
The Role of Hemoglobin A1C in Diabetes Screening and Diabetic Retinopathy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Studied Subjects
2.3. Assessments
2.4. Definition of Diabetes Mellitus by FPG, 2hPG, and A1C
2.5. Laboratory Methods
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Comparison of Diagnosis of Diabetes Mellitus Using the Plasma Glucose and A1C Criteria
3.3. Impact of Gender on the Diagnosis of Diabetes Mellitus Using the Plasma Glucose and A1C Criteria
3.4. Impact of Race/Ethnicity on the Diagnosis of Diabetes Mellitus Using the Plasma Glucose and A1C Criteria
3.5. Impact of Age on the Diagnosis of Diabetes Mellitus Using the Plasma Glucose and A1C Criteria
3.6. Impact of Body Mass Index on the Diagnosis of Diabetes Mellitus Using the Plasma Glucose and A1C Criteria
3.7. Clinical Characteristics of Defined by Different Diagnostic Criteria of Diabetes
3.8. Alternative A1C Criteria for the Diagnosis of Diabetes Mellitus
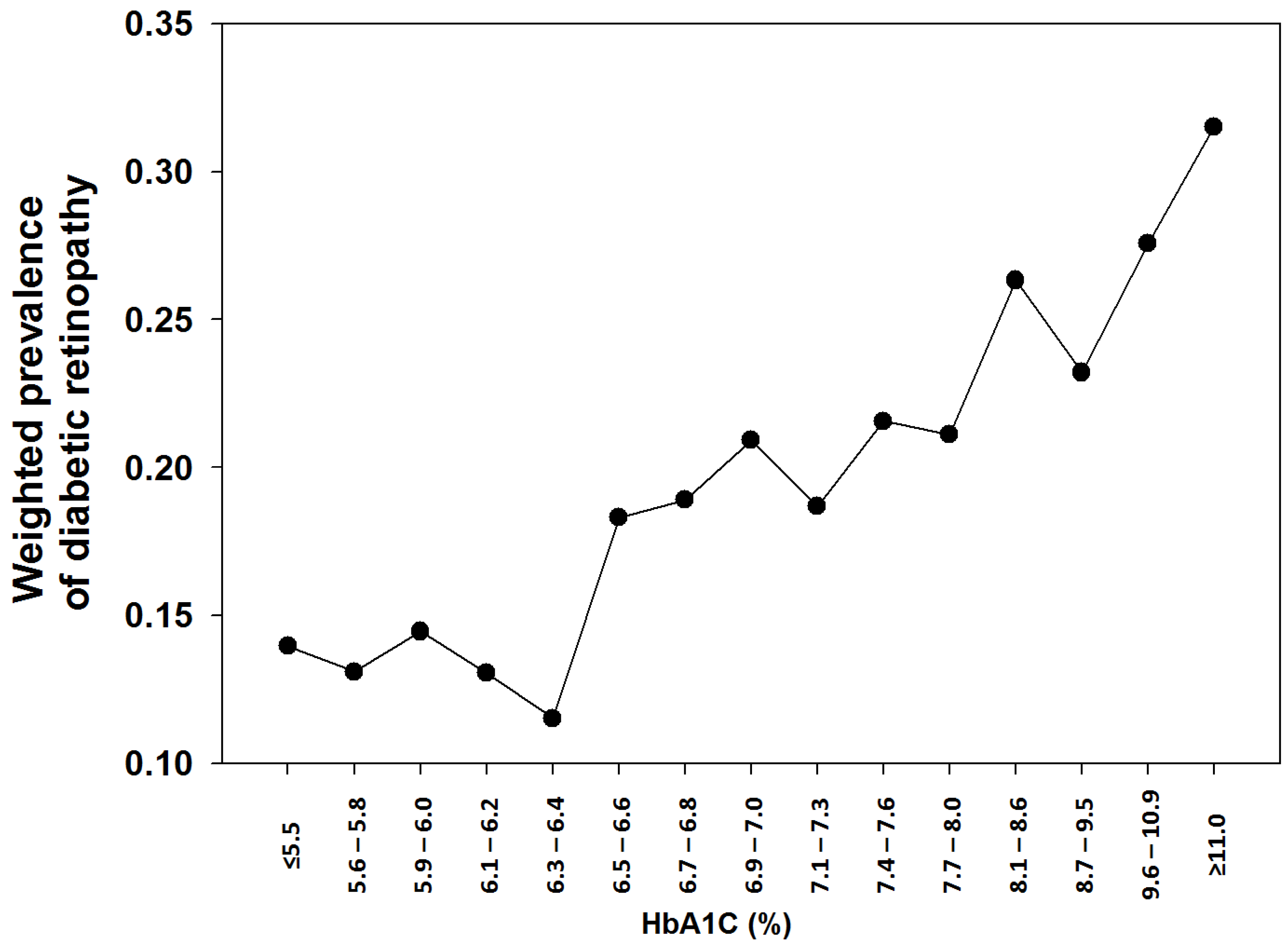
3.9. Diabetic Retinopathy in Established Diabetic Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fang, M. Trends in the Prevalence of Diabetes Among U.S. Adults: 1999–2016. Am. J. Prev. Med. 2018, 55, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report 2020; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf (accessed on 24 April 2021).
