
Molecular Cytology by One-Step Nucleic Acid Amplification (OSNA) Assay of Peritoneal Washings during D2 Gastrectomy in Advanced Gastric Cancer Patients: Preliminary Results

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
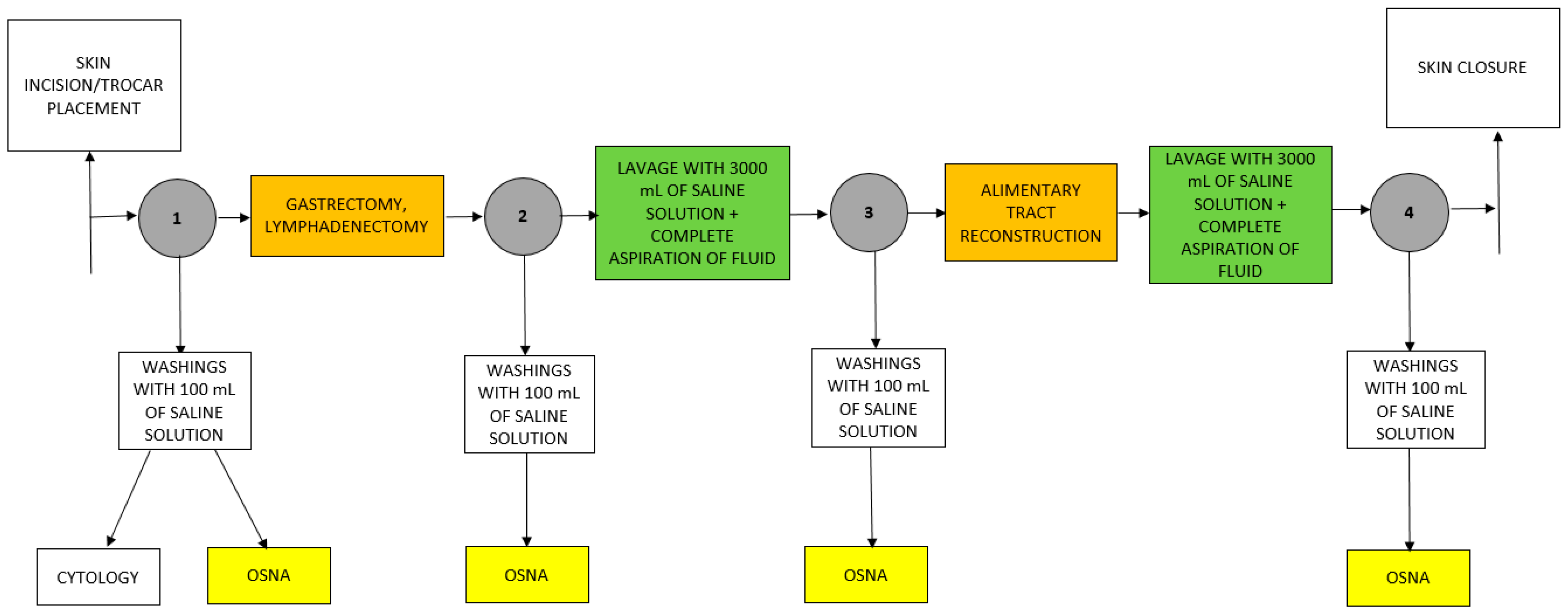
2.2. Intraperitoneal Lavage
2.3. OSNA Examination
2.4. Conventional Cytology
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuramoto, M.; Shimada, S.; Ikeshima, S.; Matsuo, A.; Yagi, Y.; Matsuda, M.; Yonemura, Y.; Baba, H. Extensive intraoperative peritoneal lavage as a standard prophylactic strategy for peritoneal recurrence in patients with gastric carcinoma. Ann. Surg. 2009, 250, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhou, Q.; Wang, H.; Zhuo, W.; Ding, Y.; Lu, J.; Wu, G.; Xu, N.; Teng, L. Predicting Peritoneal Dissemination of Gastric Cancer in the Era of Precision Medicine: Molecular Characterization and Biomarkers. Cancers 2020, 12, 2236. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H. Prevention and Treatment of Peritoneal Metastases from Gastric Cancer. J. Clin. Med. 2021, 10, 1899. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Xu, A.; Sun, X.; Zhao, X.; Xia, Y.; Rao, H.; Zhang, Y.; Zhang, R.; Chen, L.; Zhang, T.; et al. Combined Surgery and Extensive Intraoperative Peritoneal Lavage vs. Surgery Alone for Treatment of Locally Advanced Gastric Cancer: The SEIPLUS Randomized Clinical Trial. JAMA Surg. 2019, 154, 610–616. [Google Scholar] [CrossRef]
- Koganti, S.B.; Boddepalli, S.; Nambada, M.; Thumma, V.M.; Nagari, B.; Sastry, R.A. Positive Peritoneal Lavage Cytology—Implications for Staging and Management of Gastric Cancer. Indian J. Surg. Oncol. 2016, 7, 430–435. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yang, H.K. Operating room to bench for gastric cancer. Pathobiology 2011, 78, 320–327. [Google Scholar] [CrossRef]
- Marutsuka, T.; Shimada, S.; Shiomori, K.; Hayashi, N.; Yagi, Y.; Yamane, T.; Ogawa, M. Mechanisms of peritoneal metastasis after operation for non-serosa-invasive gastric carcinoma: An ultrarapid detection system for intraperitoneal free cancer cells and a prophylactic strategy for peritoneal metastasis. Clin. Cancer Res. 2003, 9, 678–685. [Google Scholar]
- Han, T.S.; Kong, S.H.; Lee, H.J.; Ahn, H.S.; Hur, K.; Yu, J.; Kim, W.H.; Yang, H.K. Dissemination of free cancer cells from the gastric lumen and from perigastric lymphovascular pedicles during radical gastric cancer surgery. Ann. Surg. Oncol. 2011, 18, 2818–2825. [Google Scholar] [CrossRef]
- Tokumitsu, Y.; Yoshino, S.; Iida, M.; Yoshimura, K.; Ueno, T.; Hazama, S.; Oka, M. Intraoperative dissemination during gastrectomy for gastric cancer associated with serosal invasion. Surg. Today 2015, 45, 746–751. [Google Scholar] [CrossRef]
- Kim, G.; Chen, E.; Tay, A.Y.; Lee, J.S.; Phua, J.N.; Shabbir, A.; So, J.B.; Tai, B.C. Extensive peritoneal lavage after curative gastrectomy for gastric cancer (EXPEL): Study protocol of an international multicentre randomised controlled trial. Jpn. J. Clin. Oncol. 2017, 47, 179–184. [Google Scholar] [CrossRef]
