
Long-Term Experience with Hyperthermic Chemotherapy (HIVEC) Using Mitomycin-C in Patients with Non-Muscle Invasive Bladder Cancer in Spain


 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
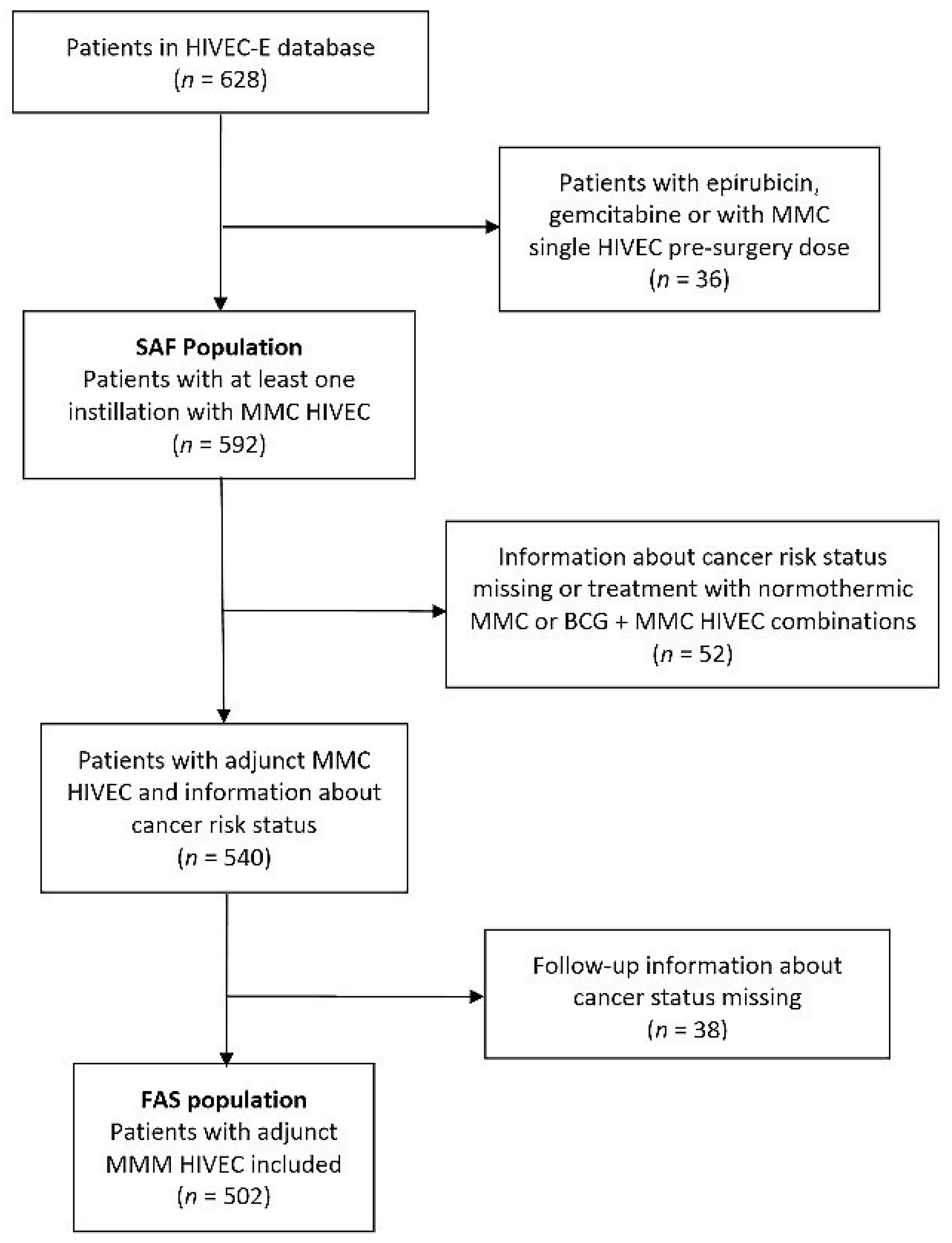
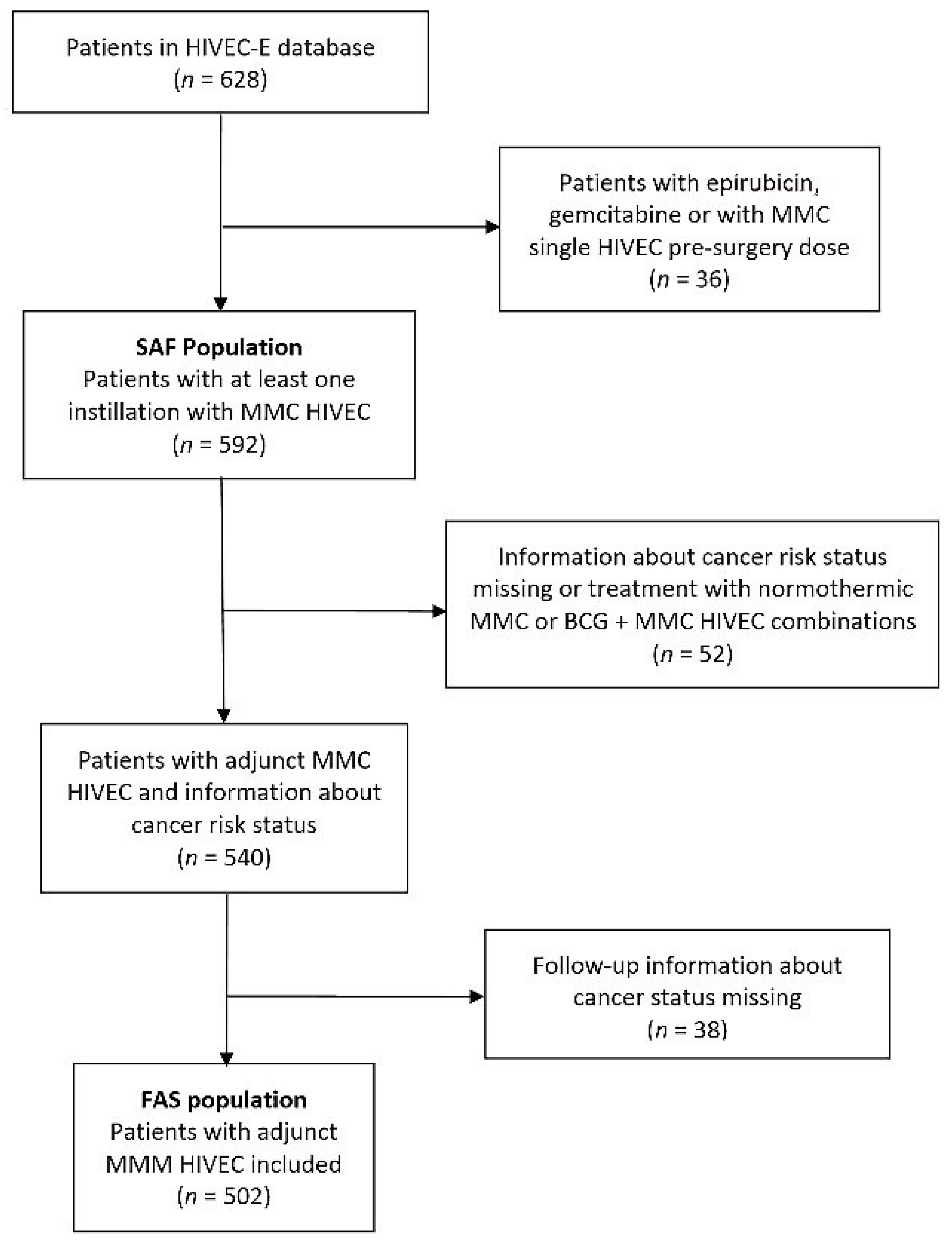
2.1. Study Population
2.2. Study Endpoints
2.3. Variables Evaluated
2.4. Statistical Analysis
3. Results
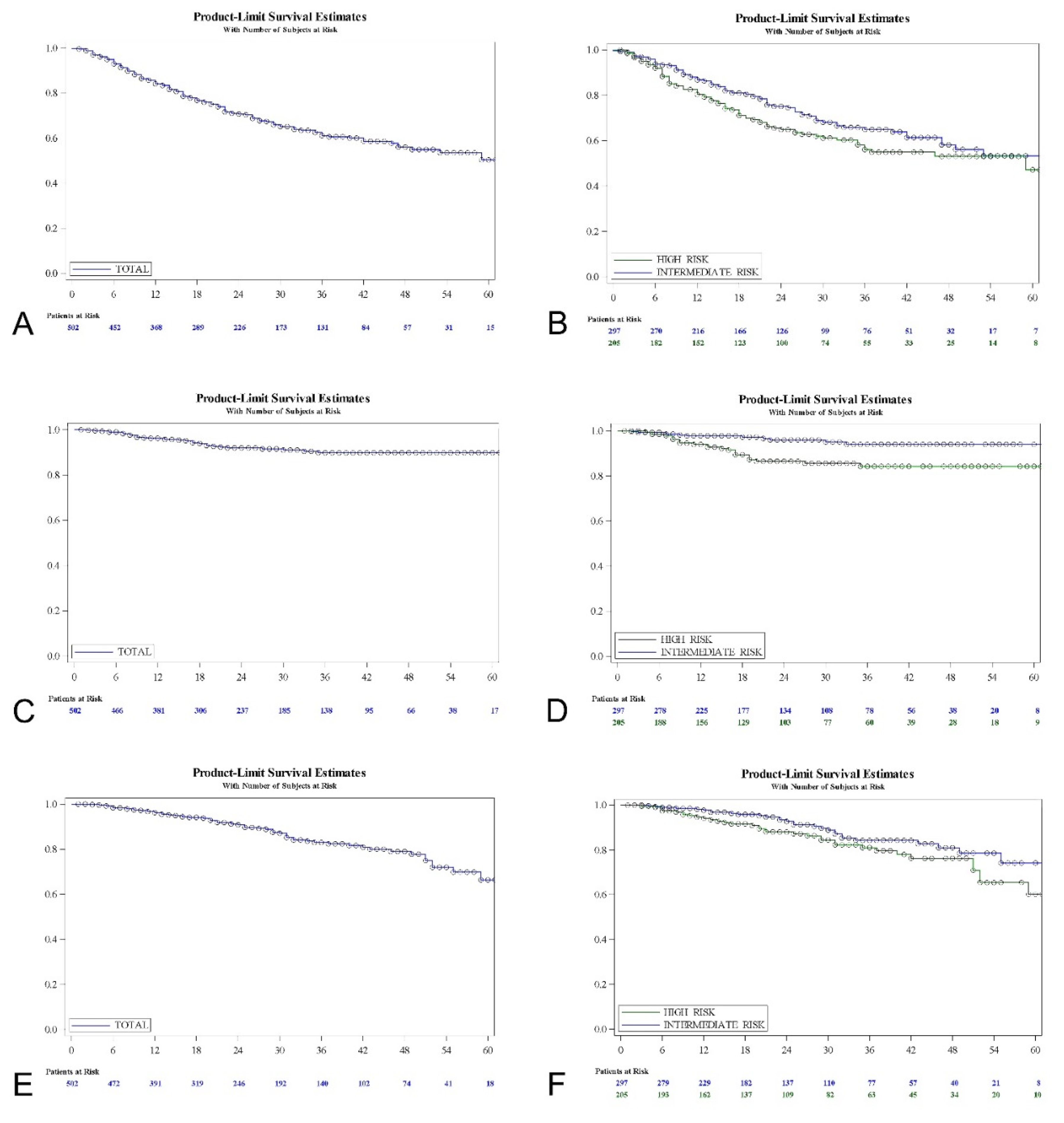
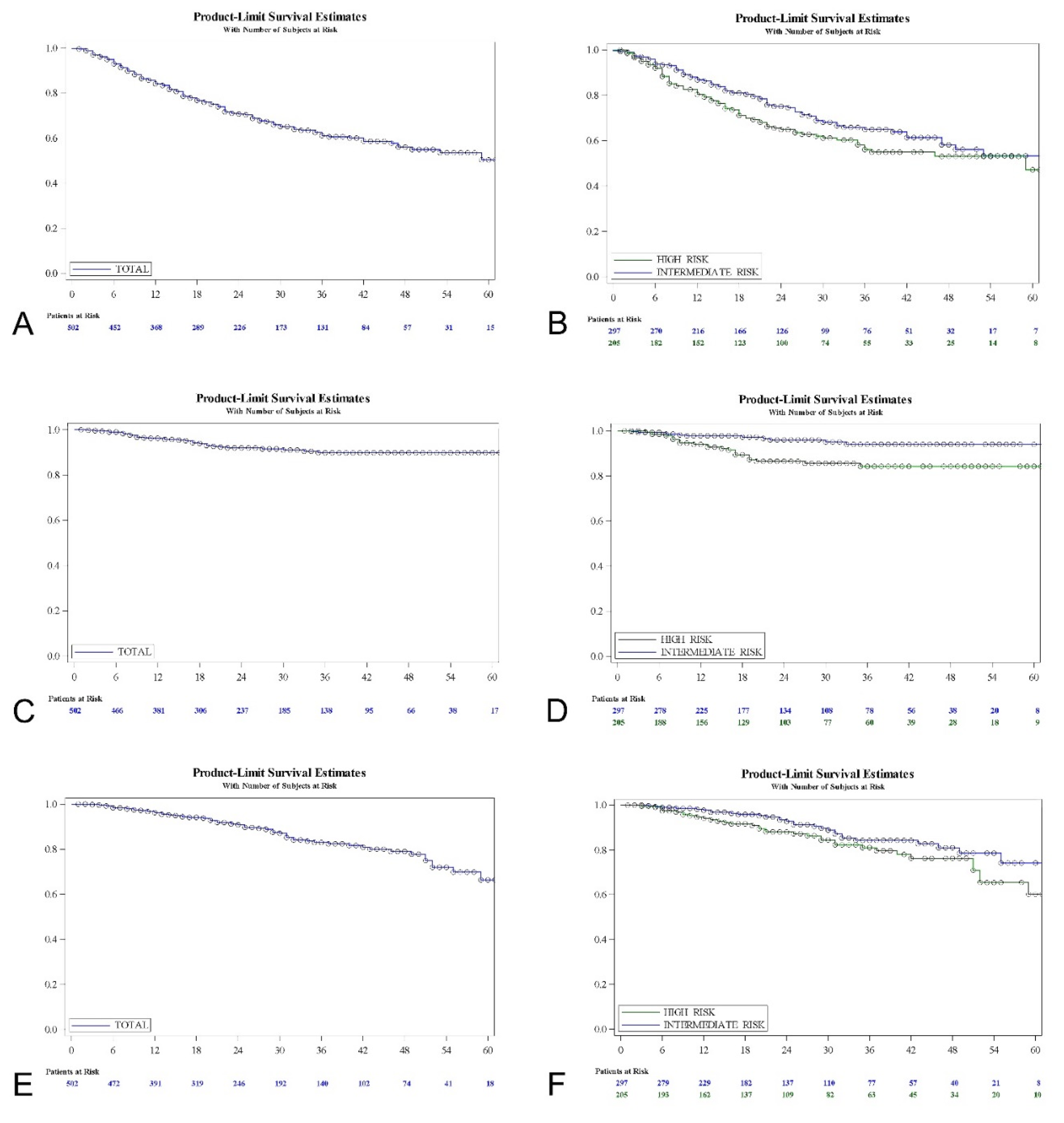
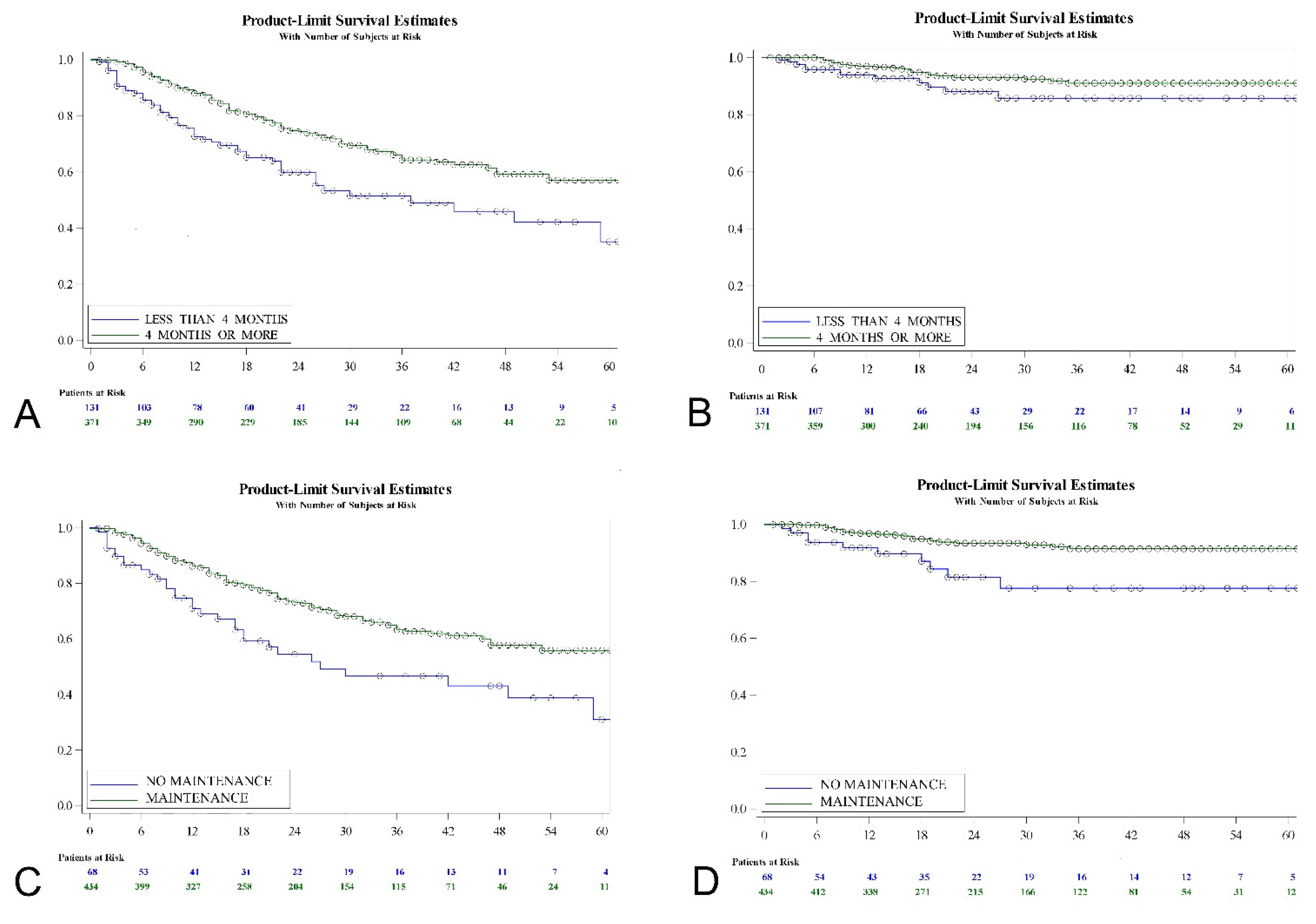
3.1. Recurrence-Free Survival
3.2. Progression-Free Survival
3.3. Overall Survival
3.4. Tolerability and Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teoh, J.Y.; Huang, J.; Ko, W.Y.; Lok, V.; Choi, P.; Ng, C.F.; Sengupta, S.; Mostafid, H.; Kamat, A.M.; Black, P.C.; et al. Global Trends of Bladder Cancer Incidence and Mortality, and Their Associations with Tobacco Use and Gross Domestic Product Per Capita. Eur. Urol. 2020, 78, 893–906. [Google Scholar] [CrossRef]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angulo, J.C.; Lopez, J.I.; Flores, N.; Toledo, J.D. The value of tumour spread, grading and growth pattern as morphological predictive parameters in bladder carcinoma. A critical revision of the 1987 TNM classification. J. Cancer Res. Clin. Oncol. 1993, 119, 578–593. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2021. [Google Scholar] [CrossRef]
- Huncharek, M.; Kupelnick, B. The influence of intravesical therapy on progression of superficial transitional cell carcinoma of the bladder: A metaanalytic comparison of chemotherapy versus bacilli Calmette-Guerin immunotherapy. Am. J. Clin. Oncol. 2004, 27, 522–528. [Google Scholar] [CrossRef]
- Gontero, P.; Sylvester, R.; Pisano, F.; Joniau, S.; Vander Eeckt, K.; Serretta, V.; Larré, S.; Di Stasi, S.; Van Rhijn, B.; Witjes, A.J.; et al. Prognostic factors and risk groups in T1G3 non-muscle-invasive bladder cancer patients initially treated with Bacillus Calmette-Guérin: Results of a retrospective multicenter study of 2451 patients. Eur. Urol. 2015, 67, 74–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, V.; Wymer, K.M.; Borah, B.J.; Saigal, C.S.; Litwin, M.S.; Packiam, V.T.; Thompson, R.H.; Tollefson, M.K.; Karnes, R.J.; Boorjian, S.A. Cost-Effectiveness of Maintenance bacillus Calmette-Guérin for Intermediate and High Risk Nonmuscle Invasive Bladder Cancer. J. Urol. 2020, 204, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Fankhauser, C.D.; Teoh, J.Y.; Mostafid, H. Treatment options and results of adjuvant treatment in nonmuscle-invasive bladder cancer (NMIBC) during the Bacillus Calmette-Guérin shortage. Curr. Opin. Urol. 2020, 30, 365–369. [Google Scholar] [CrossRef]
