
Risk Factors for Pulmonary Embolism in Patients with Paralysis and Deep Venous Thrombosis

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Methods and Patients
2.1. Study Endpoints
2.2. Ethical Aspects and Study Oversight
3. Statistics
4. Results
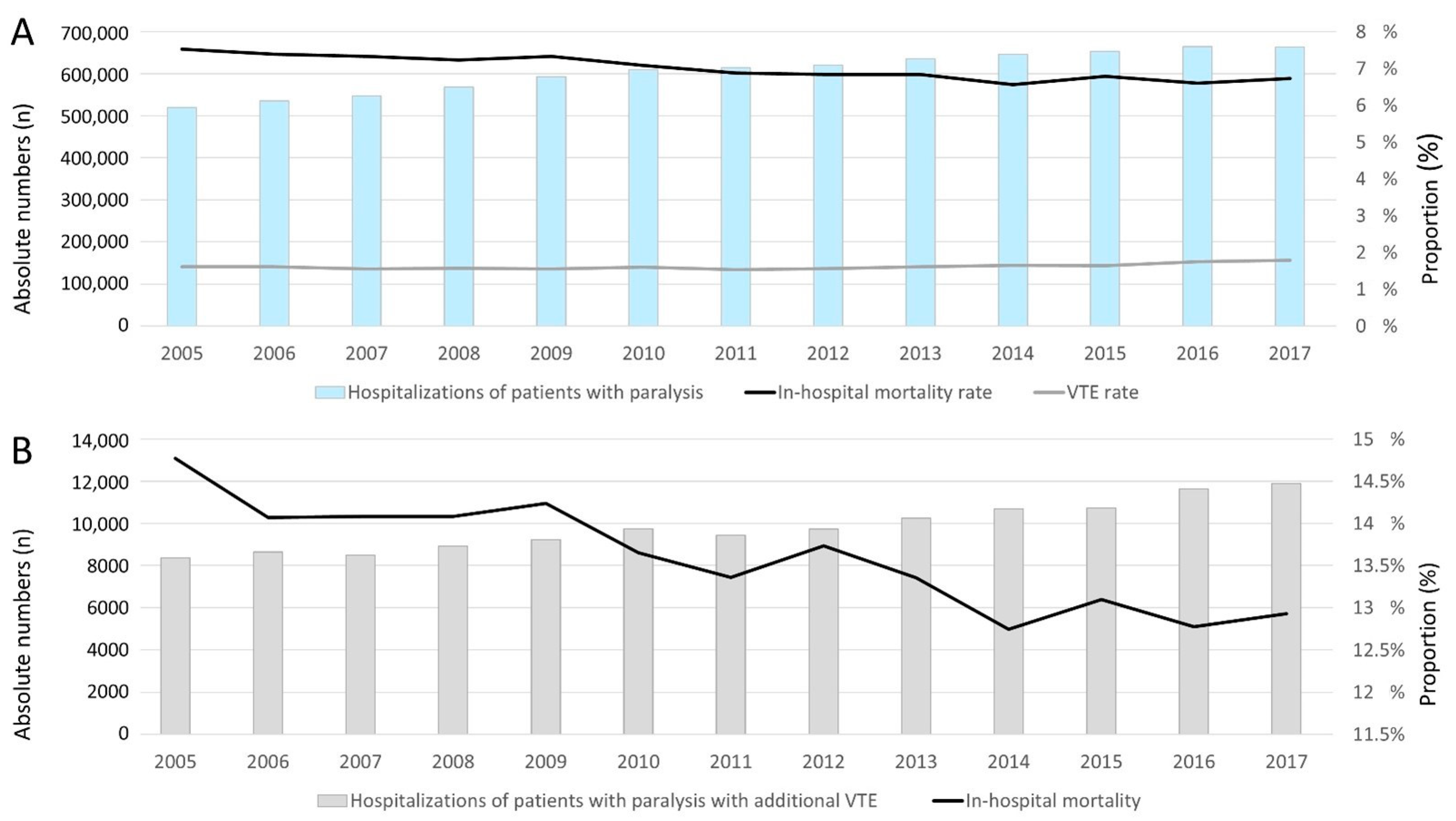
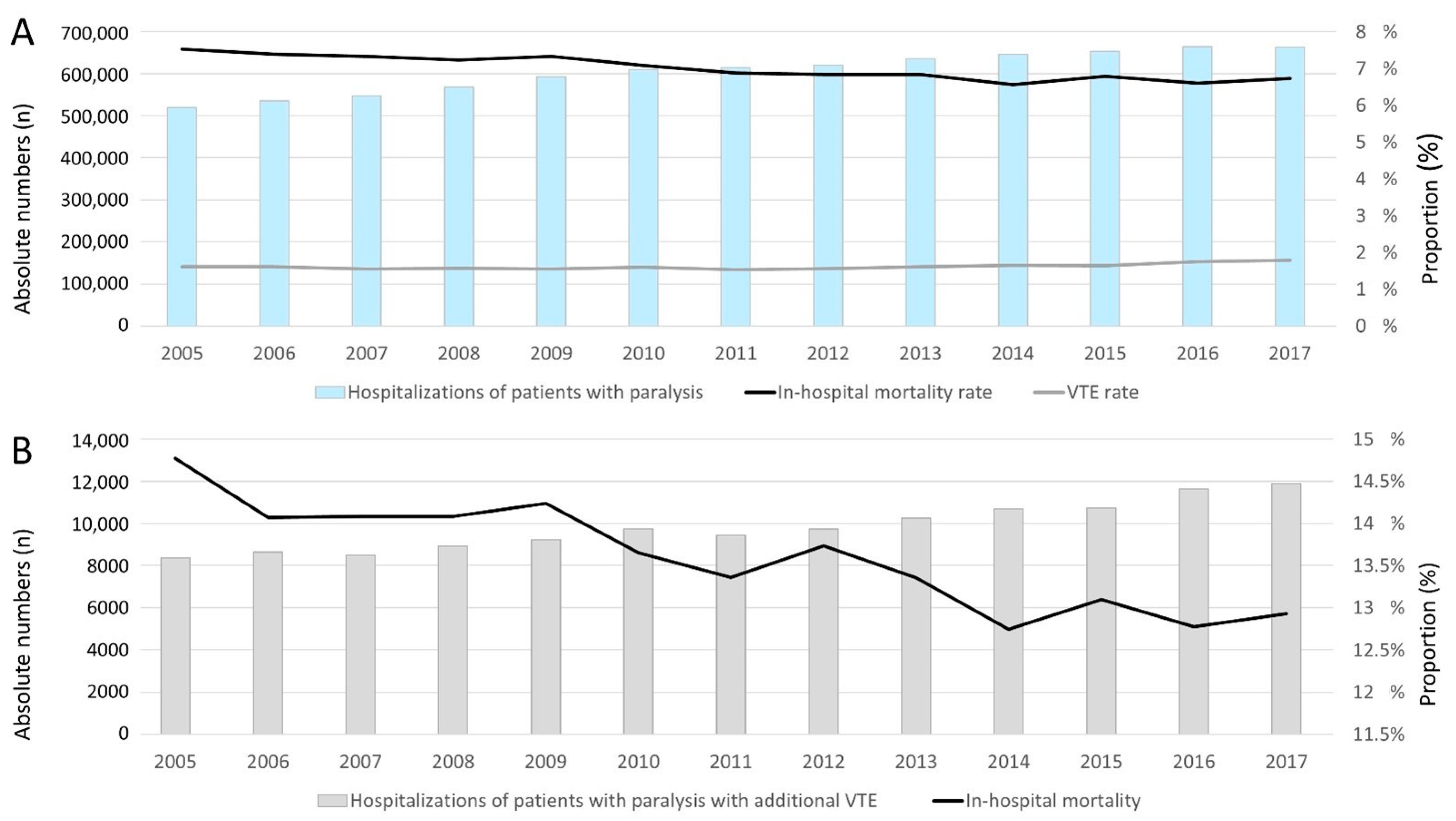
4.1. Time-Trends Regarding Hospitalizations of Patients with Paralysis with and without VTE
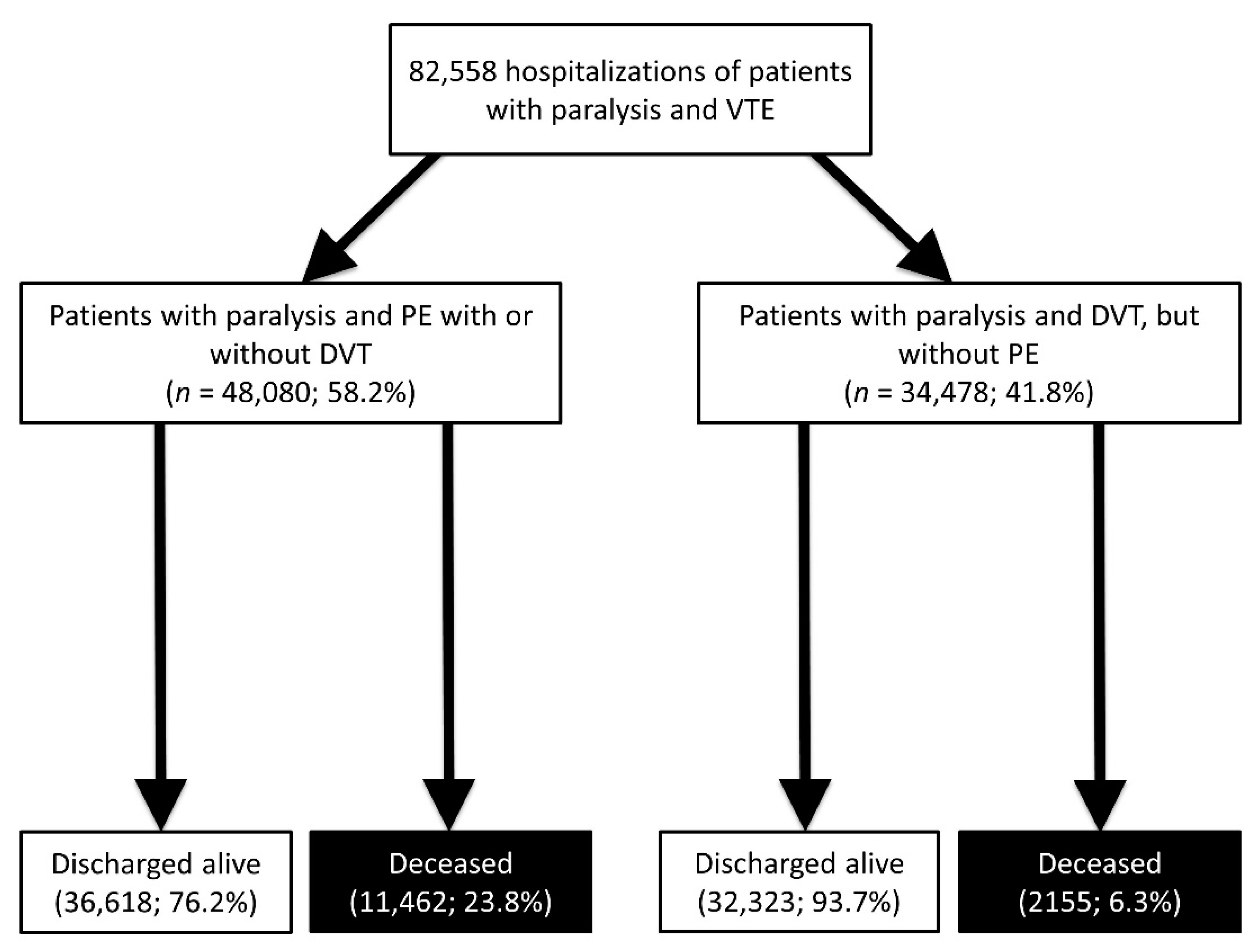
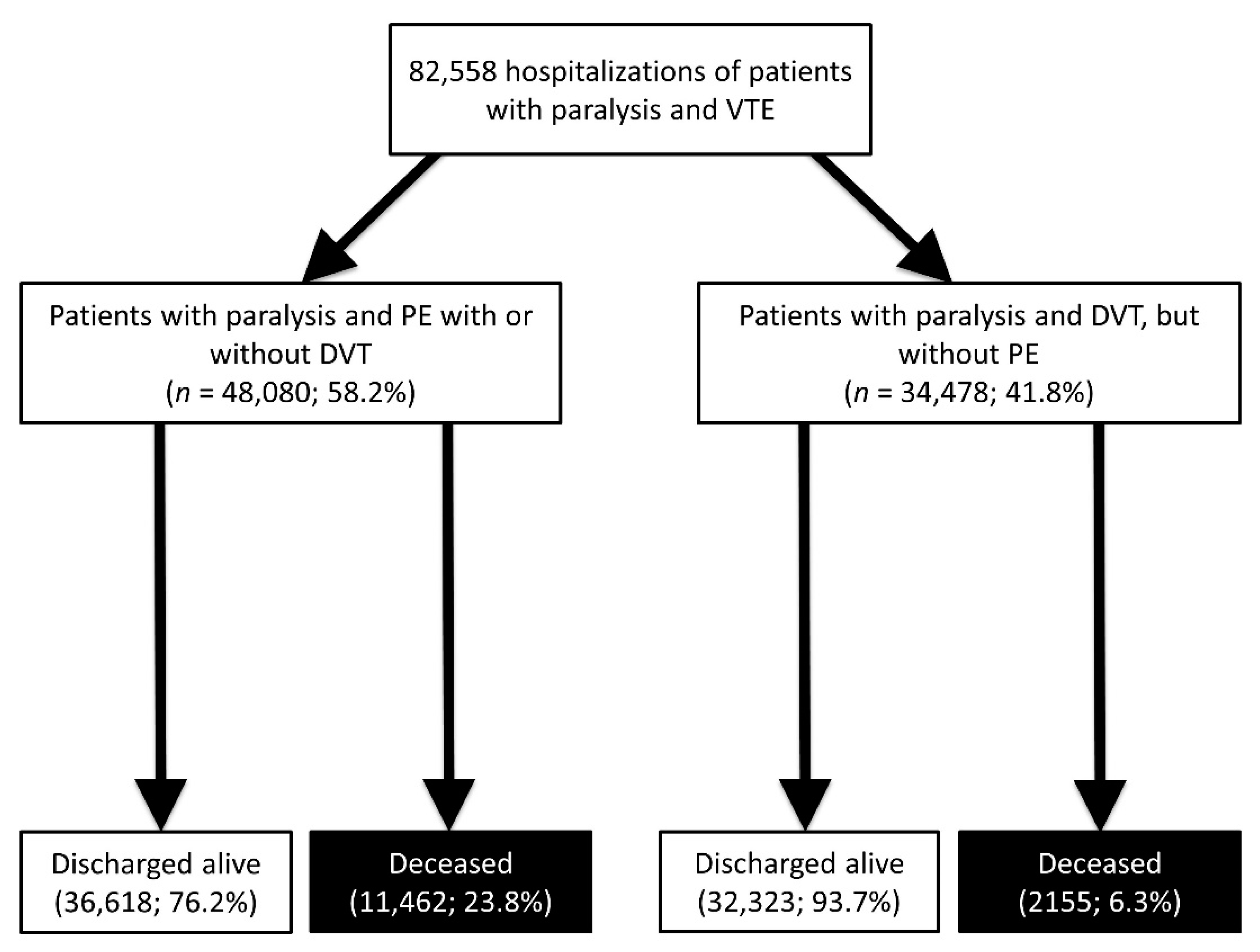
4.2. Comparison of Patients with Paralysis in Co-Prevalence with Isolated DVT (without PE) and Patients with Paralysis in Co-Prevalence with PE (with or without DVT)
4.3. Risk Factors for Occurrence of PE in Patients with Paralysis and VTE
4.4. Differences between Patients with Paralysis and VTE Who Died during Hospitalization and Those Who Were Discharged Alive
4.5. Predictors of In-Hospital Death in Patients with Paralysis and VTE
5. Discussion
- In total, 7,873,769 hospitalizations of patients with paralysis were recorded in the German nationwide inpatient sample with an increase in the total annual number from 2005 to 2017.
- Among these patients, 7.0% died during the observational period, and this rate decreased during the observational period.
- Overall, 1.6% of all hospitalized patients with paralysis had or developed an event of VTE.
- The in-hospital mortality rate was 13.5% in patients with paralysis and VTE.
- Cancer, heart failure, COPD, and obesity were important and independent risk factors for PE in patients with paralysis and VTE, whereas peripheral artery disease, arterial hypertension and hyperlipidaemia as well as stroke were independently associated with paralysis in co-prevalence with DVT only.
- Acute forms of paraplegia were strongly associated with PE in paralysis.
- Independent predictors of in-hospital death in patients with paralysis and VTE were PE, shock, age ≥ 70 years, cancer, heart failure, acute and chronic kidney disease, stroke as well as all bleeding events.
5.1. Prevalence of Hospitalizations of Patients with Paralysis
5.2. Main Causes of Paralysis
5.3. Prevalence of VTE in Hospitalizations of Patients with Paralysis
5.4. PE Is Related to a High Risk of In-Hospital Mortality in Patients with Paralysis
5.5. Predictors of PE in Patients with Paralysis
5.6. In-Hospital Mortality Rate of Patients with Paralysis
5.7. Impact of VTE on Survival of Patients with Paralysis
5.8. Independent Predictors of In-Hospital Death in Patients with Paralysis and VTE
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence Interval |
| DVT | Deep vein thrombosis and thrombophlebitis of the leg veins |