- Ohki, A.; Abe, N.; Yoshimoto, E.; Hashimoto, Y.; Takeuchi, H.; Nagao, G.; Masaki, T.; Mori, T.; Ohkura, Y.; Sugiyama, M. Gastric washing by distilled water can reduce free gastric cancer cells exfoliated into the stomach lumen. Gastric. Cancer 2018, 21, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Murata, S.; Yamamoto, H.; Yamaguchi, T.; Kaida, S.; Ishida, M.; Kodama, H.; Takebayashi, K.; Shimizu, T.; Miyake, T.; Tani, T.; et al. Viable Cancer Cells in the Remnant Stomach are a Potential Source of Peritoneal Metastasis after Curative Distal Gastrectomy for Gastric Cancer. Ann. Surg. Oncol. 2016, 23, 2920–2927. [Google Scholar] [CrossRef]
- Yepuri, N.; Bahary, N.; Jain, A.; Dhir, M. Review and Update on the Role of Peritoneal Cytology in the Treatment of Gastric Cancer. J. Surg. Res. 2019, 235, 607–614. [Google Scholar] [CrossRef]
- Takahashi, K.; Kurashina, K.; Saito, S.; Kanamaru, R.; Ohzawa, H.; Yamaguchi, H.; Miyato, H.; Hosoya, Y.; Lefor, A.K.; Sata, N.; et al. Flow cytometry-based analysis of tumor-leukocyte ratios in peritoneal fluid from patients with advanced gastric cancer. Cytom. B Clin. Cytom. 2020. [Google Scholar] [CrossRef]
- Harada, H.; Soeno, T.; Nishizawa, N.; Washio, M.; Sakuraya, M.; Ushiku, H.; Niihara, M.; Hosoda, K.; Kumamoto, Y.; Naitoh, T.; et al. Prospective study to validate the clinical utility of DNA diagnosis of peritoneal fluid cytology test in gastric cancer. Cancer Sci. 2021, 112, 1644–1654. [Google Scholar] [CrossRef]
- Yaguchi, Y.; Sugasawa, H.; Tsujimoto, H.; Takata, H.; Nakabayashi, K.; Ichikura, T.; Ono, S.; Hiraki, S.; Sakamoto, N.; Horio, T.; et al. One-step nucleic acid amplification (OSNA) for the application of sentinel node concept in gastric cancer. Ann. Surg. Oncol. 2011, 18, 2289–2296. [Google Scholar] [CrossRef]
- Kumagai, K.; Yamamoto, N.; Miyashiro, I.; Tomita, Y.; Katai, H.; Kushima, R.; Tsuda, H.; Kitagawa, Y.; Takeuchi, H.; Mukai, M.; et al. Multicenter study evaluating the clinical performance of the OSNA assay for the molecular detection of lymph node metastases in gastric cancer patients. Gastric Cancer 2014, 17, 273–280. [Google Scholar] [CrossRef]
- Bizzarri, N.; Pedone Anchora, L.; Zannoni, G.F.; Santoro, A.; Valente, M.; Inzani, F.; Gallotta, V.; Conte, C.; Chiantera, V.; Fanfani, F.; et al. Role of one-step nucleic acid amplification (OSNA) to detect sentinel lymph node low-volume metastasis in early-stage cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Fanfani, F.; Monterossi, G.; Ghizzoni, V.; Rossi, E.D.; Dinoi, G.; Inzani, F.; Fagotti, A.; Gueli Alletti, S.; Scarpellini, F.; Nero, C.; et al. One-Step Nucleic Acid Amplification (OSNA): A fast molecular test based on CK19 mRNA concentration for assessment of lymph-nodes metastases in early stage endometrial cancer. PLoS ONE 2018, 13, e0195877. [Google Scholar] [CrossRef] [PubMed]
- Kostun, J.; Pesta, M.; Slama, J.; Slunecko, R.; Vlasak, P.; Bouda, J.; Novotny, Z.; Topolcan, O.; Kucera, R.; Kulda, V.; et al. One-step nucleic acid amplification vs. ultrastaging in the detection of sentinel lymph node metastasis in endometrial cancer patients. J. Surg. Oncol. 2019, 119, 361–369. [Google Scholar] [CrossRef]
