
The ESTMJS (European Society of Temporomandibular Joint Surgeons) Consensus and Evidence-Based Recommendations on Management of Condylar Dislocation

 ,
,  , , ,
, , ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Guideline Draft
2.2. Delphi Procedure (Preliminary Voting)
2.3. Final Voting (Consensus Meeting)
3. Results
3.1. Literature Search and Search Update (2019–2021)
3.2. Participants Preliminary and Final Voting
3.2.1. Participants Preliminary Voting
3.2.2. Participants Final Voting
3.3. Voting Results
3.3.1. Terminology
3.3.2. Initial Draft
3.3.3. Preliminary Grading
3.3.4. Final Voting
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prechel, U.; Ottl, P.; Ahlers, O.M.; Neff, A. The Treatment of Temporomandibular Joint Dislocation. Dtsch. Aerzteblatt Online 2018, 115, 59–64. [Google Scholar] [CrossRef]
- Chhabra, S.; Chhabra, N.; Gupta, P. Recurrent Mandibular Dislocation in Geriatric Patients: Treatment and Prevention by a Simple and Non-invasive Technique. J. Maxillofac. Oral Surg. 2015, 14 (Suppl. 1), 231–234. [Google Scholar] [CrossRef] [PubMed]
- Marqués-Mateo, M.; Puche-Torres, M.; Iglesias-Gimilio, M.-E. Temporomandibular chronic dislocation: The long-standing condition. Med. Oral Patol. Oral Cir. Buccal 2016, 21, e776–e783. [Google Scholar] [CrossRef][Green Version]
- Sang, L.K.; Mulupi, E.; Akama, M.K.; Muriithi, J.M.; Macigo, F.G.; Chindia, M.L. Temporomandibular joint dislocation in Nairobi. East Afr. Med. J. 2010, 87, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Neff, A.; Hell, B.; Kolk, A.; Pautke, C.; Schneider, M.; Prechel, U. S3 Leitlinie Kiefergelenkluxation; AWMF Registernummer 007-063; Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. (AWMF) e.V.: Berlin, Germany, 2016. [Google Scholar]
- Thangaratinam, S.; Walker, P.; Freeman-Wang, T.; Luesley, D.; Cruickshank, M.; Redman, C. Identifying the performance criteria for appraisal of colposcopists: Benchmarking Delphi. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 1288–1291. [Google Scholar] [CrossRef] [PubMed]
- Muche-Borowski, C.; Selbmann, H.K.; Nothacker, M.; Müller, W.; Kopp, I. Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF)-Ständige Kommission Leitlinien. AWMF-Regelwerk Leitlinien. 1. Auflage 2012. Available online: http://www.awmf.org/leitlinien/awmf-regelwerk.html (accessed on 30 September 2021).
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. The 2011 Oxford CEBM Levels of Evidence (Introductory Document). 2011. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 1 October 2021).
