+: 60.8%, based on the presence of tactile allodynia CLBP only: 13.3% | NA | NA |
| Dixon, 2016 [53] | “Central sensitisation is an amplified state of neural signalling in the central nervous system (CNS) that is implicated in the pathogenesis of several chronic conditions that primarily involve pain and complex, multisymptom illnesses. When in the sensitized state, the CNS amplifies the sensory processing of the peripheral inputs so that the experience of the individual no longer accurately reflects the information provided by peripheral inputs. This state has been described as an increase in signal gain in which low-level sensory inputs are amplified into stronger signals, or as a decrease in signal inhibition processes, or both.” | Kaya, 2013 [89] Lluch, 2014 [90] Wang, 2014 [91] Batheja, 2013 [92] Woolf, 2011 [18] | NR | NA | NA |
| Hubscher, 2014 [54] | “Parallel to this peripheral phenomenon, intense ongoing peripheral nociceptive input can lead to altered central mechanisms, such as, an immediate-onset and lasting increase in the excitability of dorsal horn pain transmission neurons, referred to as central sensitisation. Central sensitisation may manifest as pain hypersensitivity (eg, allodynia, hyperalgesia, temporal summation [TS]) that can spread to non-injured areas.” | Ji, 2003 [93] Salter, 2004 [94] Woolf, 2011 [18] | NR | NA | NA |
| Huysmans, 2018 [55] | “Central sensitisation can be defined as a process of abnormal and intense enhancement of pain caused by increased neuronal responses to stimuli in the central nervous system. This central hyperexcitability is associated with altered sensory processing in the brain, malfunctioning of endogenous pain inhibitory systems, increased activity of pain facilitatory pathways, and temporal summation of second pain and/or wind-up, which leads to dysfunctional endogenous analgesic control.” | Nijs, 2015 [81] Mayer, 2012 [25] Yunus, 2007 [95] Nijs, 2010 [76] Nijs, 2011 [96] Woolf, 2011 [18] Staud, 2007 [97] Meeus, 2008 [98] Meeus, 2007 [99] | NR | 32.92 ± 12.76 (range: 16–66) | 12 out of 38 (31.6%) |
| Ide, 2020 [56] # | “The International Association for the Study of Pain defines central sensitisation (CS) as “increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input”.” | Loeser, 2008 [7] | NR | CLBP only: 7.76 ± 6.43 CLBP+: 17.77 ± 9.93 | CLBP only: 0 out of 46 (0%) CLBP+: 4 out of 206 (1.94%) |
| Knezevic, 2018 [57] # | “Central sensitisation (CS) represents “increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input.” Peripheral stimuli that are otherwise innocuous can produce augmented, prolonged, and widely spread pain.” | International Association for the Study of Pain, 2012 [100] Woolf, 2011 [18] | NR | CLBP only: 36.94 ± 16.15 CLBP+: 44.66 ± 14.98 | CLBP only: 68 out of 157 (43.3%) |
| Knezevic, 2020 [58] # | “Central sensitisation refers to hypersensitivity of the central nervous system, resulting in enhancement of pain sensations.” | Woolf, 2011 [18] Mayer, 2012 [25] Neblett, 2017 [67] | NR | CLBP only: 36.42 ± 15.51 CLBP+: 44.64 ± 13.94 | CLBP only: 65 out of 155 (41.9%) CLBP+: 51 out of 88 (58.0%) |
| Kregel, 2016 [59] # | “Central sensitisation (CS) is a neurophysiological state resulting in hyperexcitability in the central nervous system. According to Woolf, CS is “operationally defined as an amplification of neural signalling within the central nervous system that elicits pain hypersensitivity.” In clinical practice, CS manifests as pain hypersensitivity, particularly dynamic tactile allodynia, secondary punctate or pressure hyperalgesia, longer aftersensations, and enhanced temporal summation.” | Woolf, 2011 [18] Nijs, 2010 [76] | NR | CLBP only: 23.67 ± 10.50 CLBP+: 38.90 ± 14.77 | CLBP only: 1 out of 4 (25.0%) CLBP+: 7 out of 11 (63.6%) |