- Winter, A.; Engels, S.; Goos, P.; Suykers, M.C.; Henke, R.P.; Gerullis, H.; Wawroschek, F. Detection of CK19 mRNA Using One-step Nucleic Acid Amplification (OSNA) in Prostate Cancer: Preliminary Results. J. Cancer 2018, 9, 4611–4617. [Google Scholar] [CrossRef] [PubMed]
- Schem, C.; Maass, N.; Bauerschlag, D.O.; Carstensen, M.H.; Loning, T.; Roder, C.; Batic, O.; Jonat, W.; Tiemann, K. One-step nucleic acid amplification-a molecular method for the detection of lymph node metastases in breast cancer patients; results of the German study group. Virchows Arch. 2009, 454, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Jiwa, M.; Horstman, A.; Brink, A.A.; Pol, R.P.; van Diest, P.; Snijders, P.J.; Meijer, C.J. Intra-operative rapid diagnostic method based on CK19 mRNA expression for the detection of lymph node metastases in breast cancer. Int. J. Cancer 2008, 122, 2562–2567. [Google Scholar] [CrossRef] [PubMed]
- Engels, S.; Brautmeier, L.; Reinhardt, L.; Wasylow, C.; Hasselmann, F.; Henke, R.P.; Wawroschek, F.; Winter, A. Evaluation of Fast Molecular Detection of Lymph Node Metastases in Prostate Cancer Patients Using One-Step Nucleic Acid Amplification (OSNA). Cancers 2021, 13, 1117. [Google Scholar] [CrossRef]
- Märkl, B.; Grosser, B.; Bauer, K.; Vlasenko, D.; Schenkirsch, G.; Probst, A.; Kriening, B. Ultrastaging Using Ex Vivo Sentinel Lymph Node Mapping and One-Step Nucleic Acid Amplification (OSNA) in Gastric Cancer: Experiences of a European Center. Cancers 2021, 13, 2683. [Google Scholar] [CrossRef]
- Geca, K.; Rawicz-Pruszynski, K.; Mielko, J.; Mlak, R.; Sedlak, K.; Polkowski, W.P. Rapid Detection of Free Cancer Cells in Intraoperative Peritoneal Lavage Using One-Step Nucleic Acid Amplification (OSNA) in Gastric Cancer Patients. Cells 2020, 9, 2168. [Google Scholar] [CrossRef]
- Becker, K.; Mueller, J.D.; Schulmacher, C.; Ott, K.; Fink, U.; Busch, R.; Bottcher, K.; Siewert, J.R.; Hofler, H. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer 2003, 98, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.K.; Ji, J.; Han, S.U.; Terashima, M.; Li, G.; Kim, H.H.; Law, S.; Shabbir, A.; Song, K.Y.; Hyung, W.J.; et al. Extensive peritoneal lavage with saline after curative gastrectomy for gastric cancer (EXPEL): A multicentre randomised controlled trial. Lancet Gastroenterol. Hepatol. 2021, 6, 120–127. [Google Scholar] [CrossRef]
- Misawa, K.; Mochizuki, Y.; Sakai, M.; Teramoto, H.; Morimoto, D.; Nakayama, H.; Tanaka, N.; Matsui, T.; Ito, Y.; Ito, S.; et al. Randomized clinical trial of extensive intraoperative peritoneal lavage versus standard treatment for resectable advanced gastric cancer (CCOG 1102 trial). Br. J. Surg. 2019, 106, 1602–1610. [Google Scholar] [CrossRef]
- Rodriguez-Santiago, J.; Luna, A.; Garsot, E.; Aldeano, A.; Balague, C.; Rada, A. Extended intraoperative peritoneal lavage as prophylactic peritoneal recurrence for locally advanced gastric cancer: A prospective randomized trial. Clin. Transl. Oncol. 2021, 23, 1857–1865. [Google Scholar] [CrossRef]
