
A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
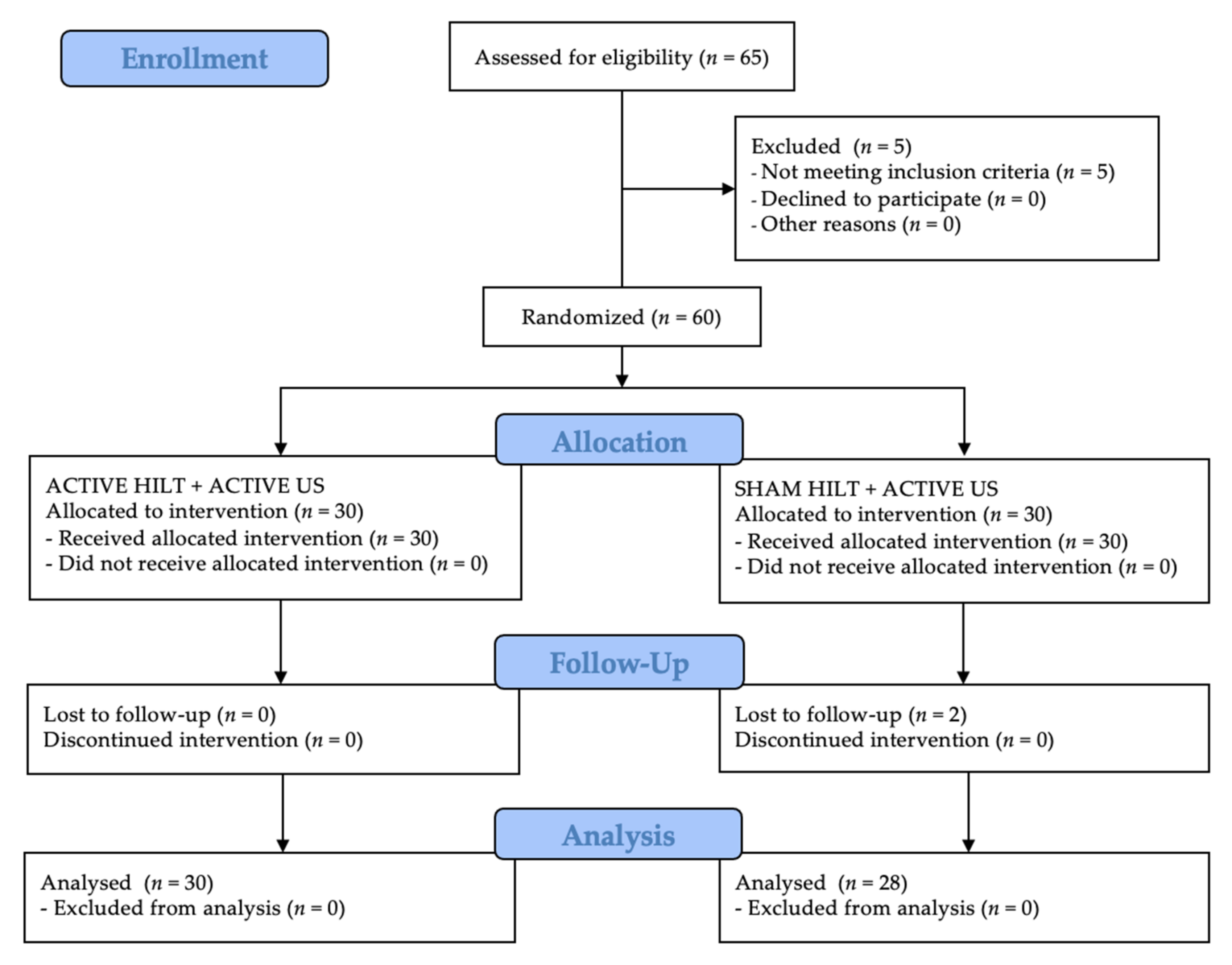
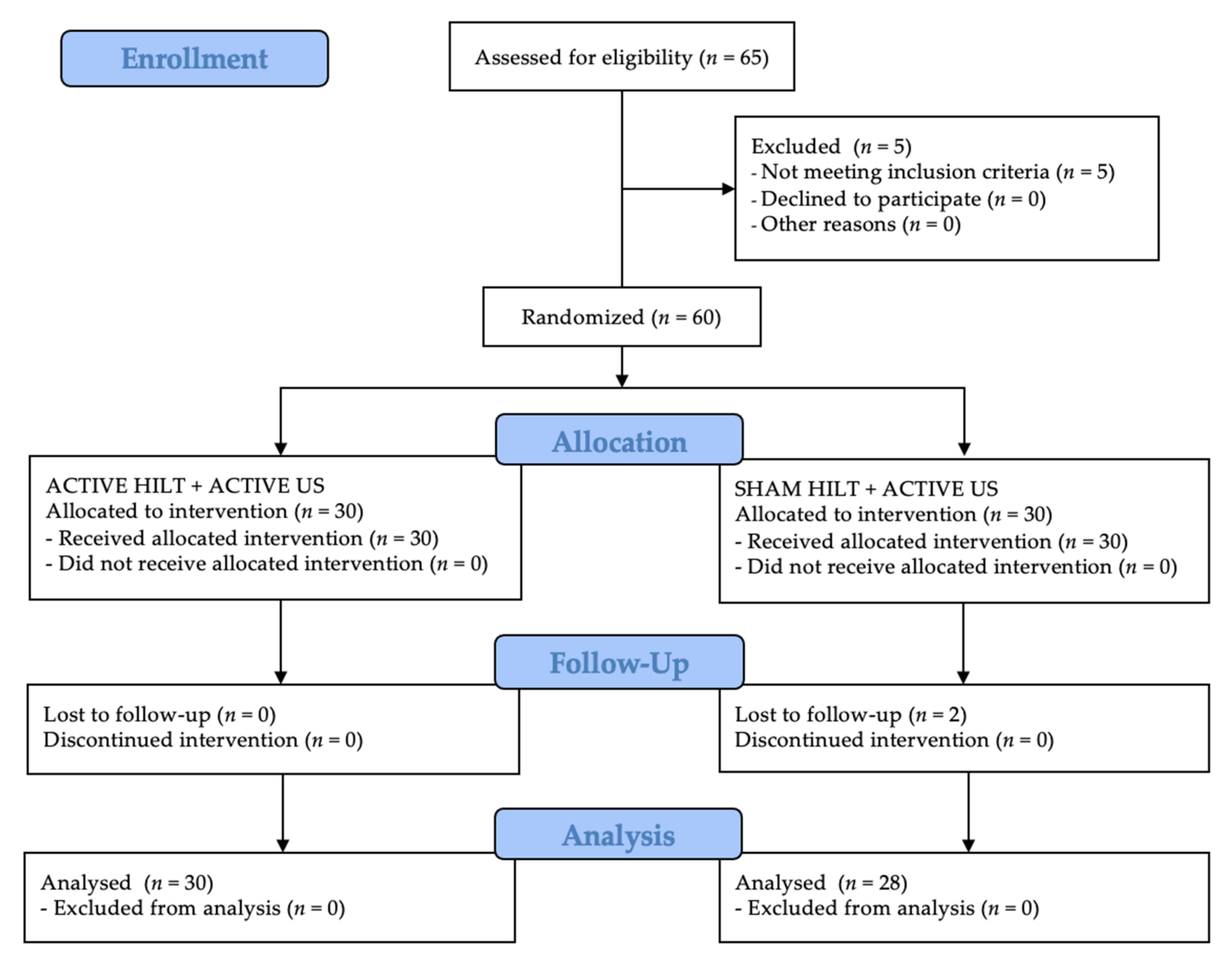
2.2. Randomization
2.3. Participants
- (1)
- Chronic nature of the condition in question (at least six months of symptom manifestations);
- (2)
- Persistent pain of plantar fasciitis physical examination:
- a.
- Pain reproduced by palpating the plantar medial calcaneal tubercle at the site of the plantar fascial insertion on the heel bone,
- b.
- Pain reproduced with passive dorsiflexion of the foot and toes, and
- c.
- Windlass test—passive dorsiflexion of the first metatarsophalangeal joint—test to provoke symptoms at the plantar fascia by creating maximal stretch), positive test if pain is reproduced); and
- (3)
- A current X-ray image of the foot (heel spur).
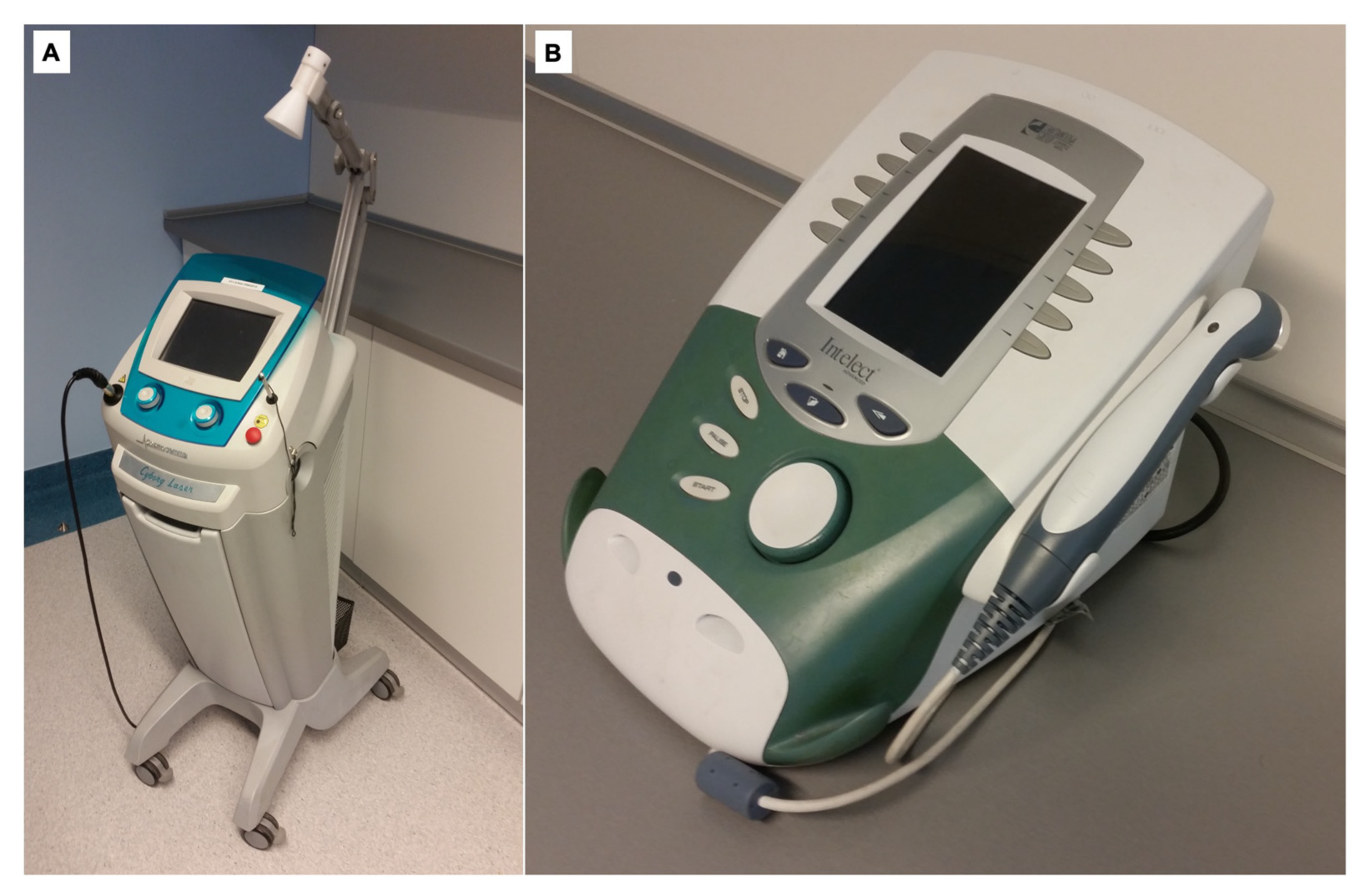
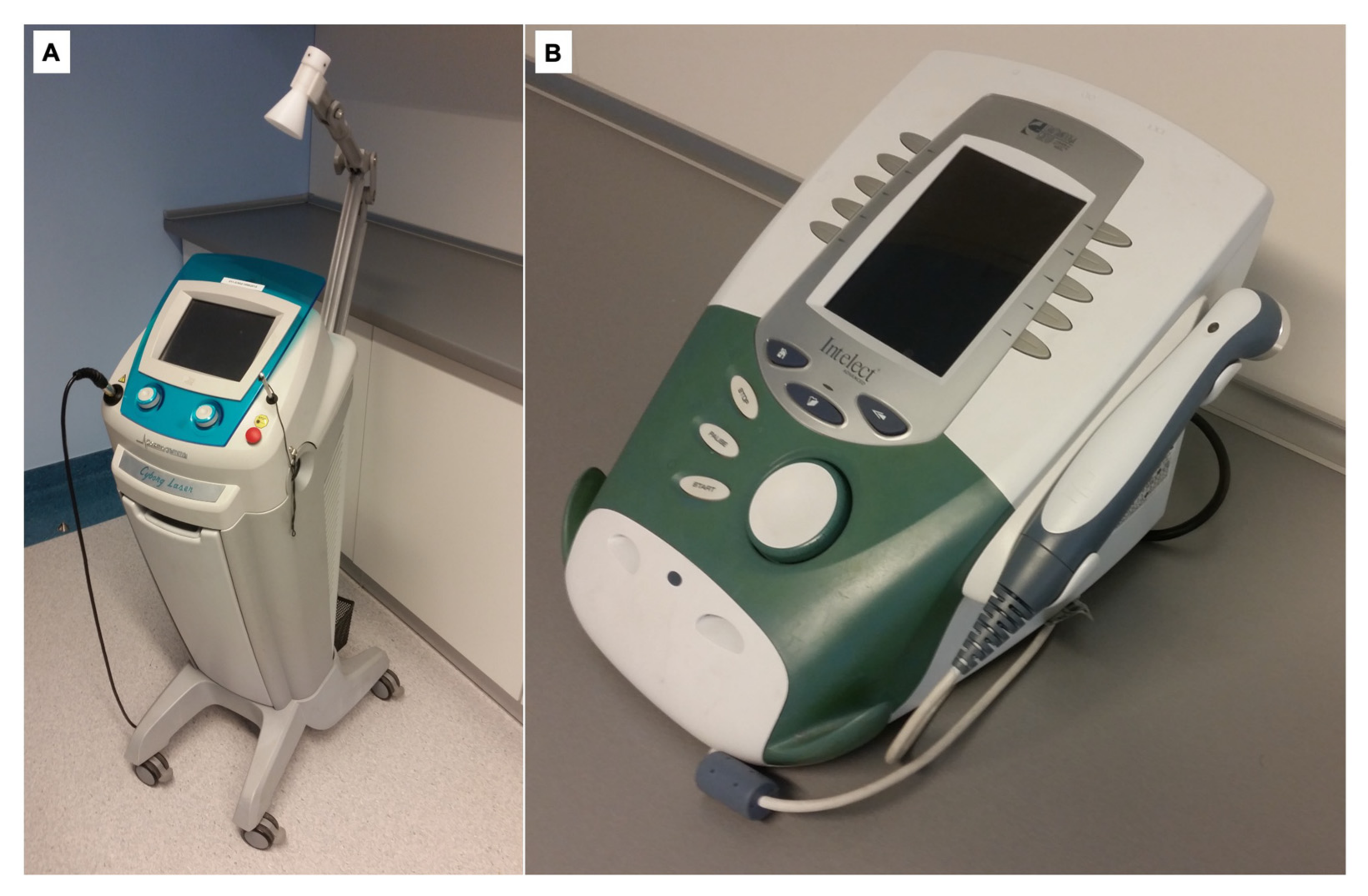
2.4. Treatment
2.5. Measurements
2.6. Sample Size
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alayat, M.S.M.; Basalamah, M.A.; Elbarrany, W.G.E.A.-E.; El-Sawy, N.A.M.; Abdel-Kafy, E.M.; El-Fiky, A.A.-R. Dose-Dependent Effect of the Pulsed Nd:YAG Laser in the Treatment of Crushed Sciatic Nerve in Wister Rats: An Experimental Model. Lasers Med. Sci. 2020, 35, 1989–1998. [Google Scholar] [CrossRef]
- Daigo, Y.; Daigo, E.; Hasegawa, A.; Fukuoka, H.; Ishikawa, M.; Takahashi, K. Utility of High-Intensity Laser Therapy Combined with Photobiomodulation Therapy for Socket Preservation After Tooth Extraction. Photobiomodul. Photomed. Laser Surg. 2020, 38, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Ebid, A.A.; Alhammad, R.M.; Alhendi, R.T.; Alqarhi, B.A.; Baweyan, E.M.; Alfadli, L.H.; Alzahrani, M.A.; Alotaibi, M.F.; Alaidrous, N.A.; Alzahrani, R.A.; et al. Immediate Effect of Pulsed High-Intensity Neodymium-Doped Yttrium Aluminum Garnet (Nd: YAG) Laser on Staphylococcus Aureus and Pseudomonas Aeruginosa Growth: An Experimental Study. J. Phys. Ther. Sci. 2019, 31, 925–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keshri, G.K.; Gupta, A.; Yadav, A.; Sharma, S.K.; Singh, S.B. Photobiomodulation with Pulsed and Continuous Wave Near-Infrared Laser (810 Nm, Al-Ga-As) Augments Dermal Wound Healing in Immunosuppressed Rats. PLoS ONE 2016, 11, e0166705. [Google Scholar] [CrossRef] [Green Version]
- Tomazoni, S.S.; Frigo, L.; Dos Reis Ferreira, T.C.; Casalechi, H.L.; Teixeira, S.; de Almeida, P.; Muscara, M.N.; Marcos, R.L.; Serra, A.J.; de Carvalho, P.d.T.C.; et al. Effects of Photobiomodulation Therapy and Topical Non-Steroidal Anti-Inflammatory Drug on Skeletal Muscle Injury Induced by Contusion in Rats-Part 1: Morphological and Functional Aspects. Lasers Med. Sci. 2017, 32, 2111–2120. [Google Scholar] [CrossRef] [PubMed]
- Tomazoni, S.S.; Frigo, L.; Dos Reis Ferreira, T.C.; Casalechi, H.L.; Teixeira, S.; de Almeida, P.; Muscara, M.N.; Marcos, R.L.; Serra, A.J.; de Carvalho, P.d.T.C.; et al. Effects of Photobiomodulation Therapy and Topical Non-Steroidal Anti-Inflammatory Drug on Skeletal Muscle Injury Induced by Contusion in Rats—Part 2: Biochemical Aspects. Lasers Med. Sci. 2017, 32, 1879–1887. [Google Scholar] [CrossRef]
