
Efficacy and Safety of Tenofovir Disoproxil Orotate in Chronic Hepatitis B Patients Previously Treated with Tenofovir Disoproxil Fumarate: Multicenter, Open-Label, Prospective Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Study Design
2.3. Laboratory Assays
2.4. Endpoints
2.5. Statistical Analyses
2.6. Ethical Declaration
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Virologic Response
3.3. Biochemical and Serologic Responses
3.4. Changes in HBV DNA Titer
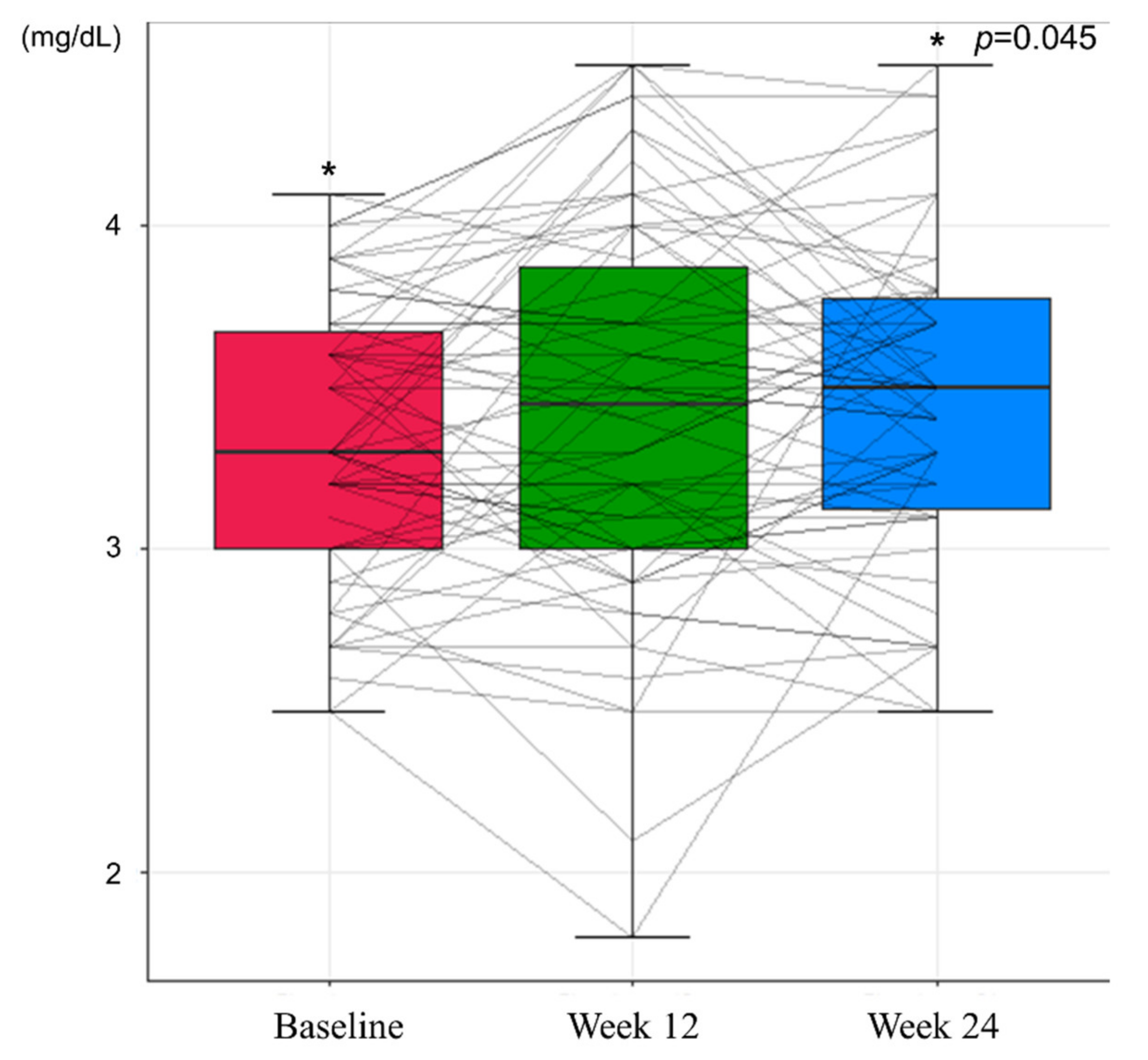
3.5. Safety Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Lai, C.L.; Yuen, M.F. Prevention of hepatitis B virus-related hepatocellular carcinoma with antiviral therapy. Hepatology 2013, 57, 399–408. [Google Scholar] [CrossRef]
- Marcellin, P.; Gane, E.; Buti, M.; Afdhal, N.; Sievert, W.; Jacobson, I.M.; Washington, M.K.; Germanidis, G.; Flaherty, J.F.; Aguilar Schall, R.; et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: A 5-year open-label follow-up study. Lancet 2013, 381, 468–475. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Mak, C.W.; Lee, S.K.; Ip, Z.M.; Lam, A.T.; Iu, H.W.; Leung, J.M.; Lai, J.W.; Lo, A.O.; et al. Entecavir treatment reduces hepatic events and deaths in chronic hepatitis B patients with liver cirrhosis. Hepatology 2013, 58, 1537–1547. [Google Scholar] [CrossRef] [PubMed]
- Chevaliez, S.; Hezode, C.; Bahrami, S.; Grare, M.; Pawlotsky, J.M. Long-term hepatitis B surface antigen (HBsAg) kinetics during nucleoside/nucleotide analogue therapy: Finite treatment duration unlikely. J. Hepatol. 2013, 58, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Seto, W.K.; Hui, A.J.; Wong, V.W.; Wong, G.L.; Liu, K.S.; Lai, C.L.; Yuen, M.F.; Chan, H.L. Treatment cessation of entecavir in Asian patients with hepatitis B e antigen negative chronic hepatitis B: A multicentre prospective study. Gut 2015, 64, 667–672. [Google Scholar] [CrossRef]
- Fardis, M.; Oliyai, R. Case study: Tenofovir disoproxil fumarate: An oral prodrug of tenofovir. In Prodrugs: Challenges and Rewards Part 1; Stella, V.J., Borchardt, R.T., Hageman, M.J., Oliyai, R., Maag, H., Tilley, J.W., Eds.; Springer: New York, NY, USA, 2007; pp. 1347–1357. [Google Scholar] [CrossRef]
- Jenh, A.M.; Pham, P.A. Tenofovir disoproxil fumarate in the treatment of chronic hepatitis B. Expert Rev. Anti. Infect. Ther. 2010, 8, 1079–1092. [Google Scholar] [CrossRef]
- Marcellin, P.; Wong, D.K.; Sievert, W.; Buggisch, P.; Petersen, J.; Flisiak, R.; Manns, M.; Kaita, K.; Krastev, Z.; Lee, S.S.; et al. Ten-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B virus infection. Liver Int. 2019, 39, 1868–1875. [Google Scholar] [CrossRef]
