
The Impact of COVID-19 Pandemic and Lockdown Restrictions on Cardiac Implantable Device Recipients with Remote Monitoring

 , ,
, ,  , , ,
, , , 
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Population
2.2. Data Collection
- -
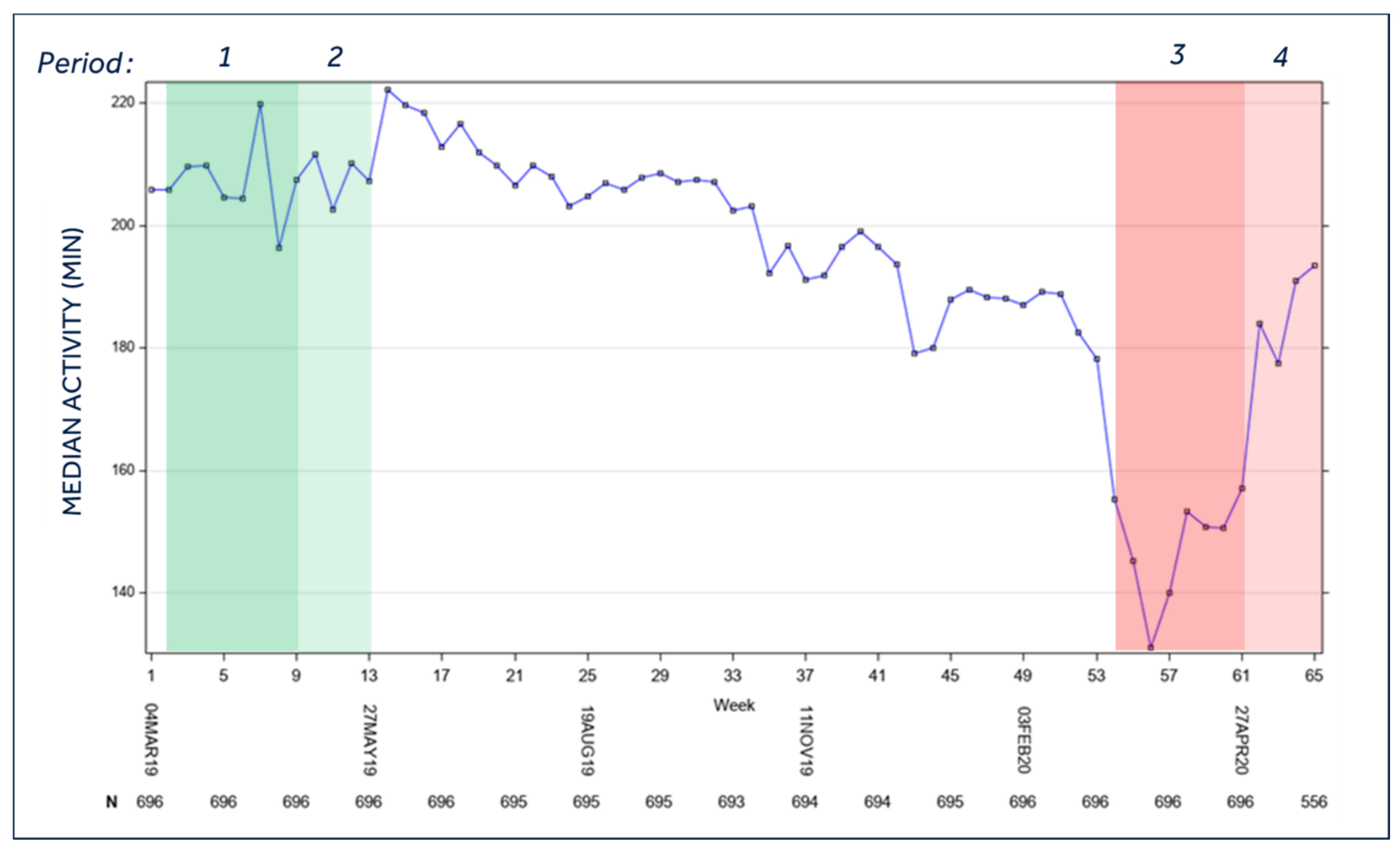
- Patient activity, that is, the total time active per day using a capacitive accelerometer; a minute is considered active if the counts exceed a threshold equal to walking approximately 70 steps/min.