- Witjes, J.A.; Palou, J.; Soloway, M.; Lamm, D.; Kamat, A.M.; Brausi, M.; Persad, R.; Buckley, R.; Colombel, M.; Böhle, A. Current clinical practice gaps in the treatment of intermediate- and high-risk non-muscle-invasive bladder cancer (NMIBC) with emphasis on the use of bacillus Calmette-Guerin (BCG): Results of an international individual patient data survey (IPDS). BJU Int. 2013, 112, 742–750. [Google Scholar] [CrossRef]
- Slovacek, H.; Zhuo, J.; Taylor, J.M. Approaches to Non-Muscle-Invasive Bladder Cancer. Curr. Oncol. Rep. 2021, 23, 105. [Google Scholar] [CrossRef] [PubMed]
- Liem, E.I.M.L.; Crezee, H.; de la Rosette, J.J.; de Reijke, T.M. Chemohyperthermia in non-muscle-invasive bladder cancer: An overview of the literature and recommendations. Int. J. Hyperth. 2016, 32, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Zargar, H.; Aning, J.; Ischia, J.; So, A.; Black, P. Optimizing intravesical mitomycin C therapy in non-muscle-invasive bladder cancer. Nat. Rev. Urol. 2014, 11, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Teicher, B.A.; Kowal, C.D.; Kennedy, K.A.; Sartorelli, A.C. Enhancement by hyperthermia of the in vitro cytotoxicity of mitomycin C toward hypoxic tumor cells. Cancer Res. 1981, 41, 1096–1099. [Google Scholar] [PubMed]
- Chiancone, F.; Fabiano, M.; Fedelini, M.; Meccariello, C.; Carrino, M.; Fedelini, P. Outcomes and complications of Hyperthermic IntraVesical using mitomycin C or epirubicin for patients with non-muscle invasive bladder cancer after bacillus Calmette-Guérin treatment failure. Cent. Eur. J. Urol. 2020, 73, 287–294. [Google Scholar]
- Rampersaud, E.N.; Vujaskovic, Z.; Inman, B.A. Hyperthermia as a treatment for bladder cancer. Oncology 2010, 24, 1149–1155. [Google Scholar]
