
Long-Term Outcomes and Predictive Factors of Hospitalized Patients with Severe Ulcerative Colitis Treated with Intravenous Corticosteroids

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Outcome Measurement during Follow-Up
2.3. Statistical Analysis
3. Results
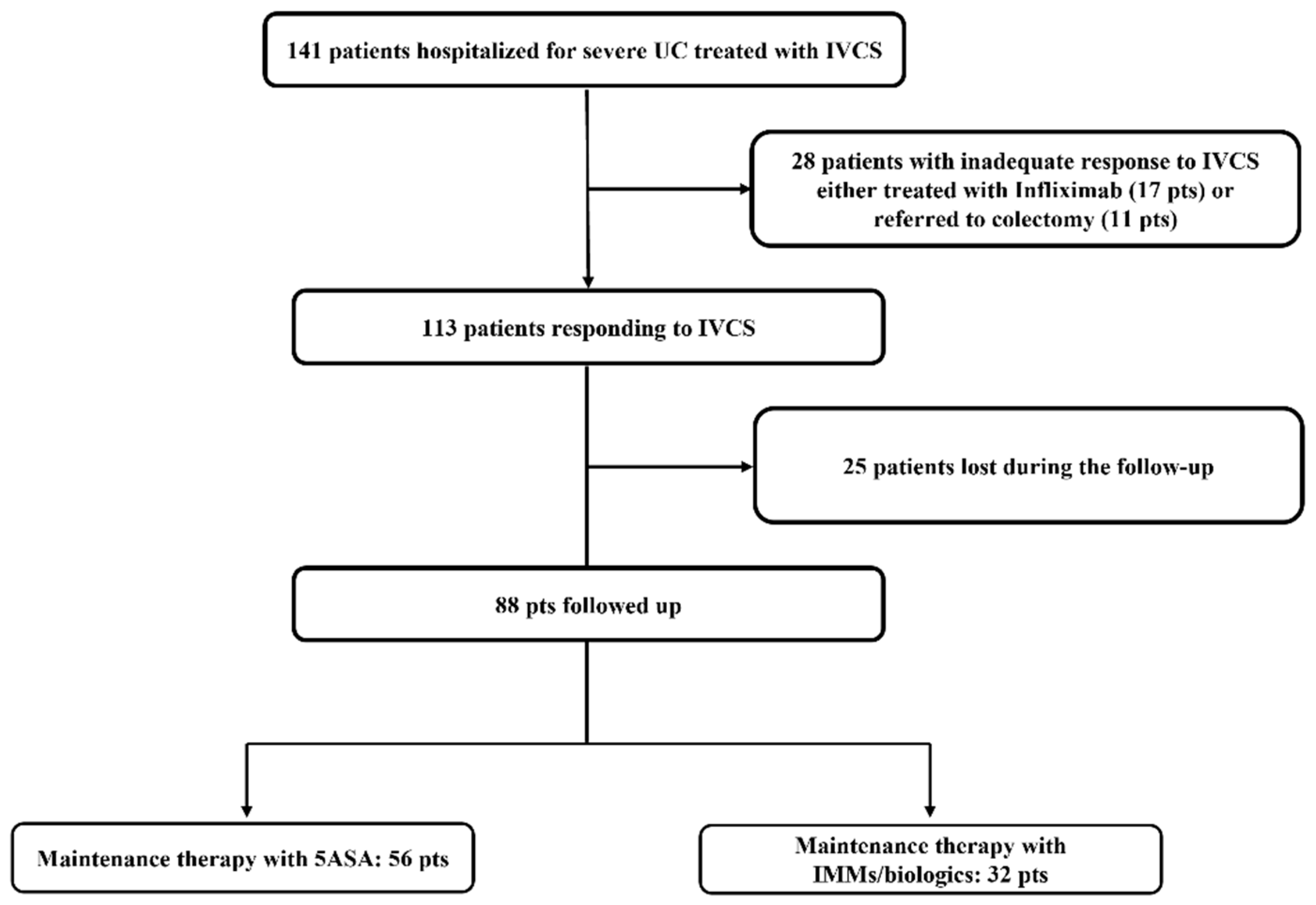
3.1. Study Population
3.2. Characteristics at Baseline of Patients Responding to IVCS and Maintenance Therapies
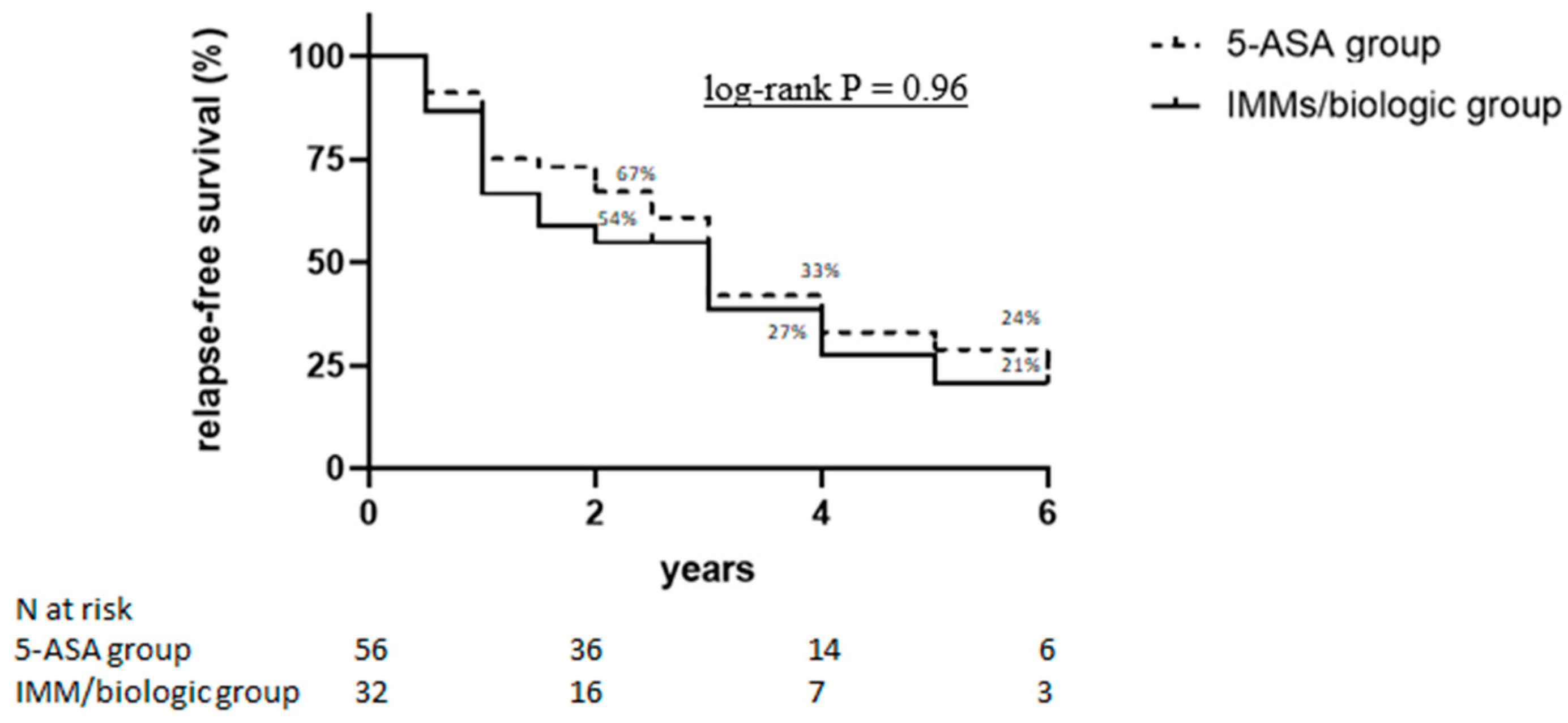
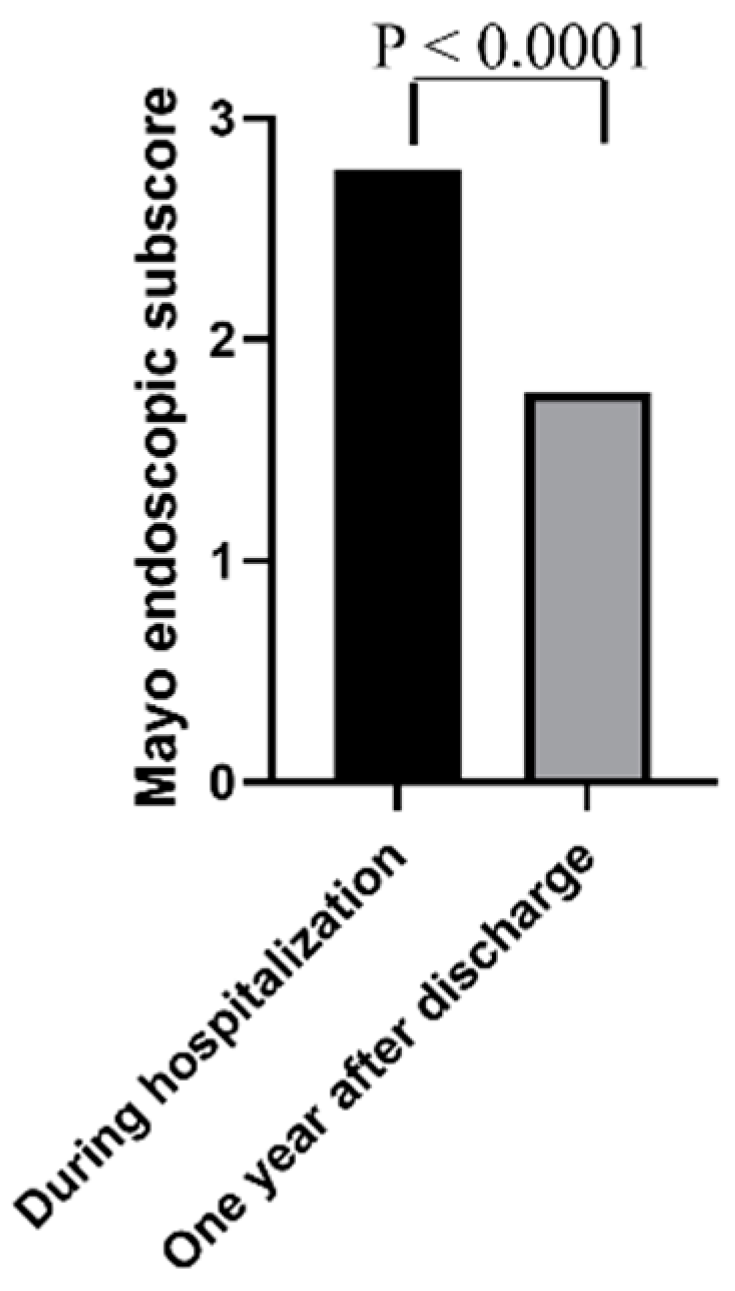
3.3. Long-Term Outcomes in Patients Responding to IVCS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Cosnes, J.; Gowerrousseau, C.; Seksik, P.; Cortot, A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 2011, 140, 1785–1794.e4. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G.; Windsor, J.W. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Dinesen, L.C.; Walsh, A.J.; Protic, M.N.; Heap, G.; Cummings, F.; Warren, B.F.; George, B.; Mortensen, N.J.; Travis, S.P. The pattern and outcome of acute severe colitis. J. Crohn’s Colitis 2010, 4, 431–437. [Google Scholar] [CrossRef]
- Turner, D.; Walsh, C.M.; Benchimol, E.; Mann, E.H.; E Thomas, K.; Chow, C.; A McLernon, R.; Walters, T.D.; Swales, J.; Steinhart, A.H.; et al. Severe paediatric ulcerative colitis: Incidence, outcomes and optimal timing for second-line therapy. Gut 2008, 57, 331–338. [Google Scholar] [CrossRef]
- Turner, D.; Walsh, C.M.; Steinhart, A.H.; Griffiths, A.M. Response to Corticosteroids in Severe Ulcerative Colitis: A Systematic Review of the Literature and a Meta-Regression. Clin. Gastroenterol. Hepatol. 2007, 5, 103–110. [Google Scholar] [CrossRef]
