
Blood Neurofilament Light Chain in Parkinson’s Disease: Comparability between Parkinson’s Progression Markers Initiative (PPMI) and Asian Cohorts

 , , and
, , and
Abstract
1. Introduction
2. Results
2.1. The SHH Cohort
2.2. The PPMI Cohort
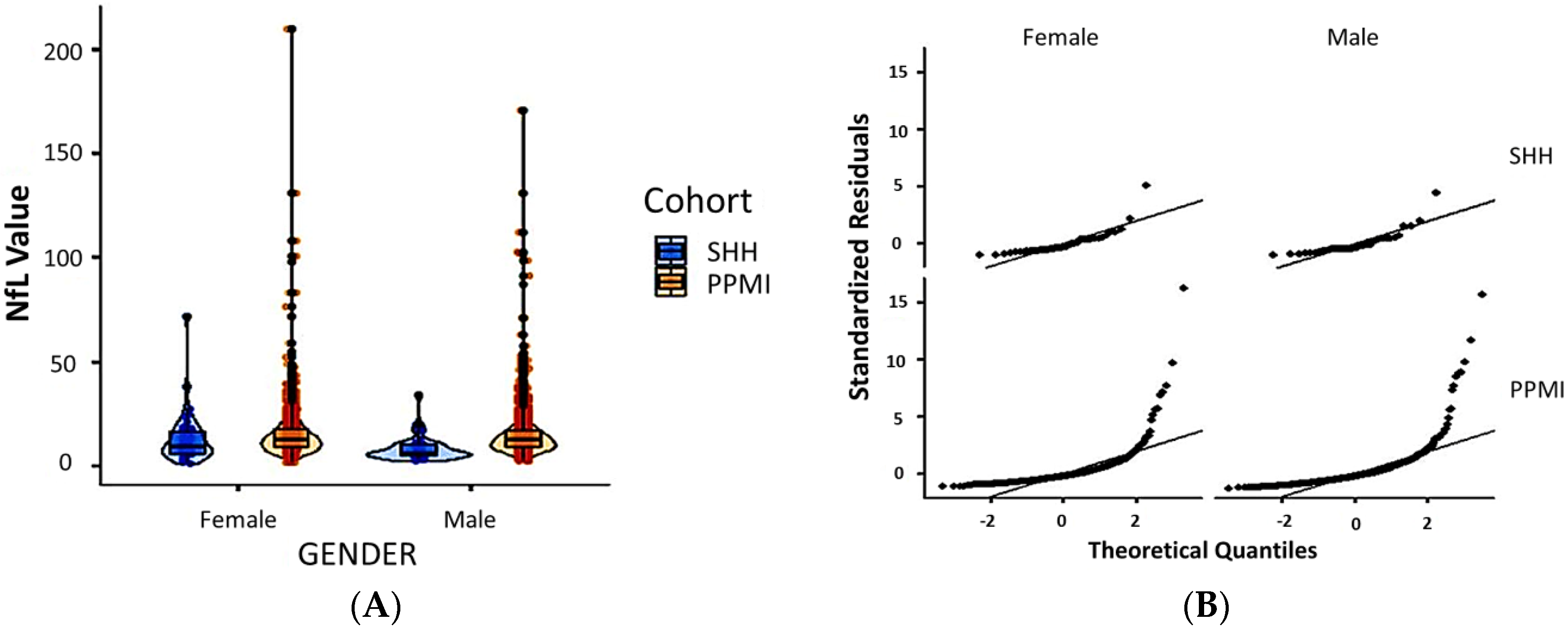
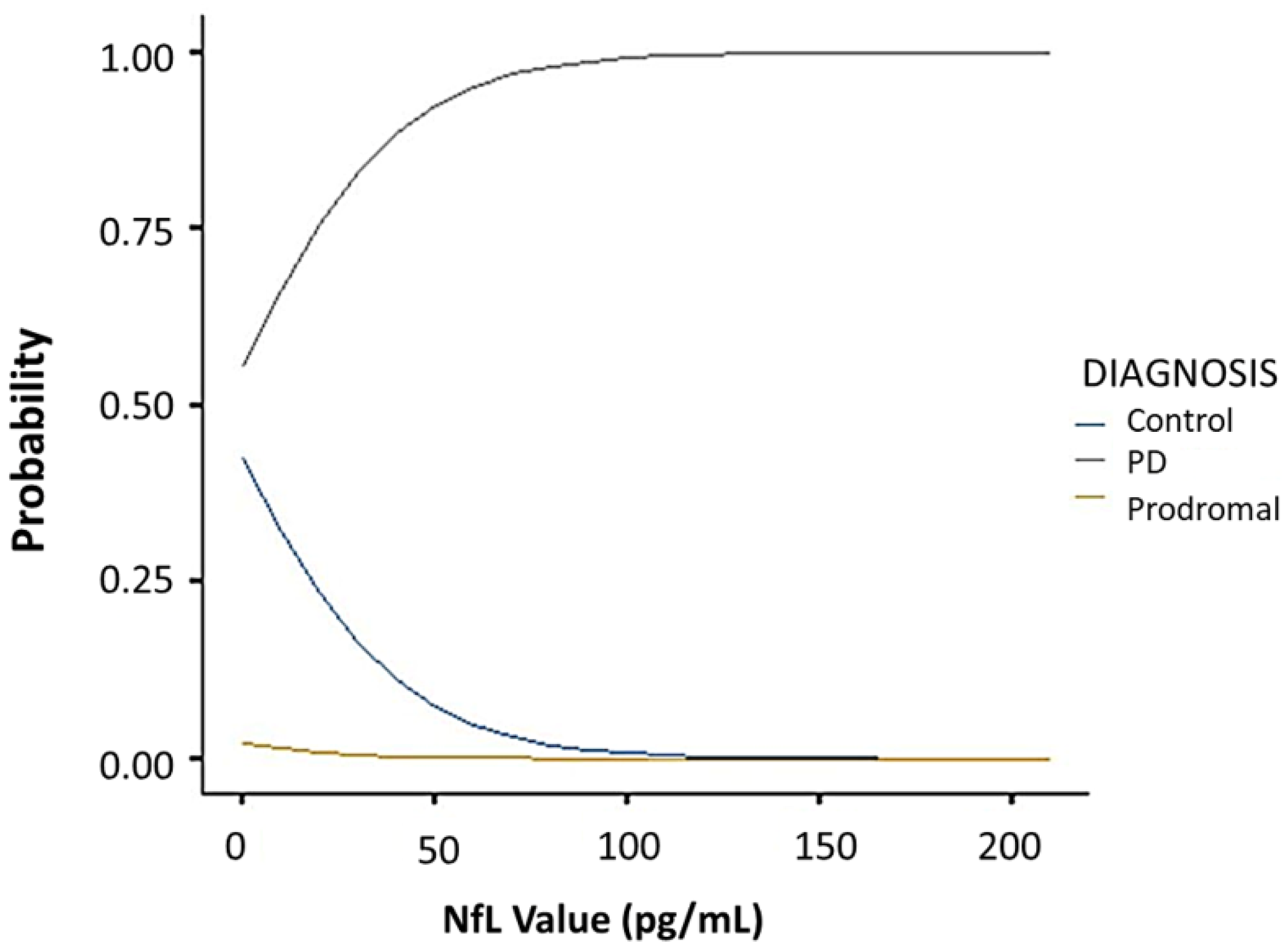
2.3. Comparison between the SHH and PPMI Cohort
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.1.1. Neurofilament Light Chain Immunomagnetic Reduction Assay
4.1.2. The PPMI Cohort
4.2. Covariate-Adjusted Regression
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef]
- Dorsey, E.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef]
- Yang, W.; Hamilton, J.L.; Kopil, C.; Beck, J.C.; Tanner, C.M.; Albin, R.L.; Ray Dorsey, E.; Dahodwala, N.; Cintina, I.; Hogan, P.; et al. Current and projected future economic burden of Parkinson’s disease in the U.S. NPJ Parkinsons Dis. 2020, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, S.T.; Afzal, M.; Morgan, P.S.; Bajaj, N.; Gowland, P.A.; Auer, D.P. The ‘swallow tail’ appearance of the healthy nigrosome—a new accurate test of Parkinson’s disease: A case-control and retrospective cross-sectional MRI study at 3T. PLoS ONE 2014, 9, e93814. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.J.; Kim, J.M.; Kim, E.; Lee, K.M.; Kang, S.Y.; Park, H.S.; Kim, K.J.; Kim, Y.E.; Oh, E.S.; Yun, J.Y.; et al. Loss of nigral hyperintensity on 3 Tesla MRI of Parkinsonism: Comparison with (123) I-FP-CIT SPECT. Mov. Disord. 2016, 31, 684–692. [Google Scholar] [CrossRef]
- Castellanos, G.; Fernandez-Seara, M.A.; Lorenzo-Betancor, O.; OrtegaCubero, S.; Puigvert, M.; Uranga, J.; Vidorreta, M.; Irigoyen, J.; Lorenzo, E.; Muñoz-Barrutia, A.; et al. Automated neuromelanin imaging as a diagnostic biomarker for Parkinson’s disease. Mov. Disord. 2015, 30, 945–952. [Google Scholar] [CrossRef]
- Langley, J.; Huddleston, D.E.; Sedlacik, J.; Boelmans, K.; Hu, X.P. Parkinson’s disease-related increase of T2*-weighted hypointensity in substantia nigra pars compacta. Mov. Disord. 2016, 32, 441–449. [Google Scholar] [CrossRef]
