
Clinical Implications of Sodium Zirconium Cyclosilicate Therapy in Patients with Systolic Heart Failure and Hyperkalemia



Abstract
:1. Background
2. Methods
2.1. Patient Selection
2.2. Study Design
2.3. SZC Therapy
2.4. Other Clinical Management
2.5. Data Collection
2.6. Statistics
3. Results
3.1. Baseline Characteristics
3.2. Before SZC Initiation
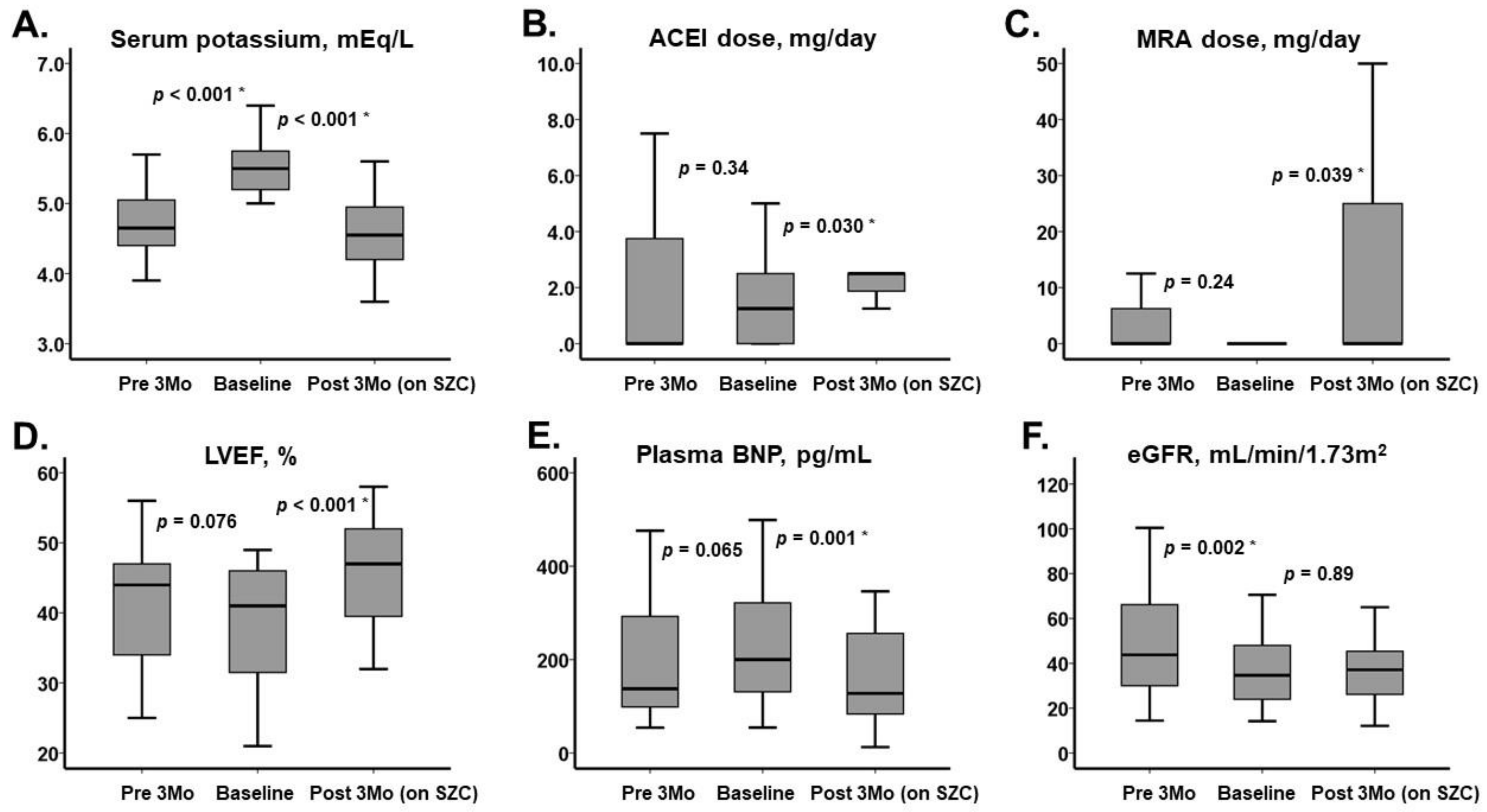
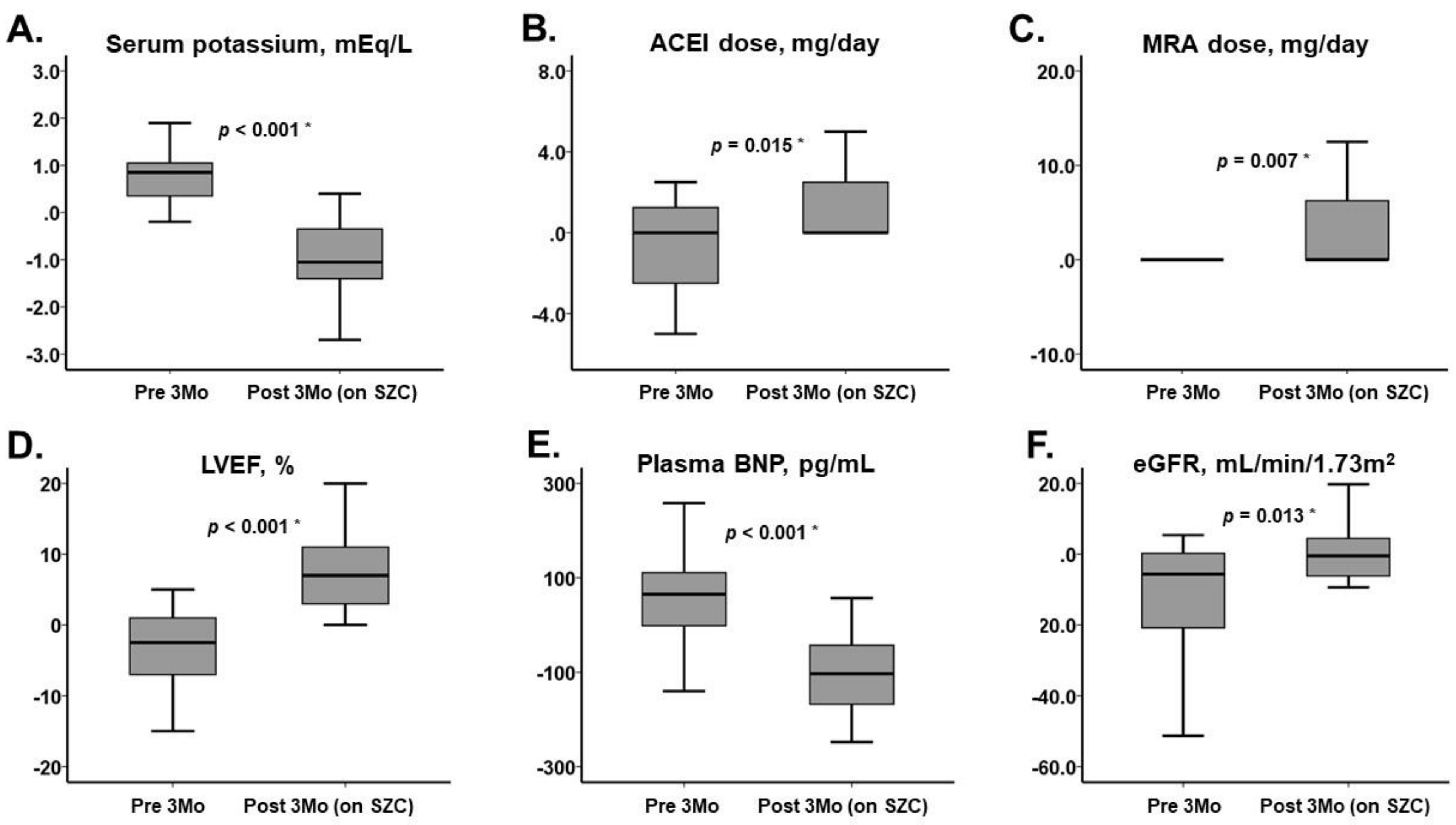
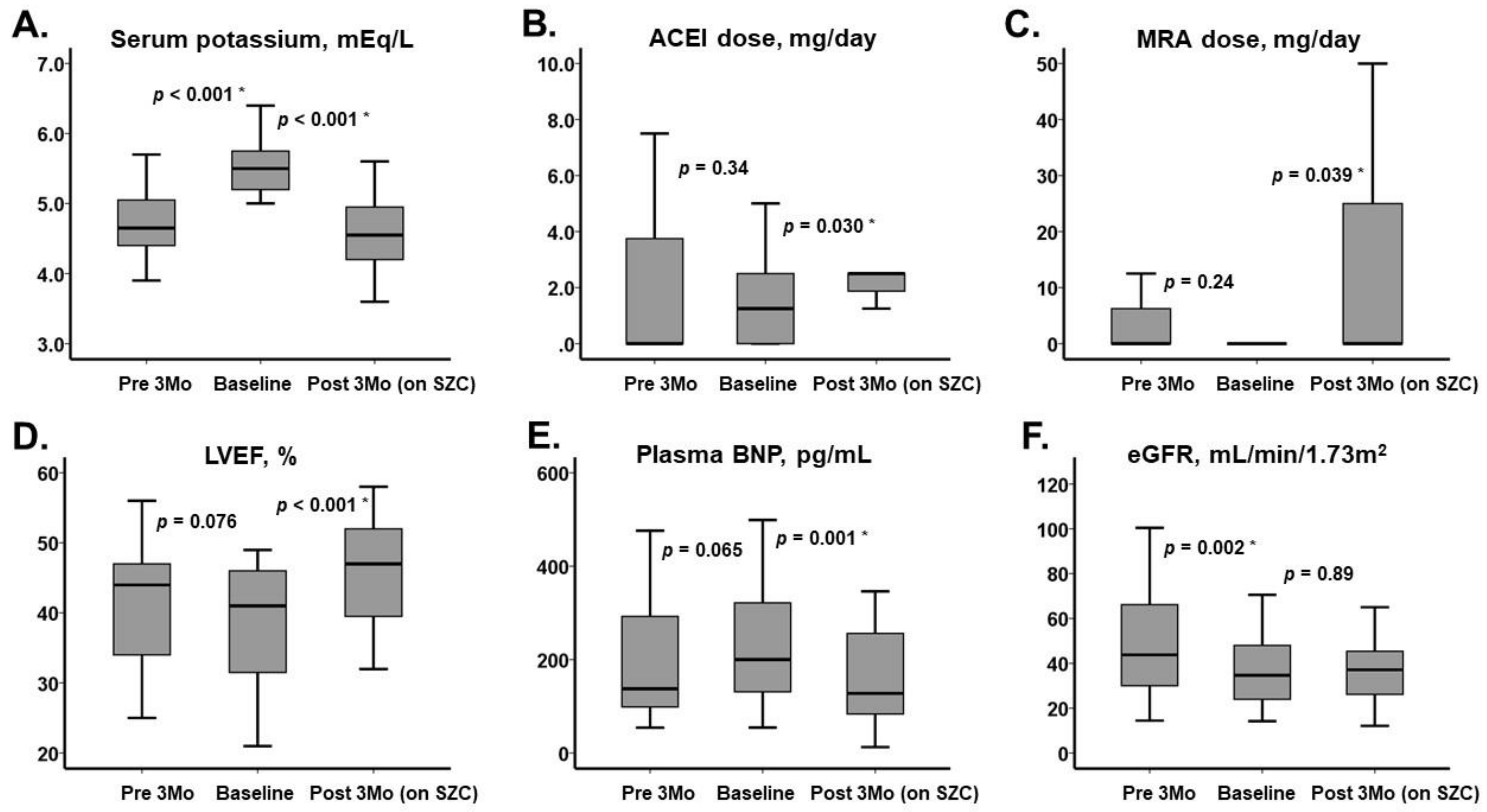
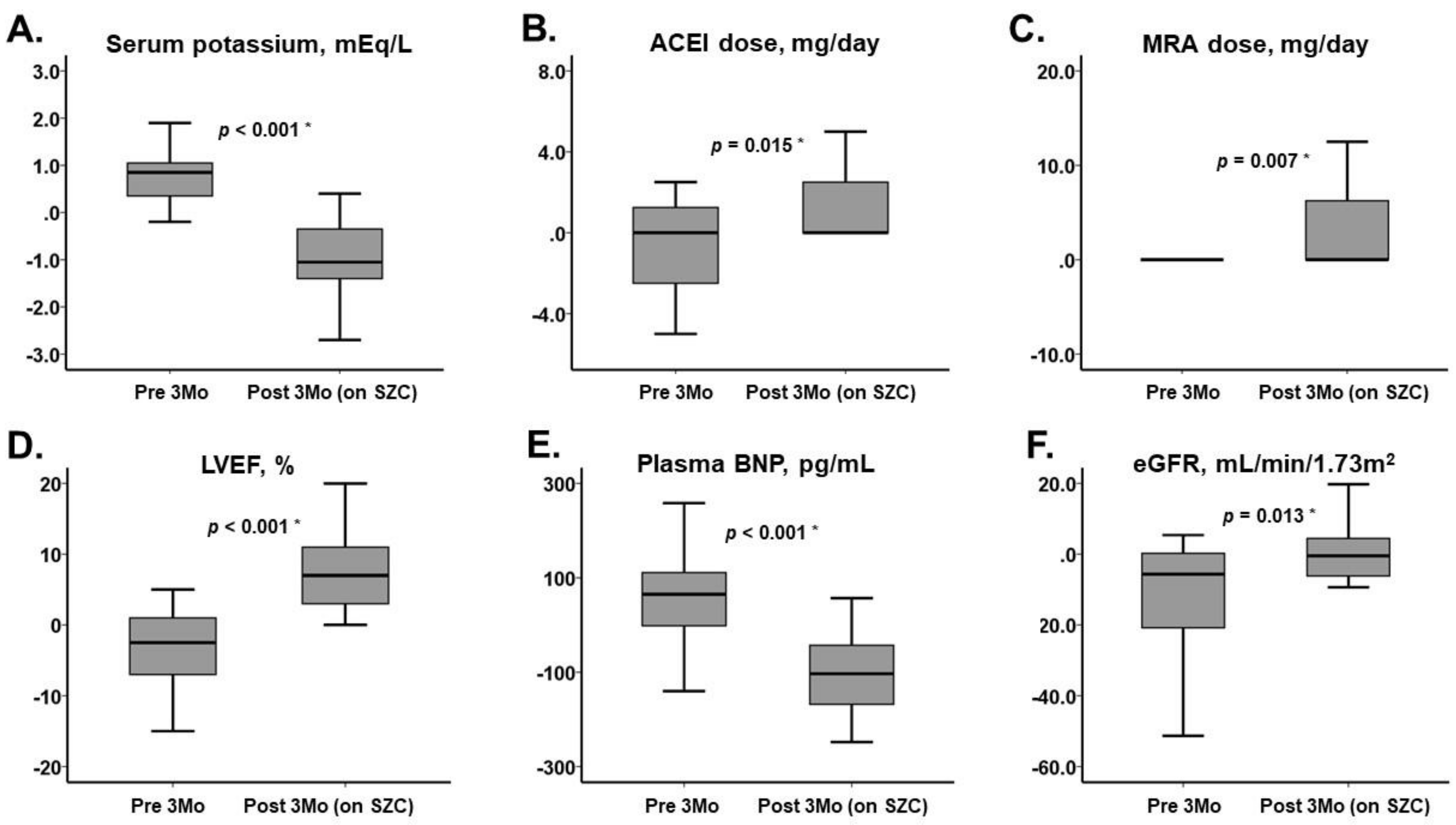
3.3. After SZC Initiation
4. Discussion
4.1. Impact of SZC on Hyperkalemia
4.2. Impact of SZC to Up-Titrate Renin–Angiotensin–Aldosterone System Inhibitors
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collins, A.J.; Pitt, B.; Reaven, N.; Funk, S.; McGaughey, K.; Wilson, D.; Bushinsky, D.A. Association of Serum Potassium with All-Cause Mortality in Patients with and without Heart Failure, Chronic Kidney Disease, and/or Diabetes. Am. J. Nephrol. 