
Stage 2: Who Are the Best Candidates for Robotic Gait Training Rehabilitation in Hemiparetic Stroke?

_H._You.png)
Abstract
:1. Introduction
2. Materials and Methods
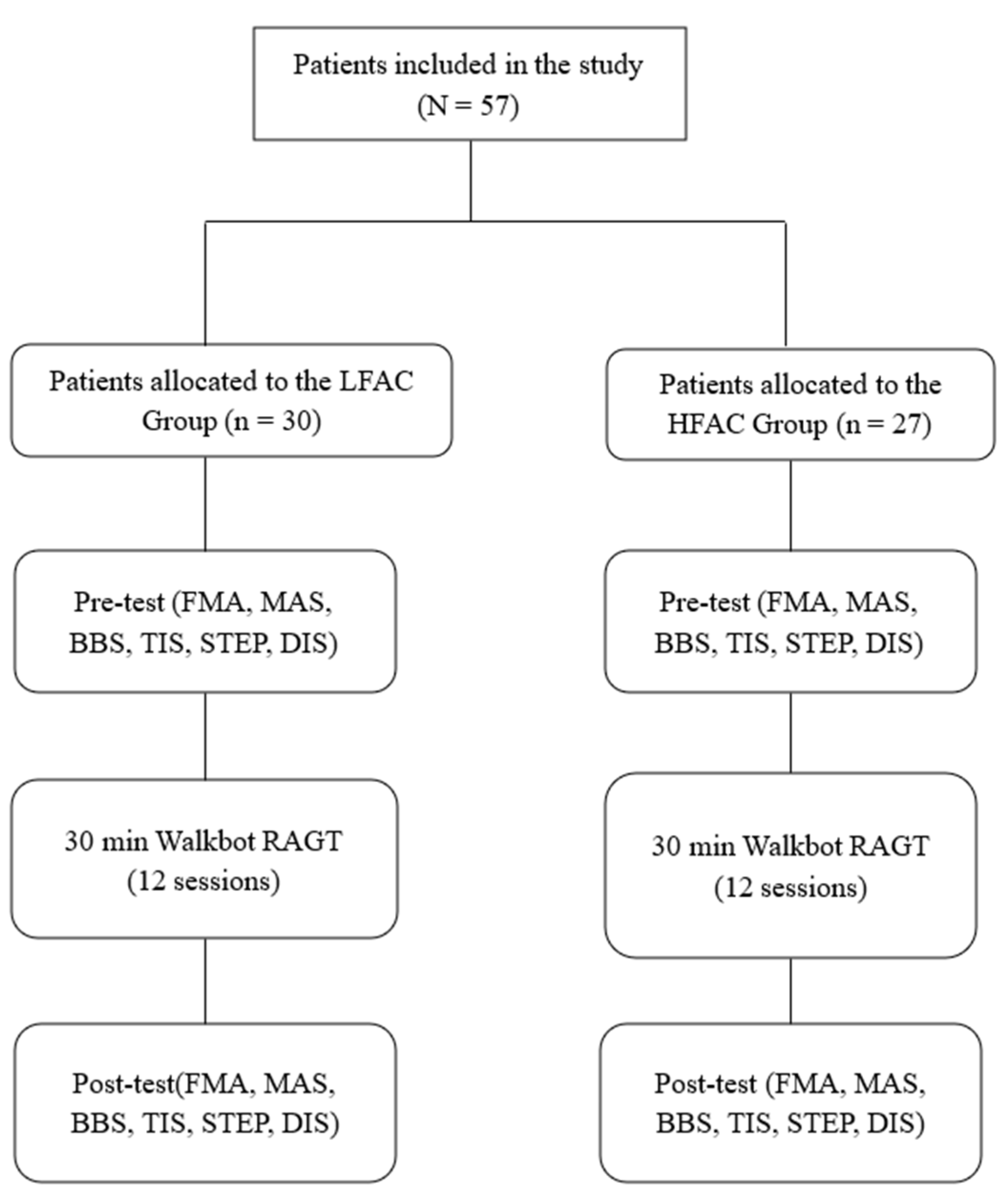
2.1. Patients
2.2. Clinical Outcome Measures
2.2.1. FAC
2.2.2. FMA Scale
2.2.3. MAS
2.2.4. BBS
2.2.5. TIS
2.2.6. Number of Walking Steps and Walking Distance
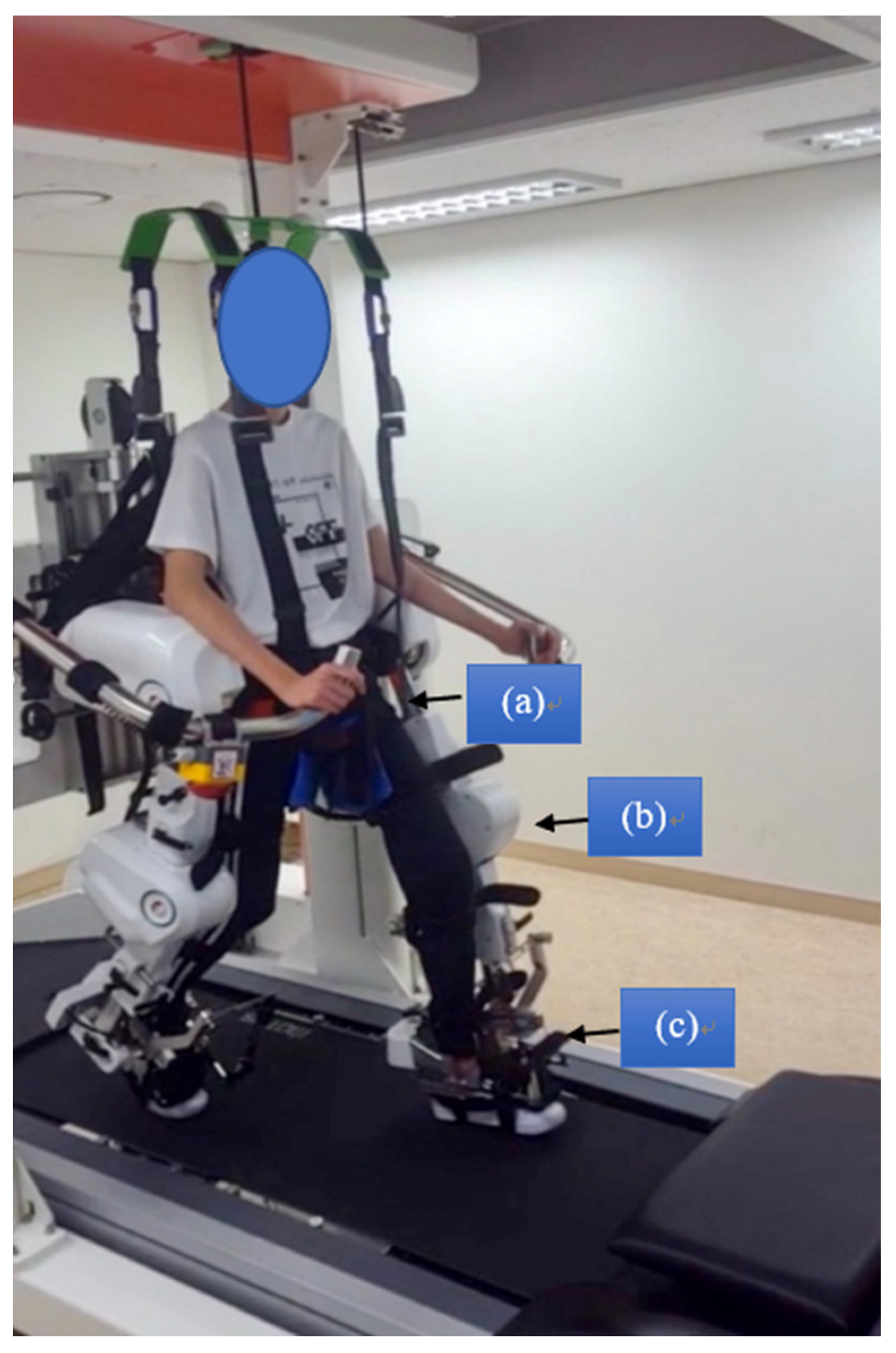
2.3. Intervention
2.4. Statistical Analysis
3. Results
3.1. FMA
3.2. MAS
3.3. BBS
3.4. TIS
3.5. Number of Steps
3.6. Walking Distance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, H.Y.; You, J.S.H. A Review of Robot-Assisted Gait Training in Stroke Patients. Brain Neurorehabilit 2017, 10, e9. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.Y.; Park, S.-W.; Lee, M.J.; Park, D.S.; Kim, E.J. Effects of robot-assisted gait training on the balance and gait of chronic stroke patients: Focus on dependent ambulators. J. Phys. Ther. Sci. 2015, 27, 3053–3057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke: A major update of the evidence. Stroke 2017, 48, e188–e189. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-Y.; Yang, L.; Park, I.J.; Kim, E.J.; Park, M.S.; You, S.H.; Kim, Y.-H.; Ko, H.-Y.; Shin, Y.-I. Effects of Innovative WALKBOT Robotic-Assisted Locomotor Training on Balance and Gait Recovery in Hemiparetic Stroke: A Prospective, Randomized, Experimenter Blinded Case Control Study With a Four-Week Follow-Up. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Park, I.J.; Park, J.-H.; Seong, H.Y.; You, S.H.; Kim, S.J.; Min, J.H.; Ko, H.Y.; Shin, Y.-I. Comparative effects of different assistance force during robot-assisted gait training on locomotor functions in patients with subacute stroke: An assessor-blind, randomized controlled trial. Am. J. Phys. Med. Rehabil. 2019, 98, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.G.; Lee, W.H.; Lee, S.H.; Yi, Y.; Kim, K.D.; Oh, B.-M. Robotic-assisted gait training combined with transcranial direct current stimulation in chronic stroke patients: A pilot double-blind, randomized controlled trial. Restor. Neurol. Neurosci. 2017, 35, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Sullivan, K.J.; Behrman, A.L.; Azen, S.P.; Wu, S.S.; Nadeau, S.E.; Dobkin, B.H.; Rose, D.K.; Tilson, J.K.; Cen, S.; et al. Body-Weight–Supported Treadmill Rehabilitation after Stroke. New Engl. J. Med. 2011, 364, 2026–2036. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, I.; Meiner, Z. The influence of locomotor treatment using robotic body-weight-supported treadmill training on rehabilitation outcome of patients suffering from neurological disorders. Harefuah 2013, 152, 166–171. [Google Scholar]