- Ba, F.; Martin, W.R. Dopamine transporter imaging as a diagnostic tool for parkinsonism and related disorders in clinical practice. Parkinsonism Relat. Disord. 2015, 21, 87–94. [Google Scholar] [CrossRef]
- Gayed, I.; Joseph, U.; Fanous, M.; Wan, D.; Schiess, M.; Ondo, W.; Won, K.S. The impact of DaTscan in the diagnosis of Parkinson disease. Clin. Nucl. Med. 2015, 40, 390–393. [Google Scholar] [CrossRef]
- Emamzadeh, F.N.; Surguchov, A. Parkinson’s Disease: Biomarkers, Treatment, and Risk Factors. Front Neurosci. 2018, 12, 612. [Google Scholar] [CrossRef]
- Forgrave, L.M.; Ma, M.; Best, J.R.; DeMarco, M.L. The diagnostic performance of neurofilament light chain in CSF and blood for Alzheimer’s disease, frontotemporal dementia, and amyotrophic lateral sclerosis: A systematic review and meta-analysis. Alzheimers Dement Amst. 2019, 11, 730–743. [Google Scholar] [CrossRef]
- Sun, Q.; Zhao, X.; Li, S.; Yang, F.; Wang, H.; Cui, F.; Huang, X. CSF Neurofilament Light Chain Elevation Predicts ALS Severity and Progression. Front Neurol. 2020, 11, 919. [Google Scholar] [CrossRef]
- Kapoor, R.; Smith, K.E.; Allegretta, M.; Arnold, D.L.; Carroll, W.; Comabella, M.; Furlan, R.; Harp, C.; Kuhle, J.; Leppert, D.; et al. Serum neurofilament light as a biomarker in progressive multiple sclerosis. Neurology 2020, 95, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.H.; Soares, C.B.; Høgedal, S.S.; Madsen, J.S.; Hansen, R.B.; Christensen, A.A.; Madsen, C.; Clausen, B.H.; Frich, L.H.; Degn, M.; et al. Acute Neurofilament Light Chain Plasma Levels Correlate With Stroke Severity and Clinical Outcome in Ischemic Stroke Patients. Front. Neurol. 2020, 11, 448. [Google Scholar] [CrossRef] [PubMed]
- Barro, C.; Chitnis, T.; Weiner, H.L. Blood neurofilament light: A critical review of its application to neurologic disease. Ann. Clin. Transl. Neurol. 2020, 7, 2508–2523. [Google Scholar] [CrossRef] [PubMed]
- Bridel, C.; van Wieringen, W.N.; Zetterberg, H.; Tijms, B.M.; Teunissen, C.E.; The NFL Group; Alvarez-Cermeño, J.C.; Andreasson, U.; Axelsson, M.; Bäckström, D.C.; et al. Diagnostic Value of Cerebrospinal Fluid Neurofilament Light Protein in Neurology: A Systematic Review and Meta-analysis. JAMA Neurol. 2019, 76, 1035–1048. [Google Scholar] [CrossRef]
