
Sentinel Lymph Node Biopsy vs. Observation in Thin Melanoma: A Multicenter Propensity Score Matching Study


 , , , ,
, , , ,  , , ,
, , ,  , ,
, ,  , , , ,
, , , , 
 add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
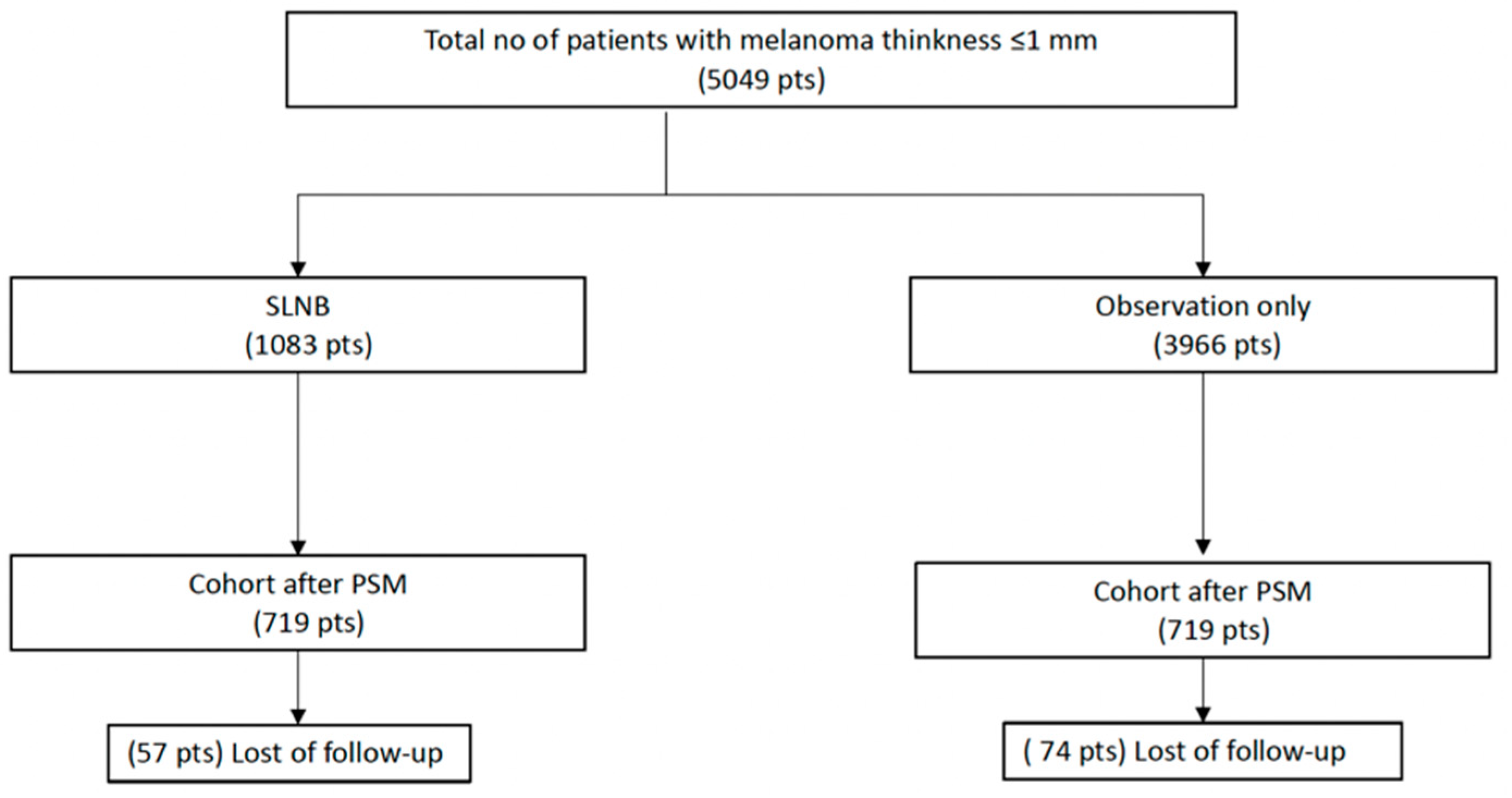
2.1. Study Population
2.2. Study Groups and Outcome Variables
2.3. Propensity Score Matching
2.4. Statistical Analysis
2.5. Missing Data
3. Results
3.1. Study Population Characteristics
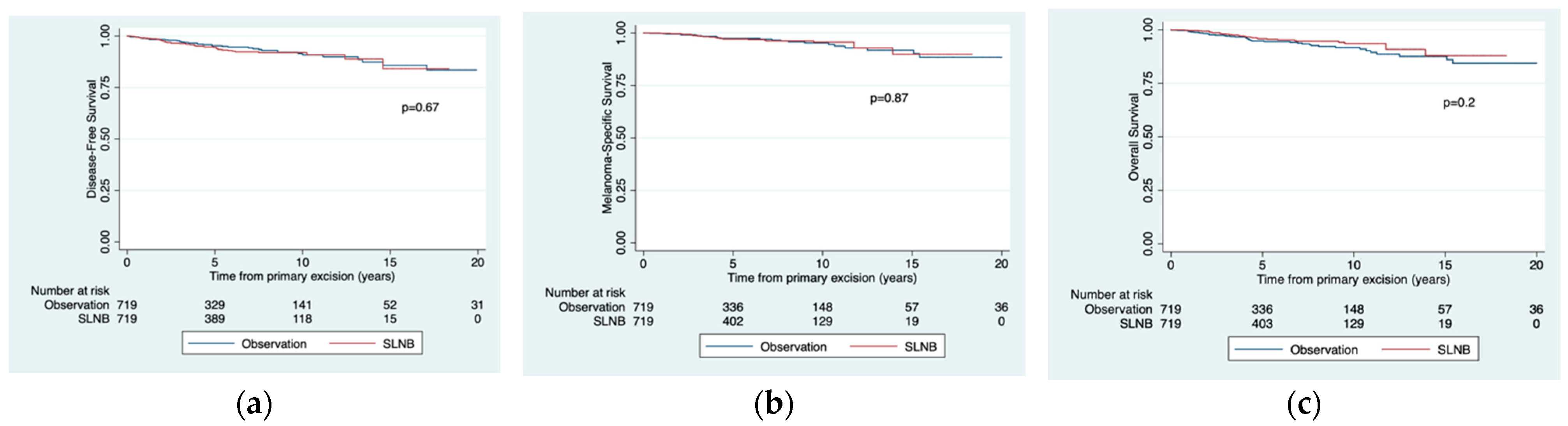
3.2. Survival Rates
3.2.1. Melanoma-Specific Survival
3.2.2. Disease-Free Survival
3.2.3. Overall Survival
3.3. Prognostic Significance of SLNB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botella-Estrada, R.; Boada-García, A.; Carrera-Álvarez, C.; Fernández-Figueras, M.; González-Cao, M.; Moreno-Ramírez, D.; Nagore, E.; Ríos-Buceta, L.; Rodríguez-Peralto, J.L.; Samaniego-González, E.; et al. Clinical Practice Guideline on Melanoma From the Spanish Academy of Dermatology and Venereology (AEDV). Actas Dermosifiliogr. 2021, 112, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Thompson, J.F.; Cochran, A.J.; Mozzillo, N.; Nieweg, O.E.; Roses, D.F.; Hoekstra, H.J.; Karakousis, C.P.; Puleo, C.A.; Coventry, B.J.; et al. Final Trial Report of Sentinel-Node Biopsy versus Nodal Observation in Melanoma. N. Engl. J. Med. 2014, 370, 599–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ríos, L.; Nagore, E.; López, J.L.; Redondo, P.; Martí, R.M.; Fernández-de-Misa, R.; Soler, B. Melanoma characteristics at diagnosis from the Spanish National Cutaneous Melanoma Registry: 15 years of experience. Actas Dermosifiliogr. 2013, 104, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Ribero, S.; Puig, S.; Boada, A.; Paradela, S.; Moreno-Ramírez, D.; Cañueto, J.; de Unamuno, B.; Brinca, A.; Descalzo-Gallego, M.A.; et al. Survival analysis and sentinel lymph node status in thin cutaneous melanoma: A multicenter observational study. Cancer Med. 2019, 8, 4235–4244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swetter, S.M.; Thompson, J.A.; Albertini, M.R.; Barker, C.A.; Baumgartner, J.; Boland, G.; Chmielowski, B.; DiMaio, D.; Durham, A.; Fields, R.C.; et al. NCCN Guidelines® Insights: Melanoma: Cutaneous, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 364–376. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [Green Version]
- Tejera-Vaquerizo, A.; Nagore, E.; Herrera-Acosta, E.; Martorell-Calatayud, A.; Martín-Cuevas, P.; Traves, V.; Herrera-Ceballos, E. Prediction of Sentinel Lymph Node Positivity by Growth Rate of Cutaneous Melanoma. Arch. Dermatol. 2012, 148, 577–584. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.B. On principles for modeling propensity scores in medical research. Pharmacoepidemiol. Drug Saf. 2004, 13, 855–857. [Google Scholar] [CrossRef]