- Mussttaf, R.A.; Jenkins, D.F.L.; Jha, A.N. Assessing the Impact of Low Level Laser Therapy (LLLT) on Biological Systems: A Review. Int. J. Radiat. Biol. 2019, 95, 120–143. [Google Scholar] [CrossRef]
- Hamblin, M.R. Mechanisms and Applications of the Anti-Inflammatory Effects of Photobiomodulation. AIMS Biophys. 2017, 4, 337–361. [Google Scholar] [CrossRef]
- Abdelbasset, W.K.; Nambi, G.; Alsubaie, S.F.; Abodonya, A.M.; Saleh, A.K.; Ataalla, N.N.; Ibrahim, A.A.; Tantawy, S.A.; Kamel, D.M.; Verma, A.; et al. A Randomized Comparative Study between High-Intensity and Low-Level Laser Therapy in the Treatment of Chronic Nonspecific Low Back Pain. Evid.-Based Complement. Altern. Med. 2020, 2020, 1350281. [Google Scholar] [CrossRef] [PubMed]
- Alayat, M.S.M.; Atya, A.M.; Ali, M.M.E.; Shosha, T.M. Long-Term Effect of High-Intensity Laser Therapy in the Treatment of Patients with Chronic Low Back Pain: A Randomized Blinded Placebo-Controlled Trial. Lasers Med. Sci. 2014, 29, 1065–1073. [Google Scholar] [CrossRef]
- Kaydok, E.; Ordahan, B.; Solum, S.; Karahan, A.Y. Short-Term Efficacy Comparison of High-Intensity and Low-Intensity Laser Therapy in the Treatment of Lateral Epicondylitis: A Randomized Double-Blind Clinical Study. Arch. Rheumatol. 2020, 35, 60–67. [Google Scholar] [CrossRef]
