1. Introduction
Because intradialytic hypotension can lead to superimposed organ hypoperfusion and ultimately mitigate long-term kidney outcomes after acute kidney injury, it remains a concern in critically ill patients requiring kidney replacement therapy. Intradialytic hypotension results from an inadequate compensatory response (heart rate, myocardial contractility, vascular tone and splanchnic flow shifts) to ultrafiltration rate, cardiac output decrease and/or arterial tonus changes during the session [
1].
Dialysate composition may influence hemodynamic tolerance of intermittent hemodialysis (IHD) performed in the ICU [
2,
3]. Usual IHD techniques use bicarbonate-rich dialysate (B-IHD) but require acidification of the dialysate with acetate, citrate or hydrochloric acid to avoid calcium carbonatation within the dialysis filter. Beyond the direct effect of acetate on cardiac contractility and vascular tone, dialysate acidification by itself may also lead to systemic vascular effects, including on the pulmonary vascular bed, due to the release of high amounts of carbon dioxide in the blood outflow, whatever the acid used [
4]. Thus, there is an unmet need to optimize tolerance of IHD, especially in critically ill patients, and modulating dialysate may reduce the rate of intradialytic hypotension.
Acetate-free biofiltration (AFB) is an alternative technique of IHD based on a bicarbonate-free dialysate (thus without the need for dialysate acidification) with post-filter reinjection of sodium bicarbonate. Few studies suggested that AFB may be better tolerated than B-IHD in patients receiving chronic dialysis [
5], but results in acute kidney injury remain elusive [
6]. Whether the potential beneficial hemodynamic effects of AFB may translate to critically ill patients remains to be established. In addition, recent studies in rats and in sheep suggested that hemodialysis with bicarbonate-free dialysate may be used as a platform of carbon dioxide removal to treat hypercapnic acidosis [
7,
8].
This report describes our findings of hemodynamic and metabolic outcomes in mechanically ventilated patients receiving dialysis with AFB or B-IHD.
2. Methods
Between February 2020 and March 2021, we prospectively included patients admitted to the ICU and receiving mechanical ventilation, who had intermittent sessions of hemodialysis.
B-IHD and AFB were performed with the Citrasate (Hemotech®, Toulouse, France) and Safebag (Hospal®, Meyzieu, France) dialysates, respectively. Sodium conductivity was 13.5 to 13.7 mSv. Membranes were the Elisio 21H (Nipro®, Cournon, France) or Evodial (Baxter®, Guyancourt, France) polyethersulfone filters. AFB dialysate composition was the following: sodium 140 mmol/L, chloride 146 mmol/L, calcium 1.5 mmol/L, magnesium 0.5 mmol/L, glucose 5.5 mmol/L, potassium 3.5 mmol/L (sodium conductivity was settled at 13.5 to 13.7 mS/cm). Solution of sodium bicarbonate that was reinjected had a concentration of 167 mmol/L. B-IHD dialysate composition was the following: sodium 140, chloride 108 mmol/L, potassium 3 mmol/L, calcium 1.65 mmol/L, magnesium 0.5 mmol/L, citrate 0.8 mmol/L, and glucose 1 g/L (sodium conductivity was settled at 14–14.5 mS/cm). Dialysate temperature was 1 °C below the patient temperature. Blood flow was settled 250 to 300 mL/min.
Characteristics of the patients were collected from their digitized medical charts. Blood pressures were measured using an arterial catheter. Intradialytic hypotension was diagnosed according to the KDOQI clinical practice guidelines (i.e., decrease in systolic blood pressure ≥ 20 mmHg or decrease in mean arterial pressure ≥ 10 mmHg) [
9]. In addition, episodes of systolic blood pressure decrease below 95 mmHg were recorded. Hemodynamic parameters (systolic, diastolic and mean blood pressure, as well as heart rate and dose of norepinephrine) were collected each 30 min.