| Kregel, 2018 [60] | “Dysregulations of ascending and descending pathways have been observed in chronic pain patients, resulting in clinical signs such as allodynia, hyperalgesia, hypersensitivity, increased or prolonged aftersensations, and temporal summation to noxious and non-noxious stimuli. Extended high-frequency stimulation of neurons has been found to cause long-lasting cellular changes because of elevated cell responsiveness, a diminished working of the inhibitory cells and network sprouting. This increase in excitability and synaptic working in the central nociceptive pathways is called central sensitisation.” | Woolf, 2011 [18] Schliessbach, 2013 [101] Baranauskas, 1998 [102] Nijs, 2015 [81] Lluch, 2014 [90] Maixner, 1998 [103] Wilgen, van, 2013 [104] | NR | CLBP: 39.06 ± 11.61 | NR |
| Leemans, 2020 [61] | NR | NA | NR | CLBP: Experimental group: 35.9 ± 10.5 CLBP: Control group: 31 ± 10.8 | NR |
| Mayer, 2012 [25] | In the abstract: “Central sensitisation has been proposed as a common pathophysiological mechanism to explain related syndromes for which no specific organic cause can be found.” In the introduction: “Central sensitisation, which involves an abnormal and intense enhancement of pain by mechanisms in the central nervous system, maybe the common link between these disorders.” | Yunus, 2007 [95] | NR | CLBP only: 41.6 ± 14.8 | NR |
| McKernan, 2019 [62] # | “Central sensitisation—the amplification of neural signalling in the central nervous system contributing to hyperalgesia.” | Woolf, 2011 [18] | NR | CLBP only: 50.83 ± 16.67 | NR |
| Mehta, 2017 [63] | “Central sensitisation; this may manifest as pain hypersensitivity, in particular dynamic tactile allodynia, secondary punctate or pressure hyperalgesia, and enhanced temporal summation. Central sensitisation is a hyperexcitability state in nociceptive pathways and has been suggested to be the main cause of chronic pain conditions.” | NR | NR | NA | NA |
| Mibu, 2019 [64] | “The International Association for the Study of Pain defines central sensitisation as an increased responsiveness of nociceptive neurons in the central nervous system to normal or subthreshold afferent input.” | Loeser, 2008 [7] | n = 104: 19 (18.3%) Based on PPT and TS | CLBP: 25.5 ± 12.2 | NR |
| Miki, 2020 [65] | “Central sensitisation is defined by the International Academy of Pain as a functional dysregulation of the central nervous system to normal or subthreshold afferent input. The nociceptive hyperexcitability and perception threshold of sensory information are reduced, and pain and other clinical symptoms are amplified.” | Loeser, 2008 [7] Woolf, 1983 [16] | NR | CLBP: 24.44 ± 12.78 | 31 out of 238 (13.0%) |
| Müller, 2019 [66] | “Central hypersensitivity: Prolonged or intense nociceptive input induces neuroplastic changes that lead to central nervous system hypersensitivity.“ | Woolf, 2011 [18] | NR | NA | NA |
| Neblett, 2017 [67] # | “Central sensitisation is a relatively new concept, which is gaining wide acceptance as a functional dysregulation in the central nervous system, resulting in nociceptive hyperexcitability and a lowered threshold for perception of sensory information, which amplifies pain and other clinical symptoms.” | Adams, 2015 [105] | NR | CLBP only: 44.21 ± 15.24 CLBP+: 49.24 ± 15.01 | CLBP only: 200 out of 322 (62.1%) CLBP+: 237 out of 323 (73.4%) |
| Noord van der, 2018 [68] # | “Central sensitisation is a common neurophysiological phenomenon in patients with chronic pain. Central sensitisation involves a hyperexcitability to a stimulus, resulting in an abnormal response to both noxious and non-noxious stimuli.” | Schliessbach, 2013 [101] Woolf, 2011 [18] | NR | CLBP only: 29.41 ± 14.03 CLBP+: 40.55 ± 14.28 | CLBP only: 4 out of 17 (23.5%) CLBP+: 32 out of 67 (47.8%) |