- Nazari, A.; Moezy, A.; Nejati, P.; Mazaherinezhad, A. Efficacy of High-Intensity Laser Therapy in Comparison with Conventional Physiotherapy and Exercise Therapy on Pain and Function of Patients with Knee Osteoarthritis: A Randomized Controlled Trial with 12-Week Follow Up. Lasers Med. Sci. 2019, 34, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, K.; Laakso, E.-L.; Salari, A.; Hasannejad, A.; Fekrazad, R.; Aris, A. The Beneficial Effects of High-Intensity Laser Therapy and Co-Interventions on Musculoskeletal Pain Management: A Systematic Review. J. Lasers Med. Sci. 2020, 11, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Taradaj, J.; Rajfur, K.; Rajfur, J.; Ptaszkowski, K.; Ptaszkowska, L.; Sopel, M.; Rosińczuk, J.; Dymarek, R. Effect of Laser Treatment on Postural Control Parameters in Patients with Chronic Nonspecific Low Back Pain: A Randomized Placebo-Controlled Trial. Braz. J. Med. Biol. Res. 2019, 52, e8474. [Google Scholar] [CrossRef] [PubMed]
- Taradaj, J.; Rajfur, K.; Shay, B.; Rajfur, J.; Ptaszkowski, K.; Walewicz, K.; Dymarek, R.; Sopel, M.; Rosińczuk, J. Photobiomodulation Using High- or Low-Level Laser Irradiations in Patients with Lumbar Disc Degenerative Changes: Disappointing Outcomes and Remarks. Clin. Interv. Aging 2018, 13, 1445–1455. [Google Scholar] [CrossRef] [Green Version]
- Kosmahl, E.M.; Kosmahl, H.E. Painful Plantar Heel, Plantar Fasciitis, and Calcaneal Spur: Etiology and Treatment. J. Orthop. Sports Phys. Ther. 1987, 9, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, A.J.; DiPreta, J.A.; Misener, D. Plantar Heel Pain. Med. Clin. N. Am. 2014, 98, 339–352. [Google Scholar] [CrossRef]
- Cutts, S.; Obi, N.; Pasapula, C.; Chan, W. Plantar Fasciitis. Ann. R. Coll. Surg. Engl. 2012, 94, 539–542. [Google Scholar] [CrossRef]