- Multhoff, G.; Habl, G.; Combs, S.E. Rationale of hyperthermia for radio(chemo)therapy and immune responses in patients with bladder cancer: Biological concepts, clinical data, interdisciplinary treatment decisions and biological tumour imaging. Int. J. Hyperth. 2016, 32, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Van der Heijden, A.G.; Verhaegh, G.; Jansen, C.F.J.; Schalken, J.A.; Witjes, J.A. Effect of hyperthermia on the cytotoxicity of 4 chemotherapeutic agents currently used for the treatment of transitional cell carcinoma of the bladder: An in vitro study. J. Urol. 2005, 173, 1375–1380. [Google Scholar] [CrossRef]
- Sousa Escandón, A.; León Mata, J.; Sousa González, D.; Alvarez Casal, M.; Rodríguez, S.; Piñeiro Vazquez, S. Neoadjuvant chemohyperthermia: Our experience after 10 years. Arch. Esp. Urol. 2018, 71, 438–446. [Google Scholar]
- Tan, W.P.; Chang, A.; Brousell, S.C.; Grimberg, D.C.; Fantony, J.J.; Longo, T.A.; Etienne, W.; Spasojevic, I.; Maccarini, P.; Inman, B.A. Safety and efficacy of intravesical chemotherapy and hyperthermia in the bladder: Results of a porcine study. Int. J. Hyperth. 2020, 37, 854–860. [Google Scholar] [CrossRef]
- Sousa, A.; Inman, B.A.; Piñeiro, I.; Monserrat, V.; Pérez, A.; Aparici, V.; Gómez, I.; Neira, P.; Uribarri, C. A clinical trial of neoadjuvant hyperthermic intravesical chemotherapy (HIVEC) for treating intermediate and high-risk non-muscle invasive bladder cancer. Int. J. Hyperth. 2014, 30, 166–170. [Google Scholar] [CrossRef]
- Sousa, A.; Piñeiro, I.; Rodríguez, S.; Aparici, V.; Monserrat, V.; Neira, P.; Carro, E.; Murias, C.; Uribarri, C. Recirculant hyperthermic IntraVEsical chemotherapy (HIVEC) in intermediate-high-risk non-muscle-invasive bladder cancer. Int. J. Hyperth. 2016, 32, 374–380. [Google Scholar] [CrossRef] [Green Version]
- Ekin, R.G.; Akarken, I.; Cakmak, O.; Tarhan, H.; Celik, O.; Ilbey, Y.O.; Divrik, R.T.; Zorlu, F. Results of Intravesical Chemo-Hyperthermia in High-risk Non-muscle Invasive Bladder Cancer. Asian Pac. J. Cancer Prev. 2015, 16, 3241–3245. [Google Scholar] [CrossRef] [Green Version]
- González-Padilla, D.A.; González-Díaz, A.; Miranda-Utrera, N.; De la Rosa Kehrmann, F.; Villacampa, F.; Guerrero-Ramos, F. HIVEC HR: Chemohyperthermia with mitomycin C vs. BCG for high-risk non-muscle invasive bladder cancer. Preliminary results from a randomized controlled trial. Eur. Urol. Suppl. 2019, 18, e768–e770. [Google Scholar] [CrossRef]