In a subset of AFB and B-IHD sessions, blood gases were measured before and after the filter for B-IHD, or before and after the filter and after the bicarbonate reinjection for AFB. The global CO2 load induced by dialysis sessions was approximated with the following formula: CO2 load = [total inflow CO2 content minus total outflow CO2 content] × blood flow × time.
Continuous variables were given as mean ± SEM and compared with the Mann–Whitney test. Discontinuous variables were given as number (percentages) and compared with Fisher’s exact test, after adjustment on the use of vasoactive agent at baseline. Hemodynamic parameters of AFB and B-IHD sessions were compared with a two-way ANOVA test with mixed-effects.
All patients included in this study gave informed consent. This study was conducted according to the Best Clinical Practices guidelines and the Declaration of Helsinki, as revised in 2004, and approved by the French national ethics committee (COOBRA study no. ID-RCB 2019-A03261-56).
3. Results
We included 49 mechanically ventilated patients (mean age 65 ± 12 years), who received 4 h sessions of AFB (
n = 66) or B-IHD (
n = 62) (
Table 1). The mean volume of ultrafiltration prescribed was similar in both groups (1.8 ± 0.8 vs. 1.8 ± 0.9 L).
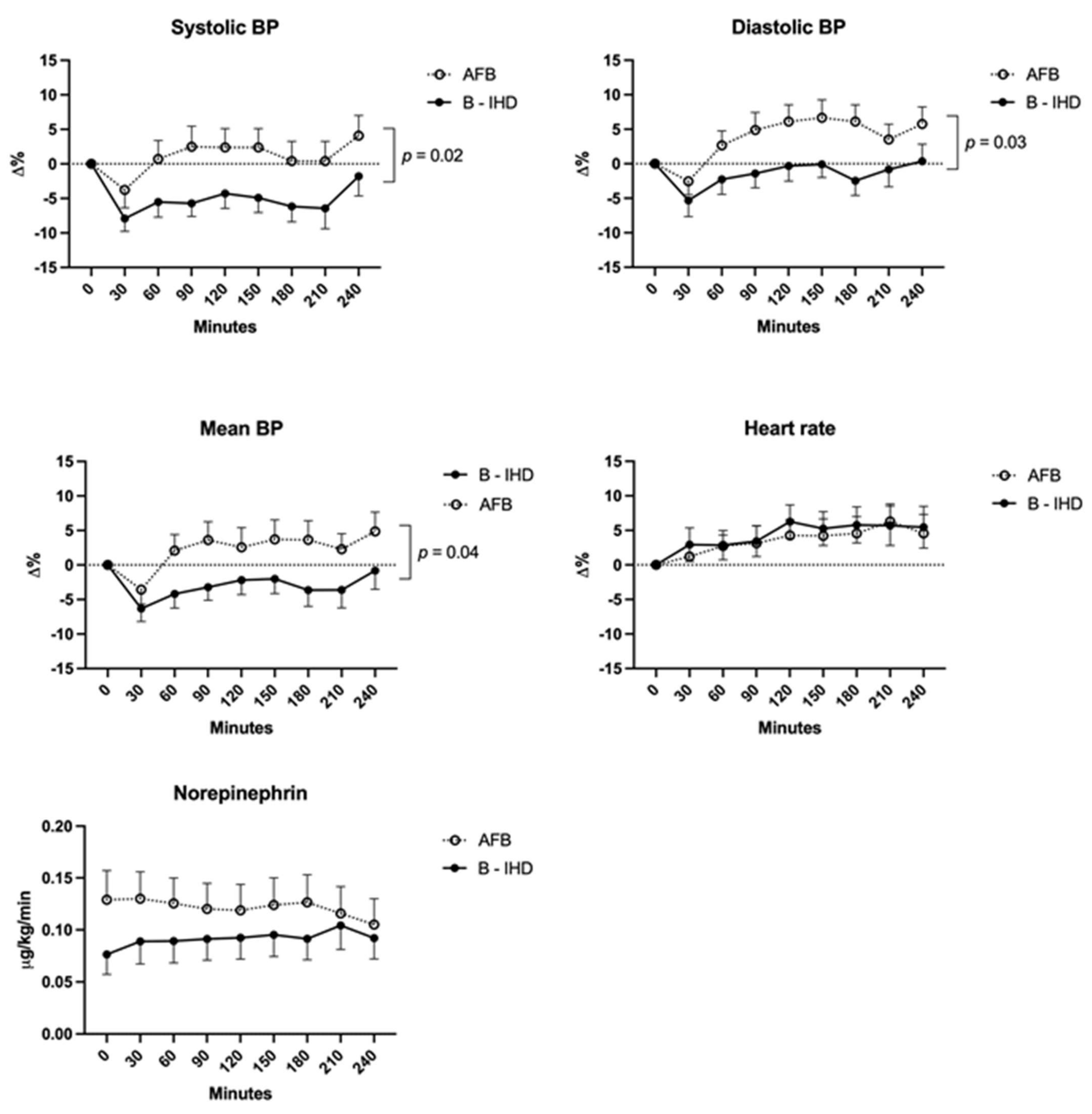
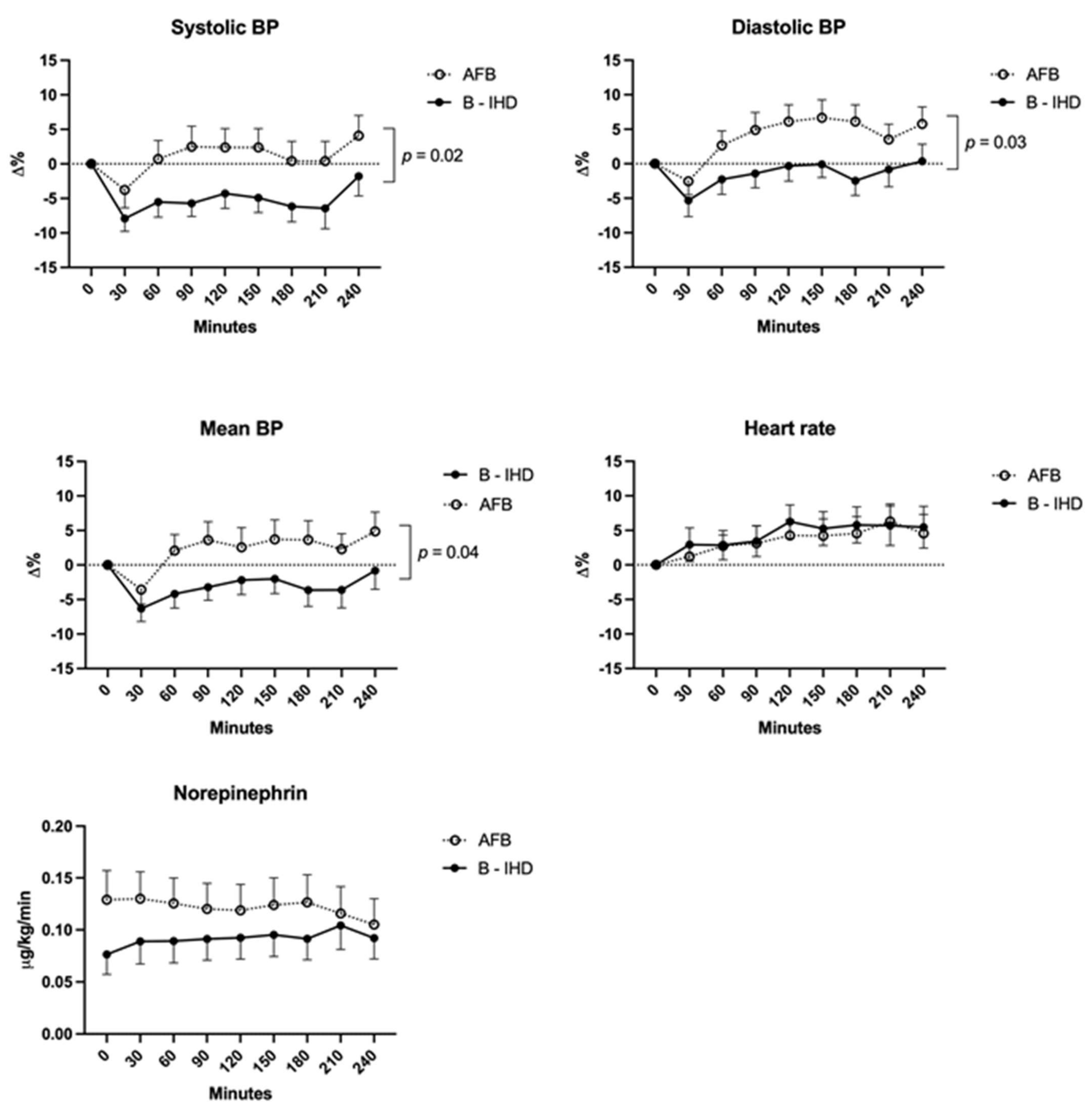
3.1. Hemodynamic Tolerance
Whereas more AFB sessions were performed in patients of male gender (89 vs. 67%,
p = 0.002), with underlying chronic obstructive broncho-pneumopathy (41 vs. 19%,