- Tejera-Vaquerizo, A.; Fernández-Figueras, M.T.; Santos-Briz, A.; Ríos-Martín, J.J.; Monteagudo, C.; Fernández-Flores, A.; Requena, C.; Traves, V.; Descalzo-Gallego, M.A.; Rodríguez-Peralto, J.L. Protocolo de diagnóstico histológico para muestras de pacientes con melanoma cutáneo. Documento de consenso de la SEAP y la AEDV para el Registro Nacional de Melanoma. Actas Dermosifiliogr. 2021, 112, 32–43. [Google Scholar] [CrossRef]
- Amin, M.; Edge, S.; Greene, F.; Byrd, D.; Brookland, R.; Washington, M.; Gershenwald, J.E.; Copton, C. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA, 2017. [Google Scholar]
- Balch, C.M.; Wilkerson, J.A.; Murad, T.M.; Soong, S.J.; Ingalls, A.L.; Maddox, W.A. The prognostic significance of ulceration of cutaneous melanoma. Cancer 1980, 45, 3012–3017. [Google Scholar] [CrossRef]
- Botella-Estrada, R.; Traves, V.; Requena, C.; Guillen-Barona, C.; Nagore, E. Correlation of Histologic Regression in Primary Melanoma With Sentinel Node Status. JAMA Dermatol. 2014, 150, 828–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gualano, M.R.; Osella-Abate, S.; Scaioli, G.; Marra, E.; Bert, F.; Faure, E.; Baduel, E.S.; Balagna, E.; Quaglino, P.; Fierro, M.T.; et al. Prognostic role of Histologic regression in primary cutaneous melanoma: A Systematic Review and Meta-analysis. Br. J. Dermatol. 2018, 178, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Morera-Sendra, N.; Tejera-Vaquerizo, A.; Traves, V.; Requena, C.; Bolumar, I.; Pla, A.; Vázquez, C.; Soriano, V.; Nagore, E. Value of sentinel lymph node biopsy and adjuvant interferon treatment in thick (>4 mm) cutaneous melanoma: An observational study. Eur. J. Dermatol. 2016, 26, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Nagore, E.; Oliver, V.; Botella-Estrada, R.; Moreno-Picot, S.; Insa, A.; Fortea, J.M. Prognostic factors in localized invasive cutaneous melanoma: High value of mitotic rate, vascular invasion and microscopic satellitosis. Melanoma Res. 2005, 15, 169–177. [Google Scholar] [CrossRef]
- Taylor, R.C.; Patel, A.; Panageas, K.S.; Busam, K.J.; Brady, M.S. Tumor-infiltrating lymphocytes predict sentinel lymph node positivity in patients with cutaneous melanoma. J. Clin. Oncol. 2007, 25, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Büttner, P.; Bertz, J.; Burg, G.; D’Hoedt, B.; Drepper, H.; Guggenmoos-Holzmann, I.; Lechner, W.; Lippold, A.; Orfanos, C.E.; et al. Primary cutaneous melanoma. Prognostic classification of anatomic location. Cancer 1995, 75, 2484–2491. [Google Scholar] [CrossRef]
- Mocellin, S.; Pasquali, S.; Rossi, C.R.; Nitti, D. Interferon alpha adjuvant therapy in patients with high-risk melanoma: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2010, 102, 493–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, D.B. Inference and missing data. Biometrika 1976, 63, 581–592. [Google Scholar] [CrossRef]