- Kim, Y.K.; Choi, M.J.; Oh, T.Y.; Yu, K.S.; Lee, S. A comparative pharmacokinetic and tolerability analysis of the novel orotic acid salt form of tenofovir disoproxil and the fumaric acid salt form in healthy subjects. Drug Des. Dev. Ther. 2017, 11, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Marcellin, P.; Heathcote, E.J.; Buti, M.; Gane, E.; de Man, R.A.; Krastev, Z.; Germanidis, G.; Lee, S.S.; Flisiak, R.; Kaita, K.; et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N. Engl. J. Med. 2008, 359, 2442–2455. [Google Scholar] [CrossRef]
- Buti, M.; Gane, E.; Seto, W.K.; Chan, H.L.; Chuang, W.L.; Stepanova, T.; Hui, A.J.; Lim, Y.S.; Mehta, R.; Janssen, H.L.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of patients with HBeAg-negative chronic hepatitis B virus infection: A randomised, double-blind, phase 3, non-inferiority trial. Lancet Gastroenterol. Hepatol. 2016, 1, 196–206. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Terrault, N.A.; Bzowej, N.H.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H. AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef]
- Chan, H.L.; Fung, S.; Seto, W.K.; Chuang, W.L.; Chen, C.Y.; Kim, H.J.; Hui, A.J.; Janssen, H.L.; Chowdhury, A.; Tsang, T.Y.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of HBeAg-positive chronic hepatitis B virus infection: A randomised, double-blind, phase 3, non-inferiority trial. Lancet Gastroenterol. Hepatol. 2016, 1, 185–195. [Google Scholar] [CrossRef]
- Liang, X.; Gao, Z.; Xie, Q.; Zhang, J.; Sheng, J.; Cheng, J.; Chen, C.; Mao, Q.; Zhao, W.; Ren, H.; et al. Long-term efficacy and safety of tenofovir disoproxil fumarate in Chinese patients with chronic hepatitis B: 5-year results. Hepatol. Int. 2019, 13, 260–269. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.H.; Park, D.S.; Kim, T.H.; Yeom, J.J.; Kim, H.C.; Moon, J.H.; Yang, J.S. Genotypes of hepatitis B virus on Jeju island. Korean J. Hepatol. 2004, 10, 42–50. [Google Scholar]
- Lin, C.L.; Kao, J.H. The clinical implications of hepatitis B virus genotype: Recent advances. J. Gastroenterol. Hepatol. 2011, 26 (Suppl. 1), 123–130. [Google Scholar] [CrossRef]
- Kim, B.K.; Revill, P.A.; Ahn, S.H. HBV genotypes: Relevance to natural history, pathogenesis and treatment of chronic hepatitis B. Antivir. Ther. 2011, 16, 1169–1186. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Tanaka, Y. Novel biomarkers for the management of chronic hepatitis B. Clin. Mol. Hepatol. 2020, 26, 261–279. [Google Scholar] [CrossRef]