- Lovely, F.W.; Copeland, R.A. Reduction eminoplasty for chronic recurrent luxation of the temporomandibular joint. J. Can. Dent. Assoc. 1981, 47, 179–184. [Google Scholar]
- Akinbami, B.O. Evaluation of the mechanism and principles of management of temporomandibular joint dislocation. Systematic review of literature and a proposed new classification of temporomandibular joint dislocation. Head Face Med. 2011, 7, 10. [Google Scholar] [CrossRef]
- Papoutsis, G.; Papoutsi, S.; Klukowska-Rötzler, J.; Schaller, B.; Exadaktylos, A.K. Temporomandibular joint dislocation: A retrospective study from a Swiss urban emergency department. Open Access Emerg. Med. 2018, 10, 171–176. [Google Scholar] [CrossRef]
- Ugboko, V.I.; Oginni, F.O.; Ajike, S.O.; Olasoji, H.O.; Adebayo, E.T. A survey of temporomandibular joint dislocation: Aetiology, demographics, risk factors and management in 96 Nigerian cases. Int. J. Oral Maxillofac. Surg. 2005, 34, 499–502. [Google Scholar] [CrossRef]
- Jeyaraj, P.; Chakranarayan, A. A Conservative Surgical Approach in the Management of Longstanding Chronic Protracted Temporomandibular Joint Dislocation: A Case Report and Review of Literature. J. Maxillofac. Oral Surg. 2016, 15 (Suppl. 2), 361–370. [Google Scholar] [CrossRef][Green Version]
- Güven, O. Management of chronic recurrent temporomandibular joint dislocations: A retrospective study. J. Craniomaxillofac. Surg. 2009, 37, 24–29. [Google Scholar] [CrossRef]
- Matsushita, K.; Abe, T.; Fujiwara, T. OK-432 (Picibanil) sclerotherapy for recurrent dislocation of the temporomandibular joint in elderly edentulous patients: Case reports. Br. J. Oral Maxillofac. Surg. 2007, 45, 511–513. [Google Scholar] [CrossRef]
- Rikhotso, E.R.; Bobat, M.A. Total Alloplastic Joint Reconstruction in a Patient With Temporomandibular Joint Ankylosis Following Condylar Dislocation Into the Middle Cranial Fossa. J. Oral Maxillofac. Surg. 2016, 74, 2378.e1–2378.e5. [Google Scholar] [CrossRef] [PubMed]
- McGoldrick, D.M.; Stassen, L.F.A. Management of acute dislocation of the temporomandibular joint in dental practice. J. Ir. Dent. Assoc. 2010, 56, 268–270. [Google Scholar]
- Arzul, L.; Henoux, M.; Marion, F.; Corre, P. Luxation chronique bilatérale des articulations temporo-mandibulaires et syndrome de Meige. Rev. Stomatol. Chir. Maxillo-Faciale Chir. Orale 2015, 116, 106–110. [Google Scholar] [CrossRef]
- Huang, I.-Y.; Chen, C.-M.; Kao, Y.-H.; Wu, C.-W. Management of long-standing mandibular dislocation. Int. J. Oral Maxillofac. Surg. 2011, 40, 810–814. [Google Scholar] [CrossRef]
- Melo, A.R.; Júnior, E.P.; Santos, L.D.M.; Vasconcelos, B.D.E. Recurrent dislocation: Scientific evidence and management following a systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Tocaciu, S.; McCullough, M.J.; Dimitroulis, G. Surgical management of recurrent TMJ dislocation—a systematic review. Oral Maxillofac. Surg. 2019, 23, 35–45. [Google Scholar] [CrossRef]