- Gillett, M.J. International Expert Committee Report on the Role of the A1C Assay in the Diagnosis of Diabetes. Clin. Biochem. Rev. 2009, 32, 1327–1334. [Google Scholar]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasso, F.C.; Pafundi, P.C.; Simeon, V.; De Nicola, L.; Chiodini, P.; Galiero, R.; Rinaldi, L.; Nevola, R.; Salvatore, T.; Sardu, C.; et al. Efficacy and durability of multifactorial intervention on mortality and MACEs: A randomized clinical trial in type-2 diabetic kidney disease. Cardiovasc. Diabetol. 2021, 20, 145. [Google Scholar] [CrossRef] [PubMed]
- Hattersley, A.; Turner, R.; Patel, P.; O’Rahilly, S.; Wainscoat, J.; Permutt, M.; Tanazawa, Y.; Chin, K.; Watkins, P. Linkage of type 2 diabetes to the glucokinase gene. Lancet 1992, 339, 1307–1310. [Google Scholar] [CrossRef]
- American Diabetes Association. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997, 20, 1183–1197. [Google Scholar] [CrossRef]
- Karnchanasorn, R.; Huang, J.; Ou, H.-Y.; Feng, W.; Chuang, L.-M.; Chiu, K.C.; Samoa, R. Comparison of the Current Diagnostic Criterion of HbA1c with Fasting and 2-Hour Plasma Glucose Concentration. J. Diabetes Res. 2016, 2016, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, S. An abnormal hemoglobin in red cells of diabetics. Clin. Chim. Acta 1968, 22, 296–298. [Google Scholar] [CrossRef]
- Koenig, R.J.; Peterson, C.M.; Jones, R.L.; Saudek, C.; Lehrman, M.; Cerami, A. Correlation of Glucose Regulation and Hemoglobin AIcin Diabetes Mellitus. N. Engl. J. Med. 1976, 295, 417–420. [Google Scholar] [CrossRef]
- World Health Organization. Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus; WHO, Ed.; WHO Reference Number: WHO/NMH/CHP/CPM/11.1; WHO: Geneva, Switzerland, 2011; Available online: https://www.who.int/diabetes/publications/report-hba1c_2011.pdf. (accessed on 24 April 2021).
