Abstract
Congenital uterine anomalies (CUA) may influence reproductive performance, resulting in adverse pregnancy associated complications. This study aimed to assess the association of CUA subtypes with reproductive, obstetric, and perinatal outcomes. We performed a systematic search of the MEDLINE, EMBASE, and Cochrane libraries for studies comparing pregnancy outcomes between women with CUA and those with a normal uterus. The random effects model was used to estimate the odds ratios (ORs) with a 95% confidence interval (CI). Women with CUA had a lower rate of live births (OR 0.47; 95% CI 0.33–0.69), and a higher rate of first trimester miscarriage (OR, 1.79; 95% CI 1.34–2.4), second trimester miscarriage (OR 2.92; 95% CI 1.35–6.32), preterm birth (OR 2.98; 95% CI 2.43–3.65), malpresentation (OR 9.1; 95% CI 5.88–14.08), cesarean section (OR 2.87; 95% CI 1.56–5.26), and placental abruption (OR 3.12; 95% CI 1.58–6.18). Women with canalization defects appear to have the poorest reproductive performance during early pregnancy. However, unification defects were associated with obstetric and neonatal outcomes throughout the course of pregnancy. It may be beneficial for clinicians to advise on potential complications that may be increased depending on the type and severity of CUA.
1. Introduction
The prevalence of congenital uterine anomalies (CUA) varies significantly, with reports ranging from 0.06 to 38% [1,2,3,4,5,6,7,8]. It can be inferred that these wide variations between studies are due to the inaccuracy of diagnostic tests, the use of different diagnostic techniques, differences in the evaluated patient population, and nonstandardized classification systems. Moreover, in many cases of CUA, it is difficult to detect because of a lack of awareness; therefore, the actual distribution and frequency of CUA occurrence in the general population are not accurately known. As medical attention starts with dysfunction (such as miscarriage or infertility), most studies have reported an increased prevalence of CUA in patients with reproductive problems.
The female reproductive tract differentiates from two Müllerian ducts, which develop within the first six weeks of fetal life [9,10]. Normal development of the female reproductive tract occurs through multistep processes, such as differentiation, migration, fusion, and subsequent absorption of the Müllerian system [11]. CUA are caused by an abnormal interruption during this development, and may result in an inability to conceive. The absence of a universally accepted classification system for CUA is problematic because such a system would allow physicians to categorize the symptomatology, treatment, and outcome in affected patients. The American Fertility Society (AFS) classification (1988) is the most commonly used classification, over the past three decades, for the categorization of CUA and is also used in most of the studies. Arcuate uterus is the mildest form of resorption failure or normal variation [12,13,14]. In arcuate uterus, the uterine cavity displays a concave contour toward the fundus and is not considered clinically relevant. Depending on the failure of organogenesis and varying degrees of fusion or absorption defects, CUA can be divided into unification defects of the Müllerian ducts (unicornuate, bicornuate, or didelphys uterus) and canalization defects from incomplete resorption of the midline septum (subseptate or septate uterus) [15].
The endometrial cavity is a space for successful embryo implantation and placenta formation, and defects in endometrial cavity formation may lead to infertility, recurrent miscarriage, and adverse pregnancy outcomes [16,17]. CUA vary, and not all patients have clinical symptoms. The pregnancy rate of women with CUA is not much different from that of women with a normal uterus, and pregnancy can be well maintained and lead to normal delivery. However, the frequency of obstetrical complications, such as miscarriage, preterm birth, intrauterine growth restriction (IUGR), and malpresentation, is high, depending on the type and severity of CUA [18,19]. Moreover, symptoms in CUA patients may include nonperiodic pelvic pain, menstrual pain, abnormal vaginal bleeding, and extrauterine pregnancies [9].
Our study aimed to evaluate the association of CUA with reproductive, obstetric, and neonatal outcomes in women, and determine whether CUA subtypes have a specific impact and the extent of the impact on a wide range of reproductive outcomes. To this end, the existing literature was thoroughly reviewed, and an updated meta-analysis was performed.
2. Materials and Methods
2.1. Search Strategy
We performed a literature search for all articles published until May 2021, and written in English, that reported comparisons of reproductive outcomes between women with CUA and women with a normal uterus. Two reviewers (Kim MA and Kim YH) independently performed an online systematic search using the MEDLINE, EMBASE, and Cochrane libraries. For the search, we combined the Medical Subject Headings (MeSH) and text terms covering CUA and reproductive outcomes. Table S1 outlines the full search strategies for each database. The reviewers manually searched and cross referenced the review articles found by electronic searches to locate additional cited articles that were missing from our online searches.
2.2. Selection Criteria
The inclusion criteria for this study were as follows: studies with an appropriate control group, and studies comparing reproductive outcomes between women with a diagnosis of CUA and women with a normal uterus. For the pregnancy outcomes of interest, the rate of clinical pregnancy (defined as the presence of an intrauterine gestational sac on sonography) among the total number of women, first trimester miscarriage, second trimester miscarriage, and recurrent pregnancy loss were investigated as reproductive outcomes. Live births, ectopic pregnancy, preterm birth, preterm premature rupture of membranes (PPROM), malpresentation, cesarean section, preeclampsia, placental abruption, postpartum hemorrhage, cervical incompetence, intrauterine fetal death (IUFD), placenta previa were investigated as obstetric outcomes. IUGR or small for gestational age (SGA; birth weight below the 10th percentile for the gestational age), low birth weight (LBW; <2500 g), and perinatal mortality among the total number of clinical pregnancies were investigated as neonatal outcomes. If the definition of the outcome was not specified, the classification of authors was based on a generalized definition. Studies that met the following criteria were excluded from the analysis: case reports and series, review articles, studies with no or an inappropriate control group, studies where data extraction was impossible, and studies reporting pregnancy outcomes in the same women before and after metroplasty. We performed data extraction for each subtype of CUA.
2.3. Study Selection
Two independent authors screened the titles and abstracts, and full articles were selected if the study met the selection criteria and reported the reproductive outcomes between women with CUA and those with a normal uterus. Full articles were retrieved for clarity, unless explicitly stated in the abstract. Studies unavailable online were collected directly from institutional libraries and references were cross checked to find additional articles. If more than one study by the same group of investigators describing the same population was published, the most recent version or the most comprehensive publication was used in the final meta-analysis.
2.4. Data Extraction
We extracted the following information from each article: name of authors, journal, study design, year of publication, country of patient, selection criteria, sample size of each group, mode of conception, type of CUA, diagnostic technique, classification of CUA, and data analyzed for reproductive outcomes.
2.5. Quality Assessment
We assessed the quality of the included studies using the Newcastle–Ottawa Scale (NOS). NOS evaluates three quality parameters: selection of the study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest for case-control or cohort studies, respectively. Each study had a maximum of nine points, giving scores for various questions in each category, and those with a score of 6 or more were considered high quality studies.
2.6. Statistical Analysis
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20] and the guidelines provided by the Cochrane Handbook for Systematic Reviews [21]. This study was not registered with the PROSPERO database. Reproductive outcomes were reported as odds ratios (ORs), representing the odds of adverse reproductive outcomes for women with CUA compared to women with a normal uterus. We used the random effects model to calculate pooled ORs and 95% confidence intervals (CI) [22]. We performed a subanalysis to analyze the differences in outcomes by the type of CUA. We considered I2 values > 25%, >50%, and >75% as evidence of low, moderate, and severe statistical heterogeneity, respectively. Sensitivity analysis was conducted to evaluate studies with a dominant effect on the meta-analysis or by excluding one study each time and assessing the effect on the main summary estimate. Statistical significance was set at p < 0.05. We performed all statistical analyses using Review Manager (RevMan) 5.4 (The Nordic Cochrane Centre: Copenhagen, Denmark).
