
Blue Laser (450 nm) Treatment of Solar Lentigines


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Blue laser Source
2.2. Patients and Treatment Methods
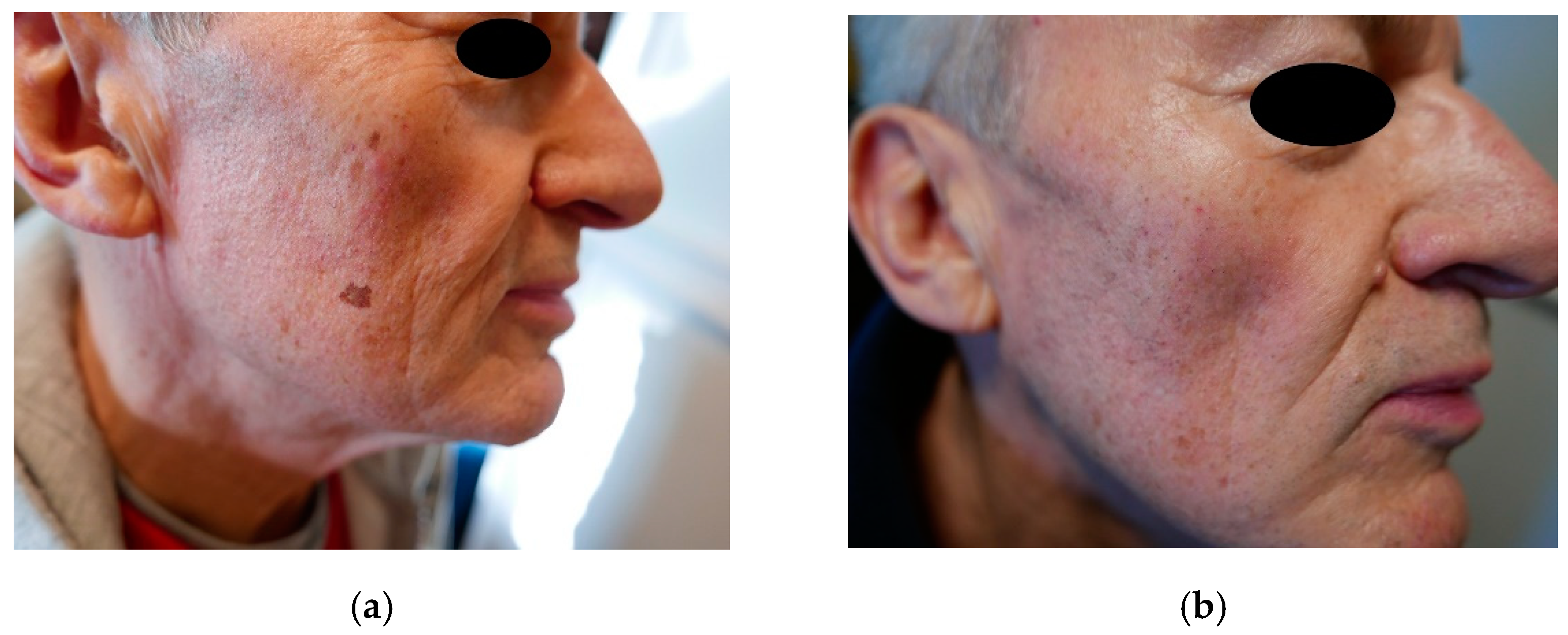
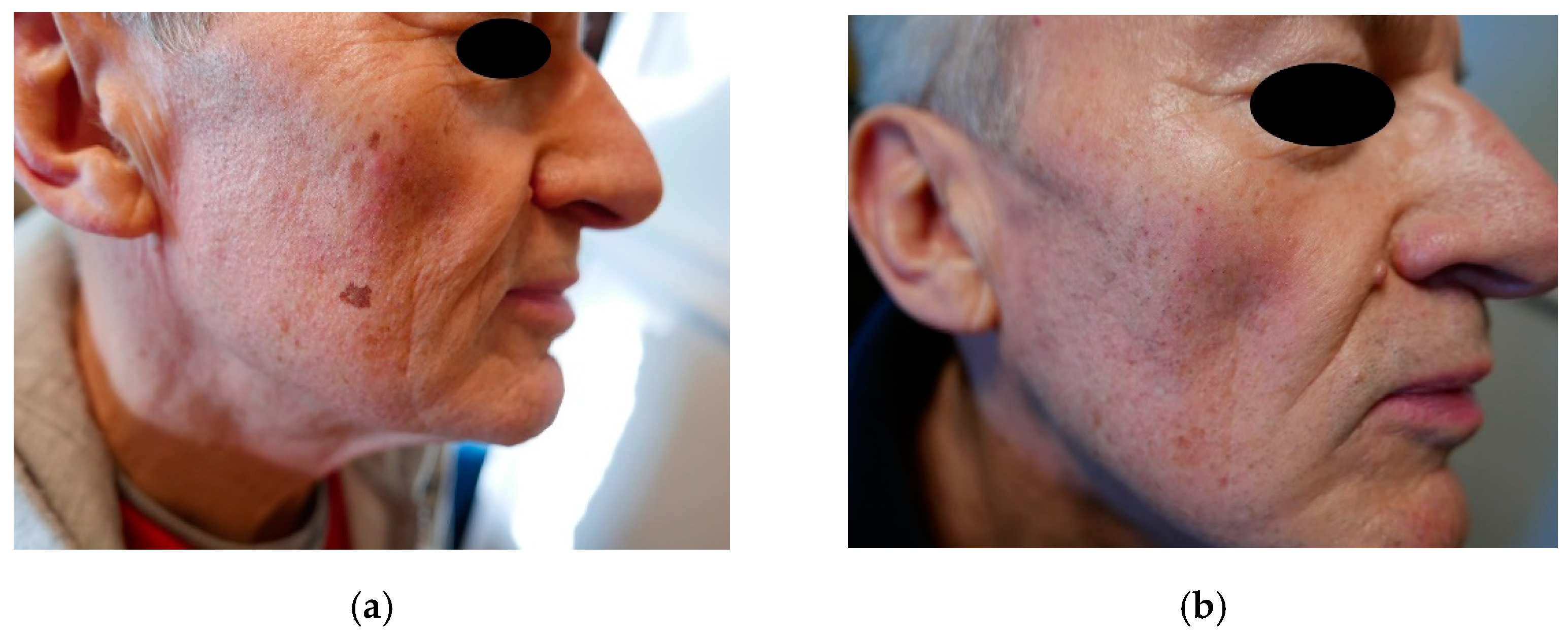
3. Results
4. Discussion
5. Conclusions
- The 450 nm blue laser has proven to be another very effective device in the treatment of lentigines. The irradiation parameters were 47 W pulses with a 15 ms duration and 2 mm spot size. Based on results for other lasers (like the KTP laser at 532 nm) we expect that further reduction in the pulse duration (with an increase in peak power) may reduce the risk of scarring.
- In areas where the skin is more delicate, i.e., the décolleté and forearms, the treatment should be performed using less power and shorter exposure time because of the possibility of slight scarring.