- -
- AT/AF burden, measured as the total duration of a fast atrial rate during a 24 h period, with an atrio-ventricular conduction ratio ≥2:1.
- -
- Optivol Fluid index, that corresponds to changes in thoracic fluid levels. The fluid index trend is the cumulative difference between the daily average and patient-specific reference intrathoracic impedances. The intrathoracic impedance is calculated from the voltage measured from an asynchronous current applied between the right ventricular lead and the device case. The Optivol index was represented as the number of days per week with Optivol index >60 Ohm or >120 Ohm.
- -
- Heart rate variability (HRV), that is, the standard deviation of 5 min median of atrial intervals during a 24 h period. Reduced HRV suggests an increase in sympathetic tone.
- -
- Night heart rate (NHR), that is, the average heart rate between midnight and 4:00 a.m. NHR is a proxy for the resting heart rate.
- -
- Percentage of ventricular pacing.
- -
- Number of VT episodes and number of total ventricular arrhythmic episodes, that includes monitored VT, VT, and fast VT and VF. Ventricular arrhythmias were analyzed as a mean weekly number of episode/100 patients and as a percentage of patients with at least one episode of ventricular arrhythmias.
- -
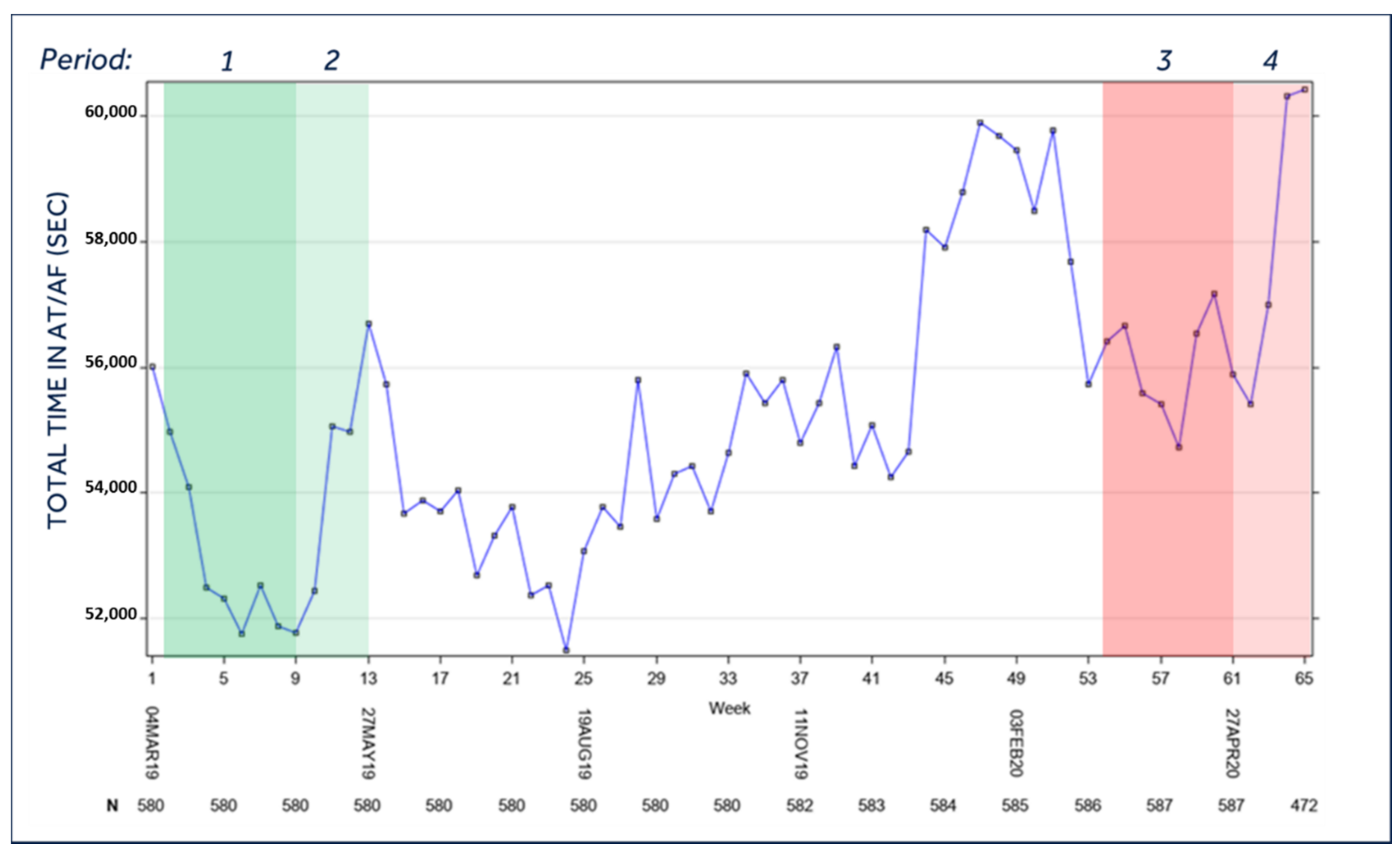
- AT/AF was summarized by the median and total duration per day and was collected only in patients with a functional atrial lead.