2017, 46, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Claggett, B.; Anand, I.; Rossignol, P.; Desai, A.S.; Zannad, F.; Pitt, B.; Solomon, S.D. Incidence, Predictors, and Outcomes Related to Hypo- and Hyperkalemia in Patients With Severe Heart Failure Treated With a Mineralocorticoid Receptor Antagonist. Circ. Hear. Fail. 2014, 7, 573–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossignol, P.; Dobre, D.; McMurray, J.J.; Swedberg, K.; Krum, H.; van Veldhuisen, D.J.; Shi, H.; Messig, M.; Vincent, J.; Girerd, N.; et al. Incidence, Determinants, and Prognostic Significance of Hyperkalemia and Worsening Renal Function in Patients with Heart Failure Receiving the Mineralocorticoid Receptor Antagonist Eplerenone or Placebo in Addition to Optimal Medical Therapy: Results from the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF). Circ. Heart Fail. 2014, 7, 51–58. [Google Scholar] [PubMed] [Green Version]
- Zannad, F.; Mcmurray, J.; Krum, H.; Van Veldhuisen, D.J.; Swedberg, K.; Shi, H.; Vincent, J.; Pocock, S.J.; Pitt, B. Eplerenone in Patients with Systolic Heart Failure and Mild Symptoms. N. Engl. J. Med. 2011, 364, 