- van Akkooi, A.C.; Voit, C.A.; Verhoef, C.; Eggermont, A.M. New developments in sentinel node staging in melanoma: Controversies and alternatives. Curr. Opin. Oncol. 2010, 22, 169–177. [Google Scholar] [CrossRef]
- Morton, D.L. Technical Details of Intraoperative Lymphatic Mapping for Early Stage Melanoma. Arch. Surg. 1992, 127, 392. [Google Scholar] [CrossRef]
- Ertekin, S.; Podlipnik, S.; Riquelme-Mc Loughlin, C.; Barreiro-Capurro, A.; Arance, A.; Carrera, C.; Malvehy, J.; Puig, S. Initial Stage of Cutaneous Primary Melanoma Plays a Key Role in the Pattern and Timing of Disease Recurrence. Acta Derm. Venereol. 2021, 101, adv00502. [Google Scholar] [CrossRef]
- Meier, F.; Will, S.; Ellwanger, U.; Schlagenhauff, B.; Schittek, B.; Rassner, G.; Garbe, C. Metastatic pathways and time courses in the orderly progression of cutaneous melanoma. Br. J. Dermatol. 2002, 147, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Barrera-Vigo, M.V.; Fernández-Canedo, I.; Blázquez-Sánchez, N.; Mendiola-Fernández, M.; Fernández-Orland, A.; Bosch-García, R.; De Troya-Martín, M.; Herrera-Ceballos, E. Longitudinal study of different metastatic patterns in the progression of cutaneous melanoma. Actas Dermosifiliogr. 2007, 98, 531–538. [Google Scholar] [CrossRef]
- Sperry, S.M.; Charlton, M.E.; Pagedar, N.A. Association of Sentinel Lymph Node Biopsy With Survival for Head and Neck Melanoma. JAMA Otolaryngol. Neck Surg. 2014, 140, 1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murtha, T.D.; Han, G.; Han, D. Predictors for Use of Sentinel Node Biopsy and the Association with Improved Survival in Melanoma Patients Who Have Nodal Staging. Ann. Surg. Oncol. 2018, 25, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Sinnamon, A.J.; Gimotty, P.A.; Karakousis, G.C.; Yang, Y.X. Survival Outcomes Following Lymph Node Biopsy in Thin Melanoma—A Propensity-Matched Analysis. Ann. Surg. Oncol. 2021, 28, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Zager, J.S.; Shyr, Y.; Chen, H.; Berry, L.D.; Iyengar, S.; Djulbegovic, M.; Weber, J.L.; Marzban, S.S.; Sondak, V.K.; et al. Clinicopathologic predictors of sentinel lymph node metastasis in thin melanoma. J. Clin. Oncol. 2013, 31, 4387–4393. [Google Scholar] [CrossRef]
- Venna, S.S.; Thummala, S.; Nosrati, M.; Leong, S.P.; Miller, J.R.; Sagebiel, R.W.; Kashani-Sabet, M. Analysis of sentinel lymph node positivity in patients with thin primary melanoma. J. Am. Acad. Dermatol. 2013, 68, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Balch, C.M.; Thompson, J.F.; Gershenwald, J.E.; Soong, S.J.; Ding, S.; McMasters, K.M.; Coit, D.G.; Eggermont, A.M.M.; Gimotty, P.A.; Johnson, T.M.; et al. Age as a predictor of sentinel node metastasis among patients with localized melanoma: An inverse correlation of melanoma mortality and incidence of sentinel node metastasis among young and old patients. Ann. Surg. Oncol. 2014, 21, 1075–1081. [Google Scholar] [CrossRef] [Green Version]