2.3. Timeframe of the Analysis
- (1)
- Period 1 (lockdown control period): 11 March 2019—5 May 2019;
- (2)
- Period 2 (post-lockdown control period): 6 May 2019—2 June 2019;
- (3)
- Period 3 (lockdown period): 9 March 2020—3 May 2020;
- (4)
- Period 4 (post-lockdown period): 4 May—31 May 2020.
2.4. Statistical Analysis
3. Results
3.1. Patients’ Activity
3.2. Burden of AF
3.3. Day and Night Heart Rate
3.4. Percentage of Ventricular Pacing
3.5. Optivol Fluid Index
3.6. Heart Rate Variability
3.7. Ventricular Arrhythmias
3.8. Patients with/without Arrhythmias during the Lockdown
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, W.; Zhang, Z.; Cheng, W.; Yang, C.; Diao, L.; Liu, W. Associations of leisure-time physical activity with cardiovascular mortality: A systematic review and meta-analysis of 44 prospective cohort studies. Eur. J. Prev. Cardiol. 2018, 25, 1864–1872. [Google Scholar] [CrossRef]
- Kivimäki, M.; Singh-Manoux, A.; Pentti, J.; Sabia, S.; Nyberg, S.T.; Alfredsson, L.; Goldberg, M.; Knutsson, A.; Koskenvuo, M.; Koskinen, A.; et al. Physical inactivity, cardiometabolic disease, and risk of dementia: An individual-participant meta-analysis. BMJ 2019, 365, l1495. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of Coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Dherange, P.; Lang, J.; Qian, P.; Oberfeld, B.; Sauer, W.H.; Koplan, B.; Tedrow, U. Arrhythmias and COVID-19. JACC Clin. Electrophysiol. 2020, 6, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Impatto Dell’Epidemia COVID-19 Sulla Mortalità Totale della Popolazione Residente Periodo Gennaio-Novembre 2020. Available online: https://www.iss.it/documents/20126/0/Rapp_Istat_Iss_FINALE+2020_rev.pdf/b4c40cbb-9506-c3f6-5b69-0ccb5f015172?t=1609328171264 (accessed on 11 August 2021).
- Biffi, M.; Candelora, A.; Massaro, G. Ventricular fibrillation triggered by earthquake during the accumoli-amatrice disaster in Italy. Circ. J. 2017, 81, 759–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakano, M.; Kondo, M.; Wakayama, Y.; Kawana, A.; Hasebe, Y.; Shafee, M.A.; Fukuda, K.; Shimokawa, H. Increased incidence of tachyarrhythmias and heart failure hospitalization in patients with implanted cardiac devices after the great East Japan earthquake disaster. Circ. J. 2012, 76, 1283–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soumya, R.S.; Unni, T.G.; Raghu, K.G. Impact of COVID-19 on the cardiovascular system: A review of available reports. Cardiovasc. Drugs 2021, 35, 411–425. [Google Scholar] [CrossRef]
- Official Declaration of the COVID-19 Pandemic by the WHO the 11th March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 August 2021).