- Park, J.-H.; Shin, Y.-I.; You, J.H.; Park, M.S. Comparative effects of robotic-assisted gait training combined with conventional physical therapy on paretic hip joint stiffness and kinematics between subacute and chronic hemiparetic stroke. NeuroRehabilitation 2018, 42, 181–190. [Google Scholar] [CrossRef]
- Kim, H.; Park, G.; Shin, J.-H.; You, J.H. Neuroplastic effects of end-effector robotic gait training for hemiparetic stroke: A randomised controlled trial. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.; Sajin, A.; Fisher, I.; Neeb, M.; Shochina, M.; Katz-Leurer, M.; Meiner, Z. The Effectiveness of Locomotor Therapy Using Robotic-Assisted Gait Training in Subacute Stroke Patients: A Randomized Controlled Trial. PMR 2009, 1, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Shin, Y.-I.; Joa, K.-L.; Shin, Y.K.; Lee, J.J.; You, S.H. Immediate effect of Walkbot robotic gait training on neuromechanical knee stiffness in spastic hemiplegia: A case report. NeuroRehabilitation 2013, 32, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.E.; Kyeong, S.; Lee, S.H.; Lee, W.-J.; Ha, S.W.; Kim, S.M.; Kang, H.; Lee, W.M.; Kang, C.S.; Kim, D.H. Structural and functional improvements due to robot-assisted gait training in the stroke-injured brain. Neurosci. Lett. 2017, 637, 114–119. [Google Scholar] [CrossRef]
- Kim, Y.-H. Robotic assisted rehabilitation therapy for enhancing gait and motor function after stroke. Precis. Futur. Med. 2019, 3, 103–115. [Google Scholar] [CrossRef]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meiβner, D.; Pohl, M. Predictive Validity and Responsiveness of the Functional Ambulation Category in Hemiparetic Patients After Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer assessment of motor recovery after stroke: A critical review of its meas-urement properties. Neurorehabil. Neural. Repair. 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Gregson, J.M.; Leathley, M.; Moore, A.; Sharma, A.K.; Smith, T.L.; Watkins, C. Reliability of the tone assessment scale and the modified ashworth scale as clinical tools for assessing poststroke spasticity. Arch. Phys. Med. Rehabil. 1999, 80, 1013–1016. [Google Scholar] [CrossRef]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health Rev. Can. Sante Publique 1992, 83, S7–S11. [Google Scholar]