- Lin, C.H.; Li, C.H.; Yang, K.C.; Lin, F.J.; Wu, C.C.; Chieh, J.J.; Chiu, M.J. Blood NfL: A biomarker for disease severity and progression in Parkinson disease. Neurology 2019, 93, e1104–e1111. [Google Scholar] [CrossRef]
- Mollenhauer, B.; Dakna, M.; Kruse, N.; Galasko, D.; Foroud, T.; Zetterberg, H.; Schade, S.; Gera, R.G.; Wang, W.; Gao, F.; et al. Validation of Serum Neurofilament Light Chain as a Biomarker of Parkinson’s Disease Progression. Mov. Disord. 2020, 35, 1999–2008. [Google Scholar] [CrossRef]
- Oosterveld, L.P.; Verberk, I.M.W.; Majbour, N.K.; El-Agnaf, O.M.; Weinstein, H.C.; Berendse, H.W.; Teunissen, C.E.; van de Berg, W.D.J. CSF or serum neurofilament light added to α-Synuclein panel discriminates Parkinson’s from controls. Mov. Disord. 2020, 35, 288–295. [Google Scholar] [CrossRef]
- Hansson, O.; Janelidze, S.; Hall, S.; Magdalinou, N.; Lees, A.J.; Andreasson, U.; Norgren, N.; Linder, J.; Forsgren, L.; Constantinescu, R.; et al. Swedish BioFINDER study. Blood-based NfL: A biomarker for differential diagnosis of parkinsonian disorder. Neurology 2017, 88, 930–937. [Google Scholar] [CrossRef]
- Sampedro, F.; Pérez-González, R.; Martínez-Horta, S.; Marín-Lahoz, J.; Pagonabarraga, J.; Kulisevsky, J. Serum neurofilament light chain levels reflect cortical neurodegeneration in de novo Parkinson’s disease. Parkinsonism Relat. Disord. 2020, 74, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Marques, T.M.; van Rumund, A.; Oeckl, P.; Kuiperij, H.B.; Esselink, R.A.J.; Bloem, B.R.; Otto, M.; Verbeek, M.M. Serum NFL discriminates Parkinson disease from atypical parkinsonisms. Neurology 2019, 92, e1479–e1486. [Google Scholar] [CrossRef]
- Lin, Y.S.; Lee, W.J.; Wang, S.J.; Fuh, J.L. Levels of plasma neurofilament light chain and cognitive function in patients with Alzheimer or Parkinson disease. Sci. Rep. 2018, 8, 17368. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.S.L.; Tan, Y.J.; Yong, A.C.W.; Saffari, S.E.; Lu, Z.; Ng, E.Y.; Ng, S.Y.E.; Chia, N.S.Y.; Choi, X.; Heng, D.; et al. Utility of plasma Neurofilament light as a diagnostic and prognostic biomarker of the postural instability gait disorder motor subtype in early Parkinson’s disease. Mol. Neurodegener. 