| DRG | Diagnosis-Related Groups |
| ICD | International Classification of Disease |
| IQR | Interquartile range |
| OPS | Surgery and interventional procedure keys (Operationen- und Prozedurenschlüssel) |
| OR | Odds ratio |
| PE | Pulmonary Embolism |
| RVD | Right ventricular dysfunction |
| VTE | Venous thromboembolism |
References
- Kelly, J.; Rudd, A.; Lewis, R.; Hunt, B.J. Venous thromboembolism after acute stroke. Stroke 2001, 32, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Warlow, C.; Ogston, D.; Douglas, A.S. Deep venous thrombosis of the legs after strokes: Part 2-Natural history. Br. Med. J. 1976, 1, 1181–1183. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.; Rudd, T.; Lewis, R.R.; Hunt, B.J. Mortality from pulmonary embolism after acute stroke: Can we do better? Age Ageing 2002, 31, 159–161. [Google Scholar] [CrossRef] [Green Version]
- Wijdicks, E.F.; Scott, J.P. Pulmonary embolism associated with acute stroke. Mayo Clin. Proc. 1997, 72, 297–300. [Google Scholar] [CrossRef]
- Sherman, D.G.; Albers, G.W.; Bladin, C.; Fieschi, C.; Gabbai, A.A.; Kase, C.S.; O’Riordan, W.; Pineo, G.F.; Investigators, P. The efficacy and safety of enoxaparin versus unfractionated heparin for the prevention of venous thromboembolism after acute ischaemic stroke (PREVAIL Study): An open-label randomised comparison. Lancet 2007, 369, 1347–1355. [Google Scholar] [CrossRef]
- Warlow, C.; Ogston, D.; Douglas, A.S. Deep venous thrombosis of the legs after strokes. Part I--incidence and predisposing factors. Br. Med. J. 1976, 1, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Hobohm, L.; Munzel, T.; Lankeit, M.; Ostad, M.A. Impact of pulmonary embolism on in-hospital mortality of patients with ischemic stroke. J. Neurol. Sci. 2020, 419, 117174. [Google Scholar] [CrossRef]
- Anderson, F.A., Jr.; Spencer, F.A. Risk factors for venous thromboembolism. Circulation 2003, 107, I9–I16. [Google Scholar] [CrossRef] [Green Version]
- Konstantinides, S.V.; Meyer, G. The 2019 ESC Guidelines on the Diagnosis and Management of Acute Pulmonary Embolism. Eur. Heart J. 2019, 40, 3453–3455. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Hobohm, L.; Barco, S.; Schmidtmann, I.; Munzel, T.; Engelhardt, M.; Goldhofer, M.; Konstantinides, S.V.; Drees, P. Venous thromboembolism in patients hospitalized for hip joint replacement surgery. Thromb. Res. 2020, 190, 1–7. [Google Scholar] [CrossRef]
- Keller, K.; Hobohm, L.; Barco, S.; Schmidtmann, I.; Munzel, T.; Engelhardt, M.; Eckhard, L.; Konstantinides, S.V.; Drees, P. Venous thromboembolism in patients hospitalized for knee joint replacement surgery. Sci. Rep. 2020, 10, 22440. [Google Scholar] [CrossRef]