- de Jong, J.J.; Hendricksen, K.; Rosier, M.; Mostafid, H.; Boormans, J.L. Hyperthermic Intravesical Chemotherapy for BCG Unresponsive Non-Muscle Invasive Bladder Cancer Patients. Bladder Cancer 2018, 4, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pijpers, O.M.; Hendricksen, K.; Mostafid, H.; de Jong, F.C.; Rosier, M.; Mayor, N.; de Jong, J.J.; Boormans, J.L. Long-term efficacy of hyperthermic intravesical chemotherapy for BCG-unresponsive non-muscle invasive bladder cancer. Urol. Oncol. 2021. [Google Scholar] [CrossRef]
- Brummelhuis, I.S.G.; Wimper, Y.; Witjes-van Os, H.G.J.M.; Arends, T.J.H.; van der Heijden, A.G.; Witjes, J.A. Long-Term Experience with Radiofrequency-Induced Hyperthermia Combined with Intravesical Chemotherapy for Non-Muscle Invasive Bladder Cancer. Cancers 2021, 13, 377. [Google Scholar] [CrossRef]
- Cambier, S.; Sylvester, R.J.; Collette, L.; Gontero, P.; Brausi, M.A.; van Andel, G.; Kirkels, W.J.; Silva, F.C.; Oosterlinck, W.; Prescott, S.; et al. EORTC Nomograms and Risk Groups for Predicting Recurrence, Progression, and Disease-specific and Overall Survival in Non-Muscle-invasive Stage Ta-T1 Urothelial Bladder Cancer Patients Treated with 1-3 Years of Maintenance Bacillus Calmette-Guérin. Eur. Urol. 2016, 69, 60–69. [Google Scholar] [CrossRef]
- Tan, W.S.; Panchal, A.; Buckley, L.; Devall, A.J.; Loubière, L.S.; Pope, A.M.; Feneley, M.R.; Cresswell, J.; Issa, R.; Mostafid, H.; et al. Radiofrequency-induced Thermo-chemotherapy Effect Versus a Second Course of Bacillus Calmette-Guérin or Institutional Standard in Patients with Recurrence of Non-muscle-invasive Bladder Cancer Following Induction or Maintenance Bacillus Calmette-Guérin Therapy (HYMN): A Phase III, Open-label, Randomised Controlled Trial. Eur. Urol. 2019, 75, 63–71. [Google Scholar] [PubMed]
- Thomsen, J.A.; Dominiak, H.N.; Lindgren, M.S.; Jensen, J.B. Adverse events of hyperthermic intravesical chemotherapy for non-muscle invasive bladder cancer patients. Scand. J. Urol. 2021, 55, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Marquette, T.; Walz, J.; Rybikowski, S.; Maubon, T.; Branger, N.; Fakhfakh, S.; Verde, K.L.; Dermeche, S.; Gravis, G.; Pignot, G. Safety of Hyperthermic IntraVEsical Chemotherapy (HIVEC) for BCG Unresponsive Non-Muscle Invasive Bladder Cancer Patients. Prog. Urol. 2020, 30, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Hendricksen, K. Device-assisted intravesical therapy for non-muscle invasive