- Dandri, M.; Locarnini, S. New insight in the pathobiology of hepatitis B virus infection. Gut 2012, 61 (Suppl. 1), i6–i17. [Google Scholar] [CrossRef]
- Yoshida, K.; Desbiolles, A.; Feldman, S.F.; Ahn, S.H.; Alidjinou, E.K.; Atsukawa, M.; Bocket, L.; Brunetto, M.R.; Buti, M.; Carey, I.; et al. Hepatitis B Core-Related Antigen to Indicate High Viral Load: Systematic Review and Meta-Analysis of 10,397 Individual Participants. Clin. Gastroenterol. Hepatol. 2021, 19, 46–60.e8. [Google Scholar] [CrossRef]
- Suzuki, F.; Miyakoshi, H.; Kobayashi, M.; Kumada, H. Correlation between serum hepatitis B virus core-related antigen and intrahepatic covalently closed circular DNA in chronic hepatitis B patients. J. Med. Virol. 2009, 81, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.K.; Seto, W.K.; Cheung, K.S.; Chong, C.K.; Huang, F.Y.; Fung, J.; Lai, C.L.; Yuen, M.F. Hepatitis B virus core-related antigen as a surrogate marker for covalently closed circular DNA. Liver Int. 2017, 37, 995–1001. [Google Scholar] [CrossRef]
- Testoni, B.; Lebosse, F.; Scholtes, C.; Berby, F.; Miaglia, C.; Subic, M.; Loglio, A.; Facchetti, F.; Lampertico, P.; Levrero, M.; et al. Serum hepatitis B core-related antigen (HBcrAg) correlates with covalently closed circular DNA transcriptional activity in chronic hepatitis B patients. J. Hepatol. 2019, 70, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Ishigami, M.; Ishizu, Y.; Kuzuya, T.; Honda, T.; Hayashi, K.; Ishikawa, T.; Nakano, I.; Hirooka, Y.; Goto, H. Cumulative incidence and risk factors for the development of hepatocellular carcinoma in patients with chronic hepatitis B who achieved sustained disappearance of viremia by nucleos(t)ide analog treatment. Hepatol. Res. 2018, 48, E240–E251. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.Y.; Chang, Y.; Nam, J.Y.; Cho, H.; Cho, E.J.; Lee, J.H.; Yu, S.J.; Yoon, J.H.; Kim, Y.J. Long-term Nucleotide Analogue Treatment Has Higher Levels of Renal Toxicities than Does Entecavir in Patients with Chronic Hepatitis B. Gut Liver 2020, 14, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Novoa, S.; Garcia-Samaniego, J.; Prieto, M.; Calleja, J.L.; Pascasio, J.M.; Delgado Blanco, M.; Crespo, J.; Buti, M.; Bonet Vidal, M.L.; Arenas Ruiz Tapiador, J.; et al. Altered Underlying Renal Tubular Function in Patients With Chronic Hepatitis B Receiving Nucleos(t)ide Analogs in a Real-World Setting: The MENTE Study. J. Clin. Gastroenterol. 2016, 50, 779–789. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 63) | |
|---|---|
| Age (year) | 49.05 ± 10.93 |
| Male, no. (%) | 42 (65.62%) |
| Platelet count | 204.34 ± 56.03 |