- Torbicki, A.; Perrier, A.; Konstantinides, S.; Agnelli, G.; Galie, N.; Pruszczyk, P.; Bengel, F.; Brady, A.J.; Ferreira, D.; Janssens, U.; et al. Guidelines on the diagnosis and management of acute pulmonary embolism: The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur. Heart J. 2008, 29, 2276–2315. [Google Scholar]
- Konstantinides, S.V.; Torbicki, A.; Agnelli, G.; Danchin, N.; Fitzmaurice, D.; Galie, N.; Gibbs, J.S.; Huisman, M.V.; Humbert, M.; Kucher, N.; et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur. Heart J. 2014, 35, 3033–3080. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Hobohm, L.; Munzel, T.; Ostad, M.A. Impact of concomitant deep or superficial venous thrombosis of the legs on survival of patients with pulmonary embolism. Int. J. Cardiol. 2020, 315, 92–98. [Google Scholar] [CrossRef]
- Schwartz, T.; Hingorani, A.; Ascher, E.; Marks, N.; Shiferson, A.; Jung, D.; Jimenez, R.; Jacob, T. Pulmonary embolism without deep venous thrombosis. Ann. Vasc. Surg. 2012, 26, 973–976. [Google Scholar] [CrossRef]
- Sorensen, H.T.; Horvath-Puho, E.; Lash, T.L.; Christiansen, C.F.; Pesavento, R.; Pedersen, L.; Baron, J.A.; Prandoni, P. Heart disease may be a risk factor for pulmonary embolism without peripheral deep venous thrombosis. Circulation 2011, 124, 1435–1441. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Prochaska, J.H.; Coldewey, M.; Gobel, S.; Ullmann, A.; Junger, C.; Lamparter, H.; Ariza, L.; Bickel, C.; Lauterbach, M.; et al. History of deep vein thrombosis is a discriminator for concomitant atrial fibrillation in pulmonary embolism. Thromb. Res. 2015, 136, 899–906. [Google Scholar] [CrossRef]
- Ungprasert, P.; Sanguankeo, A.; Upala, S.; Suksaranjit, P. Psoriasis and risk of venous thromboembolism: A systematic review and meta-analysis. QJM 2014, 107, 793–797. [Google Scholar] [CrossRef] [Green Version]
- Dumic, I.; Martin, S.; Salfiti, N.; Watson, R.; Alempijevic, T. Deep Venous Thrombosis and Bilateral Pulmonary Embolism Revealing Silent Celiac Disease: Case Report and Review of the Literature. Case Rep. Gastrointest. Med. 2017, 2017, 5236918. [Google Scholar] [CrossRef]
- Keller, K.; Hobohm, L.; Ostad, M.A.; Karbach, S.; Espinola-Klein, C.; Munzel, T.; Gelfand, J.M.; Konstantinides, S.V.; Steinbrink, K.; Gori, T. Psoriasis and its impact on the clinical outcome of patients with pulmonary embolism. Int. J. Cardiol. 2021, 343, 114–121. [Google Scholar] [CrossRef]
- Chung, W.S.; Lin, C.L. Increased risks of venous thromboembolism in patients with psoriasis. A Nationwide Cohort Study. Thromb. Haemost. 2017, 117, 1637–1643. [Google Scholar]