- Park, D. Cortisone in Ulcerative Colitis. Br. Med. J. 1955, 2, 1386. [Google Scholar] [CrossRef][Green Version]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: Definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J. Crohn’s Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Gionchetti, P.; Dignass, A.; Danese, S.; Dias, F.J.M.; Rogler, G.; Lakatos, P.L.; Adamina, M.; Ardizzone, S.; Buskens, C.J.; Sebastian, S.; et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: Part 2: Surgical management and special situations. J. Crohn’s Colitis 2017, 11, 135–149. [Google Scholar] [CrossRef]
- Lindgren, S.C.; Flood, L.M.; Kilander, A.F.; Löfberg, R.; Persson, T.B.; Sjödahl, R.I. Early predictors of glucocorticosteroid treatment failure in severe and moderately severe attacks of ulcerative colitis. Eur. J. Gastroenterol. Hepatol. 1998, 10, 831–835. [Google Scholar] [CrossRef]
- Ho, G.T.; Mowat, C.; Goddard, C.J.R.; Fennell, J.M.; Shah, N.B.; Prescott, R.J.; Satsangi, J. Predicting the outcome of severe ulcerative colitis: Development of a novel risk score to aid early selection of patients for second-line medical therapy or surgery. Aliment. Pharmacol. Ther. 2004, 19, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Travis, S.P.L. Predicting outcome in severe ulcerative colitis. Dig. Liver Dis. 2004, 36, 448–449. [Google Scholar] [CrossRef] [PubMed]
- Carbonnel, F.; Gargouri, D.; Lémann, M.; Beaugerie, L.; Cattan, S.; Cosnes, J.; Gendre, J.P. Predictive factors of outcome of intensive intravenous treatment for attacks of ulcerative colitis. Aliment. Pharmacol. Ther. 2000, 14, 273–279. [Google Scholar]
- Narula, N.; Marshall, J.K.; Colombel, J.-F.; Leontiadis, G.I.; Williams, J.G.; Muqtadir, Z.; Reinisch, W. Systematic review and meta-analysis: Infliximab or cyclosporine as rescue therapy in patients with severe ulcerative colitis refractory to steroids. Am. J. Gastroenterol. 2016, 111, 477–491. [Google Scholar] [CrossRef]