| Serrano-Ibáñez, 2020 [69] # | “The International Association of the Study of Pain has defined central sensitisation as the increased responsiveness of nociceptive neurons in the central nervous system to normal or subthreshold afferent input.” | Loeser, 2008 [7] | NR | CLBP: 63.68 ± 13.57 | CLBP: 16 out of 24 (66.7%) |
| Sharma, 2020 [70] # | “Central sensitisation involves the amplification of pain, and hypersensitivity to other environmental stimuli, within the central nervous system.” | Woolf, 2011 [18] | NR | CLBP only: 24.27 ± 13.12 CLBP+: 24.00 ± 12.53 | CLBP only: 3 out of 22 (14.8%) CLBP+: 4 out of 27 (13.6%) |
| Smart, 2012 [71] # | “Central sensitisation pain (CSP) refers to pain that arises or persists as a result of aberrant processing and/or hypersensitivity within the diffuse neural networks of the central nervous system (CNS) engaged in nociception, in the absence of or disproportionate to somatic tissue or peripheral nerve pathology.” | Costigan, 2009 [106] | NR | NR | NR |
| Tesarz, 2015 [72] | NR | NA | NR | NA | NA |
| Tesarz, 2016 [73] | NR | NA | NR | NA | NA |
| Total | 50.65% | All | 1013 out of 2347 (43.2%) | ||
| CLBP only | 289 out of 701 (41.2%) | ||||
| CLBP+ | 343 out of 819 (41.9%) | ||||
| Questionnaires | ||||
|---|---|---|---|---|
| CSI (n = 23) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Comparison between assessment methods | |
| Ansuategui Echeita, 2020a [41] | Quantify the severity of symptoms CS | Not reported | CSI with Waddle Non-organic Signs. | |
| Ansuategui Echeita, 2020b [42] | Quantify the severity of symptoms CS | Not reported | CSI with Lifting capacity | |
| Bid, 2017 [46] | A score above 40 indicates the presence of CS | Not reported | Comparing CSI (CS group/NoCS group) with PPT scores, numeric pain rating scale, Roland Morris Disability Questionnaire, Fear-Avoidance Beliefs Questionnaire, Trunk Flexors Endurance, and Trunk Extensor Endurance | |
| Bilika, 2020 [47] | Identify symptoms associated with CS | Internal consistency: Cronbach’s α = 0.994 Test-retest: ICC = 0.993 | CSI with pain catastrophizing scale. | |
| Chiarotto, 2018 [48] | Identify patient’s symptoms related to CS | Internal consistency: Cronbach’s α = 0.87 | No comparison | |
| Clark, 2018 [49] | Person’s symptoms likely to be attributable to CS | Not reported | CSI (CSI High group/CSI Low group) with Sensory Seeking, Sensory Sensitive, trait anxiety, Low Registration, and Sensation Avoidance. | |
| Clark, 2019 [50] | Individual’s symptoms likely to be attributable to CS | Not reported | CSI with sensory profiles, Sensory Sensitivity, sensation avoiding, low registration, sensation seeking, and trait anxiety. | |
| Huysmans, 2018 [55] | The degree of symptoms of CS | Not reported | CSI and 1-minute stair-climbing test, Pain catastrophizing scale, visual analogue scale at this moment, Brief Illness Perception Questionnaire, Quebec Back Pain Disability Scale, and Tampa Scale for Kinesiophobia. | |
| Ide, 2020 [56] | Assessing CS syndrome (CSS) | Not reported | CSI and EuroQOL 5-dimension, Neck Disability Index, and Oswestry Disability Index. | |
| Knezevic, 2018 [57] | Assesses 25 symptom dimensions associated with CS and CSS. | Internal consistency: Cronbach α = 0.909 Test-retest: ICC = 0.947 | No comparison | |
| Knezevic, 2020 [58] | A measure of symptoms related to CS and CSS | Not reported | CSI with Medical Outcomes Study, Fear-Avoidance Components Scale, Oswestry Disability Index, Short Form-36, Pain Catastrophizing Scale, pain intensity, and Multidimensional Scale of Perceived Social Support. | |
| Kregel, 2016 [59] | Measure the overlapping symptom dimensions present in CS. | Internal consistency: Cronbach α= 0.91 Test-retest: ICC = 0.88 | No comparison | |