- Ogdie, A.; Kay McGill, N.; Shin, D.B.; Takeshita, J.; Jon Love, T.; Noe, M.H.; Chiesa Fuxench, Z.C.; Choi, H.K.; Mehta, N.N.; Gelfand, J.M. Risk of venous thromboembolism in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: A general population-based cohort study. Eur. Heart J. 2018, 39, 3608–3614. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.J.; Pope, J.E. A meta-analysis of the risk of venous thromboembolism in inflammatory rheumatic diseases. Arthritis Res. 2014, 16, 435. [Google Scholar] [CrossRef] [Green Version]
- Zoller, B.; Li, X.; Sundquist, J.; Sundquist, K. Risk of pulmonary embolism in patients with autoimmune disorders: A nationwide follow-up study from Sweden. Lancet 2012, 379, 244–249. [Google Scholar] [CrossRef]
- Johannesdottir, S.A.; Schmidt, M.; Horvath-Puho, E.; Sorensen, H.T. Autoimmune skin and connective tissue diseases and risk of venous thromboembolism: A population-based case-control study. J. Thromb. Haemost. 2012, 10, 815–821. [Google Scholar] [CrossRef]
- Yuhara, H.; Steinmaus, C.; Corley, D.; Koike, J.; Igarashi, M.; Suzuki, T.; Mine, T. Meta-analysis: The risk of venous thromboembolism in patients with inflammatory bowel disease. Aliment. Pharm. 2013, 37, 953–962. [Google Scholar] [CrossRef]
- Grainge, M.J.; West, J.; Card, T.R. Venous thromboembolism during active disease and remission in inflammatory bowel disease: A cohort study. Lancet 2010, 375, 657–663. [Google Scholar] [CrossRef]
- Reinohl, J.; Kaier, K.; Reinecke, H.; Schmoor, C.; Frankenstein, L.; Vach, W.; Cribier, A.; Beyersdorf, F.; Bode, C.; Zehender, M. Effect of Availability of Transcatheter Aortic-Valve Replacement on Clinical Practice. N. Engl. J. Med. 2015, 373, 2438–2447. [Google Scholar] [CrossRef]
- Keller, K.; Munzel, T.; Hobohm, L.; Ostad, M.A. Predictive value of the Kuijer score for bleeding and other adverse in-hospital events in patients with venous thromboembolism. Int. J. Cardiol. 2021, 329, 179–184. [Google Scholar] [CrossRef]
- Keller, K.; Geyer, M.; Munzel, T.; Ostad, M.A.; Gori, T. Impact of atrial fibrillation on in-hospital mortality of ischemic stroke patients and identification of promoting factors of atrial thrombi—Results from the German nationwide inpatient sample and a single-center retrospective cohort. Medicine 2019, 98, e14086. [Google Scholar] [CrossRef]
- InEK GmbH–Institut für das Entgeltsystem im Krankenhaus. Deutsche Kodierrichtlinien 2018 Druckversion A4 (PDF). 2018. Available online: https://www.g-drg.de/inek_site_de/layout/set/standard/Media/Files/G-DRG-System/G-DRG-System_2018/Deutsche_Kodierrichtlinien_2018_Druckversion_A4_PDF (accessed on 5 June 2020).