- At a 450 nm wavelength, we can expect strong absorption by hemoglobin. However, this absorption peaks around 420 nm and drops for longer wavelengths. It would likely be better to use longer blue wavelengths (like 460–470 nm) to target melanin, and shorter blue wavelengths (like 420 nm) to target hemoglobin. A strong absorption implies shallow penetration in the tissue, so the epidermis (melanocytes) may receive a higher dose of light than dermis (blood vessels). We obtained positive results on the face (thin epidermis) and on the dorsum of the hands (thick epidermis) and scarring on the chest (where the thickness of the epidermis is intermediate), so we have not observed any correlation of results with the thickness of the epidermis. More prospective clinical studies are necessary to confirm the results we obtained with this small pilot study.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ortonne, J.-P. Pigmentary changes of the ageing skin. Br. J. Dermatol. 1990, 122, 21–28. [Google Scholar] [CrossRef]
- Bastiaens, M.; Hoefnagel, J.; Westendorp, R.; Vermeer, B.-J.; Bavinck, J.N.B. Solar Lentigines are Strongly Related to Sun Exposure in Contrast to Ephelides. Pigment. Cell Res. 2004, 17, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Schoenewolf, N.L.; Hafner, J.; Dummer, R.; Allemann, I.B. Laser treatment of solar lentigines on dorsum of hands: QS Ruby laser versus ablative CO2 fractional laser–a randomized controlled trial. Eur. J. Dermatol. EJD 2015, 25, 122–126. [Google Scholar] [CrossRef]
- Ortonne, J.-P.; Pandya, A.G.; Lui, H.; Hexsel, D. Treatment of solar lentigines. J. Am. Acad. Dermatol. 2006, 54, S262–S271. [Google Scholar] [CrossRef] [PubMed]
- Stem, R.S.; Dover, J.S.; Levin, J.A.; Arndt, K.A. Laser therapy versus cryotherapy of lentigines: A comparative trial. J. Am. Acad. Dermatol. 1994, 30, 985–987. [Google Scholar] [CrossRef]
- Todd, M.M.; Rallis, T.M.; Gerwels, J.W.; Hata, T.R. A Comparison of 3 Lasers and Liquid Nitrogen in the Treatment of Solar Lentigines. Arch. Dermatol. 2000, 136, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Sezer, E.; Erbil, H.; Kurumlu, Z.; Taştan, H.B.; Etikan, I. A comparative study of focal medium-depth chemical peel versus cryosurgery for the treatment of solar lentigo. Eur. J. Dermatol. 2007, 17. [Google Scholar] [CrossRef]
- Fleischer, A.B.; Schwartzel, E.H.; Colby, S.I.; Altman, D.J. The combination of 2% 4-hydroxyanisole (Mequinol) and 0.01% tretinoin is effective in improving the appearance of solar lentigines and related hyperpigmented lesions in two double-blind multicenter clinical studies. J. Am. Acad. Dermatol. 2000, 42, 459–467. [Google Scholar] [CrossRef]
- Kang, S.; Goldfarb, M.T.; Weiss, J.S.; Metz, R.D.; Hamilton, T.A.; Voorhees, J.J.; Griffiths, C. Assessment of adapalene gel for the treatment of actinic keratoses and lentigines: A randomized trial. J. Am. Acad. Dermatol. 2003, 49, 83–90. [Google Scholar] [CrossRef]
- Jarratt, M. Mequinol 2%/tretinoin 0.01% solution: An effective and safe alternative to hydroquinone 3% in the treatment of solar lentigines. Cutis 2004, 74, 319–322. [Google Scholar] [CrossRef]
- Draelos, Z.D. The combination of 2% 4-hydroxyanisole (mequinol) and 0.01% tretinoin effectively improves the appearance of solar lentigines in ethnic groups. J. Cosmet. Dermatol. 2006, 5, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Woźniak, Z.; Trzeciakowski, W.; Chlebicka, I.; Ziółkowski, P. Photodynamic diagnosis and photodynamic therapy in basal cell carcinoma using a novel laser light source. Photodiagnosis Photodyn. Ther. 2020, 31, 101883. [Google Scholar] [CrossRef] [PubMed]