- Fujiwara, T.; Liu, M.; Tsuji, T.; Sonoda, S.; Mizuno, K.; Akaboshi, K.; Hase, K.; Masakado, Y.; Chino, N. Development of a new measure to assess trunk impairment after stroke (trunk impairment scale): Its psychometric properties. Am. J. Phys. Med. Rehabil. 2004, 83, 681–688. [Google Scholar] [CrossRef]
- Chang, S.-H.; TIRR SCI Clinical Exoskeleton Group; Afzal, T.; Berliner, J.; Francisco, G.E. Exoskeleton-assisted gait training to improve gait in individuals with spinal cord injury: A pilot randomized study. Pilot Feasibility Stud. 2018, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.; Shin, Y.; Park, J.-H.; Cha, Y.J.; You, J.H. Effects of Walkbot gait training on kinematics, kinetics, and clinical gait function in paraplegia and quadriplegia. NeuroRehabilitation 2018, 42, 481–489. [Google Scholar] [CrossRef]
- Manganotti, P.; Patuzzo, S.; Cortese, F.; Palermo, A.; Smania, N.; Fiaschi, A. Motor disinhibition in affected and unaffected hemisphere in the early period of recovery after stroke. Clin. Neurophysiol. 2002, 113, 936–943. [Google Scholar] [CrossRef]
- Mustafaoglu, R.; Erhan, B.; Yeldan, I.; Gunduz, B.; Tarakci, E. Does robot-assisted gait training improve mobility, activities of daily living and quality of life in stroke? A sin-gle-blinded, randomized controlled trial. Neurol. Belg. 2020, 120, 335–344. [Google Scholar] [CrossRef]
- Wittenberg, G.F.; Richards, L.G.; Jones-Lush, L.; Roys, S.R.; Gullapalli, R.P.; Yang, S.; Guarino, P.D.; Lo, A.C. Predictors and brain connectivity changes associated with arm motor function improvement from intensive practice in chronic stroke. F1000Research 2016, 5, 2119. [Google Scholar] [CrossRef]
- Park, C.; Park, O.M.; Dohle, C.; Bialek, A.; Friel, K.; Edwards, D.; Krebs, H.I.; You, J.H. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. NeuroRehabilitation 2020, 46, 577–587. [Google Scholar] [CrossRef]