- Gupta, A.K.; Jneid, H.; Addison, D.; Ardehali, H.; Boehme, A.K.; Borgaonkar, S.; Boulestreau, R.; Clerkin, K.; Delarche, N.; DeVon, H.A.; et al. Current perspectives on Coronavirus disease 2019 and cardiovascular disease: A white paper by the JAHA Editors. JAHA 2020, 9, e017013. [Google Scholar] [CrossRef]
- Kulkarni, P.; Mahadevappa, M.; Alluri, S. COVID-19 pandemic and the impact on the cardiovascular disease patient care. CCR 2020, 16, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Bromage, D.I.; Cannatà, A.; Rind, I.A.; Gregorio, C.; Piper, S.; Shah, A.M.; McDonagh, T.A. The impact of COVID-19 on heart failure hospitalization and management: Report from a heart failure unit in London during the peak of the pandemic. Eur. J. Heart Fail. 2020, 22, 978–984. [Google Scholar] [CrossRef] [PubMed]
- Boukhris, M.; Hillani, A.; Moroni, F.; Annabi, M.S.; Addad, F.; Ribeiro, M.H.; Mansour, S.; Zhao, X.; Ybarra, L.F.; Abbate, A.; et al. Cardiovascular implications of the COVID-19 pandemic: A global perspective. Can. J. Cardiol. 2020, 36, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Rattka, M.; Baumhardt, M.; Dreyhaupt, J.; Rothenbacher, D.; Thiessen, K.; Markovic, S.; Rottbauer, W.; Imhof, A. 31 Days of COVID-19—Cardiac events during restriction of public life—A comparative study. Clin. Res. Cardiol. 2020, 109, 1476–1482. [Google Scholar] [CrossRef] [PubMed]
- AIAC Ricerca Network Investigators; Boriani, G.; Palmisano, P.; Guerra, F.; Bertini, M.; Zanotto, G.; Lavalle, C.; Notarstefano, P.; Accogli, M.; Bisignani, G.; et al. Impact of COVID-19 pandemic on the clinical activities related to arrhythmias and electrophysiology in Italy: Results of a survey promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing). Intern. Emerg. Med. 2020, 15, 1445–1456. [Google Scholar] [CrossRef]
- Lakkireddy, D.R.; Chung, M.K.; Gopinathannair, R.; Patton, K.K.; Gluckman, T.J.; Turagam, M.; Cheung, J.; Patel, P.; Sotomonte, J.; Lampert, R.; et al. Guidance for cardiac electrophysiology during the COVID-19 pandemic from the Heart Rhythm Society COVID-19 Task Force; Electrophysiology section of the american college of cardiology; and the Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology, American Heart Association. Circulation 2020, 141, e823–e831. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Fraccaro, C.; Chieffo, A.; Marchese, A.; Tarantino, F.F.; Rigattieri, S.; Limbruno, U.; Mauro, C.; La Manna, A.; Castiglioni, B.; et al. Italian Society of Interventional Cardiology (GISE) position paper for cath lab-specific preparedness recommendations for healthcare providers in case of suspected, probable or confirmed cases of COVID-19. Catheter. Cardiovasc. Interv. 2020, 96, 839–843. [Google Scholar] [CrossRef]
- Mahmud, E.; Dauerman, H.L.; Welt, F.G.P.; Messenger, J.C.; Rao, S.V.; Grines, C.; Mattu, A.; Kirtane, A.J.; Jauhar, R.; Meraj, P.; et al. Management of acute myocardial infarction during the COVID-19 pandemic: A consensus statement from the Society for Cardiovascular Angiography and Interventions (SCAI), the American College of Cardiology (ACC), and the American College of Emergency Physicians (ACEP). Catheter. Cardiovasc. Interv. 2020, 96, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Van der Velde, E.T.; Atsma, D.E.; Foeken, H.; Witteman, T.A.; Hoekstra, W.H. Remote monitoring of patients with implanted devices: Data exchange and integration. Eur. J. Prev. Cardiol. 2013, 20, 8–12. [Google Scholar] [CrossRef]