- Ericson, M.B.; Wennberg, A.M.; Larkö, O. Review of photodynamic therapy in actinic keratosis and basal cell carcinoma. Ther. Clin. Risk Manag. 2008, 4, 1–9. [Google Scholar] [PubMed]
- DI Meo, N.; Nan, K.; Noal, C.; Ottaviani, G.; Biasotto, M.; Trevisan, G. Blue diode laser: A new strategy for the management of lichen sclerosus et atrophicus. G Ital. Dermatol. Venereol. 2018, 153, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Braun, M. Combination of a new radiofrequency device and blue light for the treatment of acne vulgaris. J. Drugs Dermatol. JDD 2007, 6, 838–840. [Google Scholar]
- Gold, M.H.; Bradshaw, V.L.; Boring, M.M.; Bridges, T.M.; A Biron, J.; Lewis, T.L. Treatment of sebaceous gland hyperplasia by photodynamic therapy with 5-aminolevulinic acid and a blue light source or intense pulsed light source. J. Drugs Dermatol. JDD 2004, 3, S6–S9. [Google Scholar] [PubMed]
- Lodi, G.; Sannino, M.; Cannarozzo, G.; Giudice, A.; Del Duca, E.; Tamburi, F.; Bennardo, L.; Nisticò, S.P. Blue light-emitting diodes in hair regrowth: The first prospective study. Lasers Med Sci. 2021, 36, 1719–1723. [Google Scholar] [CrossRef]
- Szymańczyk, J.; Trzeciakowski, W.; Ivonyak, Y.; Tuchowski, P.; Szymańczyk, J. Blue Laser (450 nm) in the Treatment of Port Wine Stains and Telangiectasia. J. Clin. Med. 2021, 10, 1258. [Google Scholar] [CrossRef]
- Szymańczyk, J.; Mańkowska, A.; Szymański, K.; Półchłopek, T.; Trzeciakowski, W.; Szymańczyk, J. High-power blue laser as a versatile tool in dermatology. J. Cosmet. Dermatol. 2021. [Google Scholar] [CrossRef]
- Ivonyak, Y.; Piechal, B.; Mrozowicz, M.; Bercha, A.; Trzeciakowski, W. Note: Coupling of multiple laser diodes into a multi-mode fiber. Rev. Sci. Instruments 2014, 85, 036106. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The Validity and Practicality of Sun-Reactive Skin Types I Through VI. Arch. Dermatol. 1988, 124, 869. [Google Scholar] [CrossRef]
- Wang, C.-C.; Sue, Y.-M.; Yang, C.-H.; Chen, C.-K. A comparison of Q-switched alexandrite laser and intense pulsed light for the treatment of freckles and lentigines in Asian persons: A randomized, physician-blinded, split-face comparative trial. J. Am. Acad. Dermatol. 2006, 54, 804–810. [Google Scholar] [CrossRef]
- Yoshimura, K.; Harii, K.; Aoyama, T.; Iga, T. Experience with a Strong Bleaching Treatment for Skin Hyperpigmentation in Orientals. Plast. Reconstr. Surg. 2000, 105, 1097–1108. [Google Scholar] [CrossRef]
- Vachiramon, V.; Iamsumang, W.; Triyangkulsri, K. Q-switched double frequency Nd:YAG 532-nm nanosecond laser vs. double frequency Nd: YAG 532-nm picosecond laser for the treatment of solar lentigines in Asians. Lasers Med Sci. 2018, 33, 1941–1947. [Google Scholar] [CrossRef] [PubMed]
- Grekin, R.C.; Shelton, R.M.; Geisse, J.K.; Frieden, I. 510-nm Pigmented Lesion Dye Laser. J. Dermatol. Surg. Oncol. 1993, 19, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Vachiramon, V.; Panmanee, W.; Techapichetvanich, T.; Chanprapaph, K. Comparison of Q-switched Nd: YAG laser and fractional carbon dioxide laser for the treatment of solar lentigines in Asians. Lasers Surg. Med. 2016, 48, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-T.; Yang, K.-C. Comparison of the Frequency-Doubled Q-Switched Nd:YAG Laser and 35% Trichloroacetic Acid for the Treatment of Face Lentigines. Dermatol. Surg. 1999, 25, 202–204. [Google Scholar] [CrossRef]