2020, 15, 33. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, B.C.; Lin, C.H. Integrated Plasma and Neuroimaging Biomarkers Associated with Motor and Cognition Severity in Parkinson’s Disease. J. Parkinsons Dis. 2020, 10, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Zetterberg, H. Is there a value of Neurofilament Light as a biomarker for neurodegeneration in Parkinson’s Disease? Mov. Disord. 2020, 35, 1111–1112. [Google Scholar] [CrossRef]
- Lerche, S.; Wurster, I.; Röben, B.; Zimmermann, M.; Machetanz, G.; Wiethoff, S.; Dehnert, M.; Rietschel, L.; Riebenbauer, B.; Deuschle, C.; et al. CSF NFL in a Longitudinally Assessed PD Cohort: Age Effects and Cognitive Trajectories. Mov. Disord. 2020, 35, 1138–1144. [Google Scholar] [CrossRef]
- Wilke, C.; Dos Santos, M.C.T.; Schulte, C.; Deuschle, C.; Scheller, D.; Verbelen, M.; Brockmann, K.; Von Thaler, A.; Sünkel, U.; Roeben, B.; et al. Intra-individual Neurofilament Dynamics in Serum Mark the Conversion to Sporadic Parkinson’s Disease. Mov. Disord. 2020, 35, 1233–1238. [Google Scholar] [CrossRef]
- Qiu, X.; Lee, S.; Jackson, J.; Zhao, X.; Shields, A.; Matias, M.; Uzgiris, A. Equivalence of serum and plasma neurofilament light chain levels using highly sensitive automated immunoassay. Alzheimers Dement. 2020, 16, e045278. [Google Scholar] [CrossRef]
- Clarke, C.E.; Patel, S.; Ives, N.; Rick, C.E.; Woolley, R.; Wheatley, K.; Walker, M.F.; Zhu, S.; Kandiyali, R.; Yao, G.; et al. Clinical effectiveness and cost-effectiveness of physiotherapy and occupational therapy versus no therapy in mild to moderate Parkinson’s disease: A large pragmatic randomised controlled trial (PD REHAB). Health Technol. Assess. 2016, 20, 1–96. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.C.; Lin, W.C.; Chiu, M.J.; Lu, C.H.; Lin, C.Y.; Yang, S.Y. Development of an assay of plasma neurofilament light chain utilizing immunomagnetic reduction technology. PLoS ONE 2020, 15, e0234519. [Google Scholar] [CrossRef]
- Li, L.; Kleinman, K.; Gillman, M.W. A comparison of confounding adjustment methods with an application to early life determinants of childhood obesity. J. Dev. Orig. Health Dis. 2014, 5, 435–447. [Google Scholar] [CrossRef][Green Version]