bladder cancer. Transl. Androl. Urol. 2019, 8, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Alkhateeb, S.S.; Van Rhijn, B.W.G.; Finelli, A.; van der Kwast, T.; Evans, A.; Hanna, S.; Vajpeyi, R.; Fleshner, N.E.; Jewett, M.A.S.; Zlotta, A.R. Nonprimary pT1 nonmuscle invasive bladder cancer treated with bacillus Calmette-Guerin is associated with higher risk of progression compared to primary T1 tumors. J. Urol. 2010, 184, 81–86. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Sex, n (%) | |
| Male | 414 (82.5) |
| Female | 88 (17.5) |
| Age, years * | 69.6 ± 10.6 (34–94) |
| BMI, kg/m2 * | 3.4 ± 1.3 (1–6) |
| Smoking status, n (%) | |
| Non-smoker | 92 (18.3) |
| Ex-smoker | 256 (51) |
| Current smoker | 128 (25.5) |
| Unknown | 26 (5.2) |
| Number of tumors, n (%) (#) | |
| Single | 258 (52.4) |
| Multiple | 234 (47.6) |
| Tumor size, n (%) (#) | |
| <3 cm | 333 (67.7) |
| ≥3 cm | 159 (32.3) |
| Pathological stage, n (%) | |
| Ta | 376 (74.9) |
| T1 | 116 (23.1) |
| Primary carcinoma in situ | 10 (2) |
| Grade (##), n (%) | |
| G1 | 173 (34.45) |
| G2 | 178 (35.45) |
| G3 | 151 (30.1) |
| EAU Risk stratification, n (%) | |
| Intermediate-risk | 297 (59.2) |
| High-risk | 205 (40.8) |
| Previous treatment with MMC, n (%) | 69 (13.7) |
| Previous treatment with BCG, n (%) | 51 (10.15) |
| Follow-up, months * | 24.45 ± 16.5 (1–81) |
| Recurrence during follow-up, n (%) | 159 (31.7) |
| Progression during follow-up, n (%) | 35 (7) |
| Overall mortality, during follow-up (%) | 66 (13.15) |
| Recurrence-Free Survival | Percent | 95% CI | Log-Rank Test |
|---|---|---|---|
| Total series | |||
| 1 year | 84.12 | 80.46–87.15 | |
| 2 years | 70.72 | 66.03–74.89 | |
| 5 years | 50.37 | 41.38–58–69 | |
| Intermediate-risk | p = 0.075 | ||
| 1 year | 86.77 | 82.11–90.28 | |
| 2 years | 75.13 | 69.00–80.22 | |
| 5 years | 53.30 | 42.75–62.76 | |
| High-risk | |||
| 1 year | 80.34 | 73.99–85.29 | |
| 2 years | 64.88 | 57.37–71.40 | |
| 5 years | 47.14 | 33.44–59.67 | |
| Progression-free survival | |||
| Total series | |||
| 1 year | 96.24 | 94.01–97.65 | |
| 2 years | 91.97 | 88.69–94.31 | |
| 5 years | 89.83 | 85.81–92.75 | |
| Intermediate-risk | p = 0.001 | ||
| 1 year | 97.79 | 95.14–99.00 | |
| 2 years | 95.99 | 92.27–97.94 | |
| 5 years | 94.02 | 88.87–96.83 | |
| High-risk | |||
| 1 year | 93.99 | 89.41–96.63 | |