- Hillam, J.; Isom, B. Mandible Dislocation; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Güven, O. Nearthrosis in true long-standing temporomandibular joint dislocation; a report on pathogenesis and clinical features with review of literature. J. Cranio-Maxillofac. Surg. 2019, 47, 945–950. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, K.; Ding, Y. Modified dextrose prolotherapy for recurrent temporomandibular joint dislocation. Br. J. Oral Maxillofac. Surg. 2014, 52, 63–66. [Google Scholar] [CrossRef]
- Ardehali, M.M.; Tari, N.; Bastaninejad, S.; Amirizad, E. Comparison of different approaches to the reduction of anterior temporomandibular joint dislocation: A randomized clinical trial. Int. J. Oral Maxillofac. Surg. 2016, 45, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.; Harrigan, R.A.; Ufberg, J.; Vilke, G.M. Mandibular reduction. J. Emerg. Med. 2008, 34, 435–440. [Google Scholar] [CrossRef]
- Kummoona, R. Surgical managements of subluxation and dislocation of the temporomandibular joint: Clinical and experimental studies. J. Craniofac. Surg. 2010, 21, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- Forshaw, R.J. Reduction of temporomandibular joint dislocation: An ancient technique that has stood the test of time. Br. Dent. J. 2015, 218, 691–693. [Google Scholar] [CrossRef]
- Lowery, L.E.; Beeson, M.S.; Lum, K.K. The wrist pivot method, a novel technique for temporomandibular joint reduction. J. Emerg. Med. 2004, 27, 167–170. [Google Scholar] [CrossRef]
- Terai, H.; Kasuya, S.; Nakagawa, Y.; Ueno, T. The use of only one hand for the reduction of a temporomandibular joint dislocation: A technique suitable for self-reduction. Int. J. Oral Maxillofac. Surg. 2014, 43, 663–664. [Google Scholar] [CrossRef]
- Liu, M.; Liu, M.; Lv, K. Clinical Trial of Manual Reduction of Temporomandibular Joint Dislocation After Inhalation of Nitrous Oxide. J. Craniofac. Surg. 2019, 30, 2549–2550. [Google Scholar] [CrossRef]
- Xu, J.; Dong, S.; Zhou, H.; Somar, M.; Lv, K.; Li, Z. The Supine Position Technique Method Is Better Than the Conventional Method for Manual Reduction of Acute Nontraumatic Temporomandibular Joint Dislocation. J. Craniofac. Surg. 2016, 27, 919–922. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chen, C.T.; Lin, C.H.; Chen, Y.R. A safe and effective way for reduction of temporomandibular joint dislocation. Ann. Plast. Surg. 2007, 58, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Daelen, B.; Thorwirth, V.; Koch, A. Neurogene Kiefergelenkluxation. Definition und Therapie mit Botulinumtoxin. Nervenarzt 1997, 68, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.-Y.; Chen, H.-M.; Sun, Z.-P.; Zhang, Z.-K.; Ma, X.-C. Long-term efficacy of botulinum toxin type A for the treatment of habitual dislocation of the temporomandibular joint. Br. J. Oral Maxillofac. Surg. 2010, 48, 281–284. [Google Scholar] [CrossRef]