- Negishi, K.; Akita, H.; Tanaka, S.; Yokoyama, Y.; Wakamatsu, S.; Matsunaga, K. Comparative study of treatment efficacy and the incidence of post-inflammatory hyperpigmentation with different degrees of irradiation using two different quality-switched lasers for removing solar lentigines on Asian skin. J. Eur. Acad. Dermatol. Venereol. 2011, 27, 307–312. [Google Scholar] [CrossRef]
- Nisticò, S.P.; Tolone, M.; Zingoni, T.; Tamburi, F.; Scali, E.; Bennardo, L.; Cannarozzo, G. A New 675 nm Laser Device in the Treatment of Melasma: Results of a Prospective Observational Study. Photobiomodul. Photomed. Laser Surg. 2020, 38, 560–564. [Google Scholar] [CrossRef]
- Silvestri, M.; Bennardo, L.; Zappia, E.; Tamburi, F.; Cameli, N.; Cannarozzo, G.; Nisticò, S.P. Q-Switched 1064/532 nm Laser with Picosecond Pulse to Treat Benign Hyperpigmentations: A Single-Center Retrospective Study. Appl. Sci. 2021, 11, 7478. [Google Scholar] [CrossRef]
- Tanaka, Y.; Tsunemi, Y.; Kawashima, M. Objective assessment of intensive targeted treatment for solar lentigines using intense pulsed light with wavelengths between 500 and 635 nm. Lasers Surg. Med. 2015, 48, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Patient’s Number | Sex | Age | Type of Skin | Location of Lesion | Number of Procedures | Size (mm) | Improve-Ment (%) | Evaluation of Effects |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 74 | II | Forearms | 2 | 10–20 | 30 | Unsatisfactory |
| 2 | F | 61 | II | Forearms | 1 | 13 | 30 | Unsatisfactory |
| 3 | F | 72 | III | Face (forehead) | 6 | 14–16 | 100 | Complete disappearance |
| 4 | F | 56 | III | Face and neck | 1 | 7–11 | 0 | Resignation after one procedure |
| 5 | F | 55 | IV | Face (forehead and cheek) | 3 | 20 | 100 | Complete disappearance |
| 6 | F | 52 | III | Forearms and chest | 2 | 4–5 | 100 (forearms) | Scarring on the chest |
| 7 | F | 62 | III | Face (nose) | 1 | 15 | 100 | Complete disappearance |
| 8 | F | 74 | II | Face | 1 | 20 | 100 | Complete disappearance |
| 9 | M | 70 | II | Face (cheek) | 3 | 10 | 100 | Complete disappearance |
| 10 | M | 68 | II | Face (forehead) | 2 | 20 | 100 | Complete disappearance |
| 11 | M | 61 | III | Dorsal of hands | 1 | 5 | 100 | Complete disappearance |
| 12 | F | 70 | II | Chest | 1 | 8 | 50 | Partial disappearance |
| 13 | F | 60 | II | Face (nose) | 1 | 12 | 50 | Partial disappearance |
| 14 | M | 56 | V | Dorsal of hands | 3 | 4–5 | 100 | Complete disappearance |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szymańczyk, J.; Trzeciakowski, W.; Ivonyak, Y.; Tuchowski, P.; Bercha, A.; Szymańczyk, J. Blue Laser (450 nm) Treatment of Solar Lentigines. J. Clin. Med. 2021, 10, 4919. https://doi.org/10.3390/jcm10214919
Szymańczyk J, Trzeciakowski W, Ivonyak Y, Tuchowski P, Bercha A, Szymańczyk J. Blue Laser (450 nm) Treatment of Solar Lentigines. Journal of Clinical Medicine. 2021; 10(21):4919. https://doi.org/10.3390/jcm10214919
Chicago/Turabian StyleSzymańczyk, Jacek, Witold Trzeciakowski, Yurij Ivonyak, Piotr Tuchowski, Artem Bercha, and Janusz Szymańczyk. 2021. "Blue Laser (450 nm) Treatment of Solar Lentigines" Journal of Clinical Medicine 10, no. 21: 4919. https://doi.org/10.3390/jcm10214919
APA StyleSzymańczyk, J., Trzeciakowski, W., Ivonyak, Y., Tuchowski, P., Bercha, A., & Szymańczyk, J. (2021). Blue Laser (450 nm) Treatment of Solar Lentigines. Journal of Clinical Medicine, 10(21), 4919. https://doi.org/10.3390/jcm10214919