| 2 years | 86.52 | 80.16–90.95 | |
| 5 years | 84.23 | 77.02–89.34 | |
| Overall survival | |||
| Total series | |||
| 1 year | 96.23 | 94–97.64 | |
| 2 years | 90.8 | 87.34–93.35 | |
| 5 years | 66.35 | 54.67–75.68 | |
| Intermediate-risk | p = 0.064 | ||
| 1 year | 97.73 | 95–98.97 | |
| 2 years | 92.73 | 88.07–95.62 | |
| 5 years | 74.26 | 60.55–83.82 | |
| High-risk | |||
| 1 year | 94.09 | 89.56–96.68 | |
| 2 years | 88.09 | 82.06–92.19 | |
| 5 years | 60.12 | 43.45–73.29 |
| Univariate Analysis | Hazard Ratio | 95% CI | p-Value |
| High- vs. intermediate-risk group | 1.322 | 0.968–1.805 | 0.0783 |
| T1 vs. Ta | 1.44 | 1.019–2.037 | 0.0009 |
| Primary cis vs. T1 | 2.609 | 1.177–5.784 | |
| Primary cis vs. Ta | 3.758 | 1.746–8.088 | |
| G2 vs. G1 | 1.088 | 0.733–1.615 | 0.1065 |
| G3 vs. G2 | 1.347 | 0.927–1.956 | |
| G3 vs. G1 | 1.466 | 1.003–2.145 | |
| Cis vs. no cis | 2.551 | 1.472–4.424 | 0.0008 |
| Recurrent vs. primary | 1.756 | 1.285–2.399 | 0.0004 |
| Treatment duration < 4 vs. ≥4 months | 1.842 | 1.321–2.568 | 0.0003 |
| No maintenance vs. maintenance | 1.929 | 1.307–2.846 | 0.0009 |
| Previous MMC vs. no | 1.611 | 1.071–2.424 | 0.0299 |
| Previous BCG vs. no | 1.834 | 1.187–2.84 | 0.0063 |
| Age ≥ 70 vs. <70 years | 1.254 | 0.917–1.715 | 0.156 |
| Male vs. female | 1.326 | 0.852–2.061 | 0.2102 |
| Smoker vs. non-smoker | 1.274 | 0.81–2.004 | 0.2948 |
| Multiple vs. single tumor | 1.220 | 0.888–1.675 | 0.2199 |
| Size ≥ 3 vs. <3 cm | 1.024 | 0.724–1.449 | 0.8895 |
| Multivariate analysis | Hazard Ratio | 95% CI | p-value |
| Recurrent vs. primary | 1.828 | 1.327–2.518 | 0.0002 |
| Treatment duration < 4 vs. ≥4 months | 1.724 | 1.235–2.407 | 0.0014 |
| High- vs. intermediate-risk group | 1.472 | 1.071–2.024 | 0.0171 |
| Univariate Analysis | Hazard Ratio | 95% CI | p-Value |
| High- vs. intermediate-risk group | 3.076 | 1.506–6.289 | 0.002 |
| T1 vs. Ta | 3.159 | 1.596–6.253 | 0.0008 |
| Primary cis vs. T1 | 2.078 | 0.477–9.045 | |
| Primary cis vs. Ta | 6.563 | 1.515–28.438 | |
| G2 vs. G1 | 3.03 | 0.977–9.433 | 0.0059 |
| G3 vs. G2 | 1.808 | 0.877–3.731 | |
| G3 vs. G1 | 5.494 | 1.865–16.129 | |
| Cis vs. no cis | 4.424 | 1.718–11.363 | 0.0021 |
| Recurrent vs. primary | 2.876 | 1.431–5.784 | 0.003 |
| Treatment duration < 4 vs. ≥4 months | 1.908 | 0.948–3.84 | 0.0702 |