3. Results
3.1. Study Characteristics
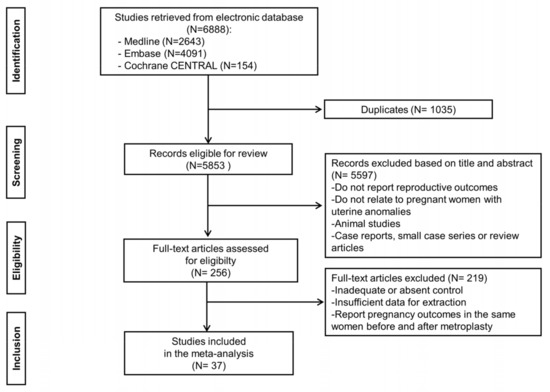
The systematic search retrieved 6888 citations in total, of which 1035 were excluded as duplicates. A total of 256 studies were considered potentially eligible for full text review by reviewing the titles and abstracts of the remaining 5853 manuscripts. Of these 256 studies, following the scrutiny of each manuscript, we identified 37 relevant studies [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59] that met the inclusion criteria as eligible for the meta-analysis (Figure 1).
Figure 1.
Flow diagram of the study selection process.
The baseline characteristics of all the included studies are shown in Table 1. Of the 37 studies included, only 5 were prospective studies, whereas the remaining 32 were retrospective studies. From these 37 studies, a total of 7053 women were identified as having CUA and 701,527 women with a normal uterus. All studies included women with different types of CUA. Of these 37 studies, 30 reported results for each specific subtype of CUA, whereas seven reported the results of the entire CUA without distinction of a particular subtype. The diagnostic methods for CUA also varied between the studies. They included hysterosalpingography (HSG), 2 dimensional (2D) or 3 dimensional ultrasound (3D-US), hysteroscopy, sonohysterography, laparoscopy, laparotomy, during cesarean section, and MRI. Each diagnostic method was used alone or in combination to confirm the CUA. The classification system used in each study to define the subtypes of CUA was inconsistent, but approximately half of the included studies used the classification of the AFS. Concerning the mode of conception, 13 studies included women who underwent assisted reproductive technologies (ART), two studies with natural conceptions (NC), seven studies with ART/NC, and 15 studies did not mention this. The median NOS for 37 studies was 7 (range, 6–9), and all included studies were considered high quality (Tables S2 and S3).
Table 1.
Characteristics of included studies.
3.2. Reproductive Outcomes
3.2.1. Clinical Pregnancy Rate
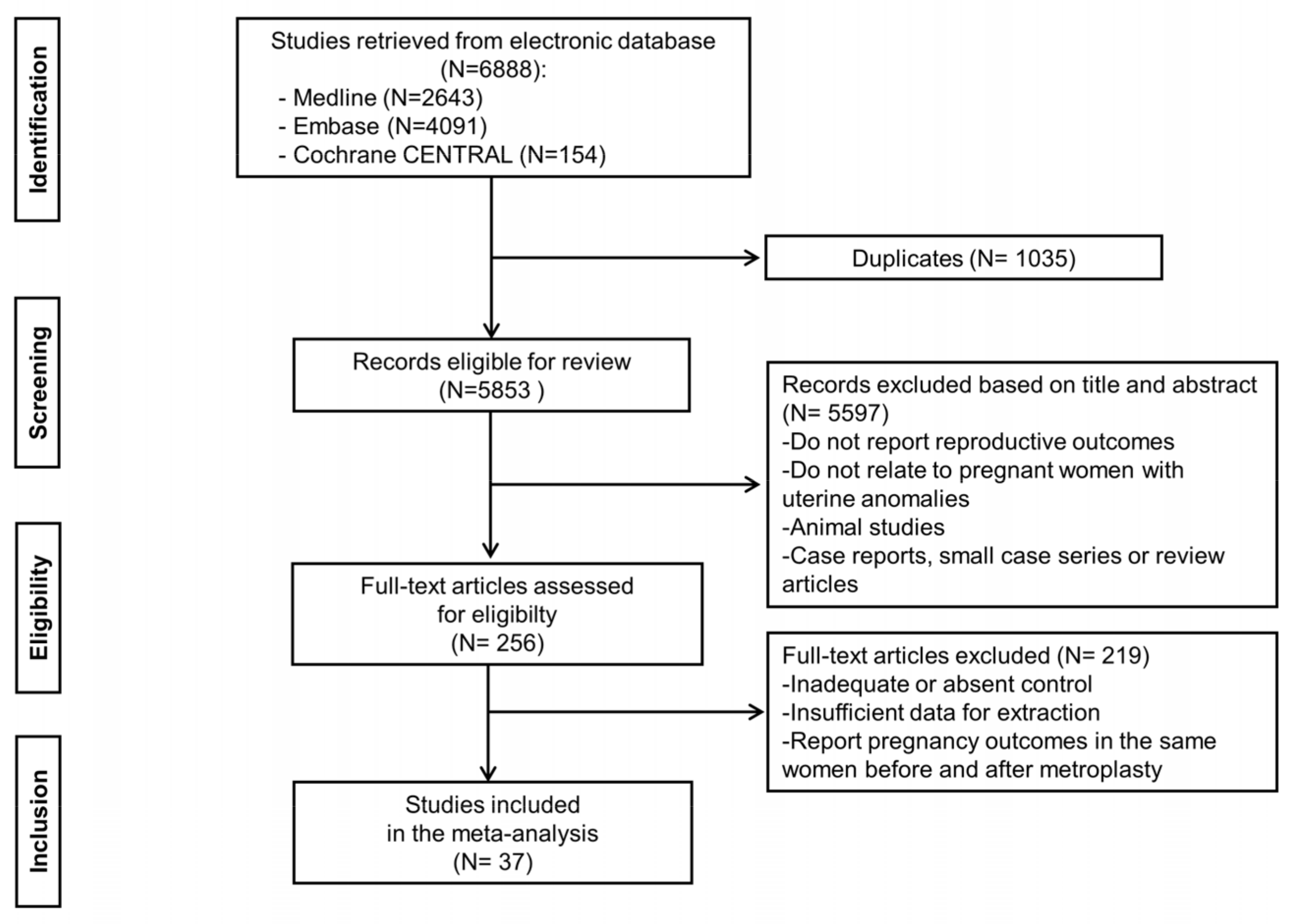
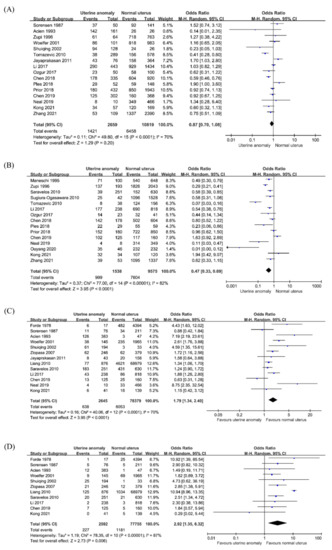
Sixteen studies compared the clinical pregnancy rate in 13,478 women, consisting of 2659 women with CUA and 10,819 women with a normal uterus. When all CUA subtypes were combined, there were no significant differences in the clinical pregnancy rate between women with CUA and the control group (OR, 0.87; 95% CI 0.7–1.08; p = 0.2; I2 = 70%; Figure 2A). In the subgroup analysis by CUA subtype (Table 2), pooled results in women with an arcuate uterus showed no significant difference in clinical pregnancy rate compared to that in women with a normal uterus (OR, 1.0; 95% CI 0.64–1.58; p = 0.99; I2 = 73%; 6 studies). In the canalization defects (OR 0.59; 95% CI 0.32–1.08; p = 0.09; I2 = 52%; seven studies), the clinical pregnancy rate decreased significantly in septate uterus (OR 0.45; 95% CI 0.21–0.95; p = 0.04; I2 = 31%; six studies) but not in subseptate (OR 0.73; 95% CI 0.28–1.92; p = 0.53; I2 = 60%; five studies). In the unification defects (OR 0.72; 95% CI 0.57–0.9; p = 0.005; I2 = 40%; 10 studies), there were no significant differences in clinical pregnancy rate between women with bicornuate uterus (OR 0.57; 95% CI 0.32–1.03; p = 0.06; I2 = 3%; five studies) or didelphys uterus (OR 0.36; 95% CI 0.09–1.39; p = 0.14; I2 = 0%; three studies) than that in women with a normal uterus. However, a meta-analysis of women with unicornuate uterus showed a significant decrease in the clinical pregnancy rate (OR 0.75; 95% CI 0.58–0.99; p = 0.04; I2 = 59%; nine studies).
Figure 2.
Reproductive outcomes in women with congenital uterine anomalies. (A) Clinical pregnancy rate, (B) live birth, (C) first trimester miscarriage, (D) second trimester miscarriage.
Table 2.