p = 0.007), admitted for sepsis (70 vs. 48%,
p = 0.02) or with ongoing vasoactive support (67 vs. 47%,
p = 0.03), episodes of intradialytic hypotension were significantly less frequent during AFB compared to B-IHD, whatever the classification used (decrease in mean blood pressure ≥ 10 mmHg: 36/66 (54%) vs. 46/62 (74%) sessions,
p-value = 0.02; systolic blood pressure decrease >20 mmHg: 27/66 (41%) vs. 40/62 (64%) sessions,
p-value = 0.007). After the adjustment on the use of vasoactive agent at the start of the session, an episode of systolic blood pressure decrease below 95 mmHg was more frequent during dialysis sessions with B-IHD (25/62 (40%)) compared to AFB (16/66 (24%); adjusted
p-value 0.03). Hemodynamic monitoring showed significantly better global tolerance of AFB sessions owing to increased diastolic blood pressure and stable systolic blood pressure, without concomitant increase in norepinephrine (
Figure 1).
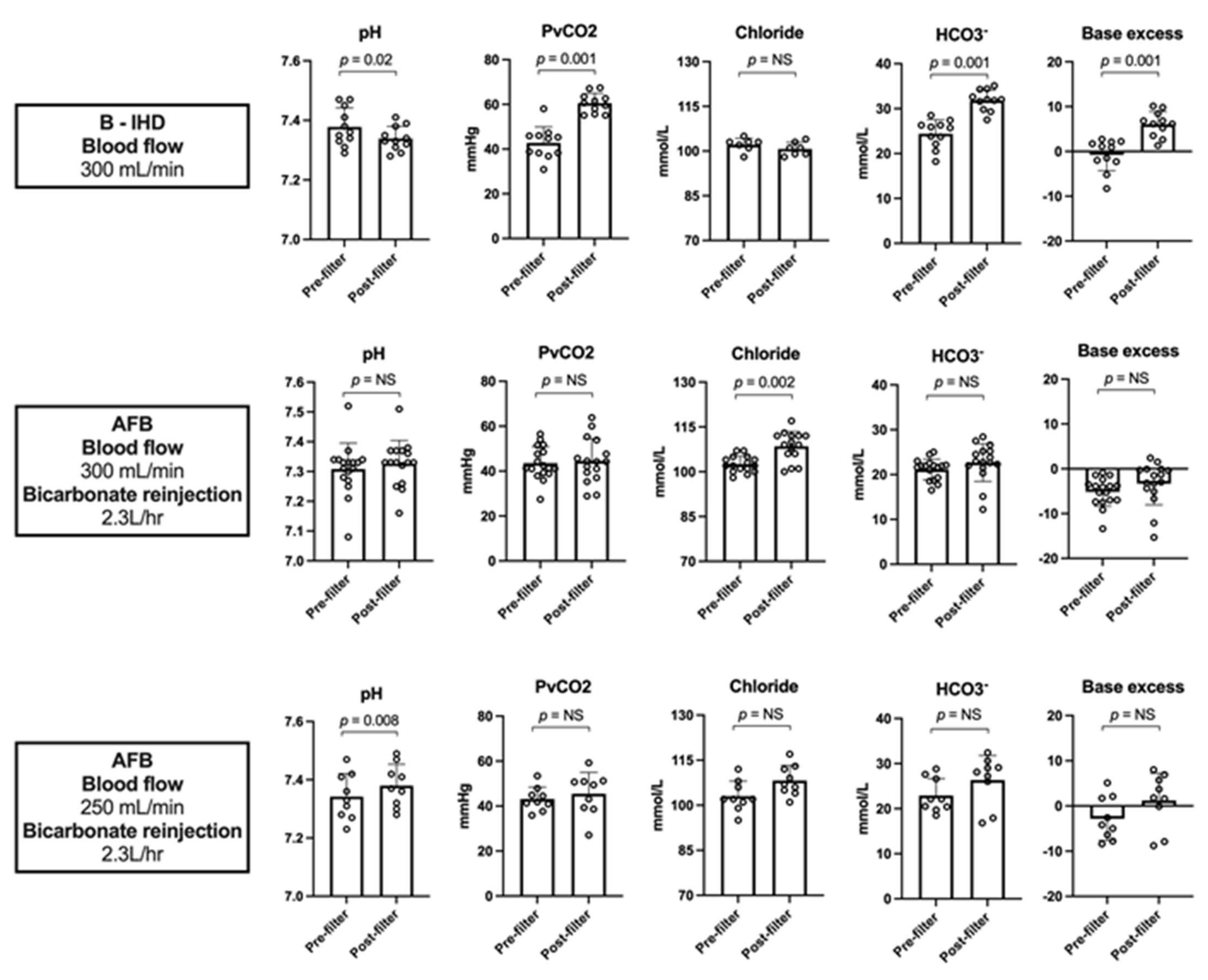
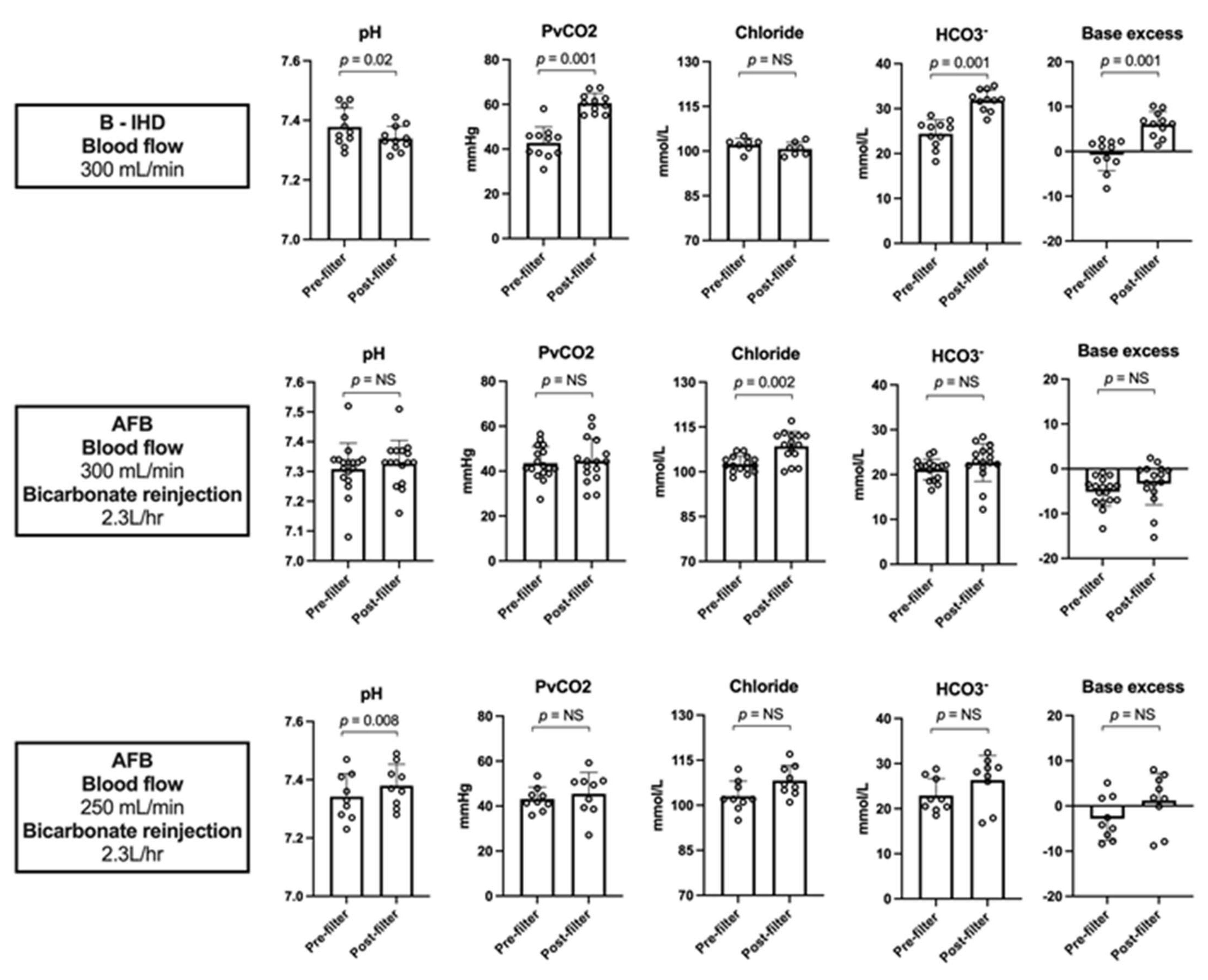
3.2. Carbon Dioxide Loading during Dialysis
In AFB sessions, optimal control of the acid-base status was obtained with a bicarbonate reinjection rate of 2.3 L/h with a blood flow of 250 mL/min (end dialysis: base excess 0.5 ± 2.6; chloride 104 ± 0.6 mmol/L), compared to 2.3 L/h and 300 mL/min, respectively (end dialysis: base excess −2.7 ± 4.6; chloride 106 ± 1.3 mmol/L).
Blood gases after the dialysis filter showed the respective metabolic impact of B-IHD and AFB: PvCO
2, bicarbonate concentration and pH in blood returning to the patients were 60 ± 4.4 mmHg, 32 ± 2.3 mmol/L and 7.34 ± 0.04 compared to 45 ± 9.6 mmHg [
p < 0.001], 24 ± 4.9 mmHg [pH < 0.001] and 7.35 ± 0.07 [
p = 0.79], respectively (
Figure 2).
Last, we estimated the net balance of CO2 induced by both techniques and the ability of dialysis with low-bicarbonate dialysate to be used as a platform for CO2 extraction. The blood exiting the AFB filter (before bicarbonate reinjection) was characterized by very low concentration of bicarbonate and partial pressure of CO2, leading to a decrease in the total CO2 content from 23 ± 3.3 to 5.2 ± 2.6 mmol/L (mean CO2 removal: 113 ± 25 mL/min). The global CO2 load (i.e., total CO2 content changes) induced by AFB sessions was +25 ± 6 compared to +80 ± 12 mL/min with B-IHD (Hodges-Lehmann difference −51.2 mL/min, p = 0.0002).