- Lu, C.L.; Perera, R.; Farrah, H.; Waring, J. Diabetes screening among active tuberculosis patients in Western Australia Tuberculosis Control Program using HbA1c. Intern. Med. J. 2018, 49, 630–633. [Google Scholar] [CrossRef]
- Mataftsi, M.; Koukos, G.; Sakellari, D. Prevalence of undiagnosed diabetes and pre-diabetes in chronic periodontitis patients assessed by an HbA1c chairside screening protocol. Clin. Oral Investig. 2019, 23, 4365–4370. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Chan, V.W.; Chan, P.; Woo, Y.; Fu, H.; Cheung, A.; Cheung, M.; Yan, C.; Chiu, K. Universal haemoglobin A1c screening reveals high prevalence of dysglycaemia in patients undergoing total knee arthroplasty. Hong Kong Med. J. 2020, 26, 32764157. [Google Scholar] [CrossRef]
- Krass, I.; Carter, R.; Mitchell, B.; Mohebbi, M.; Shih, S.T.F.; Trinder, P.; Versace, V.; Wilson, F.; Mc Namara, K. Pharmacy Diabetes Screening Trial: Protocol for a pragmatic cluster-randomised controlled trial to compare three screening methods for undiagnosed type 2 diabetes in Australian community pharmacy. BMJ Open 2017, 7, e017725. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Moellering, D.; Garvey, W.T. Use of HbA1c for Diagnoses of Diabetes and Prediabetes: Comparison with Diagnoses Based on Fasting and 2-Hr Glucose Values and Effects of Gender, Race, and Age. Metab. Syndr. Relat. Disord. 2014, 12, 258–268. [Google Scholar] [CrossRef] [Green Version]
- Kirk, J.K.; D’Agostino, R.B.; Bell, R.A.; Passmore, L.V.; Bonds, D.E.; Karter, A.J.; Narayan, K.V. Disparities in HbA1c Levels Between African-American and Non-Hispanic White Adults With Diabetes: A meta-analysis. Diabetes Care 2006, 29, 2130–2136. [Google Scholar] [CrossRef] [Green Version]
- Bergenstal, R.M.; Gal, R.L.; Connor, C.G.; Gubitosi-Klug, R.; Kruger, D.; Olson, B.A.; Willi, S.; Aleppo, G.; Weinstock, R.S.; Wood, J.; et al. Racial Differences in the Relationship of Glucose Concentrations and Hemoglobin A1c Levels. Ann. Intern. Med. 2017, 167, 95–102. [Google Scholar] [CrossRef]
- Massin, P.; Lange, C.; Tichet, J.; Vol, S.; Erginay, A.; Cailleau, M.; Eschwege, E.; Balkau, B. Hemoglobin A1c and Fasting Plasma Glucose Levels as Predictors of Retinopathy at 10 Years. Arch. Ophthalmol. 2011, 129, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Fajans, S.S.; Herman, W.H.; Oral, E. Insufficient sensitivity of hemoglobin A1C determination in diagnosis or screening of early diabetic states. Metabolism 2011, 60, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Meijnikman, A.S.; Block, C.E.M.D.; Dirinck, E.; Verrijken, A.; Mertens, I.; Corthouts, B.; Van Gaal, L.F. Not performing an OGTT results in significant underdiagnosis of (pre)diabetes in a high risk adult Caucasian population. Int. J. Obes. 2017, 41, 1615–1620. [Google Scholar] [CrossRef]