- Keller, K.; Hobohm, L.; Ebner, M.; Kresoja, K.P.; Munzel, T.; Konstantinides, S.V.; Lankeit, M. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur. Heart J. 2020, 41, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Hobohm, L.; Munzel, T.; Ostad, M.A. Impact of symptomatic atherosclerosis in patients with pulmonary embolism. Int. J. Cardiol. 2019, 278, 225–231. [Google Scholar] [CrossRef]
- Armour, B.S.; Courtney-Long, E.A.; Fox, M.H.; Fredine, H.; Cahill, A. Prevalence and Causes of Paralysis-United States, 2013. Am. J. Public Health 2016, 106, 1855–1857. [Google Scholar] [CrossRef]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Weidner, N.; Muller, O.J.; Hach-Wunderle, V.; Schwerdtfeger, K.; Krauspe, R.; Pauschert, R.; Waydhas, C.; Baumberger, M.; Goggelmann, C.; Wittgruber, G.; et al. Prevention of thromboembolism in spinal cord injury-S1 guideline. Neurol. Res. Pract. 2020, 2, 43. [Google Scholar] [CrossRef]
- Agarwal, N.K.; Mathur, N. Deep vein thrombosis in acute spinal cord injury. Spinal Cord. 2009, 47, 769–772. [Google Scholar] [CrossRef] [Green Version]
- Prandoni, P. Venous and arterial thrombosis: Two aspects of the same disease? Eur. J. Intern. Med. 2009, 20, 660–661. [Google Scholar] [CrossRef] [Green Version]
- Prandoni, P.; Bilora, F.; Marchiori, A.; Bernardi, E.; Petrobelli, F.; Lensing, A.W.; Prins, M.H.; Girolami, A. An association between atherosclerosis and venous thrombosis. N. Engl. J. Med. 2003, 348, 1435–1441. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, H.T.; Horvath-Puho, E.; Pedersen, L.; Baron, J.A.; Prandoni, P. Venous thromboembolism and subsequent hospitalisation due to acute arterial cardiovascular events: A 20-year cohort study. Lancet 2007, 370, 1773–1779. [Google Scholar] [CrossRef]
- Libertiny, G.; Hands, L. Deep venous thrombosis in peripheral vascular disease. Br. J. Surg. 1999, 86, 907–910. [Google Scholar] [CrossRef]
- Keller, K.; Hobohm, L.; Munzel, T.; Lankeit, M.; Konstantinides, S.; Ostad, M.A. Impact of Systemic Atherosclerosis on Clinical Characteristics and Short-term Outcomes in Patients with Deep Venous Thrombosis or Thrombophlebitis. Am. J. Med. Sci. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Rafi, S.; van Doormaal, F.F.; van Lienden, K.P.; Kamphuisen, P.W.; Gerdes, V.E. Venous thrombo-embolism and aortic calcifications; more evidence on the link between venous and arterial thrombosis. Thromb. Res. 2009, 124, 381–382. [Google Scholar] [CrossRef]
- Hong, C.; Zhu, F.; Du, D.; Pilgram, T.K.; Sicard, G.A.; Bae, K.T. Coronary artery calcification and risk factors for atherosclerosis in patients with venous thromboembolism. Atherosclerosis 2005, 183, 169–174. [Google Scholar] [CrossRef]
- Prandoni, P. Links between arterial and venous disease. J. Intern. Med. 2007, 262, 341–350. [Google Scholar] [CrossRef]
- Clements, R.; Churilov, L.; Wahab, A.L.; Ng, L.C. Exploratory analysis of factors associated with venous thromboembolism in Victorian acute traumatic spinal cord-injured patients 2010–2013. Spinal Cord 2017, 55, 74–78. [Google Scholar] [CrossRef]
- Alvarez Sabin, J. In-hospital mortality in stroke patients. Rev. Esp. Cardiol. 2008, 61, 1007–1009. [Google Scholar]
- Heuschmann, P.U.; Kolominsky-Rabas, P.L.; Misselwitz, B.; Hermanek, P.; Leffmann, C.; Janzen, R.W.; Rother, J.; Buecker-Nott, H.J.; Berger, K.; German Stroke Registers Study, G. Predictors of in-hospital mortality and attributable risks of death after ischemic stroke: The German Stroke Registers Study Group. Arch. Intern. Med. 2004, 164, 1761–1768. [Google Scholar] [CrossRef] [Green Version]
- Koennecke, H.C.; Belz, W.; Berfelde, D.; Endres, M.; Fitzek, S.; Hamilton, F.; Kreitsch, P.; Mackert, B.M.; Nabavi, D.G.; Nolte, C.H.; et al. Factors influencing in-hospital mortality and morbidity in patients treated on a stroke unit. Neurology 2011, 77, 965–972. [Google Scholar] [CrossRef]
- Chamberlain, J.D.; Meier, S.; Mader, L.; von Groote, P.M.; Brinkhof, M.W. Mortality and longevity after a spinal cord injury: Systematic review and meta-analysis. Neuroepidemiology 2015, 44, 182–198. [Google Scholar] [CrossRef]
- Yeo, J.D.; Walsh, J.; Rutkowski, S.; Soden, R.; Craven, M.; Middleton, J. Mortality following spinal cord injury. Spinal Cord 1998, 36, 329–336. [Google Scholar] [CrossRef] [Green Version]