| No maintenance vs. maintenance | 3.07 | 1.474–6.396 | 0.0027 |
| Previous MMC vs. no | 2.561 | 1.199–5.468 | 0.0151 |
| Previous BCG vs. no | 2.717 | 1.233–5.988 | 0.0132 |
| Age ≥ 70 vs. <70 years | 1.681 | 0.847–3.339 | 0.1377 |
| Male vs. female | 1.062 | 0.441–2.557 | 0.893 |
| Smoker vs. non-smoker | 1.011 | 0.417–2.45 | 0.9797 |
| Multiple vs. single tumor | 1.158 | 0.591–2.269 | 0.6684 |
| Size ≥ 3 vs. <3 cm | 1.165 | 0.564–2.403 | 0.6788 |
| Multivariate Analysis | Hazard Ratio | 95% CI | p-value |
| High- vs. intermediate-risk group | 3.891 | 1.886–8 | 0.0002 |
| Recurrent vs. primary | 3.32 | 1.613–6.833 | 0.0011 |
| No maintenance vs. maintenance | 2.374 | 1.125–5.01 | 0.0233 |
| Univariate Analysis | Hazard Ratio | 95% CI | p-Value |
| High- vs. intermediate-risk group | 1.572 | 0.967–2.557 | 0.0679 |
| T1 vs. Ta | 1.64 | 0.99–2.715 | 0.1579 |
| Primary cis vs. T1 | 0 | 0 | |
| Primary cis vs. Ta | 0 | 0 | |
| G2 vs. G1 | 1.801 | 0.935–3.46 | 0.0533 |
| G3 vs. G2 | 1.228 | 0.712–2.118 | |
| G3 vs. G1 | 2.212 | 1.158–4.219 | |
| Cis vs. no cis | 1.2 | 0.375–3.831 | 0.7571 |
| Recurrent vs. primary | 1.017 | 0.618–1.675 | 0.947 |
| Treatment duration <4 vs. ≥4 months | 1.948 | 1.171–3.239 | 0.0102 |
| No maintenance vs. maintenance | 1.789 | 0.984–3.253 | 0.0565 |
| Previous MMC vs. no | 0.967 | 0.461–2.024 | 0.9294 |
| Previous BCG vs. no | 0.801 | 0.29–2.217 | 0.6709 |
| Age ≥70 vs. <70 years | 3.459 | 1.943–6.157 | <0.0001 |
| Male vs. female | 1.663 | 0.793–3.496 | 0.1781 |
| Smoker vs. non-smoker | 0.973 | 0.506–1.869 | 0.9353 |
| Multiple vs. single tumor | 1.158 | 0.591–2.269 | 0.6684 |
| Size ≥3 vs. <3 cm | 1.024 | 0.724–1.449 | 0.8895 |
| Multivariate Analysis | Hazard Ratio | 95% CI | p-value |
| Age ≥70 vs. <70 years | 3.356 | 1.884–5.976 | <0.0001 |
| Treatment duration <4 vs. ≥4 months | 1.824 | 1.095–3.039 | 0.0211 |
|
Grade 1–2 n (%) |
Grade 3–4 n (%) |
Total n (%) | |
|---|---|---|---|
| Dysuria | 59 (34.7) | 0 (0) | 59 (9.9) |
| Frequency | 5 (2.9) | 0 (0) | 5 (0.8) |
| Irritative symptoms | 18 (9.4) | 1 (6.25) | 17 (2.9) |
| Bladder Pain | 37 (21.8) | 5 (31.25) | 42 (7.1) |
| Urgency | 34 (20) | 0 (0) | 34 (5.7) |
| Urinary retention | 0 (0) | 0 (0) | 0 (0) |
| Bladder spasms | 21 (12.35) | 1 (6.25) | 22 (3.7) |
| Bacterial cystitis | 11 (6.5) | 1 (6.25) | 12 (2) |