- Bouso, O.V.; González, G.F.; Mommsen, J.; Grau, V.G.; Fernández, J.R.; Micas, M.M. Neurogenic temporomandibular joint dislocation treated with botulinum toxin: Report of 4 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e33–e37. [Google Scholar] [CrossRef]
- Ziegler, C.M.; Haag, C.; Mühling, J. Treatment of recurrent temporomandibular joint dislocation with intramuscular botulinum toxin injection. Clin. Oral Investig. 2003, 7, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, S.; Yoshimura, H.; Kondo, S.; Sano, K. Temporomandibular dislocation caused by pancreatic cancer metastasis: A case report. Oncol. Lett. 2017, 14, 6053–6058. [Google Scholar] [CrossRef] [PubMed]
- Ungor, C.; Atasoy, K.T.; Taskesen, F.; Cezairli, B.; Dayisoylu, E.H.; Tosun, E.; Senel, F.C. Short-term Results of Prolotherapy in the Management of Temporomandibular Joint Dislocation. J. Craniofacial Surg. 2013, 24, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Daif, E.T. Autologous blood injection as a new treatment modality for chronic recurrent temporomandibular joint dislocation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Hegab, A.F. Treatment of chronic recurrent dislocation of the temporomandibular joint with injection of autologous blood alone, intermaxillary fixation alone, or both together: A prospective, randomised, controlled clinical trial. Br. J. Oral Maxillofac. Surg. 2013, 51, 813–817. [Google Scholar] [CrossRef]
- Kato, T.; Shimoyama, T.; Nasu, D.; Kaneko, T.; Horie, N.; Kudo, I. Autologous blood injection into the articular cavity for the treatment of recurrent temporomandibular joint dislocation: A case report. J. Oral Sci. 2007, 49, 237–239. [Google Scholar] [CrossRef]
- Machon, V.; Levorova, J.; Hirjak, D.; Wisniewski, M.; Drahos, M.; Sidebottom, A.; Foltan, R. A prospective assessment of outcomes following the use of autologous blood for the management of recurrent temporomandibular joint dislocation. Oral Maxillofac. Surg. 2018, 22, 53–57. [Google Scholar] [CrossRef]
- Varedi, P.; Bohluli, B. Autologous blood injection for treatment of chronic recurrent TMJ dislocation: Is it successful? Is it safe enough? A systematic review. Oral Maxillofac. Surg. 2015, 19, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, H.; Eriksson, L.; Abrahamsson, P.; Häggman-Henrikson, B. Treatment of temporomandibular joint luxation: A systematic literature review. Clin. Oral Investig. 2020, 24, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.H.; Rahim, A.U. Comparison of mean decrease in mouth opening by autologous blood injection in superior joint space with and without pericapsular tissue in treatment of chronic recurrent temporomandibular joint dislocation in Mayo hospital Lahore. J. Pak. Med. Assoc. 2020, 70, 1878–1882. [Google Scholar] [CrossRef] [PubMed]
- Aamir, M.; Ali, F.; Khan, M.; Khan, I.A.; Khan, U. Autologous Blood Injection for the Treatment of Recurrent Temporomandibular Joint Dislocation. Med. Forum. 2020, 31, 17–20. [Google Scholar]