- White, R.H. The epidemiology of venous thromboembolism. Circulation 2003, 107, I4–I8. [Google Scholar] [CrossRef] [Green Version]
- Dean, S.M.; Abraham, W. Venous thromboembolic disease in congestive heart failure. Congest. Heart Fail. 2010, 16, 164–169. [Google Scholar] [CrossRef]
- Goldhaber, S.Z. Venous Thromboembolism in Heart Failure Patients: Pathophysiology, Predictability, Prevention. J. Am. Coll. Cardiol. 2020, 75, 159–162. [Google Scholar] [CrossRef]
- Khorana, A.A. Venous thromboembolism and prognosis in cancer. Thromb. Res. 2010, 125, 490–493. [Google Scholar] [CrossRef] [Green Version]
- Goto, S.; Haas, S.; Ageno, W.; Goldhaber, S.Z.; Turpie, A.G.G.; Weitz, J.I.; Angchaisuksiri, P.; Nielsen, J.D.; Kayani, G.; Farjat, A.; et al. Assessment of Outcomes among Patients With Venous Thromboembolism with and without Chronic Kidney Disease. JAMA Netw. Open 2020, 3, e2022886. [Google Scholar] [CrossRef]
- Chhabra, H.S.; Sharawat, R.; Vishwakarma, G. In-hospital mortality in people with complete acute traumatic spinal cord injury at a tertiary care center in India-a retrospective analysis. Spinal Cord 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Claxton, A.R.; Wong, D.T.; Chung, F.; Fehlings, M.G. Predictors of hospital mortality and mechanical ventilation in patients with cervical spinal cord injury. Can. J. Anaesth. 1998, 45, 144–149. [Google Scholar] [CrossRef]
- Ovbiagele, B. Nationwide trends in in-hospital mortality among patients with stroke. Stroke 2010, 41, 1748–1754. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Parameters | Patients with Paralysis and PE with or without DVT (n = 48,080; 58.2%) | Patients with Paralysis and Isolated DVT (without PE) (n = 34,478; 41.8%) | p-Value |
|---|---|---|---|
| Median age (years) | 73.00 (62.00–80.00) | 74.00 (63.00–81.00) | <0.001 |
| Age ≥ 70 years | 27,337 (56.9%) | 20,781 (60.3%) | <0.001 |
| Gender (females) | 24,520 (51.0%) | 18,244 (52.9%) | <0.001 |
| In-hospital stay (days) | 15 (8–28) | 12 (7–22) | <0.001 |
| Obesity | 4586 (9.5%) | 2465 (7.1%) | <0.001 |
| Acute paraplegia and infantile cerebral palsy | |||
| Acute complete or incomplete paraplegia | 1337 (2.8%) | 88 (0.3%) | <0.001 |
| Acute complete paraplegia | 354 (0.7%) | 29 (0.1%) | <0.001 |
| Acute incomplete paraplegia | 1002 (2.1%) | 60 (0.2%) | <0.001 |
| Infantile cerebral palsy | 346 (0.7%) | 312 (0.9%) | 0.003 |
| VTE risk factors | |||
| Surgery during in-hospital stay | 30,237 (62.9%) | 18,188 (52.8%) | <0.001 |
| Cancer | 9589 (19.9%) | 3509 (10.2%) | <0.001 |
| Inflammatory bowel disease | 273 (0.6%) | 189 (0.5%) | 0.710 |
| Thrombophilia | 411 (0.8%) | 271 (0.8%) | 0.282 |
| Comorbidities | |||
| Heart failure | 11,512 (23.9%) | 5162 (14.9%) | <0.001 |
| Coronary artery disease | 7479 (15.6%) | 5198 (15.1%) | 0.060 |
| Cardiomyopathy | 711 (1.5%) | 385 (1.1%) | <0.001 |
| Peripheral artery disease | 1994 (4.1%) | 1814 (5.3%) | <0.001 |
| Chronic obstructive pulmonary disease | 4334 (9.0%) | 1923 (5.6%) | <0.001 |
| Arterial hypertension | 24,310 (50.6%) | 19,732 (57.2%) | <0.001 |
| Hyperlipidaemia | 7731 (16.1%) | 8174 (23.7%) | <0.001 |
| Acute and chronic kidney disease | 11,091 (23.1%) | 6459 (18.7%) | <0.001 |
| Diabetes mellitus | 12,468 (25.9%) | 9141 (26.5%) | 0.061 |
| Deep venous thrombosis or thrombophlebitis | 14,224 (29.6%) | 34,478 (100.0%) | <0.001 |
| Atrial fibrillation/flutter | 11,775 (24.5%) | 8568 (24.9%) | 0.236 |
| Risk stratification markers | |||
| Right ventricular dysfunction | 14,702 (30.6%) | 0 (0.0%) | <0.001 |
| Syncope | 876 (1.8%) | 255 (0.7%) | <0.001 |
| Adverse events during the in-hospital stay | |||
| All cause in-hospital death | 11,462 (23.8%) | 2155 (6.3%) | <0.001 |
| Stroke | 16,456 (34.2%) | 20,617 (59.8%) | <0.001 |
| Myocardial injury | 1742 (3.6%) | 768 (2.2%) | <0.001 |
| Shock | 2611 (5.4%) | 520 (1.5%) | <0.001 |
| Cardio-pulmonary resuscitation | 4087 (8.5%) | 329 (1.0%) | <0.001 |
| Intracerebral bleeding | 3442 (7.1%) | 1094 (3.2%) | <0.001 |
| Subarachnoid hemorrhage | 592 (1.2%) | 462 (1.3%) | 0.169 |
| Gastro-intestinal bleeding | 1026 (2.1%) | 469 (1.4%) | <0.001 |
| Reperfusion treatments and transfusion of blood constituents | |||
| Systemic thrombolysis | 3086 (6.4%) | 2174 (6.3%) | 0.512 |