- Chung, B.P.H. Effectiveness of robotic-assisted gait training in stroke rehabilitation: A retrospective matched control study. Hong Kong Physiother. J. 2017, 36, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.Y.; Shin, J.-H.; Yang, S.P.; Shin, M.A.; Lee, S.H. Robot-assisted gait training for balance and lower extremity function in patients with infratentorial stroke: A sin-gle-blinded randomized controlled trial. J. Neuroeng. Rehabil. 2019, 16, 1–12. [Google Scholar] [CrossRef]
- Bang, D.-H.; Shin, W.-S. Effects of robot-assisted gait training on spatiotemporal gait parameters and balance in patients with chronic stroke: A randomized controlled pilot trial. NeuroRehabilitation 2016, 38, 343–349. [Google Scholar] [CrossRef]
- Bonnyaud, C.; Pradon, D.; Boudarham, J.; Robertson, J.; Vuillerme, N.; Roche, N. Effects of gait training using a robotic constraint (Lokomat®) on gait kinematics and kinetics in chronic stroke pa-tients. J. Rehabil. Med. 2014, 46, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Diserens, K.; Perret, N.; Chatelain, S.; Bashir, S.; Ruegg, D.; Vuadens, P.; Vingerhoets, F. The effect of repetitive arm cycling on post stroke spasticity and motor control: Repetitive arm cycling and spasticity. J. Neurol. Sci. 2007, 253, 18–24. [Google Scholar] [CrossRef]
- Shimodozono, M.; Noma, T.; Nomoto, Y.; Hisamatsu, N.; Kamada, K.; Miyata, R.; Matsumoto, S.; Ogata, A.; Etoh, S.; Basford, J.R.; et al. Benefits of a repetitive facilitative exercise program for the upper paretic extremity after subacute stroke: A randomized controlled trial. Neurorehabil. Neural Repair 2013, 27, 296–305. [Google Scholar] [CrossRef]
- Hwang, J.; You, S.H.; Choi, W.J.; Yi, C.-H. Effects of Robot-assisted Gait With Body Weight Support on Torque, Work, and Power of Quadriceps and Hamstring Muscles in Healthy Subjects. Phys. Ther. Korea 2021, 28, 215–226. [Google Scholar] [CrossRef]
- Nielsen, B.; Nybo, L. Cerebral Changes During Exercise in the Heat. Sports Med. 2003, 33, 1–11. [Google Scholar] [CrossRef]
- Park, C.; Park, O.M.; Bialek, A.; Friel, K.; Edwards, D.; You, J.S.H. Abnormal synergistic gait mitigation in acute stroke using an innovative ankle–knee–hip interlimb humanoid robot: A preliminary randomized controlled trial. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Lee, S.; Kim, J.; Baker, L.; Long, A.; Karavas, N.; Menard, N.; Galiana, I.; Walsh, C.J. Autonomous multi-joint soft exosuit with augmentation-power-based control parameter tuning reduces energy cost of loaded walking. J. Neuroeng. Rehabil. 2018, 15, 1–9. [Google Scholar] [CrossRef]