- Shorey, C.W.; Campbell, J.H. Dislocation of the temporomandibular joint. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Oatis, G.W.; Baker, D.A. The bilateral eminectomy as definitive treatment. Int. J. Oral Surg. 1984, 13, 294–298. [Google Scholar] [CrossRef]
- Sato, J.; Segami, N.; Nishimura, M.; Suzuki, T.; Kaneyama, K.; Fujimura, K. Clinical evaluation of arthroscopic eminoplasty for habitual dislocation of the temporomandibular joint: Comparative study with conventional open eminectomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 390–395. [Google Scholar] [CrossRef]
- Undt, G.; Kermer, C.; Rasse, M. Treatment of recurrent mandibular dislocation, part II: Eminectomy. Int. J. Oral Maxillofac. Surg. 1997, 26, 98–102. [Google Scholar] [CrossRef]
- Jeyaraj, P. Chronic Recurrent Temporomandibular Joint Dislocation: A Comparison of Various Surgical Treatment Options, and Demonstration of the Versatility and Efficacy of the Dautrey’s Procedure. J. Maxillofac. Oral Surg. 2018, 17, 95–106. [Google Scholar] [CrossRef]
- Ihab, R.; Mounir, R.; Mounir, M. Patient-specific titanium onlay eminoplasty: A novel protocol for treatment of recurrent temporomandibular joint dislocation. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 16, e2114. [Google Scholar] [CrossRef]
- Iizuka, T.; Hidaka, Y.; Murakami, K.-I.; Nishida, M. Chronic recurrent anterior luxation of the mandible: A review of 12 patients treated by the LeClerc procedure. Int. J. Oral Maxillofac. Surg. 1988, 17, 170–172. [Google Scholar] [CrossRef]
- Medra, A.M.; Mahrous, A.M. Glenotemporal osteotomy and bone grafting in the management of chronic recurrent dislocation and hypermobility of the temporomandibular joint. Br. J. Oral Maxillofac. Surg. 2008, 46, 119–122. [Google Scholar] [CrossRef]
- Undt, G.; Kermer, C.; Piehslinger, E.; Rasse, M. Treatment of recurrent mandibular dislocation, part I: Leclerc blocking procedure. Int. J. Oral Maxillofac. Surg. 1997, 26, 92–97. [Google Scholar] [CrossRef]
- Ying, B.; Hu, J.; Zhu, S. Modified Leclerc blocking procedure with miniplates and temporal fascial flap for recurrent temporomandibular joint dislocation. J. Craniofac. Surg. 2013, 24, 740–742. [Google Scholar] [CrossRef]
- Georgiade, N. The surgical correction of chronic luxation of the mandibular condyle. Plast. Reconstr. Surg. 1965, 36, 339–342. [Google Scholar] [CrossRef]
- Macfarlane, W.I. Recurrent dislocation of the mandible: Treatment of seven cases by a simple surgical method. Br. J. Oral Surg. 1977, 14, 227–229. [Google Scholar] [CrossRef]
- Torres, D.E.; McCain, J.P. Arthroscopic electrothermal capsulorrhaphy for the treatment of recurrent temporomandibular joint dislocation. Int. J. Oral Maxillofac. Surg. 2012, 41, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Ybema, A.; De Bont, L.G.M.; Spijkervet, F.K.L. Arthroscopic cauterization of retrodiscal tissue as a successful minimal invasive therapy in habitual temporomandibular joint luxation. Int. J. Oral Maxillofac. Surg. 2013, 42, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Dellon, E.S.; Steele, D. Jaw Dislocation as an Unusual Complication of Upper Endoscopy. Case Rep. Gastroenterol. 2016, 10, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Han, I.; Kim, T.K.; Yoo, J.-H.; Park, J.H.; Chung, E.Y. Dislocation of the temporomandibular joint following general anesthesia. Korean J. Anesth. 2014, 67, S113–S114. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