Reproductive, obstetric, and neonatal outcomes according to the subtype of congenital uterine anomalies.
3.2.2. Live Birth
Fifteen studies compared the rate of live births in a total of 11,113 pregnancies, comprising 1538 pregnancies in women with CUA and 9575 pregnancies in women with a normal uterus. The pooled analysis showed a lower rate of live birth in women with CUA (OR, 0.47; 95% CI, 0.33–0.69; p < 0.001; I2 = 82%; Figure 2B) than that in women with a normal uterus. In subgroup analysis according to the subtype of CUA (Table 2), there was a significant decrease in live birth rate in women with arcuate uterus (OR, 0.45; 95% CI, 0.22–0.92; p = 0.03; I2 = 88%; five studies), septate uterus (OR 0.25; 95% CI 0.09–0.75; p = 0.01; I2 = 49%; four studies), and unicornuate uterus (OR 0.57; 95% CI 0.34–0.96; p = 0.04; I2 = 69%; 10 studies), but not in other types of CUA.
3.2.3. First Trimester Miscarriage
Thirteen studies reported data on first trimester miscarriage in a total of 81,024 pregnancies, which comprised 2645 pregnancies in women with CUA and 78,379 pregnancies in women with a normal uterus. The pooled analysis showed that all women with CUA had a higher rate of first trimester miscarriage than that in women with a normal uterus (OR 1.79; 95% CI 1.34–2.4; p <0.001; I2 = 70%; Figure 2C). Subgroup analysis according to the subtype of CUA (Table 2) showed that the risk of first trimester miscarriage was not significantly different between women with an arcuate uterus and those with a normal uterus (OR 1.38; 95% CI 0.88–2.17; p = 0.16; I2 = 45%; six studies). A meta-analysis of canalization defects (OR 3.32; 95% CI 1.96–5.6; p < 0.001; I2 = 64%; six studies) revealed that subseptate uterus (OR 4.36; 95% CI 2.64–7.21; p < 0.001; I2 = 15%; four studies) and septate uterus (OR 2.55; 95% CI 1.33–4.91; p = 0.005; I2 = 58%; five studies) had an increased risk of first trimester miscarriage. The meta-analysis of unification defects (OR 1.77; 95% CI 1.18–2.65; p = 0.006; I2 = 54%; eight studies) revealed that only in bicornuate uterus (OR 2.59; 95% CI 1.25–5.35; p = 0.01; I2 = 65%; six studies) had a higher risk of first trimester miscarriage, but not in unicornuate uterus (OR, 1.45; 95% CI, 0.85–2.48; p = 0.17; I2 = 37%; seven studies) and didelphys uterus (OR 1.26; 95% CI 0.33–4.76; p = 0.73; I2 = 67%; four studies).
3.2.4. Second-Trimester Miscarriage
Eleven studies reported data on second trimester miscarriage in 80,347 pregnancies, consisting of 2592 pregnancies in women with CUA and 77,755 pregnancies in women with a normal uterus. The meta-analysis indicated that all women with CUA had a higher rate of second trimester miscarriage than that in women with a normal uterus (OR 2.92; 95% CI 1.35–6.32; p = 0.006; I2 = 87%; Figure 2D). The subgroup analysis by type of CUA (Table 2) showed that women with an arcuate uterus (OR 2.01; 95% CI 1.03–3.93; p = 0.04; I2 = 11%; five studies) had a higher rate of second trimester miscarriage than that in women with a normal uterus. In canalization defects (OR 3.38; 95% CI 1.94–5.88; p < 0.001; I2 = 18%; five studies), second trimester miscarriage increased significantly in septate uterus (OR 4.33; 95% CI 2.52–7.43; p < 0.001; I2 = 0%; four studies), but not in subseptate uterus (OR 1.9; 95% CI 0.54–6.75; p = 0.32; I2 = 41%; three studies). In unification defects (OR 2.28; 95% CI 1.45–3.6; p < 0.001; I2 = 0%; seven studies), there were no significant differences in second trimester miscarriage between women with unicornuate uterus (OR 2.1, 95% CI 0.95–4.61; p = 0.07; I2 = 0%; six studies), didelphys uterus (OR 1.72; 95% CI 0.6–4.9; p = 0.31; I2 = 0%; four studies), and women with a normal uterus. However, a meta-analysis of women with bicornuate uterus showed a significant increase in second trimester miscarriage (OR 2.71; 95% CI 1.4–5.23; p = 0.003; I2 = 0%; five studies).
3.3. Obstetric Outcomes
3.3.1. Preterm Birth
Twenty-six studies reported the incidence of preterm birth in 702,769 pregnancies, consisting of 6474 pregnancies in women with CUA and 696,295 pregnancies in women with a normal uterus. The overall risk of preterm birth was significantly higher among women with CUA (OR 2.98; 95% CI 2.43–3.65; p < 0.001; I2 = 82%; Figure 3A), except for the arcuate uterus (OR 1.62; 95% CI 0.86–3.04; p = 0.13; I2 = 56%; 10 studies), compared to that in women with a normal uterus. For canalization defects (OR 3.11; 95% CI 2.24–4.32; p < 0.001; I2 = 12%; nine studies), the pooled analysis showed a significantly higher risk of preterm birth in the subseptate uterus (OR 3.15; 95% CI 1.34–7.4; p = 0.009; I2 = 61%; four studies) and septate uterus (OR 2.93; 95% CI 2.01–4.28; p < 0.001; I2 = 0%; eight studies). For unification defects (OR 3.5; 95% CI 2.74–4.46; p <0.001; I2 = 64%; 16 studies), women with unicornuate uterus (OR 2.83, 95% CI 1.92–4.19; p < 0.001; I2 = 53%; 13 studies), bicornuate uterus (OR 3.69; 95% CI 2.6–5.22; p < 0.001; I2 = 55%; 10 studies), and didelphys uterus (OR 4.93; 95% CI 3.6–6.75; p < 0.001; I2 = 13%; nine studies) had an increased rate of preterm birth compared to that in women with a normal uterus (Table 2).
Figure 3.
Obstetric outcomes in women with congenital uterine anomalies. (A) Preterm birth, (B) malpresentation, (C) cesarean section, (D) placental abruption.
3.3.2. Malpresentation
Sixteen studies reported fetal malpresentation in 690,744 pregnancies, comprising 5098 pregnancies in women with CUA and 685,646 pregnancies in women with a normal uterus. The overall risk of malpresentation was significantly increased among women with CUA (OR 9.1; 95% CI 5.88–14.08; p < 0.001; I2 = 97%; Figure 3B) compared to that in women with a normal uterus. The subgroup analysis in women with arcuate uterus (OR 3.27; 95% CI 1.66–6.44; p < 0.001; I2 = 52%; seven studies) showed a significantly higher risk of malpresentation. In the case of canalization uterus (OR 11.39; 95% CI 6.24–20.78; p < 0.001; I2 = 81%; eight studies), subseptate uterus (OR 11.42; 95% CI 3.74–34.86; p < 0.001; I2 = 85%; four studies), and septate uterus (OR 11.49; 95% CI 5.24–25.17; p < 0.001; I2 = 80%; eight studies) increased the risk of malpresentation compared to that in women with a normal uterus. In unification defects (OR 8.68; 95% CI 5.82–12.95; p < 0.001; I2 = 91%; 10 studies), unicornuate uterus (OR 8.09; 95% CI 3.14–20.84; p < 0.001; I2 = 78%; eight studies), bicornuate uterus (OR 10.87; 95% CI 6.68–17.68; p < 0.001; I2 = 86%; nine studies), and didelphys uterus (OR 7.2; 95% CI 3.09–16.74; p < 0.001; I2 = 94%; nine studies) showed a higher fetal malpresentation rate (Table 2).