- Satoh, Y.; Yamada, T.; Arai, Y.; Shimamura, R.; Hirosawa, M.; Yamakawa, R.; Takagi, S. The immediate effect of the Honda Walking Assist Device on foot and ankle function in hemiplegic stroke patients. J. Phys. Ther. Sci. 2020, 32, 405–409. [Google Scholar] [CrossRef]
- Baunsgaard, C.B.; Nissen, U.V.; Brust, A.K.; Frotzler, A.; Ribeill, C.; Kalke, Y.-B.; León, N.; Gómez, B.; Samuelsson, K.; Antepohl, W.; et al. Gait training after spinal cord injury: Safety, feasibility and gait function following 8 weeks of training with the exoskeletons from Ekso Bionics. Spinal Cord 2018, 56, 106–116. [Google Scholar] [CrossRef] [Green Version]
- Hesse, S.; Tomelleri, C.; Bardeleben, A.; Werner, C.; Waldner, A. Robot-assisted practice of gait and stair climbing in nonambulatory stroke patients. J. Rehabil. Res. Dev. 2012, 49, 613. [Google Scholar] [CrossRef]
- Morone, G.; Iosa, M.; Bragoni, M.; Angelis, D.D.; Venturiero, V.; Coiro, P.; Riso, R.; Pratesi, L.; Paolucci, S. Who may have durable benefit from robotic gait training? A 2-year follow-up randomized controlled trial in patients with subacute stroke. Stroke 2012, 43, 1140–1142. [Google Scholar] [CrossRef] [Green Version]
- Ochi, M.; Wada, F.; Saeki, S.; Hachisuka, K. Gait training in subacute non-ambulatory stroke patients using a full weight-bearing gait-assistance robot: A prospective, randomized, open, blinded-endpoint trial. J. Neurol. Sci. 2015, 353, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Reid, L.; Boyd, R.N.; Cunnington, R.; Rose, S.E. Interpreting Intervention Induced Neuroplasticity with fMRI: The Case for Multimodal Imaging Strategies. Neural Plast. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 57) | LFAC (n = 30) | HFAC (n = 27) | p-Value |
|---|---|---|---|---|
| Age (years) | 63.86 ± 12.72 | 65.47 ± 13.67 | 63.19 ± 11.8 | 0.708 1 |
| Height (cm) | 164.63 ± 8.76 | 163.43 ± 9.48 | 165.96 ± 7.84 | 0.28 1 |
| Weight (kg) | 62.46 ± 10.11 | 60.15 ± 8.37 | 65.02 ± 11.37 | 0.069 1 |
| Onset (month) | 2.04 ± 3.06 | 2.63 ± 2.26 | 3.41 ± 3.54 | 0.345 1 |
| Gender | ||||
| Male (%) | 34 (60%) | 16 (53%) | 18 (67%) | 0.306 2 |
| Female (%) | 23 (40%) | 14 (47%) | 9 (33%) | |
| Type of stroke | ||||
| Hemorrhage (%) Infarction (%) | 33 (58%) 24 (42%) | 19 (63%) 11 (37%) | 14 (52%) 13 (48%) | 0.381 2 |
| Side of hemiplegia | ||||