| Transfusion of blood constituents | 8679 (18.1%) | 3202 (9.3%) | <0.001 |
| Uni-Variate Regression Model | Multi-Variate Regression Model | |||
|---|---|---|---|---|
| Parameters | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age | 0.995 (0.994–0.996) | <0.001 | 0.994 (0.993–0.996) | <0.001 |
| Age ≥ 70 years | 0.87 (0.85–0.89) | <0.001 | 0.87 (0.84–0.90) | <0.001 |
| Gender (females) | 0.93 (0.90–0.95) | <0.001 | 0.96 (0.94–0.99) | 0.011 |
| Obesity | 1.37 (1.30–1.44) | <0.001 | 1.42 (1.35–1.50) | <0.001 |
| Acute paraplegia and infantile cerebral Palsy | ||||
| Acute complete or incomplete paraplegia | 11.18 (9.00–13.87) | <0.001 | 9.80 (7.89–12.18) | <0.001 |
| Acute complete paraplegia | 8.81 (6.03–12.87) | <0.001 | 7.55 (5.15–11.06) | <0.001 |
| Acute incomplete paraplegia | 12.21 (9.40–15.84) | <0.001 | 10.77 (8.29–14.01) | <0.001 |
| Infantile cerebral palsy | 0.79 (0.68–0.93) | 0.003 | 0.73 (0.62–0.85) | <0.001 |
| VTE risk factors | ||||
| Surgery during in-hospital stay | 1.52 (1.48–1.56) | <0.001 | 1.44 (1.40–1.48) | <0.001 |
| Cancer | 2.20 (2.11–2.29) | <0.001 | 2.18 (2.09–2.27) | <0.001 |
| Inflammatory bowel disease | 1.04 (0.86–1.25) | 0.710 | 0.99 (0.82–1.20) | 0.918 |
| Thrombophilia | 1.09 (0.93–1.27) | 0.282 | 1.04 (0.89–1.22) | 0.642 |
| Comorbidities | ||||
| Heart failure | 1.79 (1.72–1.85) | <0.001 | 1.83 (1.76–1.91) | <0.001 |
| Coronary artery disease | 1.04 (1.00–1.08) | 0.060 | 1.01 (0.97–1.05) | 0.617 |
| Cardiomyopathy | 1.33 (1.17–1.51) | <0.001 | 1.06 (0.93–1.20) | 0.414 |
| Chronic obstructive pulmonary disease | 1.68 (1.59–1.77) | <0.001 | 1.63 (1.53–1.72) | <0.001 |
| Hyperlipidaemia | 0.62 (0.60–0.64) | <0.001 | 0.65 (0.63–0.68) | <0.001 |
| Arterial hypertension | 0.76 (0.74–0.79) | <0.001 | 0.88 (0.86–0.91) | <0.001 |
| Acute and chronic kidney disease | 1.30 (1.26–1.35) | <0.001 | 1.24 (1.20–1.29) | <0.001 |
| Diabetes mellitus | 0.97 (0.94–1.00) | 0.061 | 0.97 (0.94–1.01) | 0.123 |
| Peripheral artery disease | 0.78 (0.73–0.83) | <0.001 | 0.75 (0.70–0.80) | <0.001 |
| Atrial fibrillation/flutter | 0.98 (0.95–1.01) | 0.236 | 0.96 (0.93–1.00) | 0.034 |
| Stroke (ischemic and hemorrhagic) | 0.35 (0.34–0.36) | <0.001 | 0.36 (0.35–0.37) | <0.001 |
| Parameters | Patients with Paralysis and VTE, Who Died IN-Hospital (n = 13,617; 16.5%) | Patients with Paralysis and VTE, Who Were Discharged Alive (n = 68,941; 83.5%) | p-Value |
|---|---|---|---|
| Median age (years) | 75.0 (66.0–82.0) | 73.0 (62.0–80.0) | <0.001 |
| Age ≥ 70 years | 8801 (64.6%) | 39,317 (57.0%) | <0.001 |
| Gender (females) | 6953 (51.1%) | 35,811 (51.9%) | 0.059 |
| In-hospital stay (days) | 10 (4–21) | 15 (8–27) | <0.001 |
| Obesity | 997 (7.3%) | 6054 (8.8%) | <0.001 |
| Paraplegia and infantile cerebral palsy | |||
| Acute complete or incomplete paraplegia | 255 (1.9%) | 1170 (1.7%) | 0.141 |
| Acute complete paraplegia | 85 (0.6%) | 298 (0.4%) | 0.002 |
| Acute incomplete paraplegia | 173 (1.3%) | 889 (1.3%) | 0.880 |
| Infantile cerebral palsy | 95 (0.7%) | 563 (0.8%) | 0.160 |
| VTE risk factors | |||
| Surgery during in-hospital stay | 7635 (56.1%) | 40,790 (59.2%) | <0.001 |
| Cancer | 3340 (24.5%) | 9758 (14.2%) | <0.001 |
| Inflammatory bowel disease | 79 (0.6%) | 383 (0.6%) | 0.710 |
| Thrombophilia | 78 (0.6%) | 604 (0.9%) | <0.001 |
| Comorbidities | |||
| Heart failure | 3926 (28.7%) | 12,748 (18.4%) | <0.001 |
| Coronary artery disease | 2358 (17.3%) | 10,319 (15.0%) | <0.001 |
| Cardiomyopathy | 230 (1.7%) | 866 (1.2%) | <0.001 |
| Chronic obstructive pulmonary disease | 1298 (9.5%) | 4959 (7.2%) | <0.001 |
| Arterial hypertension | 6420 (47.1%) | 37,622 (54.6%) | <0.001 |
| Hyperlipidaemia | 1732 (12.7%) | 14,173 (20.6%) | <0.001 |
| Acute and chronic kidney disease | 4205 (30.9%) | 13,345 (19.4%) | <0.001 |
| Diabetes mellitus | 3995 (29.3%) | 17,614 (25.5%) | <0.001 |
| Pulmonary embolism | 11,462 (84.2%) | 36,618 (53.1%) | <0.001 |
| Deep venous thrombosis or thrombophlebitis | 4029 (29.6%) | 44,673 (64.8%) | <0.001 |
| Stroke | 6560 (48.2%) | 30,513 (44.3%) | <0.001 |
| Myocardial injury | 727 (5.3%) | 1783 (2.6%) | <0.001 |
| Atrial fibrillation/flutter | 4026 (29.6%) | 16,317 (23.7%) | <0.001 |
| Intracerebral bleeding | 1034 (7.6%) | 3502 (5.0%) | <0.001 |
| Subarachnoid hemorrhage | 170 (1.2%) | 884 (1.3%) | 0.770 |