- Ronellenfitsch, U.; Ernst, K.; Mertens, C.; Trunk, M.J.; Strobel, P.; Marx, A.; Kienle, P.; Post, S.; Nowak, K. Extensive intraperitoneal lavage to eliminate intraperitoneal tumor cells in gastrectomy with D2 lymphadenectomy for gastric cancer. Tumori 2018, 104, 361–368. [Google Scholar] [CrossRef]
- Hasbahceci, M.; Akcakaya, A.; Guler, B.; Kunduz, E.; Malya, F.U.; Muslumanoglu, M. Use of peritoneal washing cytology for the detection of free peritoneal cancer cells before and after surgical treatment of gastric adenocarcinoma. J. Cancer Res. Ther. 2018, 14, 1225–1229. [Google Scholar] [CrossRef]
- Coccolini, F.; Catena, F.; Glehen, O.; Yonemura, Y.; Sugarbaker, P.H.; Piso, P.; Ceresoli, M.; Montori, G.; Ansaloni, L. Effect of intraperitoneal chemotherapy and peritoneal lavage in positive peritoneal cytology in gastric cancer. Systematic review and meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Mizrak Kaya, D.; Nogueras-Gonzalez, G.M.; Harada, K.; Amlashi, F.G.; Roy-Chowdhuri, S.; Estrella, J.S.; Das, P.; Lee, J.H.; Weston, B.; Bhutani, M.S.; et al. Risk of peritoneal metastases in patients who had negative peritoneal staging and received therapy for localized gastric adenocarcinoma. J. Surg. Oncol. 2018, 117, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, K.; Murata, S.; Kodama, H.; Kaida, S.; Yamaguchi, T.; Ishikawa, K.; Shimoji, M.; Miyake, T.; Ueki, T.; Kojima, M.; et al. Long-term prognosis of patients with cancer-related genes detected in postoperative peritoneal washings obtained during curative gastrectomy. Eur. J. Surg. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Study Group (n = 27) |
|---|---|
| Sex | |
| Men | 13 (48.1%) |
| Women | 14 (51.9%) |
| Age | |
| median (range) | 63 (40–80) |
| <65 years | 14 (51.9%) |
| ≥65 years | 13 (48.1%) |
| Lauren’s type | |
| Intestinal | 12 (44.5%) |
| Mixed | 7 (25.9%) |
| Diffuse | 7 (25.9%) |
| Undetermined | 1 (3.7%) |
| (y)pT | |
| in situ | 3 (11.1%) |
| 1a | 2 (7.4%) |
| 1b | 4 (14.8%) |
| 2 | 4 (14.8%) |
| 3 | 10 (37%) |
| 4a | 2 (7.4%) |
| 4b | 2 (7.4%) |
| (y)pN | |
| 0 | 12 (44.4%) |
| 1 | 6 (22.2%) |
| 2 | 4 (14.8%) |
| 3a | 2 (7.4%) |
| 3b | 3 (11.1%) |
| (y)pM | |
| 0 | 26 (96.3%) |
| 1 | 1 (3.7%) |
| Neoadjuvant chemotherapy | |
| Yes | 19 (70.4%) |
| No | 8 (29.6%) |
| No. of neoadjuvant chemotherapy cycles | |
| median (range) | 4 (4–5) |
| Extent of gastrectomy | |
| Proximal gastrectomy | 5 (18.6%) |
| Distal gastrectomy | 13 (48.1%) |
| Total gastrectomy | 9 (33.3%) |
| CCOG 1102 Trial [29] | SEIPLUS [4] | EXPEL [20] | EIPL vs. Standard Peritoneal Lavage [30] | |
|---|---|---|---|---|
| Author and year | K. Misawa; 2019 | J. Guo; 2019 | H. K. Yang; 2020 | J. Rodriguez-Santiago; 2021 |
| No. of patients randomized | 314 | 662 | 800 | 94 |
| No. of patients assigned and analyzed in EIPL group | 145 | 279 | 396 | 43 |
| No. of patients assigned and analyzed in surgery group | 150 | 271 | 401 | 43 |
| Inclusion criteria |
|
|
|
|
| Exclusion criteria |
|
|
|
|
| Type of surgery | Distal or total open gastrectomy with D2 lymphadenectomy | Proximal, distal or total gastrectomy with D2 lymphadenectomy | Open or laparoscopic radical gastrectomy | Total or distal gastrectomy with D2 lymphadenectomy (or D1 in total spleen-preserving gastrectomy) |