- Cowie, C.C.; Rust, K.F.; Byrd-Holt, D.D.; Gregg, E.; Ford, E.S.; Geiss, L.S.; Bainbridge, K.E.; Fradkin, J.E. Prevalence of Diabetes and High Risk for Diabetes Using A1C Criteria in the U.S. Population in 1988–2006. Diabetes Care 2010, 33, 562–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, C.M.; Guo, M.; Dharmage, S. HbA1cas a screening tool for detection of Type 2 diabetes: A systematic review. Diabet. Med. 2007, 24, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Vinod, K.V.; Radhakrishna, P.; Sujiv, A.; Swaminathan, R.P. Comparison of Hemoglobin A1c with fasting and 2-h plasma glucose tests for diagnosis of diabetes and prediabetes among high-risk South Indians. Indian J. Endocrinol. Metab. 2018, 22, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Kuenen, J.; Borg, R.; Zheng, H.; Schoenfeld, D.; Heine, R.J. Translating the A1C Assay Into Estimated Average Glucose Values. Diabetes Care 2008, 31, 1473–1478. [Google Scholar] [CrossRef] [Green Version]
- Wei, N.; Zheng, H.; Nathan, D.M. Empirically Establishing Blood Glucose Targets to Achieve HbA 1c Goals. Diabetes Care 2014, 37, 1048–1051. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Postprandial blood glucose. American Diabetes Association. Diabetes Care 2001, 24, 775–778. [Google Scholar] [CrossRef] [Green Version]
- Engelgau, M.M.; Thompson, T.J.; Herman, W.H.; Boyle, J.P.; Aubert, R.E.; Kenny, S.J.; Badran, A.; Sous, E.S.; Ali, M.A. Comparison of Fasting and 2-Hour Glucose and HbA1c Levels for Diagnosing Diabetes: Diagnostic criteria and performance revisited. Diabetes Care 1997, 20, 785–791. [Google Scholar] [CrossRef]
- McCane, D.R.; Hanson, R.L.; Charles, M.A.; Jacobsson, L.T.H.; Pettitt, D.D.; Bennett, P.H.; Knowler, W.C. Comparison of tests for glycated haemoglobin and fasting and two hour plasma glucose concentrations as diagnostic methods for diabetes. BMJ 1994, 308, 1323–1328. [Google Scholar] [CrossRef] [Green Version]
- Tsugawa, Y.; Takahashi, O.; Meigs, J.B.; Davis, R.B.; Imamura, F.; Fukui, T.; Taylor, W.C.; Wee, C.C. New Diabetes Diagnostic Threshold of Hemoglobin A1c and the 3-Year Incidence of Retinopathy. Diabetes 2012, 61, 3280–3284. [Google Scholar] [CrossRef] [Green Version]
- Selvin, E.; Ning, Y.; Steffes, M.W.; Bash, L.D.; Klein, R.; Wong, T.Y.; Astor, B.C.; Sharrett, A.R.; Brancati, F.L.; Coresh, J. Glycated Hemoglobin and the Risk of Kidney Disease and Retinopathy in Adults With and Without Diabetes. Diabetes 2011, 60, 298–305. [Google Scholar] [CrossRef] [Green Version]
- Tsugawa, Y.; Mukamal, K.J.; Davis, R.B.; Taylor, W.C.; Wee, C.C. Should the Hemoglobin A1cDiagnostic Cutoff Differ Between Blacks and Whites? Ann. Intern. Med. 2012, 157, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.J.; Gregg, E.W.; Geiss, L.S.; Imperatore, G.; Williams, D.E.; Zhang, X.; Albright, A.L.; Cowie, C.C.; Klein, R.; Saaddine, J.B. Association of A1C and Fasting Plasma Glucose Levels With Diabetic Retinopathy Prevalence in the U.S. Population: Implications for diabetes diagnostic thresholds. Diabetes Care 2009, 32, 2027–2032. [Google Scholar] [CrossRef] [Green Version]