- Iglesias-Pena, N.; Paradela, S.; Tejera-Vaquerizo, A.; Boada, A.; Fonseca, E. Cutaneous Melanoma in the Elderly: Review of a Growing Problem. Actas Dermosifiliogr. 2019, 110, 434–447. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Before Propensity Score Matching | After Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| OBSERVATION | SLNB | p-Value | OBSERVATION | SLNB | p-Value | |
| n = 3966 | n = 1083 | n = 719 | n = 719 | |||
| Year | N (%) | N (%) | <0.001 | N (%) | N (%) | 0.675 |
| ≤2000 | 1295 (33) | 97 (9) | 103 (14) | 88 (12) | ||
| 2001–2006 | 827 (21) | 294 (27) | 186 (26) | 197 (27) | ||
| 2007–2011 | 986 (25) | 334 (31) | 227 (32) | 227 (32) | ||
| 2012–2017 | 858 (22) | 358 (33) | 203 (28) | 207 (29) | ||
| Hospital | ||||||
| Salamanca | 108 (3) | 21 (2) | <0.001 | 12 (2) | 14 (2) | 0.544 |
| Valencia IVO | 440 (11) | 218 (20) | 119 (17) | 132 (18) | ||
| Turin | 1494 (38) | 296 (27) | 187 (26) | 204 (28) | ||
| Barcelona | 1017 (26) | 202 (19) | 163 (23) | 160 (22) | ||
| Badalona | 361 (9) | 194 (18) | 133 (18) | 105 (15) | ||
| Coimbra | 65 (2) | 14 (1) | 14 (2) | 12 (2) | ||
| A Coruña | 202 (5) | 74 (7) | 51 (7) | 43 (6) | ||
| Sevilla | 203 (5) | 40 (4) | 23 (3) | 31 (4) | ||
| Valencia La Fe | 76 (2) | 24 (2) | 17 (2) | 18 (3) | ||
| Sex | 0.001 | 0.459 | ||||
| Male | 1646 (42) | 509 (47) | 324 (45) | 338 (47) | ||
| Female | 2320 (58) | 573 (53) | 395 (55) | 381 (53) | ||
| Mean age (sd), y | 52.4 (16.4) | 51.9 (14.7) | 0.3372 | 52.9 (16.7) | 52.5 (14.9) | 0.6422 |
| Tumor location | <0.001 | 0.266 | ||||
| Head/neck | 528 (14) | 80 (7) | 86 (12) | 67 (9) | ||
| Trunk | 1579 (41) | 473 (44) | 300 (42) | 307 (43) | ||
| Extremities (upper and lower) | 1725 (45) | 518 (48) | 333 (46) | 345 (48) | ||
| Log tumor thickness. median (p25–p75) | −0.7 (−0.9–−0.4) | −0.2 (−0.5–−0.1) | <0.001 | −0.4 (−0.6–−0.2) | −0.7 (−0.3–−0.1) | 0.063 |
| Histologic subtype | <0.001 | 0.623 | ||||
| Superficial spreading melanoma | 3293 (84) | 871 (81) | 578 (80) | 592 (82) | ||
| Nodular melanoma | 45 (1) | 54 (5) | 23 (3) | 22 (3) | ||
| Other | 588 (15) | 145 (14) | 118 (16) | 105 (15) | ||
| Ulceration | <0.001 | 0.368 | ||||
| No | 3467 (99) | 890 (90) | 673 (94) | 681 (95) | ||
| Yes | 50 (1) | 100 (10) | 46 (6) | 38 (5) | ||
| Regression | <0.001 | 0.872 | ||||
| No | 2422 (74) | 494 (55) | 425 (59) | 428 (60) | ||
| Yes | 845 (26) | 399 (45) | 294 (41) | 291 (40) | ||
| Microscopic satellite | 0.1265 | 1.000 | ||||