11–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitt, B.; Remme, W.; Zannad, F.; Neaton, J.; Martinez, F.; Roniker, B.; Bittman, R.; Hurley, S.; Kleiman, J.; Gatlin, M. Eplerenone, a Selective Aldosterone Blocker, in Patients with Left Ventricular Dysfunction after Myocardial Infarction. N. Engl. J. Med. 2003, 348, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- Stavros, F.; Yang, A.; Leon, A.; Nuttall, M.; Rasmussen, H.S. Characterization of Structure and Function of ZS-9, a K+ Selective Ion Trap. PLoS ONE 2014, 9, e114686. [Google Scholar]
- Imamura, T.; Oshima, A.; Narang, N.; Ushijima, R.; Ueno, Y.; Ueno, H.; Kinugawa, K. Combination Therapy Using Sodium Zirconium Cyclosilicate and a Mineralocorticoid Receptor Antagonist in Patients with Heart Failure and Hyperkalemia. Int. Med. 2021, 60, 2093–2095. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Hsu, B.; Maeda, Y.; Shin, S.K.; Vishneva, E.M.; Rensfeldt, M.; Eklund, S.; Zhao, J. Efficacy and safety of sodium zirconium cyclosilicate for hyperkalaemia: The randomized, placebo-controlled HARMONIZE-Global study. ESC Hear. Fail. 2020, 7, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Oshima, A.; Imamura, T.; Narang, N.; Kinugawa, K. Management of hyperkalemia in chronic heart failure using sodium zirconium cyclosilicate. Clin. Cardiol. 2021, 44, 1272–1275. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Isobe, M.; Ito, H.; Okumura, K.; Ono, M.; Kitakaze, M.; Kinugawa, K.; Kihara, Y.; Goto, Y.; Komuro, I.; et al. JCS 2017/JHFS 2017 Guideline on Diagnosis and Treatment of Acute and Chronic Heart Failure―Digest Version. Circ. J. 2019, 83, 2084–2184. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| n = 24 | |
|---|---|
| Demographics | |
| Age, years | 77 (68, 86) |
| Men | 17 (71%) |
| Body mass index, kg/m2 | 21.7 (19.1, 23.0) |
| Comorbidity | |
| Hypertension | 16 (67%) |
| Atrial fibrillation | 7 (29%) |
| Diabetes mellitus | 9 (38%) |
| Ischemic heart disease | 11 (46%) |
| Hemodynamics | |
| Systolic blood pressure, mmHg | 119 (107, 138) |
| Heart rate, bpm | 77 (67, 88) |
| Medication | |
| Beta-blocker, mg/day | 2.5 (0, 6.25) |
| Angiotensin-converting enzyme inhibitor, mg/day | 1.25 (0, 2.5) |