| Kregel, 2018 [60] | An indirect tool for CS symptomatology evaluation | Not reported | CSI with PPT, CPM, current pain intensity, quality of life, pain disability, and pain catastrophizing score | |
| Leemans, 2020 [61] | Identify key symptoms associated with CS | Not reported | No comparison | |
| Mayer, 2012 [25] | Assess symptoms associated with CS | Internal consistency: Cronbach α = 0.879. Test-retest: ICC = 0.817 | No comparison | |
| McKernan, 2019 [62] | Assess key polysomatic symptoms associated with a CS disorder | Not reported | CSI with Trauma History Questionnaire, PTSD, Michigan Body Map, McGill Pain Questionnaire, Multidimensional Experiential Avoidance Questionnaire. | |
| Mibu, 2019 [64] | Assess health-related symptoms in CSS | Sensitivity: CS+ 1 or CS− 1: 73.7% (cut-off: 20) CSS+ 2 or CSS− 2: 69.2% (cut-off: 28) Specificity: CS+ 1 or CS− 1: 37.7% CSS+ 2 or CSS− 2: 69.2% | CSI and duration of symptoms, EQ-5D, pain intensity, pain interference, Widespread Pain Index score, PPT, and temporal summation. | |
| Miki, 2020 [65] | Significant deficits in CS | Not reported | CSI (low CSI group/high CSI group) with pain catastrophizing scale, Tampa Scale for Kinesiophobia, Hospital Anxiety and Depression Scale, pain intensity for LBP, pain intensity for leg pain, Roland Morris Disability Questionnaire, and EuroQoL 5 dimensions. | |
| Neblett, 2017 [67] | Screener for high risk of having CSS | Not reported | Explored the five CSI severity levels with patient-reported outcomes: for pain intensity, perceived disability, depressive symptoms, sleep disturbance, pain-reported outcomes; pain intensity, perceived disability, depressive symptoms, sleep disturbance, pain-related anxiety, and somatization-related symptoms. | |
| Noord, van der, 2018 [68] | Identifying symptoms of CS in patients with chronic pain disorders | Not reported | CSI part A with CSI part B, depression, anxiety, WPI, pain intensity, and pain catastrophizing scale. | |
| Serrano-Ibáñez, 2020 [69] | Severity of CS | Not reported | CSI with daily routines, decreased physical activity, diminished social support, emotional distress, and pain intensity. | |
| Sharma, 2020 [70] | Assess somatic and emotional health-related symptoms associated with CS | Internal consistency: Cronbach’s α = 0.87 ICC = 0.98 (95% CI: 0.97, 0.99) | CSI with the pain catastrophizing scale (strong correlation), number of pain descriptors(McGill Pain Questionnaire) (moderate correlation), and pain intensity (weak correlation) | |
| MBM (n = 1) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Version | Comparison |
| McKernan, 2019 [62] | Indicate widespread pain related to CS | Not reported | Revised version [107] | Exposure to trauma and PTSD increases CS. Findings need to be objectified with laboratory markers of CS. |
| MPQ (n = 1) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Version | Comparison |
| McKernan, 2019 [62] | Assessing various dimensions of pain (Indicator for CS) | Not reported | SF-MPQ-2 [108,109] | Exposure to trauma and PTSD increases CS. Findings need to be objectified with laboratory markers of CS. |
| WPI (n = 2) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Version | Comparison |
| Aoyagi, 2019 [43] | Assesses experience pain or tenderness in 19 specific body areas. As a continuous variable to measure CS severity | Not reported | as part of the 2011 FM survey [110,111] | FM positive when WPI ≥ 7 and ≥ 5 or WPI 3–6 and SS ≥ 9. Conclusion article: FM positive = CS |
| Aoyagi, 2020 [44] | Scores from the WPI and SS are combined to determine the presence and severity of CS. | Not reported | As part of the 2011 FM survey [110,111] | Cutoff scores of ≥ 12 with a combination of either WPI score ≥ seven and SS score ≥ five or WPI score 3 to 6 and SS score ≥ 9 distinguish those with CS as FM positive. Higher total scores indicate a greater degree of CS. |