| No | 1529 (100) | 584 (99) | 710 (99) | 711 (99) | ||
| Yes | 4 (0) | 5 (1) | 9 (1) | 8 (1) | ||
| Tumor infiltrating lymphocytes | 0.5505 | 0.473 | ||||
| No | 272 (27) | 67 (27) | 192 (27) | 175 (24) | ||
| Non-brisk | 580 (57) | 134 (54) | 377 (52) | 399 (55) | ||
| Brisk | 169 (17) | 48 (19) | 150 (21) | 145 (20) | ||
| Vascular invasion | 0.744 | 0.803 | ||||
| No | 1655 (100) | 608 (99) | 712 (99) | 710 (99) | ||
| Yes | 8 (0) | 4 (1) | 7 (1) | 9 (1) | ||
| Interferon treatment | <0.001 | 0.358 | ||||
| No | 2361 (99) | 738 (95) | 700 (97) | 694 (97) | ||
| Yes | 20 (1) | 37 (5) | 19 (3) | 25 (3) | ||
| Clark level | <0.001 | 0.838 | ||||
| I-III | 2897 (94) | 755 (74) | 588 (82) | 585 (81) | ||
| IV | 184 (6) | 263 (26) | 131 (18) | 134 (19) | ||
| Mitotic rate (mitoses/mm2) | <0.001 | 0.991 | ||||
| 0 | 1491 (82) | 248 (34) | 341 (47) | 339 (47) | ||
| 1 | 225 (12) | 282 (39) | 247 (34) | 252 (35) | ||
| 2 | 55 (3) | 116 (16) | 84 (12) | 81 (11) | ||
| ≥3 | 49 (3) | 82 (11) | 47 (7) | 47 (7) | ||
| Crude Univariate Analysis | Adjusted Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI LL | 95% CI UL | p-Value | HR | 95% CI LL | 95% CI UL | p-Value | ||
| SLNB | SLNB | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 0.96 | 0.53 | 1.73 | 0.884 | Yes | 0.84 | 0.45 | 1.56 | 0.575 |
| Year | |||||||||
| ≤2000 | Ref | - | - | - | |||||
| 2001–2006 | 0.73 | 0.35 | 1.54 | 0.410 | |||||
| 2007–2011 | 0.98 | 0.42 | 2.27 | 0.958 | |||||
| 2012–2017 | 0.67 | 0.18 | 2.54 | 0.558 | |||||
| Hospital | |||||||||
| Salamanca | Ref | - | - | - | |||||
| Valencia IVO | 0.54 | 0.07 | 4.29 | 0.562 | |||||
| Turin | 0.48 | 0.06 | 3.74 | 0.487 | |||||
| Barcelona | 0.74 | 0.10 | 5.71 | 0.772 | |||||
| Badalona | 0.39 | 0.05 | 3.22 | 0.379 | |||||
| Coimbra | NA | ||||||||
| A Coruña | 0.25 | 0.02 | 4.01 | 0.328 | |||||
| Sevilla | NA | ||||||||
| Valencia La Fe | NA | ||||||||
| Sex | |||||||||
| Male | Ref | - | - | - | |||||
| Female | 0.57 | 0.31 | 1.02 | 0.057 | |||||
| Age | 1.02 | 1.00 | 1.04 | 0.076 | Age | 1.03 | 1.01 | 1.05 | 0.011 |
| Log age | 1.98 | 0.73 | 5.34 | 0.18 | |||||
| Tumor location | |||||||||
| Head/neck | Ref | - | - | - | |||||
| Trunk | 1.39 | 0.48 | 4.02 | 0.541 | |||||
| Extremities (upper and lower) | 0.85 | 0.29 | 2.53 | 0.771 | |||||
| Tumor thickness | 13.71 | 2.68 | 69.96 | 0.002 | |||||
| Log tumor thickness | 4.76 | 1.56 | 14.51 | 0.006 | Log tumor thickness | 3.82 | 1.23 | 11.81 | 0.020 |
| Histologic subtype | |||||||||
| Superficial spreading melanoma | Ref | - | - | - | |||||
| Nodular melanoma | 4.10 | 1.59 | 10.62 | 0.004 | |||||
| Other | 1.94 | 0.92 | 4.08 | 0.082 | |||||
| Ulceration | Ulceration | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 3.23 | 1.43 | 7.28 | 0.005 | Yes | 2.66 | 1.11 | 6.38 | 0.028 |