| Albumin (g/dL) | 4.7 (4.5, 4.9) |
| Total bilirubin (mg/dL) | 0.76 (0.5, 0.95) |
| Aspartate transaminase (U/L) | 22 (19.75, 28) |
| Alanine transaminase (U/L) | 22 (17, 30.5) |
| Prothrombin time (INR) | 1.04 (1, 1.07) |
| Creatinine (mg/dL) | 0.89 ± 0.17 |
| Glomerular filtration rate (ml/min) | 91.28 ± 17.58 |
| Phosphorus (mg/dL) | 3.3 (3, 3.62) |
| HBeAg positive, no. (%) | 17 (26.98%) |
| HBcrAg (log U/mL) | 4.15 ± 1.61 |
| Diabetes, no. (%) | 6 (9.38%) |
| Hypertension, no. (%) | 10 (15.62%) |
| ALT (IU/mL) | p Value | Proportion of Normal ALT (%) | p Value | |
|---|---|---|---|---|
| Baseline | 25.63 ± 13.24 | Ref. | 87.3% | Ref. |
| Week 12 | 26.92 ± 15.84 | 0.285 | 82.26% | 0.453 |
| Week 24 | 26.75 ± 18.10 | 0.387 | 87.3% | 1.000 |
| eGFR (IU/mL) | p Value | Phosphorus (mg/dL) | p Value | |
|---|---|---|---|---|
| Baseline | 91.09 ± 17.66 | Ref. | 3.33 ± 0.43 | Ref. |
| Week 12 | 94.46 ± 18.26 | 0.010 | 3.43 ± 0.60 | 0.119 |
| Week 24 | 93.34 ± 17.80 | 0.056 | 3.44 ± 0.49 | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.; Kim, S.-G.; Jeong, S.-W.; Jang, J.-Y.; Yoo, J.-J.; Lee, S.-H.; Kim, Y.-S.; Kim, H.-S.; Lee, H.-W.; Park, S. Efficacy and Safety of Tenofovir Disoproxil Orotate in Chronic Hepatitis B Patients Previously Treated with Tenofovir Disoproxil Fumarate: Multicenter, Open-Label, Prospective Study. J. Clin. Med. 2021, 10, 5628. https://doi.org/10.3390/jcm10235628
Chang Y, Kim S-G, Jeong S-W, Jang J-Y, Yoo J-J, Lee S-H, Kim Y-S, Kim H-S, Lee H-W, Park S. Efficacy and Safety of Tenofovir Disoproxil Orotate in Chronic Hepatitis B Patients Previously Treated with Tenofovir Disoproxil Fumarate: Multicenter, Open-Label, Prospective Study. Journal of Clinical Medicine. 2021; 10(23):5628. https://doi.org/10.3390/jcm10235628
Chicago/Turabian StyleChang, Young, Sang-Gyune Kim, Soung-Won Jeong, Jae-Young Jang, Jeong-Ju Yoo, Sae-Hwan Lee, Young-Seok Kim, Hong-Soo Kim, Hyun-Woong Lee, and Suyeon Park. 2021. "Efficacy and Safety of Tenofovir Disoproxil Orotate in Chronic Hepatitis B Patients Previously Treated with Tenofovir Disoproxil Fumarate: Multicenter, Open-Label, Prospective Study" Journal of Clinical Medicine 10, no. 23: 5628. https://doi.org/10.3390/jcm10235628
APA StyleChang, Y., Kim, S.-G., Jeong, S.-W., Jang, J.-Y., Yoo, J.-J., Lee, S.-H., Kim, Y.-S., Kim, H.-S., Lee, H.-W., & Park, S. (2021). Efficacy and Safety of Tenofovir Disoproxil Orotate in Chronic Hepatitis B Patients Previously Treated with Tenofovir Disoproxil Fumarate: Multicenter, Open-Label, Prospective Study. Journal of Clinical Medicine, 10(23), 5628. https://doi.org/10.3390/jcm10235628