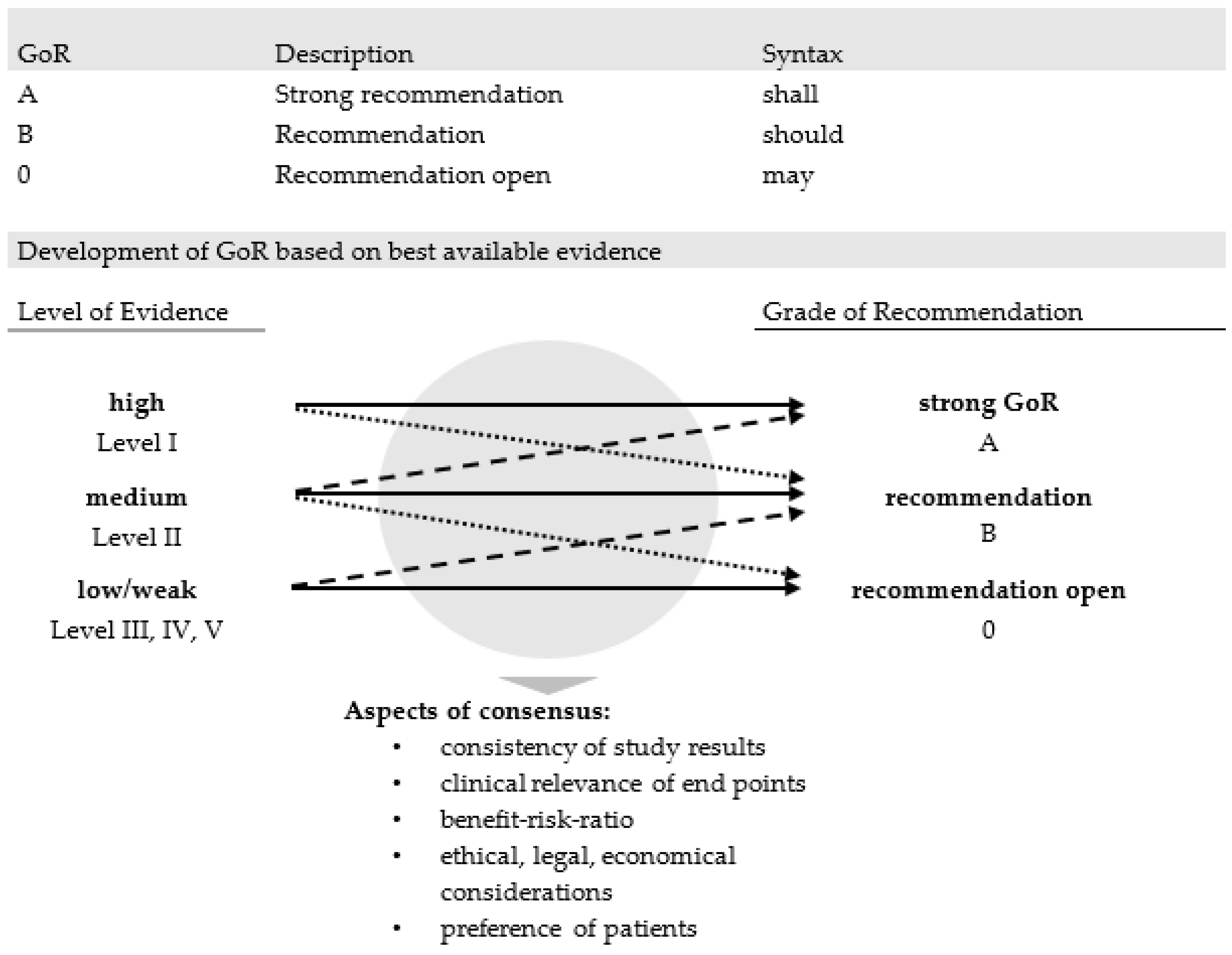
| Grade of Evidence | Study Design | |
|---|---|---|
| I | a | Meta-analysis/systematic review of GoE I papers |
| b | Randomized controlled clinical trial (RCT) | |
| II | a | Meta-analysis/systematic review of GoE II papers |
| b | Controlled clinical trial (CCT)/experimental study with the control group (prospective) | |
| III | a | Meta-analysis/systematic review of GoE III papers |
| b | Retrospective cohort study, retrospective case-control study | |
| IV | a | Meta-analysis/systematic review of GoE IV papers |
| b | Non-controlled case series (<1 subject), animal experiment | |
| V | a | Meta-analysis/systematic review of GoE V papers |
| b | Case report, expert opinion | |
| + | Good quality or sample size n > 100 | |
| − | Poor quality or sample size n < 10 | |
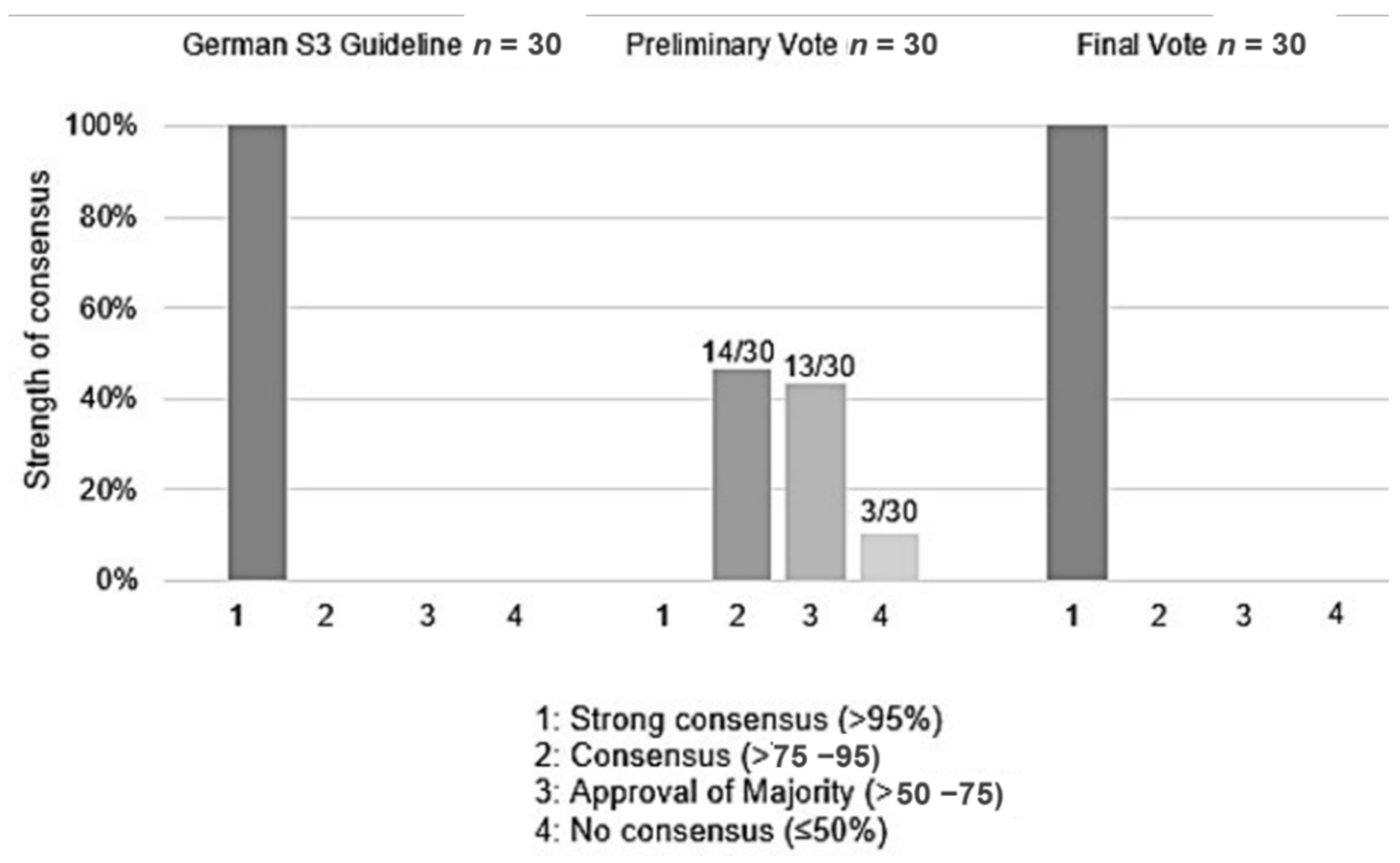
| strong consensus | >95% of participants |
| consensus | >75–95% of participants |
| approval by the majority | >50–75% of participants |
| no consensus | ≤50% of participants |
| 1. Self-reducibility | ||
| fixed | not self-reducible, needs manual reduction (medical intervention) | |
| non-fixed/(“subluxation”) | spontaneously self-reducible | |
| 2. Occurrence of dislocation over time | ||
| one-time | single episode | |
| recurrent | multiple dislocations over time | |
| habitual | dislocations during physiological movements | |
| 3. Duration of dislocation | ||
| acute | recently occurred dislocation | |
| chronic/persistent | dislocation more than 4 weeks | |
| longstanding | adaptive/degenerative changes in or around the joint | |
| Examinations | |
| 1 | Patients without acute facial trauma who for the first time experience a temporomandibular joint dislocation may be diagnosed based on medical history and physical examination (inspection, palpation) if the symptoms are sufficiently indicative of a temporomandibular joint dislocation. |
| 2 | X-rays are not mandatory in standard cases, but imaging examinations should be considered in patients with symptoms allowing for other differential diagnoses to rule out facial fractures and to provide information for further treatment planning. |
| 3 | These optional additional alternative examination methods may be indicated in the post-acute phase for the purposes of revealing pathogenesis and for appraisal of further therapeutic approaches. |
| Treatment | |
| 4 | An attempt at a manual reduction should initially be made in cases of non-traumatic temporomandibular joint dislocation. The earlier reduction is performed, the greater the chances for a successful reduction. |