| Regression | |||||||||
| No | Ref | - | - | - | |||||
| Yes | 0.97 | 0.50 | 1.89 | 0.922 | |||||
| Microscopic satellite | |||||||||
| No | Ref | - | - | - | |||||
| Yes | 5.41 | 0.72 | 40.51 | 0.098 | |||||
| Tumor infiltrating lymphocytes | |||||||||
| 1 | Ref | - | - | - | |||||
| 2 | 0.90 | 0.41 | 1.98 | 0.787 | |||||
| 3 | 0.62 | 0.14 | 2.67 | 0.517 | |||||
| Vascular invasion | |||||||||
| No | Ref | - | - | - | |||||
| Yes | NA | ||||||||
| Interferon | Interferon | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 7.70 | 3.45 | 17.19 | 0.000 | Yes | 7.29 | 2.94 | 18.06 | 0.000 |
| Clark level | |||||||||
| I-II-III | Ref | - | - | - | |||||
| IV | 1.92 | 0.93 | 3.95 | 0.076 | |||||
| Mitotic rate | |||||||||
| 0 | Ref | - | - | - | |||||
| 1 | 1.67 | 0.66 | 4.20 | 0.276 | |||||
| 2 | 2.28 | 0.63 | 8.20 | 0.204 | |||||
| ≥3 | 4.16 | 1.34 | 12.89 | 0.014 | |||||
| Crude Univariate Analysis | Adjusted Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI LL | 95% CI UL | p-Value | HR | 95% CI LL | 95% CI UL | p-Value | ||
| SLNB | SLNB | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 1.11 | 0.72 | 1.73 | 0.634 | Yes | 0.84 | 0.49 | 1.43 | 0.509 |
| Year | |||||||||
| ≤2000 | Ref | - | - | - | |||||
| 2001–2006 | 0.67 | 0.39 | 1.15 | 0.142 | |||||
| 2007–2011 | 0.62 | 0.34 | 1.14 | 0.124 | |||||
| 2012–2017 | 0.42 | 0.17 | 1.07 | 0.068 | |||||
| Hospital | |||||||||
| Salamanca | Ref | - | - | - | |||||
| Valencia IVO | 1.34 | 0.18 | 10.01 | 0.776 | |||||
| Turin | 1.25 | 0.17 | 9.21 | 0.829 | |||||
| Barcelona | 1.32 | 0.18 | 9.89 | 0.785 | |||||
| Badalona | 0.58 | 0.07 | 4.64 | 0.606 | |||||
| Coimbra | NA | ||||||||
| A Coruña | 0.50 | 0.05 | 5.53 | 0.573 | |||||
| Sevilla | NA | ||||||||
| Valencia La Fe | 0.95 | 0.06 | 15.16 | 0.970 | |||||
| Gender | |||||||||
| Male | Ref | - | - | - | |||||
| Female | 0.73 | 0.47 | 1.12 | 0.152 | |||||
| Age | 1.02 | 1.01 | 1.04 | 0.006 | Age | 1.03 | 1.01 | 1.04 | 0.003 |
| Log Age | 2.47 | 1.17 | 5.23 | 0.018 | |||||
| Localization | |||||||||
| Head/Neck | Ref | - | - | - | |||||
| Trunk | 0.95 | 0.44 | 2.07 | 0.907 | |||||
| Extremities (upper and lower) | 1.02 | 0.48 | 2.17 | 0.965 | |||||
| Tumor thickness | 7.32 | 2.33 | 23.06 | 0.001 | |||||
| Log tumor thickness | 3.03 | 1.43 | 6.40 | 0.004 | |||||
| Histologic subtype | Histologic subtype | ||||||||
| Superficial spreading melanoma | Ref | - | - | - | Superficial spreading melanoma | Ref | - | - | - |
| Nodular melanoma | 5.40 | 2.73 | 10.67 | 0.000 | Nodular melanoma | 1.58 | 0.56 | 4.47 | 0.389 |
| Others | 2.36 | 1.39 | 4.01 | 0.001 | Others | 2.51 | 1.36 | 4.63 | 0.003 |
| Ulceration | Ulceration | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 4.14 | 2.34 | 7.33 | 0.000 | Yes | 3.06 | 1.40 | 6.70 | 0.005 |