- Groenwold, R.H.H.; Palmer, T.M.; Tilling, K. To Adjust or Not to Adjust? When a “Confounder” Is Only Measured After Exposure. Epidemiology 2021, 32, 194–201. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PwP | Control | p-Value | |
|---|---|---|---|
| Number of patients (n) | 61 | 25 | |
| Age (years, mean ± SD) | 66.77 ± 6.38 | 68.04 ± 8.97 | 0.56 |
| Male (n) | 29 | 17 | |
| Female (n) | 32 | 8 | 0.10 |
| Disease duration (years, mean ± SD) | 2.61 ± 2.22 | N/A | |
| MMSE (mean ± SD) | 26.64 ± 2.99 | 27.00 ± 3.55 | 0.28 |
| MoCA (mean ± SD) | 22.28 ± 4.84 | 22.72 ± 4.10 | 0.88 |
| UPDRS-I (mean ± SD) | 2.20 ± 1.67 | N/A | |
| UPDRS-II | 7.61 ± 5.63 | N/A | |
| UPDRS-III | 21.84 ± 8.65 | N/A | |
| Plasma NfL (all, mean ± SD) | 9.39 ± 6.91 | 14.42 ± 13.84 | 0.05 * |
| Male | 8.58 ± 6.21 | 7.25 ± 4.43 | |
| Female | 10.29 ± 7.62 | 17.79 ± 15.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-H.; Chan, L.; Chung, C.-C.; Bamodu, O.A.; Hong, C.-T. Blood Neurofilament Light Chain in Parkinson’s Disease: Comparability between Parkinson’s Progression Markers Initiative (PPMI) and Asian Cohorts. J. Clin. Med. 2021, 10, 5085. https://doi.org/10.3390/jcm10215085
Chen J-H, Chan L, Chung C-C, Bamodu OA, Hong C-T. Blood Neurofilament Light Chain in Parkinson’s Disease: Comparability between Parkinson’s Progression Markers Initiative (PPMI) and Asian Cohorts. Journal of Clinical Medicine. 2021; 10(21):5085. https://doi.org/10.3390/jcm10215085
Chicago/Turabian StyleChen, Jia-Hung, Lung Chan, Chen-Chih Chung, Oluwaseun Adebayo Bamodu, and Chien-Tai Hong. 2021. "Blood Neurofilament Light Chain in Parkinson’s Disease: Comparability between Parkinson’s Progression Markers Initiative (PPMI) and Asian Cohorts" Journal of Clinical Medicine 10, no. 21: 5085. https://doi.org/10.3390/jcm10215085
APA StyleChen, J.-H., Chan, L., Chung, C.-C., Bamodu, O. A., & Hong, C.-T. (2021). Blood Neurofilament Light Chain in Parkinson’s Disease: Comparability between Parkinson’s Progression Markers Initiative (PPMI) and Asian Cohorts. Journal of Clinical Medicine, 10(21), 5085. https://doi.org/10.3390/jcm10215085