- Kempen, J.H.; O’Colmain, B.J.; Leske, M.C.; Haffner, S.M.; Klein, R.; Moss, S.E.; Taylor, H.R.; Hamman, R.F.; Eye Diseases Prevalence Research Group. The Prevalence of Diabetic Retinopathy among Adults in the United States. Arch. Ophthalmol. 2004, 122, 552–563. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Saaddine, J.B.; Chou, C.-F.; Cotch, M.F.; Cheng, Y.; Geiss, L.S.; Gregg, E.; Albright, A.L.; Klein, B.E.K.; Klein, R. Prevalence of Diabetic Retinopathy in the United States, 2005–2008. JAMA 2010, 304, 649–656. [Google Scholar] [CrossRef]
- Galiero, R.; Pafundi, P.C.; Nevola, R.; Rinaldi, L.; Acierno, C.; Caturano, A.; Salvatore, T.; Adinolfi, L.E.; Costagliola, C.; Sasso, F.C. The Importance of Telemedicine during COVID-19 Pandemic: A Focus on Diabetic Retinopathy. J. Diabetes Res. 2020, 2020, 9036847. [Google Scholar] [CrossRef]
- Sasso, F.C.; Pafundi, P.C.; Gelso, A.; Bono, V.; Costagliola, C.; Marfella, R.; Sardu, C.; Rinaldi, L.; Galiero, R.; Acierno, C.; et al. Telemedicine for screening diabetic retinopathy: The NO BLIND Italian multicenter study. Diabetes Metab. Res. Rev. 2018, 35, e3113. [Google Scholar] [CrossRef]


{kind=link}
| Mean (n) | STD (%) | |||
|---|---|---|---|---|
| n | 10,416 | |||
| Age | Years | 48 | ± | 17 |
| Gender | Female | 5256 | 50.46% | |
| Body mass index | kg/m2 | 28.57 | ± | 6.62 |
| Hemoglobin A1C | % | 5.5 | ± | 0.6 |
| Hemoglobin A1C | mmol/mol | 37 | ± | 6.6 |
| Fasting plasma glucose | mmol/L | 5.6 | ± | 1.0 |
| 2-h postchallenged plasma glucose | mmol/L | 6.6 | ± | 2.8 |
| Mexican Americans | 1670 | 16.03% | ||
| Other Hispanics | 1058 | 10.16% | ||
| Non-Hispanic Whites | 4768 | 45.78% | ||
| Non-Hispanic Blacks | 1884 | 18.09% | ||
| Others | 1036 | 9.95% |
| Diabetes by FPG/2hPG | Total (n) | Diabetes by A1C | Diabetes by A1C | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Unweighted | Weighted | ||||||||
| n | % | % | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | |||
| 95% CI | 95%CI | 95%CI | 95%CI | ||||||
| a. All subjects | |||||||||
| All | No | 9607 | 53 | 0.55% | 0.30% | 25.90% | 99.70% | 84.07% | 95.70% |
| Yes | 809 | 217 | 26.82% | 25.90% | (25.87–25.92) | (99.70–99.70) | (84.03–84.10) | (95.70–95.70) | |
| b. Gender | |||||||||
| Female | No | 4877 | 23 | 0.47% | 0.29% | 24.52% | 99.71% | 83.34% | 95.75% |
| Yes | 379 | 99 | 26.12% | 24.52% | (24.49–24.56) | (99.71–99.71) | (83.29–83.40) | (96.75–95.76) | |
| Male | No | 4730 | 30 | 0.63% | 0.31% | 27.31% | 99.69% | 84.74% | 95.64% |
| Yes | 430 | 118 | 27.44% | 27.31% | (27.27–27.34) | (96.69–96.69) | (84.69–84.80) | (95.64–95.65) | |
| c. Race/ethnicity | |||||||||
| Mexican American | No | 1518 | 4 | 0.26% | 0.21% | 34.90% | 99.79% | 92.71% | 95.18% |
| Yes | 152 | 45 | 29.61% | 34.90% | (34.81–34.98) | (99.78–99.79) | (92.63–92.79) | (95.17–95.19) | |
| Other Hispanic | No | 966 | 8 | 0.83% | 0.52% | 27.38% | 99.48% | 76.58% | 95.69% |
| Yes | 92 | 22 | 23.91% | 27.38% | (27.27–27.49) | (99.48–99.49) | (76.40–76.75) | (95.68–96.70) | |