| Regression | |||||||||
| No | Ref | - | - | - | |||||
| Yes | 0.69 | 0.41 | 1.16 | 0.161 | |||||
| Microscopic satellite | |||||||||
| No | Ref | - | - | - | |||||
| Yes | 5.54 | 1.15 | 26.58 | 0.033 | |||||
| Tumor infiltrating lymphocytes | |||||||||
| No | Ref | - | - | - | |||||
| Non-brisk | 1.02 | 0.53 | 1.94 | 0.960 | |||||
| Brisk | 0.91 | 0.28 | 2.94 | 0.873 | |||||
| Vascular invasion | |||||||||
| No | Ref | - | - | - | |||||
| Yes | NA | ||||||||
| Interferon | Interferon treatment | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 10.80 | 5.97 | 19.52 | 0.000 | Yes | 15.12 | 7.36 | 31.07 | 0.000 |
| Clark level | Clark level | ||||||||
| I-II-III | Ref | - | - | - | I-II-III | Ref | - | - | - |
| IV | 2.17 | 1.30 | 3.61 | 0.003 | IV | 2.38 | 1.35 | 4.18 | 0.003 |
| Mitotic rate | Mitotic rate | ||||||||
| 0 | Ref | - | - | - | 0 | Ref | - | - | - |
| 1 | 1.72 | 0.85 | 3.50 | 0.131 | 1 | 2.03 | 0.93 | 4.42 | 0.074 |
| 2 | 3.06 | 1.26 | 7.44 | 0.014 | 2 | 3.08 | 1.15 | 8.21 | 0.025 |
| ≥3 | 7.30 | 3.38 | 15.78 | 0.000 | 3 or more | 7.66 | 3.02 | 19.45 | 0.000 |
| Crude Univariate Analysis | Adjusted Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | LL 95%CI | UL 95%CI | p-Value | HR | LL 95%CI | UL 95%CI | p-Value | ||
| SLNB | SLNB | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 0.74 | 0.46 | 1.19 | 0.211 | Yes | 0.61 | 0.37 | 1.00 | 0.050 |
| Year | |||||||||
| ≤2000 | Ref | - | - | - | |||||
| 2001–2006 | 1.06 | 0.56 | 1.99 | 0.857 | |||||
| 2007–2011 | 1.15 | 0.56 | 2.36 | 0.710 | |||||
| 2012–2017 | 1.69 | 0.71 | 4.02 | 0.236 | |||||
| Hospital | |||||||||
| Salamanca | Ref | - | - | - | |||||
| Valencia IVO | 0.97 | 0.13 | 7.37 | 0.980 | |||||
| Turin | 0.47 | 0.06 | 3.62 | 0.468 | |||||
| Barcelona | 1.11 | 0.15 | 8.32 | 0.922 | |||||
| Badalona | 0.93 | 0.12 | 7.10 | 0.944 | |||||
| Coimbra | 3.29 | 0.20 | 53.37 | 0.402 | |||||
| A Coruña | 1.25 | 0.15 | 10.71 | 0.838 | |||||
| Sevilla | 0.66 | 0.06 | 7.34 | 0.738 | |||||
| Valencia La Fe | NA | ||||||||
| Sex | Sex | ||||||||
| Male | Ref | - | - | - | Male | Ref | - | - | - |
| Female | 0.41 | 0.25 | 0.67 | 0.000 | Female | 0.48 | 0.29 | 0.79 | 0.004 |
| Age | 1.05 | 1.04 | 1.07 | 0.000 | Age | 1.05 | 1.03 | 1.07 | 0.000 |
| Log age | 10.71 | 4.15 | 27.62 | 0.000 | |||||
| Tumor location | |||||||||
| Head/neck | Ref | - | - | - | |||||
| Trunk | 0.84 | 0.40 | 1.75 | 0.646 | |||||
| Extremities (upper and lower) | 0.68 | 0.33 | 1.41 | 0.302 | |||||
| Tumor thickness | 4.47 | 1.40 | 14.33 | 0.012 | |||||
| Log tumor thickness | 2.38 | 1.12 | 5.03 | 0.023 | |||||
| Histologic subtype | |||||||||
| Superficial spreading melanoma | Ref | - | - | - | |||||
| Nodular melanoma | 2.36 | 0.94 | 5.94 | 0.068 | |||||
| Other | 1.52 | 0.83 | 2.79 | 0.177 | |||||