- Salameh, R.; Kirchgesner, J.; Allez, M.; Carbonnel, F.; Meyer, A.; Gornet, J.-M.; Beaugerie, L.; Amiot, A. Long-term outcome of patients with acute severe ulcerative colitis responding to intravenous steroids. Aliment. Pharmacol. Ther. 2020, 51, 1096–1104. [Google Scholar] [CrossRef]
- Truelove, S.C.; Witts, L.J. Cortisone in ulcerative colitis: Final report on a therapeutic trial. Br. Med. J. 1955, 2, 1041–1048. [Google Scholar] [CrossRef]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated Oral 5-Asa for Mildely to Moderately Active Ulcerative Colitis. A randomized study. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef]
- D’Haens, G.; Sandborn, W.J.; Feagan, B.G.; Geboes, K.; Hanauer, S.B.; Irvine, E.J.; Lémann, M.; Marteau, P.; Rutgeerts, P.; Schölmerich, J.; et al. A Review of Activity Indices and Efficacy End Points for Clinical Trials of Medical Therapy in Adults with Ulcerative Colitis. Gastroenterology 2007, 132, 763–786. [Google Scholar] [CrossRef]
- Harbord, M.; Eliakim, R.; Bettenworth, D.; Karmiris, K.; Katsanos, K.; Kopylov, U.; Kucharzik, T.; Molnár, T.; Raine, T.; Sebastian, S.; et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: Current management. J. Crohn’s Colitis 2017, 11, 769–784. [Google Scholar] [CrossRef]
- Vedamurthy, A.; Xu, L.; Luther, J.; Colizzo, F.; Garber, J.J.; Khalili, H.; Ananthakrishnan, A.N. Long-term outcomes of immunosuppression-naïve steroid responders following hospitalization for ulcerative colitis. Dig. Dis. Sci. 2018, 63, 2740–2746. [Google Scholar] [CrossRef]
- Marti-Aguado, D.; Ballester, M.P.; Tosca, J.; Bosca-Watts, M.M.; Navarro, P.; Anton, R.; Pascual, I.; Mora, F.; Minguez, M. Long-term follow-up of patients treated with aminosalicylates for ulcerative colitis: Predictive factors of response: An observational case-control study. United Eur. Gastroenterol. J. 2019, 7, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Bello, C.; Belaiche, J.; Louis, E.; Reenaers, C. Evolution and predictive factors of relapse in ulcerative colitis patients treated with mesalazine after a first course of corticosteroids. J. Crohn’s Colitis 2011, 5, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; McGinley, E.L.; Binion, D.G.; Saeian, K. Simple score to identify colectomy risk in ulcerative colitis hospitalizations. Inflamm. Bowel. Dis. 2010, 16, 1532–1540. [Google Scholar] [CrossRef] [PubMed]
- Moskovitz, D.N.; Van Assche, G.; Maenhout, B.; Arts, J.; Ferrante, M.; Vermeire, S.; Rutgeerts, P. Incidence of Colectomy During Long-term Follow-up After Cyclosporine-Induced Remission of Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2006, 4, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Bojic, D.; Radojicic, Z.; Nedeljkovic-Protic, M.; Al-Ali, M.; Jewell, D.P.; Travis, S.P. Long-term outcome after admission for acute severe ulcerative colitis in Oxford: The 1992–1993 cohort. Inflamm. Bowel Dis. 2009, 15, 823–828. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Maintenance Therapy with 5-ASA (n = 56) | Maintenance Therapy with IMM/Biologic (n = 32) | p |
|---|---|---|---|
| Male gender, n (%) | 33 (59%) | 14 (44%) | 0.19 |
| Age, y (mean ± SD) | 52 ± 19.0 | 44 ± 14.2 | 0.08 |
| Appendectomy | |||
| Yes, n (%) | 3 (5%) | 3 (9%) | 0.056 |
| Age at diagnosis: | |||
| A2: 17–40 y | 31 (55%) | 16 (50%) | 0.66 |
| A3: >40 y | 25 (45%) | 16 (50%) | 0.66 |
| Ulcerative colitis | |||
| E2: left-sided colitis | 20 (36%) | 8 (25%) | 0.35 |
| E3: extensive colitis | 36 (64%) | 24 (75%) | 0.35 |
| Duration of disease, months—median (IQR) | 132 (108) | 108 (138) | 0.46 |
| Previous anti-TNF therapies | 6 (11%) | 8 (25%) | 0.044 |
| Smoking habits | |||
| Former | 18 (32%) | 14 (44%) | 0.74 |
| Current | 7 (13%) | 6 (19%) | 0.34 |