| Mineralocorticoid receptor antagonist, mg/day | 0 (0, 0) |
| Furosemide, mg/day | 10 (0, 20) |
| Laboratory data | |
| Hemoglobin, g/dL | 11.7 (10.9, 12.8) |
| Serum potassium, mEq/L | 5.5 (5.2, 5.8) |
| Serum sodium, mEq/L | 137 (134, 140) |
| eGFR, mL/min/1.73 m2 | 34.7 (24.0, 48.0) |
| Serum total bilirubin, mg/dL | 1.2 (0.8, 1.5) |
| Serum C-reactive protein, mg/dL | 0.6 (0.2, 0.9) |
| Plasma B-type natriuretic peptide, pg/mL | 200 (131, 322) |
| Echocardiography | |
| Left ventricular end-diastolic diameter, mm | 51 (45, 58) |
| Left ventricular ejection fraction, % | 41 (32, 46) |
| Left atrial diameter, mm | 41 (35, 44) |
| Six-minute walk distance, m | 325 (285, 351) |
| Pre 3 Months | Baseline | Post 3 Months | p Value | |
|---|---|---|---|---|
| Beta-blocker | 15 (63%) | 17 (71%) | 17 (71%) | 0.37 |
| Angiotensin converting enzyme II inhibitor | 10 (42%) | 14 (58%) | 18 (75%) † | 0.008 * |
| Mineralocorticoid receptor antagonist | 5 (21%) | 5 (21%) | 7 (27%) † | 0.008 * |