| Ulceration | Ulceration | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 2.75 | 1.41 | 5.38 | 0.003 | Yes | 2.58 | 1.25 | 5.34 | 0.011 |
| Regression | |||||||||
| No | Ref | - | - | - | |||||
| Yes | 1.32 | 0.81 | 2.18 | 0.267 | |||||
| Microscopic satellite | |||||||||
| No | Ref | - | - | - | |||||
| Yes | 3.43 | 0.51 | 23.23 | 0.202 | |||||
| Tumor infiltrating lymphocytes | |||||||||
| No | Ref | - | - | - | |||||
| Non-Brisk | 0.73 | 0.38 | 1.41 | 0.343 | |||||
| Brisk | 0.49 | 0.15 | 1.68 | 0.254 | |||||
| Vascular invasion | |||||||||
| No | Ref | - | - | - | |||||
| Yes | NA | ||||||||
| Interferon treatment | Interferon treatment | ||||||||
| No | Ref | - | - | - | No | Ref | - | - | - |
| Yes | 4.28 | 2.02 | 9.05 | 0.000 | Yes | 5.69 | 2.43 | 13.31 | 0.000 |
| Clark level | Clark level | ||||||||
| I-II-III | Ref | - | - | - | I-II-III | Ref | - | - | - |
| IV | 2.00 | 1.15 | 3.45 | 0.014 | IV | 1.86 | 1.06 | 3.27 | 0.031 |
| Mitotic rate | |||||||||
| 0 | Ref | - | - | - | |||||
| 1 | 1.57 | 0.80 | 3.09 | 0.190 | |||||
| 2 | 1.91 | 0.75 | 4.89 | 0.176 | |||||
| ≥3 | 2.61 | 1.04 | 6.54 | 0.041 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tejera-Vaquerizo, A.; Boada, A.; Ribero, S.; Puig, S.; Paradela, S.; Moreno-Ramírez, D.; Cañueto, J.; de Unamuno-Bustos, B.; Brinca, A.; Descalzo-Gallego, M.A.; et al. Sentinel Lymph Node Biopsy vs. Observation in Thin Melanoma: A Multicenter Propensity Score Matching Study. J. Clin. Med. 2021, 10, 5878. https://doi.org/10.3390/jcm10245878
Tejera-Vaquerizo A, Boada A, Ribero S, Puig S, Paradela S, Moreno-Ramírez D, Cañueto J, de Unamuno-Bustos B, Brinca A, Descalzo-Gallego MA, et al. Sentinel Lymph Node Biopsy vs. Observation in Thin Melanoma: A Multicenter Propensity Score Matching Study. Journal of Clinical Medicine. 2021; 10(24):5878. https://doi.org/10.3390/jcm10245878
Chicago/Turabian StyleTejera-Vaquerizo, Antonio, Aram Boada, Simone Ribero, Susana Puig, Sabela Paradela, David Moreno-Ramírez, Javier Cañueto, Blanca de Unamuno-Bustos, Ana Brinca, Miguel A. Descalzo-Gallego, and et al. 2021. "Sentinel Lymph Node Biopsy vs. Observation in Thin Melanoma: A Multicenter Propensity Score Matching Study" Journal of Clinical Medicine 10, no. 24: 5878. https://doi.org/10.3390/jcm10245878
APA StyleTejera-Vaquerizo, A., Boada, A., Ribero, S., Puig, S., Paradela, S., Moreno-Ramírez, D., Cañueto, J., de Unamuno-Bustos, B., Brinca, A., Descalzo-Gallego, M. A., Osella-Abate, S., Cassoni, P., Podlipnik, S., Carrera, C., Vidal-Sicart, S., Pigem, R., Toll, A., Rull, R., Alos, L., ... Nagore, E. (2021). Sentinel Lymph Node Biopsy vs. Observation in Thin Melanoma: A Multicenter Propensity Score Matching Study. Journal of Clinical Medicine, 10(24), 5878. https://doi.org/10.3390/jcm10245878