3.3.3. Cesarean Section
Twenty-one studies reported data on the incidence of cesarean section in a total of 698,716 pregnancies, which comprised 5283 pregnancies in women with CUA and 693,433 pregnancies in women with a normal uterus. A significant difference was observed in the incidence of cesarean section among women with all CUA (OR, 2.87; 95% CI, 1.56–5.26; p < 0.001; I2 = 99%; Figure 3C), except for unicornuate uterus (OR 1.24; 95% CI 0.76–2.03; p = 0.39; I2 = 71%; nine studies), compared to that in women with a normal uterus. The outcomes of subgroup analysis (Table 2) showed a significantly higher risk of cesarean section in the arcuate uterus (OR 2.22; 95% CI 1.07–4.61; p = 0.03; I2 = 61%; six studies), subseptate uterus (OR 5.91; 95% CI 1.59–21.95; p = 0.008; I2 = 87%; three studies), septate uterus (OR 4.84; 95% CI 2.33–10.02; p < 0.001; I2 = 68%; six studies), bicornuate uterus (OR 5.23; 95% CI 2.11–12.96; p < 0.001; I2 = 95%; eight studies), and didelphys uterus (OR 7.55; 95% CI 2.4–23.72; p < 0.001; I2 = 96%; seven studies).
3.3.4. Placental Abruption
Nine studies reported data on the incidence of placental abruption in a total of 618,188 pregnancies, consisting of 3145 pregnancies in women with CUA and 615,043 pregnancies in women with a normal uterus. The overall risk of placental abruption was significantly higher among women with CUA (OR 3.12; 95% CI, 1.58–6.18; p = 0.001; I2 = 84%; Figure 3D) than that in women with a normal uterus. In the subgroup analysis based on CUA subtype (Table 2), it was shown that there was a significantly higher risk of placental abruption in the arcuate uterus (OR 4.56; 95% CI 1.03–20.06; p = 0.04; I2 = 36%; four studies), septate uterus (OR 5.33; 95% CI 1.5–18.95; p = 0.01; I2 = 0%; three studies), unicornuate uterus (OR 7.78; 95% CI 1.99–30.45; p = 0.003; I2 = 0%; three studies), and bicornuate uterus (OR 6.53; 95% CI 1.96–21.78; p = 0.002; I2 = 70%; four studies), but not in the didelphys uterus (OR 2.68; 95% CI 0.51–14.17; p = 0.24; I2 = 0%; three studies).
3.4. Neonatal Outcomes
3.4.1. Intrauterine Growth Restriction or Small for Gestational Age
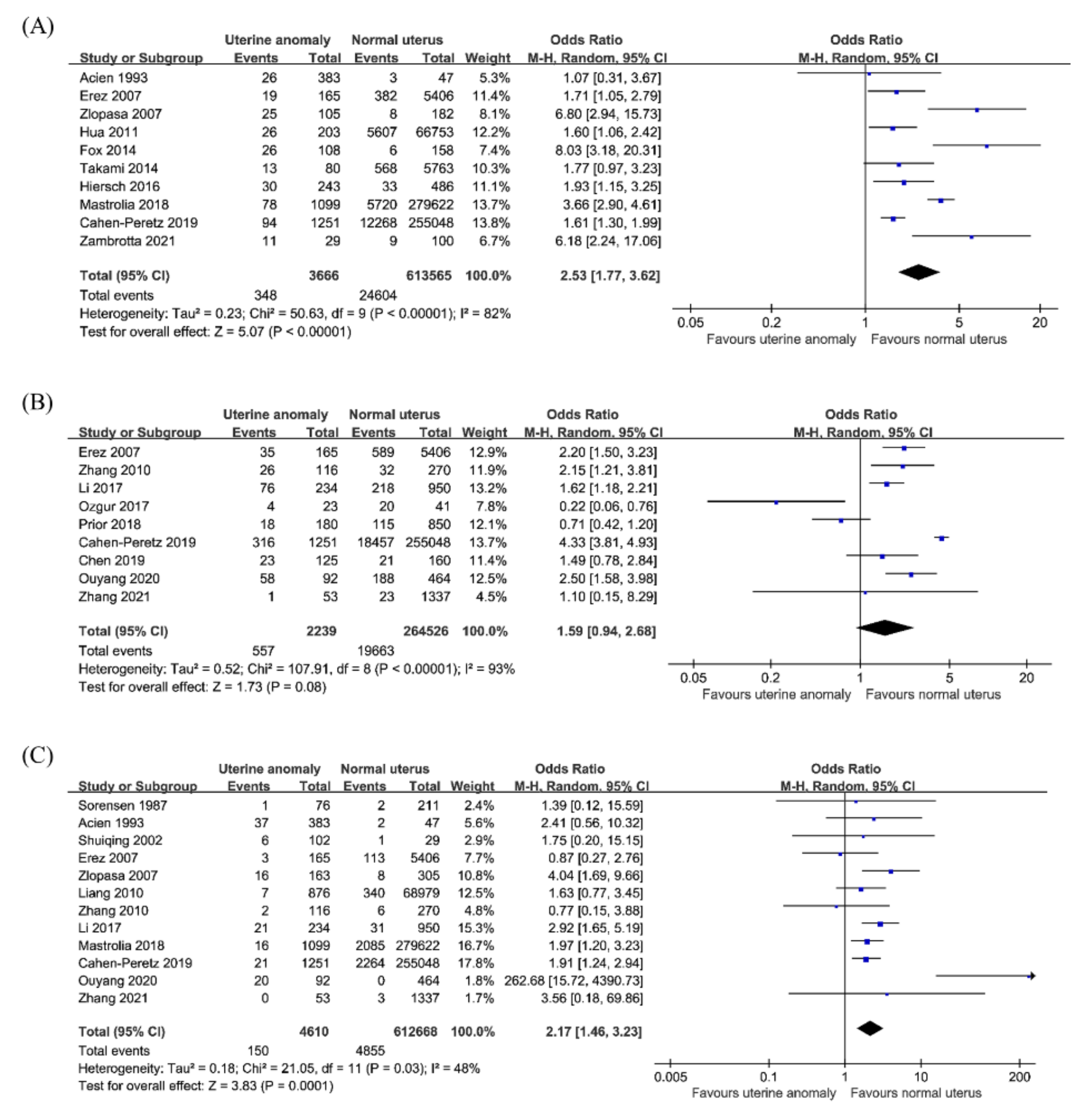
Ten studies reported the incidence of IUGR or SGA in 617,231 pregnancies, consisting of 3666 pregnancies in women with CUA and 613,565 pregnancies in women with a normal uterus. Meta-analysis of ten studies revealed that women with CUA have an increased risk of IUGR or SGA compared to that in women with a normal uterus (OR 2.53; 95% CI 1.77–3.62; p < 0.001; I2 = 82%; Figure 4A). In the subgroup analysis (Table 2), no significant differences in the rates of IUGR or SGA were observed in women with arcuate uterus (OR 3.77; 95% CI 0.92–15.46; p = 0.07; I2 = 75%; five studies) and septate uterus (OR 1.9; 95% CI 0.89–4.08; p = 0.1; I2 = 2%; five studies). The outcome of the subgroup analysis showed that the risk of IUGR or SGA was significantly higher in women with subseptate uterus (OR 2.4; 95% CI 1.13–5.09; p = 0.02; I2 = 0%; three studies), unicornuate uterus (OR 3.5; 95% CI 1.24–9.91; p = 0.02; I2 = 43%; five studies), bicornuate uterus (OR 2.84; 95% CI 1.68–4.8; p < 0.001; I2 = 57%; six studies), and didelphys uterus (OR 4.03; 95% CI 2.0–8.12; p < 0.001; I2 = 44%; six studies) than that in women with a normal uterus.
Figure 4.
Neonatal outcomes in women with congenital uterine anomalies. (A) Intrauterine growth restriction or small for gestational age, (B) low birth weight, (C) perinatal mortality.
3.4.2. Low Birth Weight
Nine studies reported data on the incidence of LBW in 266,765 pregnancies, consisting of 2239 pregnancies in women with CUA and 264,526 pregnancies in women with a normal uterus. The result for LBW was not significant (OR 1.59; 95% CI 0.94–2.68; p = 0.08; I2 = 93%; Figure 4B) in women with CUA compared to women with a normal uterus. In the subgroup analysis by CUA subtype (Table 2), no significant differences were found between LBW rate in women with arcuate uterus (OR, 1.5; 95% CI 0.7–3.25; p = 0.3; I2 = 0%; two studies) or septate uterus (OR 1.73; 95% CI 0.91–3.29; p = 0.09; I2 = 0%; two studies) and that in women with a normal uterus. The risk of LBW was a higher in women with unification defects (OR 1.99; 95% CI 1.38–2.87; p < 0.001; I2 = 57%; seven studies), with an OR of 1.8 in unicornuate uterus (OR 1.84; 95% CI 1.08–3.14; p = 0.02; I2 = 72%; seven studies), 1.9 in bicornuate uterus (OR 1.91; 95% CI 1.12–3.27; p = 0.02; I2 = 0%; two studies), and 2.9 in didelphys uterus (OR 2.87; 95% CI 1.38–5.97; p = 0.005; I2 = 0%; two studies).