- Boriani, G.; De Ponti, R.; Guerra, F.; Palmisano, P.; Zanotto, G.; D’Onofrio, A.; Ricci, R.P. Sinergy between drugs and devices in the fight against sudden cardiac death and heart failure. Eur. J. Prev. Cardiol. 2021, 28, 110–123. [Google Scholar] [CrossRef]
- O’Shea, C.J.; Thomas, G.; Middeldorp, M.E.; Harper, C.; Elliott, A.D.; Ray, N.; Lau, D.H.; Campbell, K.; Sanders, P. Ventricular arrhythmia burden during the Coronavirus disease 2019 (COVID-19) pandemic. Eur. Heart J. 2021, 42, 520–528. [Google Scholar] [CrossRef]
- Russo, V.; Solimene, F.; Zanotto, G.; Pisanò, E.C.; Della Bella, P.; Iacopino, S.; Pignalberi, C.; Calvi, V.; Maglia, G.; Quartieri, F.; et al. Seasonal trend of ventricular arrhythmias in a nationwide remote monitoring database of implantable defibrillators and cardiac resynchronization devices. Int. J. Cardiol. 2019, 275, 104–106. [Google Scholar] [CrossRef]
- Boriani, G.; Vitolo, M. COVID-19 pandemic: Complex interactions with the arrhythmic profile and the clinical course of patients with cardiovascular disease. Eur. Heart J. 2021, 42, 529–532. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | (N = 696) |
|---|---|
| Age at first implant (yrs), Mean ± SD | 63.7 ± 13.2 |
| Time from first implant to 4 March 2019 (yrs), Mean ± SD | 4.85 ± 3.62 |
| Gender (Male), %, n/Pts | 78.0% (536/687) |
| Therapy, %, n/Pts | |
| Dual chamber | 17.8% (124/696) |
| Biventricular | 59.3% (413/696) |
| Single chamber | 21.0% (146/696) |
| Other/Unknown | 1.9% (13/696) |
| Prevention, %, n/Pts | |
| Primary | 68.1% (474/696) |
| Secondary | 15.1% (105/696) |
| Other/Unknown | 16.8% (117/696) |
| Medical history, %, n/Pts | |
| History of HF | 70.0% (471/673) |
| NYHA Class 3/4 | 37.9% (232/612) |
| History of VT/VF | 32.6% (220/675) |
| History of AT/AF | 29.1% (197/677) |
| Paroxysmal AF | 17.4% (118/677) |
| Persistent AF | 3.7% (25/677) |
| Permanent AF | 8.0% (54/677) |
| MI | 31.4% (214/681) |
| Third grade AV block | 6.2% (43/696) |
| LBBB | 38.2% (266/696) |
| Sinus Node Disease | 7.6% (49/646) |
| History of syncope | 14.2% (78/549) |
| History of Stroke/TIA | 6.0% (35/586) |
| Hypertension | 58.1% (377/649) |
| Diabetes | 23.8% (145/609) |
| Chronic Kidney Disease | 11.7% (76/652) |
| COPD | 11.0% (65/591) |
| CHADS2 ≥ 2, %, n/Pts | 58.8% (306/520) |
| CHADS2-VASC ≥ 4, %, n/Pts | 31.5% (98/311) |
| LVEF at baseline (%), Mean ± SD | 33.7 ± 12.1 |
| Clinical Characteristics | AT/AF < 1 h and no VT/VF Arrythmias (N = 595) | AT/AF ≥ 1 h a/o VT/VF Arrythmias (N = 101) | p-Value |
|---|---|---|---|
| Age at first implant (yrs), Mean ± SD | 63.2 ± 13.4 | 66.5 ± 11.2 | 0.044 |
| Time from first implant to 4 March 2019 (yrs), Mean ± SD | 4.90 ± 3.65 | 4.57 ± 3.45 | 0.321 |
| Gender (Male), %, n/Pts | 77.9% (457/587) | 79.0% (79/100) | 0.798 |
| Therapy, %, n/Pts | |||
| Dual chamber | 17.6% (105/595) | 18.8% (19/101) | 0.242 |
| Biventricular | 58.5% (348/595) | 64.4% (65/101) | |
| Single chamber | 22.2% (132/595) | 13.9% (14/101) | |
| Other/Unknown | 1.7% (10/595) | 3.0% (3/101) | |
| Prevention, %, n/Pts | |||
| Primary | 69.1% (411/595) | 62.4% (63/101) | 0.309 |