| Renal colic | 1 (0.6) | 0 (0) | 1 (0.2) |
| Hematuria | 18 (10.6) | 3 (18.75) | 21 (3.55) |
| Incontinence | 8 (4.7) | 1 (6.25) | 9 (1.5) |
| Fever | 2 (1.2) | 1 (6.25) | 3 (0.5) |
| Flu-like symptoms | 0 (0) | 0 (0) | 0 (0) |
| Skin rash | 27 (15.9) | 2 (12.5) | 29 (4.9) |
| Other AEs | 7 (4.1) | 3 (18.75) | 12 (2) |
| Total number EAs | 248 (100) | 18 (100) | 266 (100) |
| Number of patients with AES | 170 | 16 | 186 |
| Number of patients w/o AEs | - | - | 406 |
| SAF population | - | - | 592 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plata, A.; Guerrero-Ramos, F.; Garcia, C.; González-Díaz, A.; Gonzalez-Valcárcel, I.; de la Morena, J.M.; Díaz-Goizueta, F.J.; del Álamo, J.F.; Gonzalo, V.; Montero, J.; et al. Long-Term Experience with Hyperthermic Chemotherapy (HIVEC) Using Mitomycin-C in Patients with Non-Muscle Invasive Bladder Cancer in Spain. J. Clin. Med. 2021, 10, 5105. https://doi.org/10.3390/jcm10215105
Plata A, Guerrero-Ramos F, Garcia C, González-Díaz A, Gonzalez-Valcárcel I, de la Morena JM, Díaz-Goizueta FJ, del Álamo JF, Gonzalo V, Montero J, et al. Long-Term Experience with Hyperthermic Chemotherapy (HIVEC) Using Mitomycin-C in Patients with Non-Muscle Invasive Bladder Cancer in Spain. Journal of Clinical Medicine. 2021; 10(21):5105. https://doi.org/10.3390/jcm10215105
Chicago/Turabian StylePlata, Ana, Félix Guerrero-Ramos, Carlos Garcia, Alejandro González-Díaz, Ignacio Gonzalez-Valcárcel, José Manuel de la Morena, Francisco Javier Díaz-Goizueta, Julio Fernández del Álamo, Victoria Gonzalo, Javier Montero, and et al. 2021. "Long-Term Experience with Hyperthermic Chemotherapy (HIVEC) Using Mitomycin-C in Patients with Non-Muscle Invasive Bladder Cancer in Spain" Journal of Clinical Medicine 10, no. 21: 5105. https://doi.org/10.3390/jcm10215105
APA StylePlata, A., Guerrero-Ramos, F., Garcia, C., González-Díaz, A., Gonzalez-Valcárcel, I., de la Morena, J. M., Díaz-Goizueta, F. J., del Álamo, J. F., Gonzalo, V., Montero, J., Sousa-Escandón, A., León, J., Pontones, J. L., Delgado, F., Adriazola, M., Pascual, Á., Calleja, J., Ruano, A., Martínez-Piñeiro, L., & Angulo, J. C. (2021). Long-Term Experience with Hyperthermic Chemotherapy (HIVEC) Using Mitomycin-C in Patients with Non-Muscle Invasive Bladder Cancer in Spain. Journal of Clinical Medicine, 10(21), 5105. https://doi.org/10.3390/jcm10215105