3.4.3. Perinatal Mortality
Twelve studies reported data on perinatal mortality in a total of 617,278 pregnancies, consisting of 4610 pregnancies in women with CUA and 612,668 pregnancies in women with a normal uterus. The overall risk of perinatal mortality was higher in women with CUA than that in women with a normal uterus (OR, 2.17; 95% CI 1.46–3.23; p < 0.001; I2 = 48%; Figure 4C). In the subgroup analysis by CUA subtype (Table 2), no significant differences were observed in perinatal mortality rate in women with an arcuate uterus (OR 2.11; 95% CI 0.79–5.63; p = 0.14; I2 = 0%; five studies), subseptate uterus (OR 2.51; 95% CI 0.82–7.69; p = 0.11; I2 = 0%; three studies), and didelphys uterus (OR 1.75; 95% CI 0.77–3.96; p = 0.18; I2 = 0%; five studies). Conversely, women with a septate uterus (OR 2.57; 95% CI 1.08–6.08; p = 0.03; I2 = 0%; six studies), unicornuate uterus (OR 3.85; 95% CI 1.61–9.2; p = 0.002; I2 = 42%; nine studies), and bicornuate uterus (OR 3.17; 95% CI 2.08–4.84; p < 0.001; I2 = 0%; seven studies) showed a higher rate of perinatal mortality than that in those with a normal uterus.
3.5. Other Outcomes
The pooled analysis showed that women with CUA had a higher rate of preeclampsia (OR 1.25; 95% CI 1.07–1.46; p = 0.004; I2 = 0%; five studies), IUFD (OR 2.06; 95% CI 1.36–3.11; p < 0.001; I2 = 7%; seven studies), PPROM (OR 3.5; 95% CI 2.22–5.54; p < 0.001; I2 = 26%; three studies), recurrent pregnancy loss (OR 2.61; 95% CI 2.31–2.94; p < 0.001; I2 = 0%; three studies), and cervical incompetence (OR 7.94; 95% CI 3.81–16.55; p < 0.001; I2 = 85%; four studies) than that in women with a normal uterus. No significant differences in the rate of ectopic pregnancy (OR 1.28; 95% CI 0.81–2.02; p = 0.29; I2 = 0%; 11 studies), postpartum hemorrhage (OR 1.02; 95% CI 0.67–1.55; p = 0.93; I2 = 0%; six studies), and placenta previa (OR 1.56; 95% CI 0.6–4.07; p = 0.36; I2 = 83%; six studies) were found between women with CUA and those with a normal uterus. The outcomes from the subgroup analysis according to the CUA subtype are shown in Table 2. Concerning ectopic pregnancy, preeclampsia, and placenta previa, no significant differences were noted in the arcuate uterus and canalization defects. In the unification defects, the rate of placenta previa was significantly higher in women with a bicornuate uterus (OR 3.59; 95% CI 1.89–6.82; p <0.001; I2 = 0%; four studies) than that in women with a normal uterus. Additionally, the overall risk of PPROM (OR 4.66; 95% CI 2.83–7.69; p < 0.001; I2 = 0%; two studies), and cervical incompetence (OR 9.04; 95% CI 6.11–13.37; p < 0.001; I2 = 0%; three studies) was increased in women with unification defects. Likewise, women with septate uterus showed a higher rate of PPROM (OR 4.66; 95% CI 1.79–12.15; p = 0.002; I2 = 0%; two studies) than that in women with a normal uterus. In women with bicornuate uterus, the risk of recurrent pregnancy loss (OR 2.69; 95% CI 2.05–3.52; p < 0.001; I2 = 0%; two studies) increased, and in women with unicornuate uterus, the risk of IUFD (OR 2.4; 95% CI 1.27–4.53; p = 0.007; I2 = 0%; four studies) increased.
4. Discussion
This systematic review and meta-analysis investigated the reproductive, obstetric, and neonatal outcomes of women with CUA. This extensive and updated meta-analysis is an attempt to review all published studies on the reproductive effects of CUA, to investigate the association between CUA and all obstetric complications analyzed in the studies. Based on the results of this meta-analysis, the presence of CUA has a negative impact on most pregnancy outcomes, further supporting the theory of inadequate implantation, fetal development, and pregnancy maintenance in CUA.
We found a significant decrease in the clinical pregnancy rate in the septate uterus and unicornuate uterus, over threefold increased risk of miscarriage in women with canalization defects, and a twofold increased risk in the bicornuate uterus, but this risk of miscarriage was not found in the unicornuate and didelphys uterus. The risk of preterm birth in women with both canalization and unification defects was over threefold higher than that in women with a normal uterus. As gestational weeks progressed, malpresentation and, consequently, cesarean section rates were significantly higher in all subtypes of CUA due to a lack of uterine volume corresponding to fetal growth in the second trimester of pregnancy. Particularly, in all subtypes of CUA, the risk of placental abruption was ninefold higher in the canalization defects, sevenfold higher in the unification defects, and fivefold higher even in the arcuate uterus. Additionally, we found that unification defects can be associated with a range of obstetric and fetal complications, including LBW (twofold risk), IUGR (over threefold risk), IUFD (2.5-fold risk), perinatal mortality (threefold risk), placenta previa (over threefold risk), and cervical incompetence (ninefold risk). We noted a similar risk of PPROM has been shown in the septate uterus and unification defects, with a fivefold increase. A septate uterus was not associated with adverse neonatal outcomes, including LBW, IUGR or SGA, and IUFD, except for perinatal mortality (threefold risk). There were no significant differences in preeclampsia and ectopic pregnancy between the CUA subtypes and a normal uterus. Unlike other CUA subtypes, there was no significant difference in most pregnancy outcomes between women with an arcuate uterus and those with a normal uterus, except for second trimester miscarriage, placental abruption, malpresentation, and cesarean section. An arcuate uterus, milder forms of CUA, or normal variants are less likely to influence fertilization and early implantation processes, and impact the risk of miscarriage. The more severe forms of CUA affect all stages of reproduction, from fertilization to early and late pregnancy complications.
The causes and pathophysiological mechanisms of various reproductive and obstetrical complications in patients with CUA remain unclear. Embryo implantation is influenced by the vascularity and thickness of the endometrium and the morphology of the uterine cavity [60]. The uterine septum is known to be composed of fibroelastic tissue with inadequate vascularization of the endometrium, which reduces endometrial receptivity to estrogen, resulting in reduced endometrial maturation and proliferation [61,62]. Miscarriage can easily occur as the embryos implant on the septum because the septum with suboptimal endometrium is morbid with reduced blood supply. Even if implantation occurs, it does not provide a proper environment for subsequent placental and embryonic growth. In contrast, Dabirashrafi et al. found significantly more blood vessels and muscle tissues and less connective tissue in the septum of the uterus, which might result in poor decidualization, placentation, and uncoordinated muscle contractility [63]. Abnormalities of space in the uterine cavity, arrangement of uterine musculature, and impaired ability to distend are likely to have a negative effect on pregnancy maintenance. In addition, increased muscle mass and decreased connective tissue in the malformed cervix can cause asymmetric uterine cavity pressure, impairing the ability of distention and growth of the uterine cavity, which also leads to late miscarriage and preterm birth.
Currently, there is no universally accepted standard classification for CUA [11]. The differences in sensitivity and specificity of the diagnostic tests inevitably affect the classification and diagnosis of CUA subtypes. Therefore, classification systems and standardized tests are essential for counseling and determining the management of CUA patients. Accurate assessment of the internal and external uterine contours is critical for diagnosing and classifying CUA. Previously, the gold standard diagnostic method was a combination of laparoscopy and hysteroscopy. However, imaging techniques are less invasive, such as 2D- or 3D-US, HSG, sonohysterography, and magnetic resonance imaging (MRI) for screening, diagnosing, and classifying CUA [64]. Particularly, 2D-US and HSG are helpful in screening for CUA, while 3D-US and MRI are suitable for categorizing CUA accurately [40,65,66,67].