| Secondary | 15.0% (89/595) | 15.8% (16/101) | |
| Other/Unknown | 16.0% (95/595) | 21.8% (22/101) | |
| Medical history, %, n/Pts | |||
| History of HF | 69.5% (398/573) | 73.0% (73/100) | 0.476 |
| NYHA Class 3/4 | 38.1% (200/525) | 36.8% (32/87) | 0.815 |
| History of VT/VF | 31.0% (179/577) | 41.8% (41/98) | 0.035 |
| History of AT/AF | 24.3% (140/577) | 57.0% (57/100) | <0.001 |
| Paroxysmal AF | 13.9% (80/577) | 38.0% (38/100) | <0.001 |
| Persistent AF | 2.1% (12/577) | 13.0% (13/100) | <0.001 |
| Permanent AF | 8.3% (48/577) | 6.0% (6/100) | 0.429 |
| MI | 30.3% (177/585) | 38.5% (37/96) | 0.105 |
| 3rd grade AV block | 6.2% (37/595) | 5.9% (6/101) | 0.915 |
| LBBB | 38.2% (227/595) | 38.6% (39/101) | 0.930 |
| Sinus Node Disease | 7.1% (39/552) | 10.6% (10/94) | 0.226 |
| History of syncope | 13.6% (63/463) | 17.4% (15/86) | 0.350 |
| History of Stroke/TIA | 5.4% (27/500) | 9.3% (8/86) | 0.158 |
| Hypertension | 57.0% (314/551) | 64.3% (63/98) | 0.177 |
| Diabetes | 23.2% (121/521) | 27.3% (24/88) | 0.410 |
| Chronic Kidney Disease | 11.4% (63/554) | 13.3% (13/98) | 0.590 |
| COPD | 57.0% (252/442) | 69.2% (54/78) | 0.043 |
| CHADS2 ≥ 2, %, n/Pts | 31.7% (83/262) | 30.6% (15/49) | 0.883 |
| CHADS2-VASC ≥ 4, %, n/Pts | 10.5% (53/505) | 14.0% (12/86) | 0.343 |
| LVEF at baseline (%), Mean ± SD | 34.4 ± 13.1 | 31.4 ± 7.9 | 0.706 |
| Follow-up | |||
| Average Median activity (min), Mean ± SD | 152.0 ± 111.9 | 123.8 ± 109.5 | 0.008 |
| Average Median heart rate variability (ms), Mean ± SD | 87.0 ± 31.6 | 82.6 ± 44.4 | 0.136 |
| Average Number of days with Optivol threshold > 60 | 52.8 ± 143.5 | 87.7 ± 194.1 | 0.004 |
| Average Number of days with Optivol threshold > 120 | 25.3 ± 109.6 | 50.6 ± 165.2 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diemberger, I.; Vicentini, A.; Cattafi, G.; Ziacchi, M.; Iacopino, S.; Morani, G.; Pisanò, E.; Molon, G.; Giovannini, T.; Dello Russo, A.; et al. The Impact of COVID-19 Pandemic and Lockdown Restrictions on Cardiac Implantable Device Recipients with Remote Monitoring. J. Clin. Med. 2021, 10, 5626. https://doi.org/10.3390/jcm10235626
Diemberger I, Vicentini A, Cattafi G, Ziacchi M, Iacopino S, Morani G, Pisanò E, Molon G, Giovannini T, Dello Russo A, et al. The Impact of COVID-19 Pandemic and Lockdown Restrictions on Cardiac Implantable Device Recipients with Remote Monitoring. Journal of Clinical Medicine. 2021; 10(23):5626. https://doi.org/10.3390/jcm10235626
Chicago/Turabian StyleDiemberger, Igor, Alessandro Vicentini, Giuseppe Cattafi, Matteo Ziacchi, Saverio Iacopino, Giovanni Morani, Ennio Pisanò, Giulio Molon, Tiziana Giovannini, Antonio Dello Russo, and et al. 2021. "The Impact of COVID-19 Pandemic and Lockdown Restrictions on Cardiac Implantable Device Recipients with Remote Monitoring" Journal of Clinical Medicine 10, no. 23: 5626. https://doi.org/10.3390/jcm10235626
APA StyleDiemberger, I., Vicentini, A., Cattafi, G., Ziacchi, M., Iacopino, S., Morani, G., Pisanò, E., Molon, G., Giovannini, T., Dello Russo, A., Boriani, G., Bertaglia, E., Biffi, M., Bongiorni, M. G., Rordorf, R., & Zucchelli, G. (2021). The Impact of COVID-19 Pandemic and Lockdown Restrictions on Cardiac Implantable Device Recipients with Remote Monitoring. Journal of Clinical Medicine, 10(23), 5626. https://doi.org/10.3390/jcm10235626