4. Discussion
In this study, we showed that hemodynamic tolerance was better in mechanically ventilated critically ill patients receiving AFB compared to conventional B-IHD, despite higher vasoactive support at the start of AFB sessions. This held true that the tolerance was assessed using the K/DOQI classification or the quantitative assessment of hemodynamic parameters. Because other dialysis and patient characteristics were balanced between the two groups or in favor of B-IHD, the discrepancies between the contents of the blood that returns to the patients during AFB and B-IHD probably account for the divergent hemodynamic tolerance. We first hypothesized that large amounts of CO
2 in blood outflow during B-IHD may activate circulating inflammatory cells [
10,
11] and increase systemic inflammation with a subsequent decrease in the vascular tone. As an alternative hypothesis, the euhydric hypercapnic blood (i.e., high PvCO
2, high bicarbonate levels, normal pH) that returns to the patient during B-IHD may modulate the vascular tone of the pulmonary artery [
12,
13,
14] and subsequently alter the heart response during dialysis. These should be tested in further comparative studies in human or animal experiments.
Last, we confirmed in humans the potential of dialysis with low-bicarbonate dialysate to remove CO
2 [
7]. We first showed confirmed that the CO
2 load was significantly reduced during AFB sessions compared to B-IHD sessions. This may be of utmost interest in patients at risk to develop hypercapnic acidosis (for instance, with chronic obstructive pulmonary disease or severe asthma) but also at risk of hypercapnia-induced high intracranial pressure. Second, we report a case of COVID-19-related acute respiratory distress syndrome complicated by refractory hypercapnia and core pulmonal successfully reversed by AFB. Even if the development of customized “balanced” dialysates with low chloride concentrations and no bicarbonate will be helpful in developing true “respiratory dialysis” [
7], AFB may be already tested in cases of refractory hypercapnic conditions, as salvage therapy.
This study has some limitations, mainly related to its uncontrolled design. First, the risk factors of hemodialysis intolerance were not balanced between the two groups, but these risk factors were more frequent in the AFB sessions group. The positive results in favor of AFB we observed thus reinforce its probable superiority. Secondly, at baseline, hemodynamic status of patients was heterogeneous. Further comparative randomized studies are thus required to confirm our results, especially in patients with vasoactive support (i.e., with the highest risk to develop hypotension during sessions). Last, the mechanisms by which tolerance of AFB is superior to B-IHD still remain elusive and will require additional studies in humans or in animals.
5. Conclusions
We showed that AFB is safe in critically ill patients. Notwithstanding the non-controlled design of this study and its potential biases, our findings suggest that hemodynamic tolerance of AFB is superior to B-IHD in mechanically ventilated patients. If confirmed, it may reduce superimposed artificial kidney-induced kidney injuries and improve long-term kidney outcomes. Its use as a platform for CO2 removal also warrants further research.
Author Contributions
O.C. and S.F. designed the study; A.G., P.T., O.M., C.M., B.S., M.-B.N., L.L., N.K., O.C. and S.F. followed the patients; A.G., P.T. and S.F. collected the data; S.F. performed the statistical analyses; S.F., O.C. and N.K. wrote the manuscript; all the authors approved the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the French national ethics committee (COOBRA study no. ID-RCB 2019-A03261-56).
Informed Consent Statement
According to the recommendations of the Ethical Committee, patients gave oral informed consent to be included in the study.
Data Availability Statement
The data that support the findings of this study are available from S.F. but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of S.F.
Acknowledgments
We greatly acknowledge Arnaud Mari (Centre Hospitalier de Saint-Brieuc, France) for his helpful discussion of the study.
Conflicts of Interest
No authors had competing interests within the field of this study.