- Johal, K.S.; Milner, S.A. Plantar Fasciitis and the Calcaneal Spur: Fact or Fiction? Foot Ankle Surg. 2012, 18, 39–41. [Google Scholar] [CrossRef]
- Menz, H.B.; Thomas, M.J.; Marshall, M.; Rathod-Mistry, T.; Hall, A.; Chesterton, L.S.; Peat, G.M.; Roddy, E. Coexistence of Plantar Calcaneal Spurs and Plantar Fascial Thickening in Individuals with Plantar Heel Pain. Rheumatology 2019, 58, 237–245. [Google Scholar] [CrossRef]
- Landorf, K.B.; Menz, H.B. Plantar Heel Pain and Fasciitis. BMJ Clin. Evid. 2008, 2008, 1111. [Google Scholar]
- Kociuga, N.; Kociuga, J.; Woldańska-Okońska, M.; Kubsik, A. Physiotherapeutic proceeding in symptomatic calcaneal spur treatment. Wiad. Lek. 2016, 69, 758–764. [Google Scholar] [PubMed]
- Li, X.; Zhang, L.; Gu, S.; Sun, J.; Qin, Z.; Yue, J.; Zhong, Y.; Ding, N.; Gao, R. Comparative Effectiveness of Extracorporeal Shock Wave, Ultrasound, Low-Level Laser Therapy, Noninvasive Interactive Neurostimulation, and Pulsed Radiofrequency Treatment for Treating Plantar Fasciitis: A Systematic Review and Network Meta-Analysis. Medicine 2018, 97, e12819. [Google Scholar] [CrossRef]
- Scott, J.; Huskisson, E.C. Graphic Representation of Pain. Pain 1976, 2, 175–184. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A Review of Three Commonly Used Pain Rating Scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: Oxford, UK, 2014; ISBN 978-0-19-176545-2. [Google Scholar]