| Steroid dependence, | |||
| Yes, n (%) | 13 (23%) | 15 (47%) | 0.032 |
| Partial Mayo Clinic score, (mean ± SD) | 6.7 ± 1.1 | 6.6 ± 0.8 | 0.79 |
| Endoscopic Mayo Clinic subscore, | |||
| (mean ± SD) | 2.6 ± 0.6 | 2.6 ± 0.5 | 0.79 |
| C-reactive-protein (CRP) | |||
| Positive (>5 mg/L), n (%) | 55 (98%) | 28 (87%) | 0.056 |
| Hemoglobin g/dL | |||
| median (IQR) | 11. 9 (2.8) | 11. 7 (2.3) | 0.909 |
| Albumin g/dL | |||
| median (IQR) | 3 (0.7) | 3.5 (0.8) | 0.0048 |
| Long-Term Outcomes, n pts (%) | Maintenance Therapy with 5-ASA (n = 56) | Maintenance Therapy with IMM/Biologic (n = 32) | p |
|---|---|---|---|
| Relapse, n (%) | |||
| (partial Mayo score >4), | 39 (70%) | 21 (66%) | 0.81 |
| Steroid-free clinical remission | 24 (43%) | 14 (44%) | 0.83 |
| Re-hospitalization, n (%) | 17 (30%) | 11 (34%) | 0.81 |
| Colectomy, n (%) | 11 (20%) | 4 (13%) | 0.56 |
| Corticosteroids, n (%) | 32 (57%) | 17 (53%) | 0.82 |
| IMMs, n (%) | 9 (16%) | 3 (9%) | 0.52 |
| Biologic therapy, n (%) | 15 (27%) | 16 (50%) | 0.037 |
| Month 6 (73 pts) | Month 12 (62 pts) | Month 24 (52 pts) | |
|---|---|---|---|
| Relapse (partial Mayo score >4), n (%) | 24 (33%) | 18 (29%) | 19 (36%) |
| Steroid-free clinical remission, n (%) | 44 (60%) | 41(66%) | 33 (63%) |
| Re-hospitalization, n (%) | 4 (5%) | 6 (10%) | 4 (8%) |
| Colectomy, n (%) | 2 (3%) | 0 | 0 |
| Corticosteroids, n (%) | 17 (23%) | 14 (23%) | 12 (23%) |
| IMMs, n (%) | 1 (1.4%) | 11 (18%) | 7 (13%) |
| Biologic therapy, n (%) | 6 (8%) | 5 (8%) | 5 (10%) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Risk Factors | HR (95% CI) | p Value | HR (95% CI) | p Value |
| 5-ASA maintenance therapy | 1.01 (0.39 to 2.57) | 0.99 | - | |
| IMM/biologic maintenance therapy | 0.85 (0.34 to 2.16) | 0.74 | - | |
| Previous anti-TNF exposure | 8.71 (1.85 to 69.93) | 0.008 | 6.51 (0.67 to 62.86) | 0.89 |