References
- Douvris, A.; Zeid, K.; Hiremath, S.; Bagshaw, S.M.; Wald, R.; Beaubien-Souligny, W.; Kong, J.; Ronco, C.; Clark, E.G. Mechanisms for hemodynamic instability related to renal replacement therapy: A narrative review. Intensive Care Med. 2019, 45, 1333–1346. [Google Scholar] [CrossRef] [Green Version]
- Schortgen, F.; Soubrier, N.; Delclaux, C.; Thuong, M.; Girou, E.; Brun-Buisson, C.; Lemaire, F.; Brochard, L. Hemodynamic tolerance of intermittent hemodialysis in critically ill patients: Usefulness of practice guidelines. Am. J. Respir. Crit. Care Med. 2000, 162, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Vanherweghem, J.L.; Degaute, J.P.; Berré, J.; Dufaye, P.; Kahn, R.J. Acetate-induced myocardial depression during hemodialysis for acute renal failure. Kidney Int. 1982, 22, 653–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marano, M.; D’Amato, A.; Cantone, A. Carbon dioxide: Global warning for nephrologists. World J. Nephrol. 2016, 5, 429. [Google Scholar] [CrossRef] [PubMed]
- Tessitore, N.; Santoro, A.; Panzetta, G.O.; Wizemann, V.; Perez-Garcia, R.; Martinez Ara, J.; Perrone, B.; Mantovani, W.; Poli, A. Acetate-free biofiltration reduces intradialytic hypotension: A European multicenter randomized controlled trial. Blood Purif. 2013, 34, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Bret, M.; Hurot, J.M.; Mercatello, A.; Coronel, B.; Dorez, D.; Laville, M.; Moskovtchenko, J.F. Acetate-free biofiltration for acute renal failure. Ren. Fail. 1998, 20, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Cove, M.E.; Vu, L.H.; Ring, T.; Federspiel, W.J.; Kellum, J.A. Respiratory Dialysis—A Novel Low Bicarbonate Dialysate to Provide Extracorporeal CO2 Removal. Crit. Care Med. 2020, 48, e592–e598. [Google Scholar] [CrossRef] [PubMed]
- Vu, L.H.; Kellum, J.A.; Federspiel, W.J.; Cove, M.E. Carbon dioxide removal using low bicarbonate dialysis in rodents. Perfusion 2019, 34, 578–583. [Google Scholar] [CrossRef] [PubMed]
- KD Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am. J. Kidney Dis. 2005, 45, S1–S153. [Google Scholar]
- Thom, S.R.; Bhopale, V.M.; Hu, J.P.; Yang, M. Increased carbon dioxide levels stimulate neutrophils to produce microparticles and activate the nucleotide-binding domain-like receptor 3 inflammasome. Free Radic. Biol. Med. 2017, 106, 406–416. [Google Scholar] [CrossRef] [Green Version]
- Abolhassani, M.; Guais, A.; Chaumet-Riffaud, P.; Sasco, A.J.; Schwartz, L. Carbon dioxide inhalation causes pulmonary inflammation. Am. J. Physiol. Lung Cell. Mol. Physiol. 2009, 296, L657–L665. [Google Scholar] [CrossRef] [Green Version]
- Barer, G.R.; Shaw, J.W. Pulmonary vasodilator and vasoconstrictor actions of carbon dioxide. J. Physiol. 1971, 213, 633–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, I.C.; Dong, H.P.; Yang, R.C.; Wang, T.H.; Tsai, J.H.; Yang, P.H.; Huang, M.S. Effect of carbon dioxide on pulmonary vascular tone at various pulmonary arterial pressure levels induced by endothelin-1. Lung 2010, 188, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Vaňková, M.; Snetkov, V.A.; Knock, G.A.; Aaronson, P.I.; Ward, J.P.T. Euhydric hypercapnia increases vasoreactivity of rat pulmonary arteries via HCO3− transport and depolarisation. Cardiovasc. Res. 2005, 65, 505–512. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}
{kind=link}