| Non-Hispanic White | No | 4380 | 8 | 0.18% | 0.14% | 21.35% | 99.86% | 90.62% | 95.36% |
| Yes | 388 | 80 | 20.62% | 21.35% | (21.32–21.38) | (99.86–99.86) | (90.58–90.66) | (95.35–95.36) | |
| Non-Hispanic Black | No | 1775 | 29 | 1.63% | 1.30% | 41.27% | 98.70% | 59.57% | 97.31% |
| Yes | 109 | 44 | 40.37% | 41.27% | (41.17–41.37) | (98.70–98.71) | (59.45–59.69) | (97.31–97.32) | |
| Other | No | 968 | 4 | 0.41% | 0.23% | 41.55% | 99.77% | 89.72% | 97.29% |
| Yes | 68 | 26 | 38.24% | 41.55% | (41.43–41.67) | (99.77–99.78) | (89.61–89.83) | (97.28–97.30) | |
| d. Age (years) | |||||||||
| 20–29 | No | 1860 | 0 | 0.00% | 0.00% | 14.32% | 100.00% | 100.00% | 99.07% |
| Yes | 27 | 6 | 22.22% | 14.32% | (14.22–14.43) | (100.00–100.00) | (100.00–100.00) | (99.07–99.08) | |
| 30–39 | No | 1867 | 2 | 0.11% | 0.08% | 36.21% | 99.92% | 91.94% | 98.36% |
| Yes | 65 | 28 | 43.08% | 36.21% | (36.12–36.31) | (99.92–99.92) | (91.85–92.02) | (98.35–98.36) | |
| 40–49 | No | 1846 | 7 | 0.38% | 0.27% | 29.38% | 99.73% | 83.13% | 96.86% |
| Yes | 97 | 30 | 30.93% | 29.38% | (29.31–29.45) | (99.73–99.73) | (83.03–83.22) | (96.86–96.87) | |
| 50–59 | No | 1526 | 12 | 0.79% | 0.45% | 32.57% | 99.55% | 82.99% | 95.62% |
| Yes | 142 | 52 | 36.62% | 32.57% | (32.51–32.63) | (99.55–99.55) | (82.91–83.07) | (95.61–95.63) | |
| 60–69 | No | 1293 | 17 | 1.31% | 0.66% | 29.81% | 99.34% | 83.14% | 92.80% |
| Yes | 194 | 55 | 28.35% | 29.81% | (29.75–29.87) | (99.33–99.34) | (83.06–83.22) | (92.79–92.81) | |
| ≥70 | No | 1215 | 15 | 1.23% | 0.78% | 15.81% | 99.22% | 81.44% | 84.45% |
| Yes | 284 | 46 | 16.20% | 15.81% | (15.77–15.85) | (99.21–99.22) | (81.35–81.54) | (84.43–84.46) | |
| e. BMI (kg/m2) | |||||||||
| <22.50 | No | 1550 | 1 | 0.06% | 0.03% | 7.21% | 99.97% | 80.89% | 98.21% |
| Yes | 51 | 6 | 11.76% | 7.21% | (7.14–7.27) | (99.97–99.97) | (80.56–81.22) | (98.20–98.21) | |
| 22.50–24.99 | No | 1591 | 7 | 0.44% | 0.15% | 18.37% | 99.85% | 82.76% | 96.88% |
| Yes | 93 | 17 | 18.28% | 18.37% | (18.30–18.44) | (99.85–99.85) | (82.61–82.90) | (96.80–96.89) | |
| 25.00–27.49 | No | 1730 | 4 | 0.23% | 0.09% | 12.44% | 99.91% | 88.03% | 95.64% |
| Yes | 137 | 22 | 16.06% | 12.44% | (12.39–12.49) | (99.91–99.91) | (87.90–88.15) | (95.63–95.65) | |
| 27.50–29.99 | No | 1584 | 7 | 0.44% | 0.29% | 14.85% | 99.71% | 75.34% | 95.09% |
| Yes | 142 | 29 | 20.42% | 14.85% | (14.80–14.90) | (99.70–99.71) | (75.20–75.48) | (95.08–95.09) | |
| 30.00–32.49 | No | 1112 | 11 | 0.99% | 0.41% | 32.06% | 99.59% | 84.25% | 95.59% |
| Yes | 106 | 33 | 31.13% | 32.06% | (31.98–32.13) | (99.59–99.60) | (84.15–84.35) | (95.58–95.60) | |
| 32.50–34.99 | No | 758 | 1 | 0.13% | 0.06% | 34.48% | 99.94% | 97.68% | 95.07% |
| Yes | 77 | 30 | 38.96% | 34.48% | (34.39–34.56) | (99.93–99.94) | (97.64–97.73) | (95.06–95.08) | |
| 35.00–37.49 | No | 474 | 10 | 2.11% | 1.50% | 28.23% | 98.50% | 70.38% | 91.55% |
| Yes | 75 | 20 | 26.67% | 28.23% | (28.14–28.31) | (98.49–98.50) | (70.25–70.51) | (91.53–91.57) | |