| Left (%) | 36 (63%) | 19 (64%) | 17 (63%) | 0.977 2 |
| Right (%) | 21 (37%) | 11 (36%) | 10 (37%) |
| Pre-Test | LFAC | HFAC | p-Value |
|---|---|---|---|
| FMA | 12.73 ± 16.15 | 32.59 ± 24.25 | 0.001 * |
| MAS | 1.57 ± 0.82 | 1.37 ± 0.74 | 0.348 |
| BBS | 3.2 ± 3.46 | 15.48 ± 10.33 | 0.000 * |
| TIS | 3.97 ± 5.33 | 9.11 ± 5.41 | 0.001 * |
| STEP | 646.4 ± 347.67 | 654.15 ± 340.79 | 0.933 |
| DIS | 350.43 ± 185.58 | 364.74 ± 223.96 | 0.793 |
| LFAC | HFAC | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Mean Change, MCID | Pre-Test | Post-Test | Mean Change, MCID | Time Main Effect | Between Groups | Time × Group | |
| FMA | 12.73 ± 16.15 | 15.5 ± 17.15 | 2.77 < 3.13 | 32.59 ± 24.25 | 36.37 ± 24.94 | 3.78 < 4.8 | 0.404 | 0.000 ** | 0.303 |
| MAS | 1.57 ± 0.82 | 1.47 ± 0.73 | −0.1 < 0.13 | 1.37 ± 0.74 | 1.37 ± 0.74 | 0 < 0.14 | 0.805 | 0.363 | 0.000 |
| BBS | 3.2 ± 3.46 | 7.23 ± 4.6 | 4.03 ‡ > 0.84 | 15.48 ± 10.33 | 27.19 ± 6.25 | 11.71 ‡ > 1.2 | 0.000 ** | 0.000 ** | 0.000 ** |
| TIS | 3.97 ± 5.33 | 4.87 ± 5.59 | 0.9 < 1.02 | 9.11 ± 5.41 | 12.96 ± 5.26 | 3.85 ‡ > 1 | 0.026 ** | 0.000 ** | 0.167 |
| STEP | 646.4 ± 347.67 | 1043.83 ± 346 | 397.43 ‡ > 63.17 | 654.15 ± 340.79 | 1125.07 ± 311.58 | 470.92 ‡ > 59.96 | 0.000 ** | 0.482 | 0.000 |
| DIS | 350.43 ± 185.58 | 564 ± 183.85 | 213.57 ‡ > 33.57 | 364.74 ± 223.96 | 590.22 ± 216.55 | 225.48 ‡ > 41.67 | 0.000 ** | 0.593 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, W.; Park, C.; Oh, S.; You, S.H. Stage 2: Who Are the Best Candidates for Robotic Gait Training Rehabilitation in Hemiparetic Stroke? J. Clin. Med. 2021, 10, 5715. https://doi.org/10.3390/jcm10235715
Oh W, Park C, Oh S, You SH. Stage 2: Who Are the Best Candidates for Robotic Gait Training Rehabilitation in Hemiparetic Stroke? Journal of Clinical Medicine. 2021; 10(23):5715. https://doi.org/10.3390/jcm10235715
Chicago/Turabian StyleOh, Wonjun, Chanhee Park, Seungjun Oh, and Sung (Joshua) H. You. 2021. "Stage 2: Who Are the Best Candidates for Robotic Gait Training Rehabilitation in Hemiparetic Stroke?" Journal of Clinical Medicine 10, no. 23: 5715. https://doi.org/10.3390/jcm10235715
APA StyleOh, W., Park, C., Oh, S., & You, S. H. (2021). Stage 2: Who Are the Best Candidates for Robotic Gait Training Rehabilitation in Hemiparetic Stroke? Journal of Clinical Medicine, 10(23), 5715. https://doi.org/10.3390/jcm10235715