- Laitinen, J. Acupuncture and Transcutaneous Electric Stimulation in the Treatment of Chronic Sacrolumbalgia and Ischialgia. Am. J. Chin. Med. 1976, 4, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Yesil, H.; Dundar, U.; Toktas, H.; Eyvaz, N.; Yeşil, M. The Effect of High Intensity Laser Therapy in the Management of Painful Calcaneal Spur: A Double Blind, Placebo-Controlled Study. Lasers Med. Sci. 2020, 35, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Ordahan, B.; Karahan, A.Y.; Kaydok, E. The Effect of High-Intensity versus Low-Level Laser Therapy in the Management of Plantar Fasciitis: A Randomized Clinical Trial. Lasers Med. Sci. 2018, 33, 1363–1369. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Study Group (n = 30) | Control Group (n = 30) | p-Value | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Me | Min | Max | Q1 | Q3 | SD | Me | Min | Max | Q1 | Q3 | SD | ||||
| Age (year) | 59.9 | 59.5 | 33.0 | 78.0 | 52.0 | 67.0 | 10.1 | 60.4 | 61.0 | 44.0 | 84.0 | 48.0 | 65.0 | 11.9 | 0.87 * |
| Weight (kg) | 79.5 | 79.5 | 54.0 | 108 | 67.0 | 90.0 | 15.2 | 79.9 | 80.0 | 53.0 | 105 | 72.0 | 90.0 | 13.4 | 0.92 * |
| Height (cm) | 171.1 | 170 | 159 | 187 | 164 | 178 | 7.7 | 167.8 | 167 | 152 | 188 | 160 | 175 | 10.1 | 0.20 * |
| BMI (kg/m2) | 27.2 | 25.9 | 18.7 | 37.6 | 23.3 | 29.7 | 4.9 | 28.5 | 27.7 | 20.9 | 39.0 | 24.5 | 30.9 | 4.8 | 0.43 ** |
| Sex | F—n = 19; 63.3% M—n = 11; 36.7% | F—n = 17; 56.7% M—n = 13; 43.3% | 0.70 *** | ||||||||||||
| Studied limb | L—n = 14; 46.7% R—n = 16; 53.3% | L—n = 16; 53.3% R—n = 14; 46.7% | 0.68 *** | ||||||||||||