| Loop diuretics | 11 (46%) | 13 (54%) | 15 (63%) | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, T.; Oshima, A.; Narang, N.; Kinugawa, K. Clinical Implications of Sodium Zirconium Cyclosilicate Therapy in Patients with Systolic Heart Failure and Hyperkalemia. J. Clin. Med. 2021, 10, 5523. https://doi.org/10.3390/jcm10235523
Imamura T, Oshima A, Narang N, Kinugawa K. Clinical Implications of Sodium Zirconium Cyclosilicate Therapy in Patients with Systolic Heart Failure and Hyperkalemia. Journal of Clinical Medicine. 2021; 10(23):5523. https://doi.org/10.3390/jcm10235523
Chicago/Turabian StyleImamura, Teruhiko, Akira Oshima, Nikhil Narang, and Koichiro Kinugawa. 2021. "Clinical Implications of Sodium Zirconium Cyclosilicate Therapy in Patients with Systolic Heart Failure and Hyperkalemia" Journal of Clinical Medicine 10, no. 23: 5523. https://doi.org/10.3390/jcm10235523
APA StyleImamura, T., Oshima, A., Narang, N., & Kinugawa, K. (2021). Clinical Implications of Sodium Zirconium Cyclosilicate Therapy in Patients with Systolic Heart Failure and Hyperkalemia. Journal of Clinical Medicine, 10(23), 5523. https://doi.org/10.3390/jcm10235523