| ≥37.50 | No | 808 | 12 | 1.49% | 0.92% | 46.02% | 99.08% | 87.01% | 93.18% |
| Yes | 128 | 60 | 46.88% | 46.02% | (45.95–46.08) | (99.07–99.08) | (86.95–87.07) | (93.17–93.19) | |
| Non-Diabetic by Both A1C and FPG/2hPG | Diabetic by FPG/2hPG but not A1C | Diabetic by FPG/2hPG and A1C | Diabetic by A1C But Not FPG/2hPG | p * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (unweighted percent) | 9554 | 91.72% | 592 | 5.68% | 217 | 2.08% | 53 | 0.51% | ||
| weighted percent | 94.02% | 4.22% | 1.48% | 0.28% | ||||||
| Age | Years | 45 | (45–45) | 62 | (59–61) | 56 | (54–58) | 62 | (55–65) | 0.01 |
| Gender (weighted percent) | Female | 52.23% | 51.57% | 47.95% | 50.57% | <0.0001 | ||||
| Body mass index | kg/m2 | 28.30 | (28.17–28.43) | 30.19 | (30.06–31.17) | 33.45 | (33.62–35.49) | 33.99 | (32.58–36.87) | <0.0001 |
| Race/ethnicity (weighted percent) | <0.0001 | |||||||||
| Mexican Americans | 8.22% | 9.27% | 14.22% | 5.90% | ||||||
| Other Hispanics | 5.41% | 5.43% | 5.86% | 9.45% | ||||||
| Non-Hispanic Whites | 68.54% | 74.30% | 57.71% | 31.51% | ||||||
| Non-Hispanic Blacks | 10.80% | 6.64% | 13.34% | 47.78% | ||||||
| Others | 7.02% | 4.36% | 8.87% | 5.36% | ||||||
| Hemoglobin A1C | % | 5.4 | (5.3–5.4) | 5.8 | (5.7–5.8) | 7.8 | (7.6–7.8) | 6.6 | (6.3–6.9) | <0.0001 |
| Hemoglobin A1C | mmol/mol | 36 | (34–36) | 40 | (39–40) | 62 | (60–62) | 49 | (45–52) | <0.0001 |
| FPG | mmol/L | 5.4 | (5.4–5.4) | 6.7 | (6.5–6.8) | 9.5 | (9.2–9.7) | 6.3 | (5.7–6.7) | <0.0001 |
| 2hPG | mmol/L | 5.9 | (5.9–5.9) | 11.7 | (11.5–12.0) | 17.0 | (16.3–17.2) | 8.2 | (7.2–9.2) | <0.0001 |
| FPG ≥ 7.0 mmol/L only | - | 21.37% | 6.62% | - | <0.0001 | |||||
| 2hPG ≥ 11.1 mmol/L only | - | 59.72% | 14.16% | - | ||||||
| Both FPG ≥ 7.0 mmol/L and 2hPG ≥ 11.1 mmol/L | - | 18.90% | 79.22% | - | ||||||
| Prevalence of Newly Defined Diabetes by A1c | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | Area under ROC | |
|---|---|---|---|---|---|---|
| A1C ≥ 5.5% (37 mmol/mol) | 37.11% | 84.47% | 60.64% | 11.48% | 98.48% | 0.8353 |
| (37.11–37.12) | (84.45–84.49) | (60.64–60.65) | (11.48–11.49) | (98.47–98.48) | ||
| A1C ≥ 5.6% (38 mmol/mol) | 27.68% | 78.84% | 70.64% | 13.96% | 98.22% | 0.8289 |
| (27.68–27.69) | (78.81–78.86) | (70.63–70.65) | (13.95–13.97) | (98.22–98.22) | ||
| A1C ≥ 5.7% (39 mmol/mol) | 19.27% | 73.00% | 79.56% | 17.76% | 97.99% | 0.8251 |
| (19.27–19.28) | (72.97–73.02) | (79.56–79.57) | (17.74–17.77) | (97.99–97.99) | ||
| A1C ≥ 5.8% (40 mmol/mol) | 12.96% | 65.24% | 86.25% | 22.29% | 97.62% | 0.8222 |
| (12.96–12.97) | (65.21–65.27) | (86.25–86.26) | (22.28–22.31) | (97.62–97.62) | ||
| A1C ≥ 5.9% (41 mmol/mol) | 8.39% | 58.62% | 91.11% | 28.49% | 97.33% | 0.8162 |
| (8.38–8.39) | (58.59–58.64) | (91.10–91.11) | (28.47–28.51) | (97.33–97.33) | ||
| A1C ≥ 6.0% (42 mmol/mol) | 5.23% | 51.75% | 94.46% | 36.08% | 97.00% | 0.8108 |
| (5.22–5.23) | (51.72–51.78) | (94.45–94.46) | (36.057–36.10) | (97.00–97.01) | ||