| Variable | Measurement | Study Group (n = 30) | Control Group (n = 30) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Me | Min | Max | Q1 | Q3 | SD | Me | Min | Max | Q1 | Q3 | SD | ||||
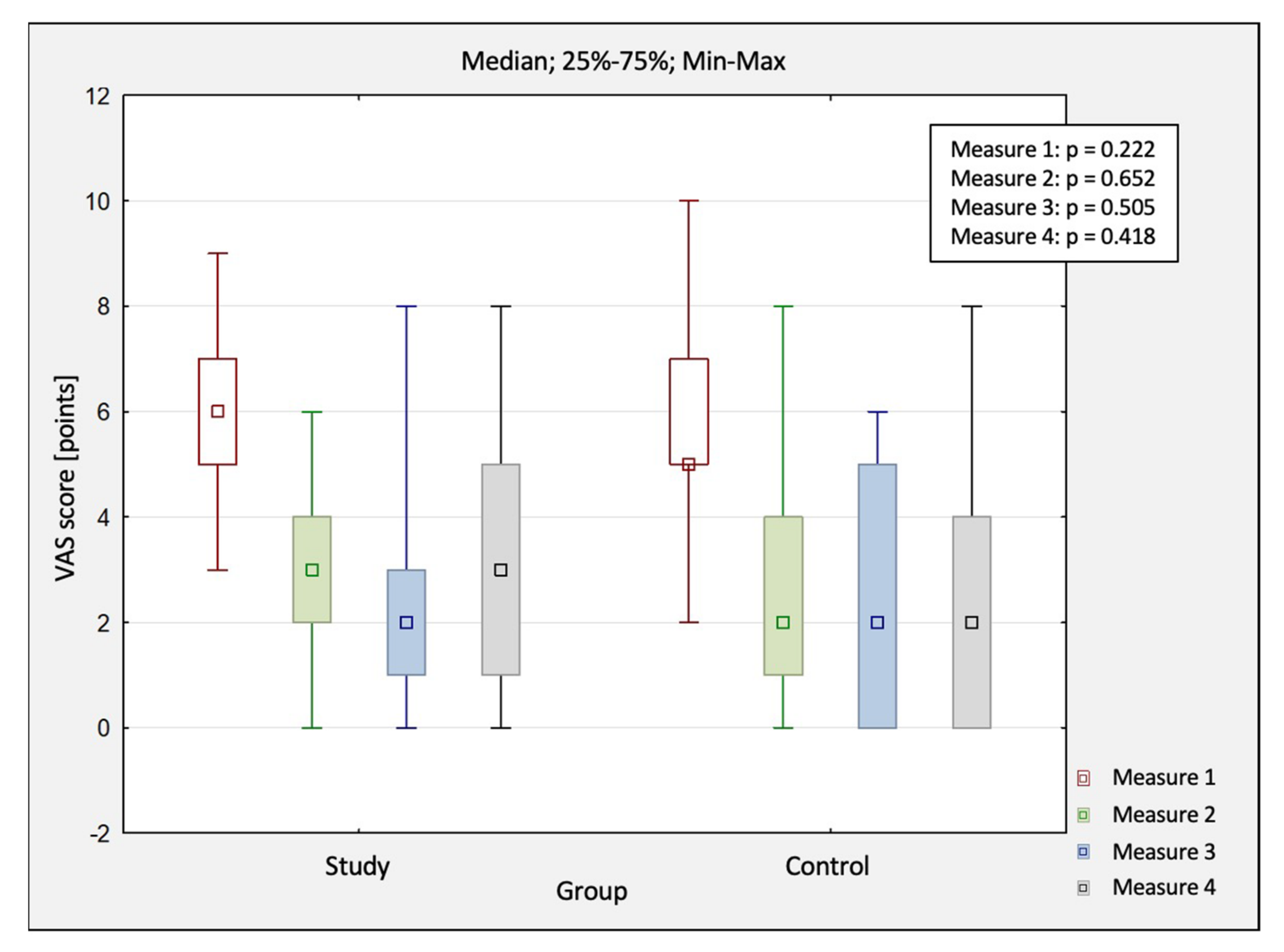
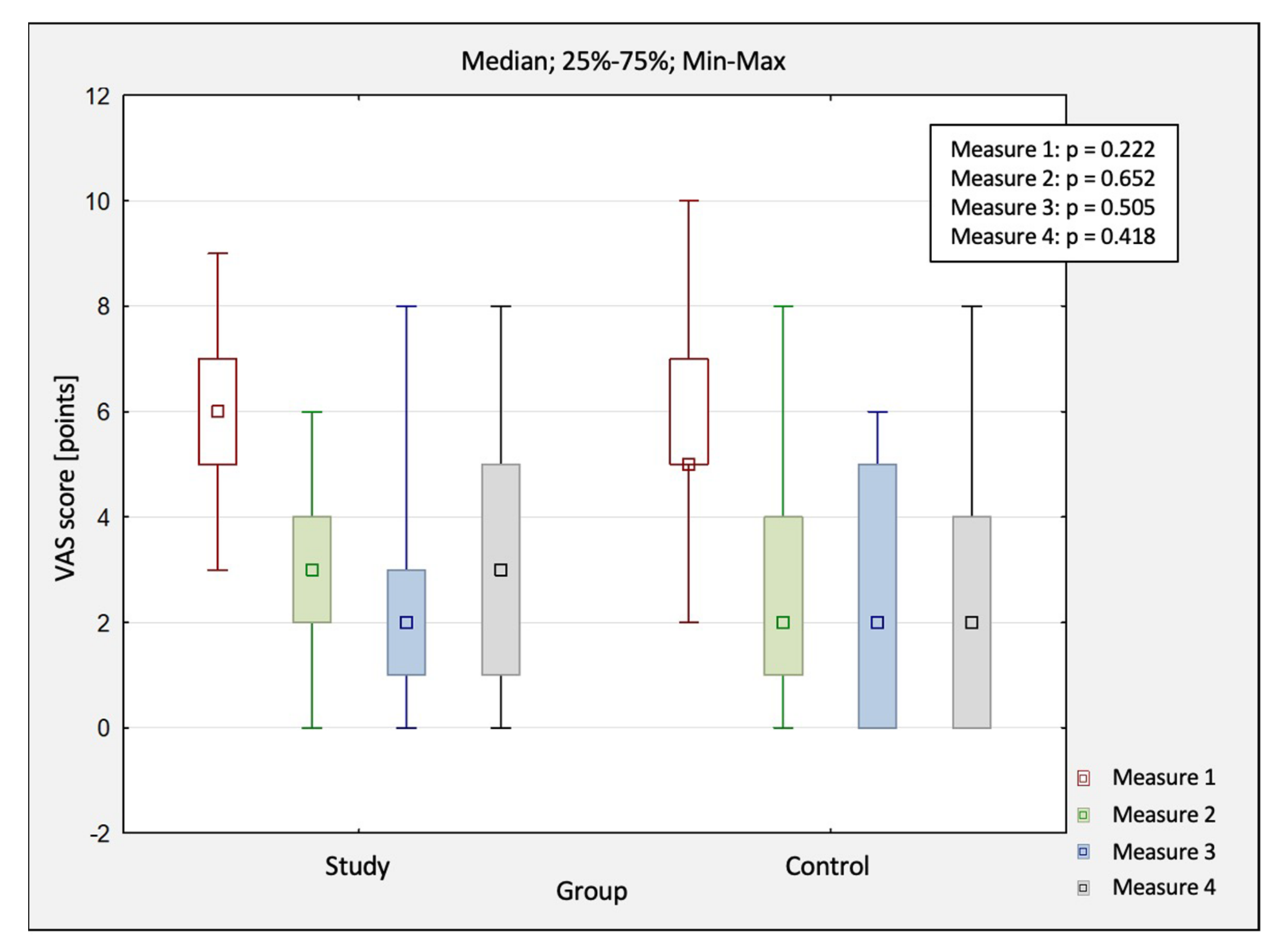
| VAS (pts) | M1 | 6.3 | 6.0 | 3.0 | 9.0 | 5.0 | 7.0 | 1.4 | 5.7 | 5.0 | 2.0 | 10.0 | 5.0 | 7.0 | 2.0 |
| M2 | 2.8 | 3.0 | 0.0 | 6.0 | 2.0 | 4.0 | 1.5 | 2.7 | 2.0 | 0.0 | 8.0 | 1.0 | 4.0 | 2.0 | |
| M3 | 2.6 | 2.0 | 0.0 | 8.0 | 1.0 | 3.0 | 2.0 | 2.3 | 2.0 | 0.0 | 6.0 | 0.0 | 5.0 | 2.2 | |
| M4 | 3.1 | 3.0 | 0.0 | 8.0 | 1.0 | 5.0 | 2.5 | 2.5 | 2.0 | 0.0 | 8.0 | 0.0 | 4.0 | 2.4 | |
| p-value * | <0.001 | <0.001 | |||||||||||||
| p-value ** | M1 vs. M2: p < 0.001 M1 vs. M3: p < 0.001 M1 vs. M4: p < 0.001 M2 vs. M3: p = 1.00 M2 vs. M4: p = 1.00 M3 vs. M4: p = 1.00 | M1 vs. M2: p < 0.001 M1 vs. M3: p < 0.001 M1 vs. M4: p < 0.001 M2 vs. M3: p = 1.00 M2 vs. M4: p = 1.00 M3 vs. M4: p = 1.00 | |||||||||||||
| Variable | Measurement | Study Group (n = 30) | Control Group (n = 30) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Me | Min | Max | Q1 | Q3 | SD | Me | Min | Max | Q1 | Q3 | SD | ||||
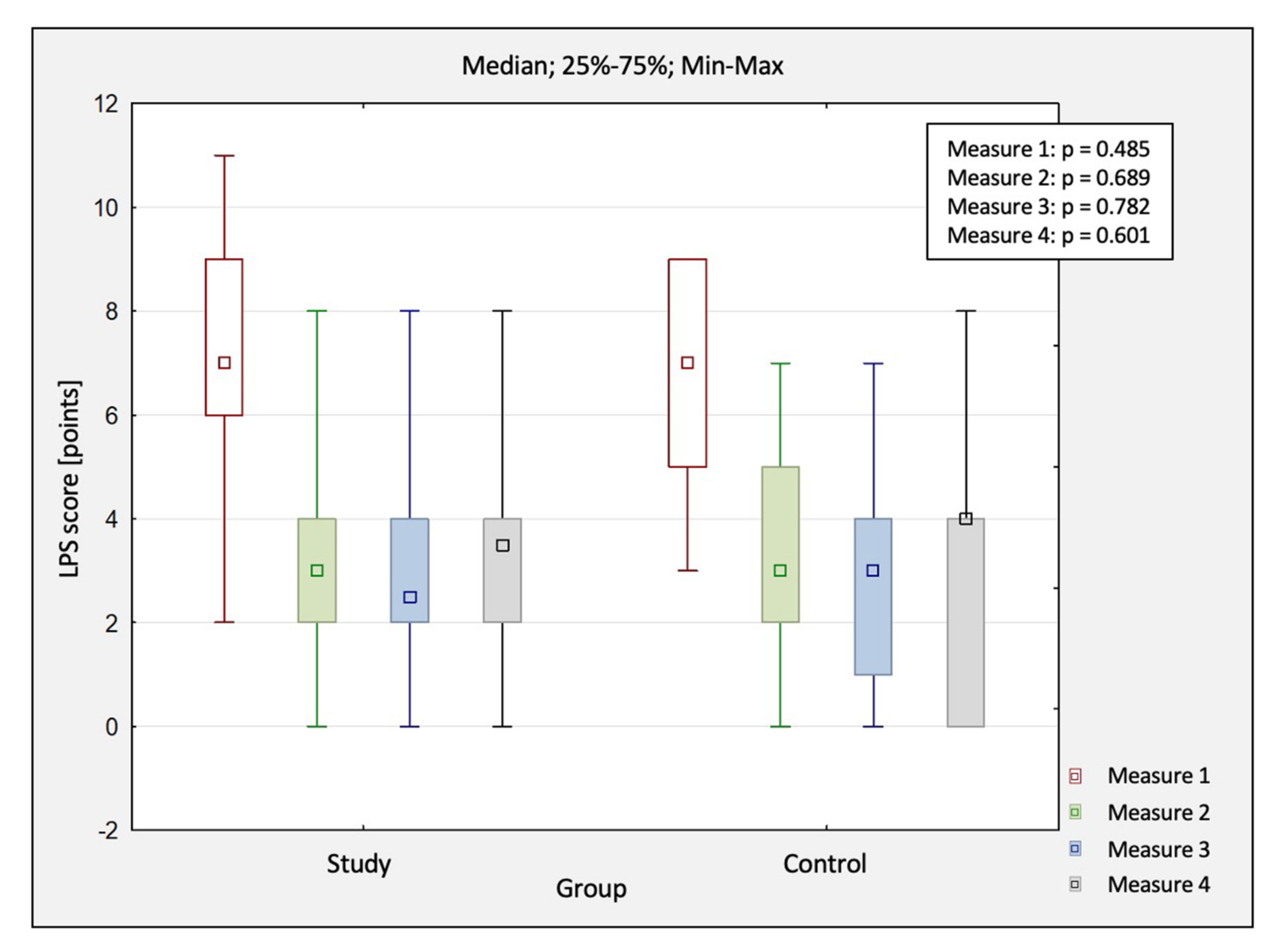
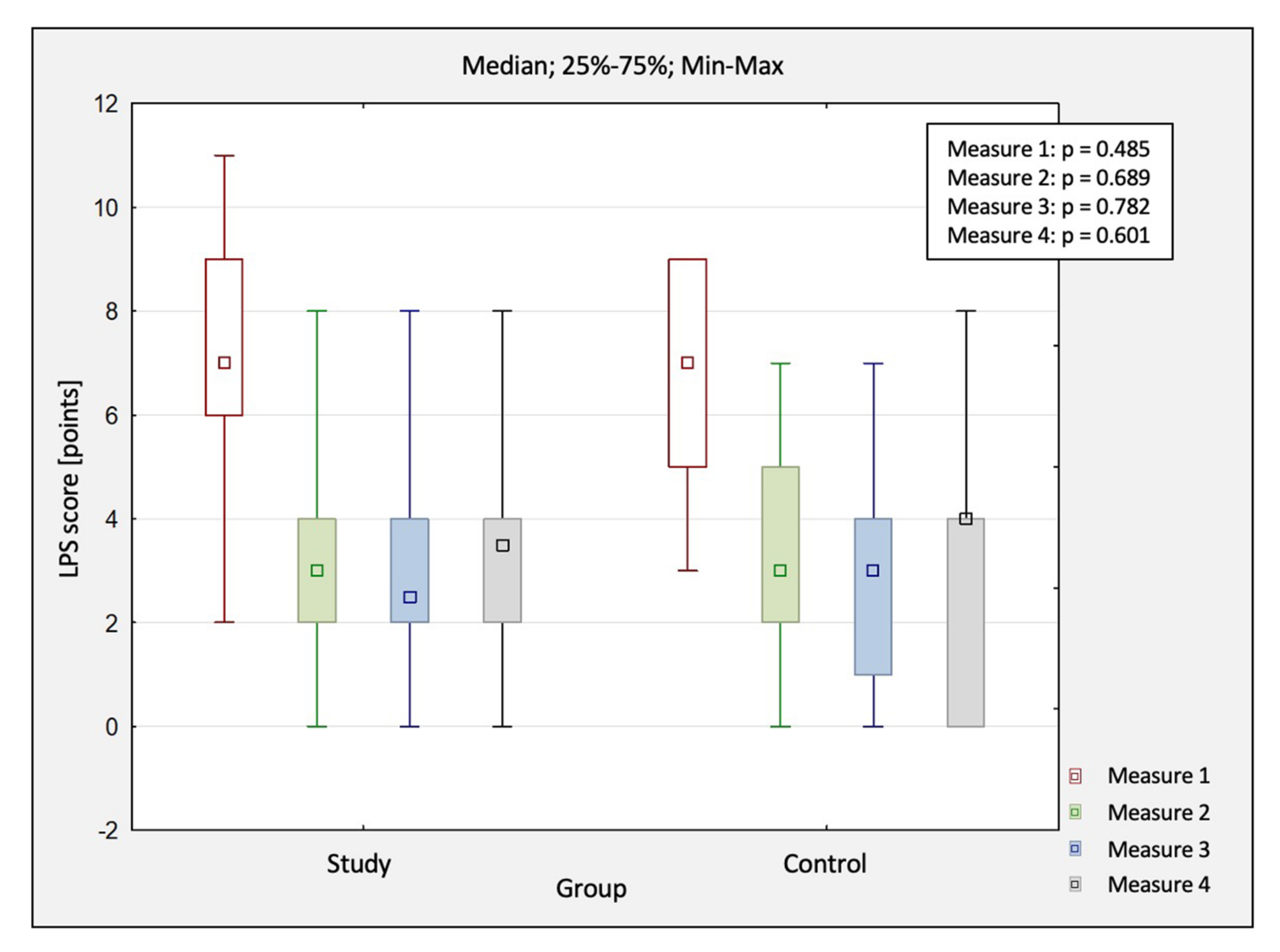
| LPS (pts) | M1 | 7.2 | 7.0 | 2.0 | 11.0 | 6.0 | 9.0 | 2.1 | 6.7 | 7.0 | 3.0 | 9.0 | 5.0 | 9.0 | 2.0 |
| M2 | 3.3 | 3.0 | 0.0 | 8.0 | 2.0 | 4.0 | 1.8 | 3.5 | 3.0 | 0.0 | 7.0 | 2.0 | 5.0 | 2.0 | |
| M3 | 3.0 | 2.5 | 0.0 | 8.0 | 2.0 | 4.0 | 2.0 | 2.7 | 3.0 | 0.0 | 7.0 | 1.0 | 4.0 | 2.1 | |
| M4 | 3.2 | 3.5 | 0.0 | 8.0 | 2.0 | 4.0 | 2.2 | 2.8 | 4.0 | 0.0 | 8.0 | 0.0 | 4.0 | 2.6 | |