| 5 | The ESTMJS members have no experience with these alternative repositioning procedures described in the literature. The ESTMJS members, therefore, recommend that any attempt at a manual reduction should initially be made according to the Hippocratic method of reduction, as it has demonstrated a high rate of success according to literature. |
| 6 | Reduction may be performed separately one side at a time or bilaterally. |
| 7 | In the literature, there is a recommendation to use of bite blocks and double gloves to help to prevent bite injuries and associated infections. ESTMJS Members recommend the thumbs should be put on the oblique line instead. |
| 8 | If a reduction is to be performed with the patient in a sitting position, the patient’s head should be stabilized. |
| 9 | The attempt at a manual reduction of an acute dislocation may initially be made without the administration of any medications. |
| 10 | If such attempts are unsuccessful, further attempts should be made under medication (muscle relaxants and/or analgesics) and, if required, under analog sedation or under general anesthesia. |
| 11 | In patients with potential infectious diseases, dementia, etc., unilateral dislocation reduction may also be performed via the extraoral route |
| 12 | In acute dislocations, bandages may be used after reduction to help maintain stabilization. |
| 13 | In cases of recurrent, longstanding and/or habitual dislocations, securing methods should be considered. |
| 14 | Non-surgical methods should have failed before any minimally invasive or open-surgical intervention. |
| 15 | Treatment of recurrent/persistent temporomandibular joint dislocation with botulinum toxin thus far remains an off-label use of the drug. Warnings of the manufacturers regarding the use of and indications for botulinum toxin shall be observed. |
| 16 | The authors of this recommendation, however, are of the opinion that the use of botulinum toxin for the treatment of recurrent dislocations should be included as a potential indication. |
| 17 | If reduction by non-surgical methods remains unsuccessful, e.g., in cases of longstanding dislocations, surgical methods should be considered. |
| 18 | Also, in patients with recurrent dislocations, an indication for open surgical treatment should be established after the failure of non-surgical treatments and/or minimally invasive therapy. |
| 19 | The small sample size, varying follow-up periods, and inhomogeneous target parameters render comparisons and evaluation of long-term effects difficult (damage, recurrence of dislocation). Especially in cases of persisting dislocations, an individualized approach based on the entire range of available surgical methods and procedures should be considered. |
| 20 | After any surgical treatment, patients should, for a few days, eat soft foods only and refrain from opening mouth widely. |