| Gastro-intestinal bleeding | 411 (3.0%) | 1084 (1.6%) | <0.001 |
| Transfusion of blood constituents | 3233 (23.7%) | 8648 (12.5%) | <0.001 |
| Shock | 1557 (11.4%) | 1574 (2.3%) | <0.001 |
| Uni-Variate Regression Model | Multi-Variate Regression Model | |||
|---|---|---|---|---|
| Parameters | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age | 1.016 (1.015–1.017) | <0.001 | 1.016 (1.014–1.017) | <0.001 |
| Age ≥ 70 years | 1.38 (1.33–1.43) | <0.001 | 1.35 (1.29–1.41) | <0.001 |
| Gender (females) | 0.97 (0.93–1.00) | 0.059 | 0.90 (0.87–0.94) | <0.001 |
| Obesity | 0.82 (0.77–0.88) | <0.001 | 0.89 (0.82–0.95) | 0.001 |
| Paraplegia and infantile cerebral palsy | ||||
| Acute complete or incomplete paraplegia | 1.11 (0.97–1.27) | 0.141 | 0.99 (0.86–1.14) | 0.987 |
| Acute complete paraplegia | 1.45 (1.14–1.85) | 0.003 | 1.31 (1.02–1.68) | 0.037 |
| Acute incomplete paraplegia | 0.99 (0.84–1.16) | 0.880 | 0.88 (0.74–1.04) | 0.129 |
| Infantile cerebral palsy | 0.86 (0.69–1.06) | 0.160 | 1.25 (1.00–1.57) | 0.050 |
| VTE risk factors | ||||
| Surgery during in-hospital stay | 0.88 (0.85–0.91) | <0.001 | 0.83 (0.80–0.86) | <0.001 |
| Cancer | 1.97 (1.89–2.06) | <0.001 | 2.18 (2.08–2.28) | <0.001 |
| Inflammatory bowel disease | 1.05 (0.82–1.34) | 0.710 | 1.18 (0.92–1.51) | 0.199 |
| Thrombophilia | 0.65 (0.52–0.83) | <0.001 | 0.78 (0.61–0.99) | 0.043 |
| Comorbidities | ||||
| Heart failure | 1.79 (1.72–1.87) | <0.001 | 1.50 (1.43–1.57) | <0.001 |
| Coronary artery disease | 1.19 (1.13–1.25) | <0.001 | 1.04 (0.98–1.09) | 0.185 |
| Cardiomyopathy | 1.35 (1.17–1.57) | <0.001 | 1.17 (1.00–1.36) | 0.048 |
| Chronic obstructive pulmonary disease | 1.36 (1.28–1.45) | <0.001 | 1.21 (1.13–1.29) | <0.001 |
| Hyperlipidaemia | 0.56 (0.53–0.59) | <0.001 | 0.58 (0.54–0.61) | <0.001 |
| Arterial hypertension | 0.74 (0.72–0.77) | <0.001 | 0.76 (0.73–0.79) | <0.001 |
| Acute and chronic kidney disease | 1.86 (1.79–1.94) | <0.001 | 1.62 (1.55–1.69) | <0.001 |
| Diabetes mellitus | 1.21 (1.16–1.26) | <0.001 | 1.13 (1.09–1.18) | <0.001 |
| Pulmonary embolism | 4.70 (4.47–4.93) | <0.001 | 4.28 (4.07–4.50) | <0.001 |
| Peripheral artery disease | 1.46 (1.35–1.58) | <0.001 | 1.31 (1.21–1.43) | <0.001 |
| Atrial fibrillation/flutter | 1.35 (1.30–1.41) | <0.001 | 1.17 (1.12–1.22) | <0.001 |
| Stroke (ischemic and hemorrhagic) | 1.17 (1.13–1.22) | <0.001 | 1.32 (1.27–1.37) | <0.001 |
| Risk stratification parameters | ||||
| Syncope | 1.08 (0.92–1.26) | 0.340 | 0.98 (0.84–1.15) | 0.790 |
| Right ventricular dysfunction in PE | 4.94 (4.75–5.15) | <0.001 | 4.84 (4.64–5.05) | <0.001 |
| Shock | 5.46 (5.08–5.87) | <0.001 | 5.06 (4.69–5.46) | <0.001 |
| Adverse in-hospital events | ||||
| Intracerebral bleeding | 1.54 (1.43–1.65) | <0.001 | 1.85 (1.72–1.99) | <0.001 |
| Subarachnoid bleeding | 0.98 (0.83–1.15) | 0.770 | 1.39 (1.17–1.64) | <0.001 |
| Gastro-intestinal bleeding | 1.95 (1.74–2.19) | <0.001 | 1.66 (1.47–1.87) | <0.001 |
| Transfusion of blood constituents | 2.16 (2.07–2.26) | <0.001 | 1.90 (1.81–1.99) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keller, K.; Wöllner, J.; Schmitt, V.H.; Ostad, M.A.; Sagoschen, I.; Münzel, T.; Espinola-Klein, C.; Hobohm, L. Risk Factors for Pulmonary Embolism in Patients with Paralysis and Deep Venous Thrombosis. J. Clin. Med. 2021, 10, 5412. https://doi.org/10.3390/jcm10225412
Keller K, Wöllner J, Schmitt VH, Ostad MA, Sagoschen I, Münzel T, Espinola-Klein C, Hobohm L. Risk Factors for Pulmonary Embolism in Patients with Paralysis and Deep Venous Thrombosis. Journal of Clinical Medicine. 2021; 10(22):5412. https://doi.org/10.3390/jcm10225412
Chicago/Turabian StyleKeller, Karsten, Jens Wöllner, Volker H. Schmitt, Mir A. Ostad, Ingo Sagoschen, Thomas Münzel, Christine Espinola-Klein, and Lukas Hobohm. 2021. "Risk Factors for Pulmonary Embolism in Patients with Paralysis and Deep Venous Thrombosis" Journal of Clinical Medicine 10, no. 22: 5412. https://doi.org/10.3390/jcm10225412
APA StyleKeller, K., Wöllner, J., Schmitt, V. H., Ostad, M. A., Sagoschen, I., Münzel, T., Espinola-Klein, C., & Hobohm, L. (2021). Risk Factors for Pulmonary Embolism in Patients with Paralysis and Deep Venous Thrombosis. Journal of Clinical Medicine, 10(22), 5412. https://doi.org/10.3390/jcm10225412