There is still insufficient evidence on the efficacy and safety of surgical interventions for improving reproductive performance. There is a lack of evidence on improving reproductive outcomes with surgical intervention. Some reports have shown that hysteroscopic septal division can reduce the risk of miscarriage and improve live birth rates [6,68,69,70], but surgical management for incidentally diagnosed septum and fusion or unification defects is controversial and unproven [71]. Various hysteroscopic instruments, including microscissors, forceps, operating loop, electrosurgical needle, and laser energy, have been proposed for surgical correction [72]. Gradually, several methods are being introduced to help the proliferation of endometrial tissue, reduce adhesion formation and minimize intraoperative or postoperative complications [73]. Tissue vaporization and coagulation with low power diode laser energy can rapidly remove the uterine septum without damaging the underlying myometrium [74,75]. Still, there is a lack of large scale studies on which technique is better.
Chan et al. [18] previously reported the correlation between CUA and representative pregnancy outcomes, such as miscarriage, preterm birth, and malpresentation, by meta-analyzing nine studies. Venetis et al. [19] analyzed the pregnancy outcomes in women with CUA by adding LBW, IUGR, PPROM, placental abruption, and perinatal mortality extracted from 24 studies. We conducted an extensive and updated meta-analysis to evaluate the association between the different types of CUA and various reproductive, obstetric, and neonatal outcomes, in 37 studies where a more comprehensive assessment of the evidence was available. Undoubtedly, the negative impacts of CUA on pregnancy begin in the early stages of fertilization and the impacts span the entire reproductive process. However, the lack of data on individual CUA subtypes makes it difficult to draw clear conclusions about the exact subtype specific effects on complications and their underlying mechanisms. Although most women with CUA experience a normal reproductive outcome, it is necessary to advise on the risks that may be increased depending on the type and severity of CUA.
To fully investigate the effects of CUA on obstetric and fetal complications, collecting all published studies and conducting a thorough and conclusive meta-analysis may be hampered by the heterogeneity of the currently available studies. This meta-analysis was confounded by the heterogeneity of the included clinical studies. The use of several diagnostic methods with variable accuracies, the absence of a universal classification system, discrepancies in interpretation of CUA classification, and the heterogeneity of study populations have all contributed to a difficulty in deriving the study results. As we collected and analyzed studies published over the past half century, there are inevitable differences in study population characteristics, diagnostic methods, classification system of CUA, and definition of outcome. Most of the included studies have a retrospective design, and various confounding variables, such as age, body mass index, hormonal status, and socioeconomic status, that can introduce bias. Therefore, future studies should be conducted through well designed prospective observational studies that consider these potential confounding factors to establish more detailed evidence of the risk of adverse reproductive outcomes in women with CUA.
This study showed that all subtypes of CUA have an increased risk of second trimester miscarriage, preterm birth, placental abruption, fetal malpresentation, and cesarean section. It was found that women with canalization defects seem to have the poorest reproductive performance in early pregnancy. In unification defects, only the unicornuate uterus is shown to reduce fertility, and bicornuate uterus increases miscarriage, while didelphys uterus is not associated with risk of fertility and miscarriage. However, unification defects were primarily associated with obstetric and neonatal outcomes throughout pregnancy. The abnormal uterine environment disrupts fertilization, implantation, and later pregnancy and birth outcomes. In conclusion, women with CUA can develop adverse reproductive, obstetric, and neonatal outcomes according to CUA subtypes. The uterus is an essential organ in which critical phenomena of the reproductive process occur, including sperm migration, embryo implantation, fetal development and growth, and, finally, the induction of labor and childbirth. CUA can influence these uterine functions and prevent successful pregnancies. It may be beneficial for clinicians to care for women with CUA and inform them about potential complications and treatment options through evidence based counseling and an accurate diagnosis before and during pregnancy.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/jcm10214797/s1, Table S1: Search strategies; Table S2: Study Quality Assessment for Cohort studies (Newcastle–Ottawa Scale); Table S3: Study Quality Assessment for Case–Control Studies (Newcastle–Ottawa Scale).
Author Contributions
M.-A.K. and Y.-H.K.: the conception and design of the study; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript; H.S.K.: analysis and interpretation of data; M.-A.K., H.S.K. and Y.-H.K.: critical revision of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a faculty research grant of Yonsei University College of Medicine (6-2013-0183).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
All authors declare that they have no conflict of interest.
References
- Simón, C.; Martinez, L.; Pardo, F.; Tortajada, M.; Pellicer, A. Müllerian defects in women with normal reproductive outcome. Fertil. Steril. 1991, 56, 1192–1193. [Google Scholar] [CrossRef]
- Makino, T.; Hara, T.; Oka, C.; Toyoshima, K.; Sugi, T.; Iwasaki, K.; Umeuchi, M.; Iizuka, R. Survey of 1120 Japanese women with a history of recurrent spontaneous abortions. Eur. J. Obstet. Gynecol. Reprod. Biol. 1992, 44, 123–130. [Google Scholar] [CrossRef]
- Makino, T.; Umeuchi, M.; Nakada, K.I.; Nozawa, S.; Iizuka, R. Incidence of congenital uterine anomalies in repeated reproductive wastage and prognosis for pregnancy after metroplasty. Int. J. Fertil. 1992, 37, 167–170. [Google Scholar] [PubMed]
- Clifford, K.; Rai, R.; Watson, H.; Regan, L. An informative protocol for the investigation of recurrent miscarriage: Preliminary experience of 500 consecutive cases. Hum. Reprod. 1994, 9, 1328–1332. [Google Scholar] [CrossRef] [PubMed]
- Acién, P. Incidence of mullerian defects in fertile and infertile women. Hum. Reprod. 1997, 12, 1372–1376. [Google Scholar] [CrossRef] [Green Version]
- Homer, H.A.; Li, T.C.; Cooke, I.D. The septate uterus: A review of management and reproductive outcome. Fertil. Steril. 2000, 73, 1–14. [Google Scholar] [CrossRef]
- Guimarães Filho, H.A.; Mattar, R.; Pires, C.R.; Araujo Júnior, E.; Moron, A.F.; Nardozza, L.M. Prevalence of uterine defects in habitual abortion patients attended on at a university health service in brazil. Arch. Gynecol. Obstet. 2006, 274, 345–348. [Google Scholar] [CrossRef]
- Guimarães Filho, H.A.; Mattar, R.; Pires, C.R.; Araujo Júnior, E.; Moron, A.F.; Nardozza, L.M. Comparison of hysterosalpingography, hysterosonography and hysteroscopy in evaluation of the uterine cavity in patients with recurrent pregnancy losses. Arch. Gynecol. Obstet. 2006, 274, 284–288. [Google Scholar] [CrossRef]