| QST measurements | ||||
| PPT (n = 7) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Method /location(s) | Comparison |
| Aoyagi, 2019 [43] | Identifying individuals with CS | Not reported | Handheld algometer Thumbnail Lower back | PPT values were compared between the FM-negative and FM-positive group. FM scores were used as a dichotomous variable to identify the presence of CS and as a continuous variable to examine associations between CS, QST and other self-reported measures. |
| Aoyagi, 2020 [44] | Identifying individuals with CS | Not reported | Handheld algometer Thumbnail Lower leg | PPT values were compared between the FM-negative and FM-positive group. |
| Kregel, 2018 [60] | To objectify CS symptomatology/evaluation of CS symptoms | Not reported | Handheld algometer Lower back Hand Upper leg | The CSI compared with measures of pain intensity, quality of life, pain disability, pain catastrophizing, PPT, and CPM |
| Leemans, 2020 [61] | Altered sensory processing, including signs of CS | Not reported | Handheld algometer Three spots in the lower back 2nd Toe | No conclusions about CS |
| Mibu, 2019 [64] | The lowest tertile PPT, in combination with a positive TS, are patients with CS. | Not reported | Handheld algometer Lower arm | No comparison |
| Tesarz, 2015 [72] | It covers all relevant aspects of the somatosenosory system, including large and small fibre functions and signs of central sensitisation. | Not reported | Handheld algometer Low back Dorsum hand | No comparison |
| Tesarz, 2016 [73] | It covers all relevant aspects of the somatosenosory system, including large and small fibre functions, and signs of central sensitisation | Not reported | Handheld algometer Low back Dorsum hand | No comparison |
| CPM (n = 3) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Method/location(s) | Comparison |
| Aoyagi, 2019 [43] | Discriminate individuals with CS | Not reported | PPT before and after. Conditioning painful stimulus cuff to ischemic pain. Thumbnail Lower back | PPT values were compared between the FM-negative and FM-positive group. FM scores were used as a dichotomous variable to identify the presence of CS and as a continuous variable to examine associations between CS, QST and other self-reported measures. |
| Kregel, 2018 [60] | To objectify CS symptomatology/evaluation of CS symptoms | Not reported | Cold Pressor Test. 1 min. 22 °C, 2 min. 12 °C, 30 s. wait, PPT measurements Upper leg | The CSI compared with measures of pain intensity, quality of life, pain disability, pain catastrophizing, PPT, and CPM |
| Leemans, 2020 [61] | Altered sensory processing, including signs of CS, to evaluate the efficacy of the descending inhibitory modulation of pain | Not reported | Cold pressor test. 0.7 °C until intolerable or 2 min. PPT before and after 2nd Toe | No comparison |
| TS (n = 4) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Method/ location(s) | Comparison |
| Hubscher, 2014 [54] | Thermal pain thresholds and tolerance (heat/cold) and TS of heat pain. The distal site as a marker of possible CS. | Not reported | One sequence of 10 consecutive heat pulses of <1-s duration at an interstimulus interval of 0.33 Hz was delivered. The temperature increased from 41 °C to a maximum of 47 °C at a rate of 10 °C/3. The pain intensity of each heat pulses was assessed. Location: 2 sites: on the surface of the low back and a distal site, the volar surface of the forearm | No comparison |
| Mibu, 2019 [64] | The lowest tertile PPT, in combination with a positive TS, are patients with CS. | Not reported | Previous determined PPT was applied ten times Lower arm | No comparison |