| p-value * | <0.01 | <0.01 | |||||||||||||
| p-value ** | M1 vs. M2: p < 0.001 M1 vs. M3: p < 0.001 M1 vs. M4: p < 0.001 M2 vs. M3: p = 1.00 M2 vs. M4: p = 1.00 M3 vs. M4: p = 1.00 | M1 vs. M2: p = 0.002 M1 vs. M3: p < 0.001 M1 vs. M4: p < 0.001 M2 vs. M3: p = 1.00 M2 vs. M4: p = 1.00 M3 vs. M4: p = 1.00 | |||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tkocz, P.; Matusz, T.; Kosowski, Ł.; Walewicz, K.; Argier, Ł.; Kuszewski, M.; Hagner-Derengowska, M.; Ptaszkowski, K.; Dymarek, R.; Taradaj, J. A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis. J. Clin. Med. 2021, 10, 4891. https://doi.org/10.3390/jcm10214891
Tkocz P, Matusz T, Kosowski Ł, Walewicz K, Argier Ł, Kuszewski M, Hagner-Derengowska M, Ptaszkowski K, Dymarek R, Taradaj J. A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis. Journal of Clinical Medicine. 2021; 10(21):4891. https://doi.org/10.3390/jcm10214891
Chicago/Turabian StyleTkocz, Piotr, Tomasz Matusz, Łukasz Kosowski, Karolina Walewicz, Łukasz Argier, Michał Kuszewski, Magdalena Hagner-Derengowska, Kuba Ptaszkowski, Robert Dymarek, and Jakub Taradaj. 2021. "A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis" Journal of Clinical Medicine 10, no. 21: 4891. https://doi.org/10.3390/jcm10214891
APA StyleTkocz, P., Matusz, T., Kosowski, Ł., Walewicz, K., Argier, Ł., Kuszewski, M., Hagner-Derengowska, M., Ptaszkowski, K., Dymarek, R., & Taradaj, J. (2021). A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis. Journal of Clinical Medicine, 10(21), 4891. https://doi.org/10.3390/jcm10214891