- Lin, P.C.; Bhatnagar, K.P.; Nettleton, G.S.; Nakajima, S.T. Female genital anomalies affecting reproduction. Fertil. Steril. 2002, 78, 899–915. [Google Scholar] [CrossRef]
- Motta, P.M.; Nottola, S.A.; Makabe, S. Natural history of the female germ cell from its origin to full maturation through prenatal ovarian development. Eur. J. Obstet. Gynecol. Reprod. Biol. 1997, 75, 5–10. [Google Scholar] [CrossRef]
- Rackow, B.W.; Arici, A. Reproductive performance of women with müllerian anomalies. Curr. Opin. Obstet. Gynecol. 2007, 19, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Buttram, V.C., Jr.; Gomel, V.; Siegler, A.; DeCherney, A.; Gibbons, W.; March, C. The american fertility society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil. Steril. 1988, 49, 944–955. [Google Scholar]
- Salim, R.; Regan, L.; Woelfer, B.; Backos, M.; Jurkovic, D. A comparative study of the morphology of congenital uterine anomalies in women with and without a history of recurrent first trimester miscarriage. Hum. Reprod. 2003, 18, 162–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinonen, P.K.; Saarikoski, S.; Pystynen, P. Reproductive performance of women with uterine anomalies. An evaluation of 182 cases. Acta Obstet. Gynecol. Scand. 1982, 61, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Chandler, T.M.; Machan, L.S.; Cooperberg, P.L.; Harris, A.C.; Chang, S.D. Mullerian duct anomalies: From diagnosis to intervention. Br. J. Radiol. 2009, 82, 1034–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kupesic, S. Clinical implications of sonographic detection of uterine anomalies for reproductive outcome. Ultrasound Obstet. Gynecol. 2001, 18, 387–400. [Google Scholar] [CrossRef] [Green Version]
- Kupesic, S.; Kurjak, A. Diagnosis and treatment outcome of the septate uterus. Croat. Med. J. 1998, 39, 185–190. [Google Scholar]
- Chan, Y.Y.; Jayaprakasan, K.; Tan, A.; Thornton, J.G.; Coomarasamy, A.; Raine-Fenning, N.J. Reproductive outcomes in women with congenital uterine anomalies: A systematic review. Ultrasound Obstet. Gynecol. 2011, 38, 371–382. [Google Scholar] [CrossRef]
- Venetis, C.A.; Papadopoulos, S.P.; Campo, R.; Gordts, S.; Tarlatzis, B.C.; Grimbizis, G.F. Clinical implications of congenital uterine anomalies: A meta-analysis of comparative studies. Reprod. Biomed. Online 2014, 29, 665–683. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Reprint--preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P. Characteristics of meta-analyses and their component studies in the cochrane database of systematic reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, X. Clinical outcomes analysis of infertile women with unicornuate uterus in ivf-et. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102111. [Google Scholar] [CrossRef]
- Zambrotta, E.; Di Gregorio, L.M.; Di Guardo, F.; Agliozzo, R.; Maugeri, G.C.; Gulino, F.A.; Cutello, S.; Cerana, M.C.; Palumbo, M. Congenital uterine anomalies and perinatal outcomes: A retrospective single-center cohort study. Clin. Exp. Obstet. Gynecol. 2021, 48, 161–164. [Google Scholar]
- Kong, W.Y.; Zhao, S.R.; Deng, K.; Zhang, Q.; Liu, W.; Yan, L. Effects of bicornuate uterus on pregnancy and obstetric outcomes of in vitro fertilization / intracytoplasmic sperm injection. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Y.; Cai, P.; Gong, F.; Lin, G.; Qin, J.; Li, X. The risk of twin pregnancies should be minimized in patients with a unicornuate uterus undergoing ivf-et. Sci. Rep. 2020, 10, 5571. [Google Scholar] [CrossRef] [PubMed]
- Neal, S.A.; Morin, S.J.; Werner, M.D.; Gueye, N.A.; Pirtea, P.; Scott, R.T., Jr.; Goodman, L.R. Three-dimensional ultrasound diagnosis of t-shaped uterus is associated with adverse pregnancy outcomes after embryo transfer. Reprod. Biomed. Online 2019, 39, 777–783. [Google Scholar] [CrossRef]
- Chen, X.; Liu, P.; Sheng, Y.; Li, W.; Tang, R.; Ding, L.; Qin, Y.; Chen, Z.J. The impact of unicornuate uterus on perinatal outcomes after ivf/icsi cycles: A matched retrospective cohort study. J. Matern. Fetal Neonatal Med. 2019, 32, 2469–2474. [Google Scholar] [CrossRef]
- Cahen-Peretz, A.; Sheiner, E.; Friger, M.; Walfisch, A. The association between müllerian anomalies and perinatal outcome. J. Matern. Fetal Neonatal Med. 2019, 32, 51–57. [Google Scholar] [CrossRef]
- Prior, M.; Richardson, A.; Asif, S.; Polanski, L.; Parris-Larkin, M.; Chandler, J.; Fogg, L.; Jassal, P.; Thornton, J.G.; Raine-Fenning, N.J. Outcome of assisted reproduction in women with congenital uterine anomalies: A prospective observational study. Ultrasound Obstet. Gynecol. 2018, 51, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Pleş, L.; Alexandrescu, C.; Ionescu, C.A.; Arvătescu, C.A.; Vladareanu, S.; Moga, M.A. Three-dimensional scan of the uterine cavity of infertile women before assisted reproductive technology use. Medicine 2018, 97, e12764. [Google Scholar] [CrossRef]
- Mastrolia, S.A.; Baumfeld, Y.; Hershkovitz, R.; Loverro, G.; Di Naro, E.; Yohai, D.; Schwarzman, P.; Weintraub, A.Y. Bicornuate uterus is an independent risk factor for cervical os insufficiency: A retrospective population based cohort study. J. Matern. Fetal Neonatal Med. 2017, 30, 2705–2710. [Google Scholar] [CrossRef]
- Mastrolia, S.A.; Baumfeld, Y.; Hershkovitz, R.; Yohay, D.; Trojano, G.; Weintraub, A.Y. Independent association between uterine malformations and cervical insufficiency: A retrospective population-based cohort study. Arch. Gynecol. Obstet. 2018, 297, 919–926. [Google Scholar] [CrossRef]
- Chen, Y.; Nisenblat, V.; Yang, P.; Zhang, X.; Ma, C. Reproductive outcomes in women with unicornuate uterus undergoing in vitro fertilization: A nested case-control retrospective study. Reprod. Biol. Endocrinol. 2018, 16, 64. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, K.; Bulut, H.; Berkkanoglu, M.; Coetzee, K. Reproductive outcomes of ivf patients with unicornuate uteri. Reprod. Biomed. Online 2017, 34, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ouyang, Y.; Yi, Y.; Lin, G.; Lu, G.; Gong, F. Pregnancy outcomes of women with a congenital unicornuate uterus after ivf-embryo transfer. Reprod. Biomed. Online 2017, 35, 583–591. [Google Scholar] [CrossRef] [Green Version]
- Hiersch, L.; Yeoshoua, E.; Miremberg, H.; Krissi, H.; Aviram, A.; Yogev, Y.; Ashwal, E. The association between mullerian anomalies and short-term pregnancy outcome. J. Matern. Fetal Neonatal Med. 2016, 29, 2573–2578. [Google Scholar] [CrossRef]
- Takami, M.; Aoki, S.; Kurasawa, K.; Okuda, M.; Takahashi, T.; Hirahara, F. A classification of congenital uterine anomalies predicting pregnancy outcomes. Acta Obstet. Gynecol. Scand. 2014, 93, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.S.; Roman, A.S.; Stern, E.M.; Gerber, R.S.; Saltzman, D.H.; Rebarber, A. Type of congenital uterine anomaly and adverse pregnancy outcomes. J. Matern. Fetal Neonatal Med. 2014, 27, 949–953. [Google Scholar] [CrossRef]
- Jayaprakasan, K.; Chan, Y.Y.; Sur, S.; Deb, S.; Clewes, J.S.; Raine-Fenning, N.J. Prevalence of uterine anomalies and their impact on early pregnancy in women conceiving after assisted reproduction treatment. Ultrasound Obstet. Gynecol. 2011, 37, 727–732. [Google Scholar] [CrossRef]
- Hua, M.; Odibo, A.; Longman, R.; Roehl, K.A.; Macones, G.; Cahill, A. Congenital uterine anomalies and adverse pregnancy outcomes. Am. J. Obstet. Gynecol. 2011, 204, S334–S335. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhao, Y.Y.; Qiao, J. Obstetric outcome of women with uterine anomalies in china. Chin. Med. J. 2010, 123, 418–422. [Google Scholar]