| Tesarz, 2015 [72] | It covers all relevant aspects of the somatosenosory system, including large and small fibre functions, and signs of central sensitisation | Not reported | Pinprick 256N Low back Dorsum hand | No comparison |
| Tesarz, 2016 [73] | It covers all relevant aspects of the somatosenosory system, including large and small fibre functions and signs of central sensitisation. | Not reported | Pinprick 256N Low back Dorsum hand | No comparison |
| Thermal QST (n = 3) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Method/Location(s) | Comparison |
| Hubscher, 2014 [54] | Thermal pain thresholds and tolerance (heat/cold) and TS of heat pain. The distal site as a marker of possible CS. | Not reported | CPT, CPTol, HPT, HPTol. 2 sites: on the surface of the low back and a distal site, the volar surface of the forearm | No comparison |
| Tesarz, 2015 [72] | All relevant aspects of the somatosenosory system, including large and small fibre functions and signs of central sensitisation. | Not reported | TSA 2001-II CDT, WDT, TSL, CPT, HPT. Low back Dorsum hand | No comparison |
| Tesarz, 2016 [73] | All relevant aspects of the somatosenosory system, including large and small fibre functions and signs of central sensitisation. | Not reported | TSA 2001-II CDT, WDT, TSL, CPT, PHS, HPT. Low back Dorsum hand | No comparison |
| Other QST measures (n = 2) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Method/Location(s) | Comparison |
| Tesarz, 2015 [72] | All relevant aspects of the somatosenosory system, including large and small fibre functions and signs of central sensitisation | Not reported | MPT (Pinprick stimulators), MPS (Pinprick stimulators), DMA (brush, cotton wool and Q-tip), MDT (von Frey filaments), VDT (tuning fork 64 Hz) Low back Dorsum hand | No comparison |
| Tesarz, 2016 [73] | It covers all relevant aspects of the somatosenosory system, including large and small fibre functions and signs of central sensitisation. | Not reported | MPT (Pinprick stimulators), MPS (Pinprick stimulators), DMA (brush, cotton wool and Q-tip), MDT (von Frey filaments), VDT (tuning fork 64 Hz) Low back Dorsum hand | No comparison |
| No measurements (n = 6) | ||||
| Study (1st author, year) | The goal of the test | Clinimetrics | Explanation of possible HACS measures | |
| Ashina, 2018 [45] | Not reported | Not reported | Discussion section: lower cephalic and extra-cephalic PPT and higher TTS in the chronic headache group than episodic headache and control groups suggest that comorbidity of back pain and frequent headaches is associated with signs of CS. TTS is increased, suggesting that low back pain can induce CS. | |
| Defrin, 2014 [52] | Not reported | Not reported | Results section: the development of tactile allodynia and inference of CS has more to do with individual predisposition than with the intensity of the precipitating noxious input. Discussion section: Neural mechanism: CS and ectopic hyperexcitability. The presence of tactile allodynia strongly implies the presence of CS. The observed ~60% incidence of leg allodynia in radicular patients suggests that peripheral nervous system generators of leg pain often induce CS. The 40% who did not (yet) develop CS despite comparable leg pain were presumably less prone to doing so. | |
| Dixon, 2016 [53] | Not reported | Not reported | CS is used as an explanatory model of the results | |
| Mehta, 2017 [63] | Not reported | Not reported | Changes in PPT and CPM are consistent with normalization of peripheral and CS | |
| Müller, 2019 [66] | Not reported | Not reported | Negative findings for QST as a predictor for FBSS. They conclude that the negative findings do not necessarily mean that central hypersensitivity is not involved in FBSS. | |
| Smart, 2012 [71] | Not reported | Not reported | Based on clinical examination, patients were, i.e., CS | |