| Steroid dependence | 3.04 (1.13 to 8.19) | 0.02 | 1.09 (0.33 to 3.53) | 0.11 |
| Partial Mayo Clinic score <2 at 6 months after discharge | 0.20 (0.05 to 0.76) | 0.02 | 0.22 (0.05 to 0.88) | 0.03 |
| Disease duration (months) | 0.99 (0.99 to 1.01) | 0.78 | - | |
| Smoking habits | 0.77 (0.23 to 2.59) | 0.6 | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Cristofaro, E.; Salvatori, S.; Marafini, I.; Zorzi, F.; Alfieri, N.; Musumeci, M.; Biancone, L.; Calabrese, E.; Monteleone, G. Long-Term Outcomes and Predictive Factors of Hospitalized Patients with Severe Ulcerative Colitis Treated with Intravenous Corticosteroids. J. Clin. Med. 2021, 10, 5413. https://doi.org/10.3390/jcm10225413
De Cristofaro E, Salvatori S, Marafini I, Zorzi F, Alfieri N, Musumeci M, Biancone L, Calabrese E, Monteleone G. Long-Term Outcomes and Predictive Factors of Hospitalized Patients with Severe Ulcerative Colitis Treated with Intravenous Corticosteroids. Journal of Clinical Medicine. 2021; 10(22):5413. https://doi.org/10.3390/jcm10225413
Chicago/Turabian StyleDe Cristofaro, Elena, Silvia Salvatori, Irene Marafini, Francesca Zorzi, Norma Alfieri, Martina Musumeci, Livia Biancone, Emma Calabrese, and Giovanni Monteleone. 2021. "Long-Term Outcomes and Predictive Factors of Hospitalized Patients with Severe Ulcerative Colitis Treated with Intravenous Corticosteroids" Journal of Clinical Medicine 10, no. 22: 5413. https://doi.org/10.3390/jcm10225413
APA StyleDe Cristofaro, E., Salvatori, S., Marafini, I., Zorzi, F., Alfieri, N., Musumeci, M., Biancone, L., Calabrese, E., & Monteleone, G. (2021). Long-Term Outcomes and Predictive Factors of Hospitalized Patients with Severe Ulcerative Colitis Treated with Intravenous Corticosteroids. Journal of Clinical Medicine, 10(22), 5413. https://doi.org/10.3390/jcm10225413