- Tomaževič, T.; Ban-Frangež, H.; Virant-Klun, I.; Verdenik, I.; Požlep, B.; Vrtačnik-Bokal, E. Septate, subseptate and arcuate uterus decrease pregnancy and live birth rates in ivf/icsi. Reprod. Biomed. Online 2010, 21, 700–705. [Google Scholar] [CrossRef] [Green Version]
- Sugiura-Ogasawara, M.; Ozaki, Y.; Kitaori, T.; Kumagai, K.; Suzuki, S. Midline uterine defect size is correlated with miscarriage of euploid embryos in recurrent cases. Fertil. Steril. 2010, 93, 1983–1988. [Google Scholar] [CrossRef]
- Saravelos, S.H.; Cocksedge, K.A.; Li, T.C. The pattern of pregnancy loss in women with congenital uterine anomalies and recurrent miscarriage. Reprod. Biomed. Online 2010, 20, 416–422. [Google Scholar] [CrossRef] [Green Version]
- Liang, F.; Hu, W. Pregnancy complications and obstetric outcomes among women with congenital uterine malformations. Int. J. Gynecol. Obstet. 2010, 109, 159–160. [Google Scholar] [CrossRef]
- Ban-Frangez, H.; Tomazevic, T.; Virant-Klun, I.; Verdenik, I.; Ribic-Pucelj, M.; Bokal, E.V. The outcome of singleton pregnancies after ivf/icsi in women before and after hysteroscopic resection of a uterine septum compared to normal controls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 146, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Zlopasa, G.; Skrablin, S.; Kalafatić, D.; Banović, V.; Lesin, J. Uterine anomalies and pregnancy outcome following resectoscope metroplasty. Int. J. Gynaecol. Obstet. 2007, 98, 129–133. [Google Scholar] [CrossRef]
- Erez, O.; Dukler, D.; Novack, L.; Rozen, A.; Zolotnik, L.; Bashiri, A.; Koifman, A.; Mazor, M. Trial of labor and vaginal birth after cesarean section in patients with uterine müllerian anomalies: A population-based study. Am. J. Obstet. Gynecol. 2007, 196, 537.e1–537.e11. [Google Scholar] [CrossRef] [PubMed]
- Woelfer, B.; Salim, R.; Banerjee, S.; Elson, J.; Regan, L.; Jurkovic, D. Reproductive outcomes in women with congenital uterine anomalies detected by three-dimensional ultrasound screening. Obstet. Gynecol. 2001, 98, 1099–1103. [Google Scholar] [PubMed]
- Ravasia, D.J.; Brain, P.H.; Pollard, J.K. Incidence of uterine rupture among women with mullerian duct anomalies who attempt vaginal birth after cesarean delivery. Am. J. Obstet. Gynecol. 1999, 181, 877–881. [Google Scholar] [CrossRef]
- Cooney, M.J.; Benson, C.B.; Doubilet, P.M. Outcome of pregnancies in women with uterine duplication anomalies. J. Clin. Ultrasound 1998, 26, 3–6. [Google Scholar] [CrossRef]
- Acién, P. Reproductive performance of women with uterine malformations. Hum. Reprod. 1993, 8, 122–126. [Google Scholar] [CrossRef]
- Shuiqing, M.; Xuming, B.; Jinghe, L. Pregnancy and its outcome in women with malformed uterus. Chin. Med. Sci. J. 2002, 17, 242–245. [Google Scholar]
- Zupi, E.; Solima, E.; Marconi, D.; Valli, E.; Romanini, C. Uterine anomalies prevalence and reproductive outcome in women undergoing diagnostic hysteroscopy. Gynaecol. Endosc. 1996, 5, 147–150. [Google Scholar]
- Maneschi, F.; Zupi, E.; Marconi, D.; Valli, E.; Romanini, C.; Mancuso, S. Hysteroscopically detected asymptomatic mullerian anomalies: Prevalence and reproductive implications. J. Reprod. Med. Obstet. Gynecol. 1995, 40, 684–688. [Google Scholar]
- Ben-Rafael, Z.; Seidman, D.S.; Recabi, K.; Bider, D.; Mashiach, S. Uterine anomalies: A retrospective, matched-control study. J. Reprod. Med. Obstet. Gynecol. 1991, 36, 723–727. [Google Scholar]
- Sorensen, S.S.; Trauelsen, A.G.H. Obstetric implications of minor mullerian anomalies in oligomenorrheic women. Am. J. Obstet. Gynecol. 1987, 156, 1112–1118. [Google Scholar] [CrossRef]
- Forde, P.; O’Driscoll, D.; Murphy, H. Pregnancy associated with uterine abnormality. Ir. Med. J. 1978, 71, 164–165. [Google Scholar]
- Simón, C.; Moreno, C.; Remohí, J.; Pellicer, A. Cytokines and embryo implantation. J. Reprod. Immunol. 1998, 39, 117–131. [Google Scholar] [CrossRef]
- Candiani, G.B.; Fedele, L.; Zamberletti, D.; De Virgiliis, D.; Carinelli, S. Endometrial patterns in malformed uteri. Acta Eur. Fertil. 1983, 14, 311–318. [Google Scholar] [PubMed]
- Fedele, L.; Bianchi, S.; Marchini, M.; Franchi, D.; Tozzi, L.; Dorta, M. Ultrastructural aspects of endometrium in infertile women with septate uterus. Fertil. Steril. 1996, 65, 750–752. [Google Scholar] [CrossRef]
- Dabirashrafi, H.; Bahadori, M.; Mohammad, K.; Alavi, M.; Moghadami-Tabrizi, N.; Zandinejad, K.; Ghafari, V. Septate uterus: New idea on the histologic features of the septum in this abnormal uterus. Am. J. Obstet. Gynecol. 1995, 172, 105–107. [Google Scholar] [CrossRef]
- Chan, Y.Y.; Jayaprakasan, K.; Zamora, J.; Thornton, J.G.; Raine-Fenning, N.; Coomarasamy, A. The prevalence of congenital uterine anomalies in unselected and high-risk populations: A systematic review. Hum. Reprod. Update 2011, 17, 761–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saravelos, S.H.; Cocksedge, K.A.; Li, T.C. Prevalence and diagnosis of congenital uterine anomalies in women with reproductive failure: A critical appraisal. Hum. Reprod. Update 2008, 14, 415–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcal, L.; Nothaft, M.A.; Coelho, F.; Volpato, R.; Iyer, R. Mullerian duct anomalies: Mr imaging. Abdom. Imaging 2011, 36, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Grimbizis, G.F.; Di Spiezio Sardo, A.; Saravelos, S.H.; Gordts, S.; Exacoustos, C.; Van Schoubroeck, D.; Bermejo, C.; Amso, N.N.; Nargund, G.; Timmerman, D.; et al. The thessaloniki eshre/esge consensus on diagnosis of female genital anomalies. Hum. Reprod. 2016, 31, 2–7. [Google Scholar] [CrossRef]
- Valle, R.F.; Ekpo, G.E. Hysteroscopic metroplasty for the septate uterus: Review and meta-analysis. J. Minim. Invasive Gynecol. 2013, 20, 22–42. [Google Scholar] [CrossRef]
- Kowalik, C.R.; Goddijn, M.; Emanuel, M.H.; Bongers, M.Y.; Spinder, T.; de Kruif, J.H.; Mol, B.W.; Heineman, M.J. Metroplasty versus expectant management for women with recurrent miscarriage and a septate uterus. Cochrane Database Syst. Rev. 2011, 6, Cd008576. [Google Scholar] [CrossRef]
- Rikken, J.F.; Kowalik, C.R.; Emanuel, M.H.; Mol, B.W.; Van der Veen, F.; van Wely, M.; Goddijn, M. Septum resection for women of reproductive age with a septate uterus. Cochrane Database Syst. Rev. 2017, 1, Cd008576. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.A.; Saravelos, S.H.; Li, T.C.; Jayaprakasan, K. Reproductive implications and management of congenital uterine anomalies: Scientific impact paper no. 62 november 2019. BJORG 2020, 127, e1–e13. [Google Scholar] [CrossRef]
- Esteban Manchado, B.; Lopez-Yarto, M.; Fernandez-Parra, J.; Rodriguez-Oliver, A.; Gonzalez-Paredes, A.; Laganà, A.S.; Garzon, S.; Haimovich, S. Office hysteroscopic metroplasty with diode laser for septate uterus: A multicenter cohort study. Minim. Invasive Ther. Allied Technol. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bosteels, J.; Weyers, S.; Kasius, J.; Broekmans, F.J.; Mol, B.W.; D’Hooghe, T.M. Anti-adhesion therapy following operative hysteroscopy for treatment of female subfertility. Cochrane Database Syst. Rev. 2015, 11, Cd011110. [Google Scholar] [CrossRef] [PubMed]
- Nappi, L.; Falagario, M.; Angioni, S.; De Feo, V.; Bollino, M.; Sorrentino, F. The use of hysteroscopic metroplasty with diode laser to increase endometrial volume in women with septate uterus: Preliminary results. Gynecol. Surg. 2021, 18, 11. [Google Scholar] [CrossRef]
- Nappi, L.; Sorrentino, F.; Angioni, S.; Pontis, A.; Greco, P. The use of laser in hysteroscopic surgery. Minerva Ginecol. 2016, 68, 722–726. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).