| CLBP Only | CLBP+ | |||
|---|---|---|---|---|
| Author, Year | Assessment | Type | CSI Part A | |
| Disability | ||||
| Ansuategui Echeita, 2020b [42] | Lifting capacity | PA | −0.53 | |
| Ide, 2020 [56] # | Neck Disability Index | Q | 0.58 | 0.60 |
| Ide, 2020 [56] # | Oswestry Disability Index ᵕ | Q | 0.50 | |
| Kregel, 2018 [60] | Physical components (Short Form-36) ᵕ | Q | −0.62 | |
| Pain | ||||
| Huysmans, 2018 [55] | Pain Score VAS: 7 days | Q | 0.51 | |
| Huysmans, 2018 [55] | Pain Score VAS: now | Q | 0.51 | |
| McKernan, 2019 [62] | McGill Pain Questionnaire ᵕ | Q | 0.62 | |
| McKernan, 2019 [62] | Michigan Body Map | Q | 0.55 | |
| Serrano-Ibáñez, 2020 [69] # | NRS pain intensity ᵕ | Q | 0.60 | |
| Co-morbidities | ||||
| Van der Noord, 2018 [68] | Central sensitivity syndrome | Q | 0.51 | |
| Psychological elements | ||||
| Bilika, 2020 [47] # | Pain Catastrophizing Scale (total score) ᵔ ᵕ | Q | 0.74 | 0.56 |
| Clark, 2018 [49] | Sensory profile: Sensory seeking ᵕ | Q | −0.53 | |
| Clark, 2018 [49] | Sensory profile: Sensory Sensitive ᵔ | Q | 0.57 | |
| Clark, 2018 [49] | State-Trait Anxiety Inventory ᵕ | Q | 0.63 | |
| Clark, 2019 [50] | Sensory profile: Low registration ᵕ | Q | 0.54 | |
| Clark, 2019 [50] | Sensory profile: Sensory Sensitive ᵔ | Q | 0.63 | |
| Huysmans, 2018 [55] | Pain Catastrophizing Scale (total score) ᵔ ᵕ | Q | 0.52 | |
| Kregel, 2018 [60] | Mental components (Short Form-36) ᵕ | Q | −0.64 | |
| McKernan, 2019 [62] | PTSD (PCL) | Q | 0.65 | |
| Miki, 2020 [65] | Anxiety (Hospital Anxiety and Depression Scale) | Q | 0.50 | |
| Miki, 2020 [65] | Pain Catastrophizing Scale (total score) ᵔ ᵕ | Q | 0.54 | |
| Serrano-Ibáñez, 2020 [69] # | Emotional distress | Q | 0.56 | |
| Sharma, 2020 [70] | Pain Catastrophizing Scale (total score) ᵔ ᵕ | Q | 0.50 | |
| Van der Noord, 2018 [68] | Anxiety (SCL-90) | Q | 0.65 | |
| Van der Noord, 2018 [68] | Depression (SCL-90) | Q | 0.67 | |
| Sleep | ||||
| Knezevic, 2020 [58] # | Sleep problem Index II (MOS sleep scale) | Q | −0.52 | |
| Indicator Tests | ||
|---|---|---|
| Hypersensitivity | Pressure pain threshold (PPT) | |
| Temporal summation | Wind-up ratio (WUR) | Positive WUR |
| Reduced pain inhibition | Conditioned pain modulation (CPM) | Negative CPM |
| Questionnaire | Central Sensitisation Inventory (CSI) | Score ≥ 40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuttert, I.; Timmerman, H.; Petersen, K.K.; McPhee, M.E.; Arendt-Nielsen, L.; Reneman, M.F.; Wolff, A.P. The Definition, Assessment, and Prevalence of (Human Assumed) Central Sensitisation in Patients with Chronic Low Back Pain: A Systematic Review. J. Clin. Med. 2021, 10, 5931. https://doi.org/10.3390/jcm10245931
Schuttert I, Timmerman H, Petersen KK, McPhee ME, Arendt-Nielsen L, Reneman MF, Wolff AP. The Definition, Assessment, and Prevalence of (Human Assumed) Central Sensitisation in Patients with Chronic Low Back Pain: A Systematic Review. Journal of Clinical Medicine. 2021; 10(24):5931. https://doi.org/10.3390/jcm10245931
Chicago/Turabian StyleSchuttert, Ingrid, Hans Timmerman, Kristian K. Petersen, Megan E. McPhee, Lars Arendt-Nielsen, Michiel F. Reneman, and André P. Wolff. 2021. "The Definition, Assessment, and Prevalence of (Human Assumed) Central Sensitisation in Patients with Chronic Low Back Pain: A Systematic Review" Journal of Clinical Medicine 10, no. 24: 5931. https://doi.org/10.3390/jcm10245931
APA StyleSchuttert, I., Timmerman, H., Petersen, K. K., McPhee, M. E., Arendt-Nielsen, L., Reneman, M. F., & Wolff, A. P. (2021). The Definition, Assessment, and Prevalence of (Human Assumed) Central Sensitisation in Patients with Chronic Low Back Pain: A Systematic Review. Journal of Clinical Medicine, 10(24), 5931. https://doi.org/10.3390/jcm10245931