| A1C ≥ 6.1% (43 mmol/mol) | 3.15% | 45.44% | 96.66% | 45.14% | 96.70% | 0.8055 |
| (3.15–3.15) | (45.41–45.47) | (96.66–96.66) | (45.11–45.17) | (96.70–96.70) | ||
| A1C ≥ 6.2% (44 mmol/mol) | 1.73% | 40.69% | 98.17% | 57.31% | 96.48% | 0.8047 |
| (1.73–1.73) | (40.66–40.71) | (98.17–98.17) | (57.27–57.34) | (96.47–96.48) | ||
| A1C ≥ 6.3% (45 mmol/mol) | 0.95% | 36.28% | 99.00% | 68.62% | 96.26% | 0.8034 |
| 0.94–0.95) | (36.25–36.31) | (99.00–99.00) | (68.58–68.65) | (96.25–96.26) | ||
| A1C ≥ 6.4% (46 mmol/mol) | 0.53% | 30.14% | 99.43% | 76.29% | 95.93% | 0.7994 |
| (0.53–0.53) | (30.11–30.17) | (99.43–99.43) | (76.25–76.33) | (95.92–95.93) |
| A1C | Unweighted | Weighted | |||
|---|---|---|---|---|---|
| Total | Retinopathy | Retinopathy | |||
| n | n | % | % | 95% CI | |
| ≤5.5 (37 mmol/mol) | 251 | 38 | 15.14% | 13.97% | (13.91–14.03) |
| 5.6–5.8 (38–40 mmol/mol) | 283 | 38 | 13.43% | 13.10% | (13.05–13.15) |
| 5.9–6.0 (41–42 mmol/mol) | 253 | 36 | 14.23% | 14.46% | (14.40–14.52) |
| 6.1–6.2 (43–44 mmol/mol) | 245 | 49 | 20.00% | 13.05% | (13.00–13.11) |
| 6.3–6.4 (45–46 mmol/mol) | 301 | 33 | 10.96% | 11.52% | (11.47–11.57) |
| 6.5–6.6 (48–49 mmol/mol) | 257 | 52 | 20.23% | 18.32% | (18.25–18.38) |
| 6.7–6.8 (50–51 mmol/mol) | 256 | 59 | 23.05% | 18.92% | (18.85–18.98) |
| 6.9–7.0 (52–53 mmol/mol) | 227 | 41 | 18.06% | 20.93% | (20.85–21.01) |
| 7.1–7.3 (54–56 mmol/mol) | 295 | 62 | 21.02% | 18.69% | (18.63–18.75) |
| 7.4–7.6 (57–60 mmol/mol) | 249 | 60 | 24.10% | 21.57% | (21.50–21.64) |
| 7.7–8.0 (61–64 mmol/mol) | 265 | 61 | 23.02% | 21.11% | (21.03–21.18) |
| 8.1–8.6 (65–70 mmol/mol) | 270 | 77 | 28.52% | 26.33% | (26.26–26.41) |
| 8.7–9.5 (72–80 mmol/mol) | 260 | 73 | 28.08% | 23.22% | (23.14–23.29) |
| 9.6–10.9 (81–96 mmol/mol) | 244 | 76 | 31.15% | 27.57% | (27.49–27.65) |
| ≥11.0 (97 mmol/mol) | 251 | 76 | 30.28% | 31.52% | (31.43–31.61) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang Villacreses, M.M.; Karnchanasorn, R.; Ou, H.-Y.; Samoa, R.; Chuang, L.-M.; Chiu, K.C. The Role of Hemoglobin A1C in Diabetes Screening and Diabetic Retinopathy. J. Clin. Med. 2021, 10, 4947. https://doi.org/10.3390/jcm10214947
Chang Villacreses MM, Karnchanasorn R, Ou H-Y, Samoa R, Chuang L-M, Chiu KC. The Role of Hemoglobin A1C in Diabetes Screening and Diabetic Retinopathy. Journal of Clinical Medicine. 2021; 10(21):4947. https://doi.org/10.3390/jcm10214947
Chicago/Turabian StyleChang Villacreses, Maria Mercedes, Rudruidee Karnchanasorn, Horng-Yih Ou, Raynald Samoa, Lee-Ming Chuang, and Ken C. Chiu. 2021. "The Role of Hemoglobin A1C in Diabetes Screening and Diabetic Retinopathy" Journal of Clinical Medicine 10, no. 21: 4947. https://doi.org/10.3390/jcm10214947
APA StyleChang Villacreses, M. M., Karnchanasorn, R., Ou, H.-Y., Samoa, R., Chuang, L.-M., & Chiu, K. C. (2021). The Role of Hemoglobin A1C in Diabetes Screening and Diabetic Retinopathy. Journal of Clinical Medicine, 10(21), 4947. https://doi.org/10.3390/jcm10214947