| 21 | Moreover, especially after autologous blood injection therapy and after surgery on the capsular ligament complex immobilization may be indicated. The goal is here to limit the maximum opening of the jaws; rigid fixation is not recommended. |
| 22 | In case of secondary damage such as malocclusion (e.g., anterior open bite due to persisting dislocations refractory to treatment), an individualized approach based on the range of functional surgical procedures for temporomandibular joints as well as reconstructive and orthognathic surgery may be required. |
| Recommendations | |
| 23 | The treatment of temporomandibular joint dislocation should be initiated as early as possible to limit degenerative changes or their progression, resulting from recurrent dislocation or increasing dislocation rate, and thus to enhance the chances of success of conservative/minimally invasive treatment methods. |
| 24 | The treatment which has the best chance of success is dependent on numerous factors (pathogenesis, age of patient, secondary diagnoses, compliance, treatment goals, care structures, among others). Thus, the best treatment for each individual patient should be determined based on a thorough medical history and physical examination. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neff, A.; McLeod, N.; Spijkervet, F.; Riechmann, M.; Vieth, U.; Kolk, A.; Sidebottom, A.J.; Bonte, B.; Speculand, B.; Saridin, C.; et al. The ESTMJS (European Society of Temporomandibular Joint Surgeons) Consensus and Evidence-Based Recommendations on Management of Condylar Dislocation. J. Clin. Med. 2021, 10, 5068. https://doi.org/10.3390/jcm10215068
Neff A, McLeod N, Spijkervet F, Riechmann M, Vieth U, Kolk A, Sidebottom AJ, Bonte B, Speculand B, Saridin C, et al. The ESTMJS (European Society of Temporomandibular Joint Surgeons) Consensus and Evidence-Based Recommendations on Management of Condylar Dislocation. Journal of Clinical Medicine. 2021; 10(21):5068. https://doi.org/10.3390/jcm10215068
Chicago/Turabian StyleNeff, Andreas, Niall McLeod, Frederik Spijkervet, Merle Riechmann, Ulla Vieth, Andreas Kolk, Andrew J. Sidebottom, Bernard Bonte, Bernard Speculand, Carrol Saridin, and et al. 2021. "The ESTMJS (European Society of Temporomandibular Joint Surgeons) Consensus and Evidence-Based Recommendations on Management of Condylar Dislocation" Journal of Clinical Medicine 10, no. 21: 5068. https://doi.org/10.3390/jcm10215068
APA StyleNeff, A., McLeod, N., Spijkervet, F., Riechmann, M., Vieth, U., Kolk, A., Sidebottom, A. J., Bonte, B., Speculand, B., Saridin, C., Wilms, C. T., Politis, C., Ângelo, D. F., Hirjak, D., Aagaard, E., Spallaccia, F., Monje, F., Undt, G., Gerbino, G., ... Skroch, L. (2021). The ESTMJS (European Society of Temporomandibular Joint Surgeons) Consensus and Evidence-Based Recommendations on Management of Condylar Dislocation. Journal of Clinical Medicine, 10(21), 5068. https://doi.org/10.3390/jcm10215068