| EIPL group | EIPL using 10 L of saline (1 L for 10 times) | EIPL using 10 L of saline (1 L for 10 times) | EIPL using 10 L of saline (1 L for 10 times) | EIPL using 10 L of saline (1 L for 10 times) |
| Surgery group | Peritoneal lavage with no more than 3 L of saline before closure of abdomen | Peritoneal lavage with no more than 3 L of saline before closure of abdomen | Peritoneal lavage with no more than 2 L of saline before closure of abdomen | Peritoneal lavage with no more than 2 L of saline before closure of abdomen |
| Method of peritoneal lavage assessment | Cytology | Cytology | Cytology | |
| Primary endpoint | DFS rate | OS rate | OS rate | OS rate |
| Secondary endpoints | OS, peritoneal recurrence-free survival, incidence of adverse events | Safety and efficacy of EIPL | DFS, peritoneal recurrence | Incidence of adverse events, type of recurrence |
| Results | 3-year DFS rate:
| Mortality:
| OS:
| 3-year OS rate:
|
| Conclusions | EIPL did not improve survival or peritoneal recurrence in patients who underwent gastrectomy for advanced GC | EIPL increases the safety of D2 gastrectomy and decrease short-term postoperative complications and wound pain | EIPL + surgery did not have a survival benefit compared with surgery alone and is not recommended for patients undergoing curative gastrectomy for GC | EIPL in patients with locally advanced GC, regardless of peritoneal cytology, has not been effective as prophylaxis of peritoneal recurrence or better survival. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gęca, K.; Rawicz-Pruszyński, K.; Mlak, R.; Sędłak, K.; Skórzewska, M.; Pelc, Z.; Małecka-Massalska, T.; Polkowski, W.P. Molecular Cytology by One-Step Nucleic Acid Amplification (OSNA) Assay of Peritoneal Washings during D2 Gastrectomy in Advanced Gastric Cancer Patients: Preliminary Results. J. Clin. Med. 2021, 10, 5230. https://doi.org/10.3390/jcm10225230
Gęca K, Rawicz-Pruszyński K, Mlak R, Sędłak K, Skórzewska M, Pelc Z, Małecka-Massalska T, Polkowski WP. Molecular Cytology by One-Step Nucleic Acid Amplification (OSNA) Assay of Peritoneal Washings during D2 Gastrectomy in Advanced Gastric Cancer Patients: Preliminary Results. Journal of Clinical Medicine. 2021; 10(22):5230. https://doi.org/10.3390/jcm10225230
Chicago/Turabian StyleGęca, Katarzyna, Karol Rawicz-Pruszyński, Radosław Mlak, Katarzyna Sędłak, Magdalena Skórzewska, Zuzanna Pelc, Teresa Małecka-Massalska, and Wojciech P. Polkowski. 2021. "Molecular Cytology by One-Step Nucleic Acid Amplification (OSNA) Assay of Peritoneal Washings during D2 Gastrectomy in Advanced Gastric Cancer Patients: Preliminary Results" Journal of Clinical Medicine 10, no. 22: 5230. https://doi.org/10.3390/jcm10225230
APA StyleGęca, K., Rawicz-Pruszyński, K., Mlak, R., Sędłak, K., Skórzewska, M., Pelc, Z., Małecka-Massalska, T., & Polkowski, W. P. (2021). Molecular Cytology by One-Step Nucleic Acid Amplification (OSNA) Assay of Peritoneal Washings during D2 Gastrectomy in Advanced Gastric Cancer Patients: Preliminary Results. Journal of Clinical Medicine, 10(22), 5230. https://doi.org/10.3390/jcm10225230