
Clinical Diagnostic Imaging Study of Osteoradionecrosis of the Jaw: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. MDCT and CBCT
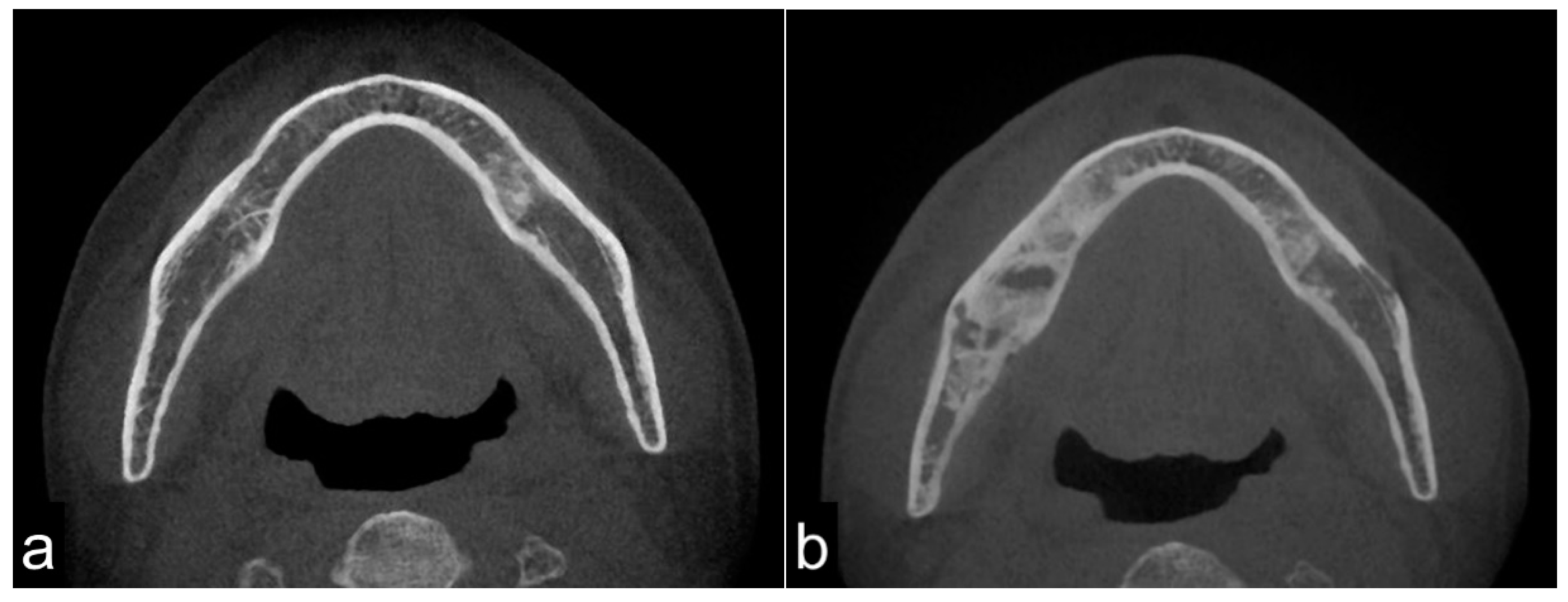
- Sclerosis of the affected bone
- Resorption of the affected bone
- A periosteum reaction of the affected bone
2.2. MRI
2.3. FDG-PET/CT
2.4. Bone Scintigraphy and SPECT
2.5. Treatment
3. Results
3.1. Clinical Findings
3.2. CT Findings
3.3. MRI Findings
3.4. PET/CT Findings
3.5. Bone Scintigraphy and SPECT Findings
3.6. Treatment Outcome
4. Discussion
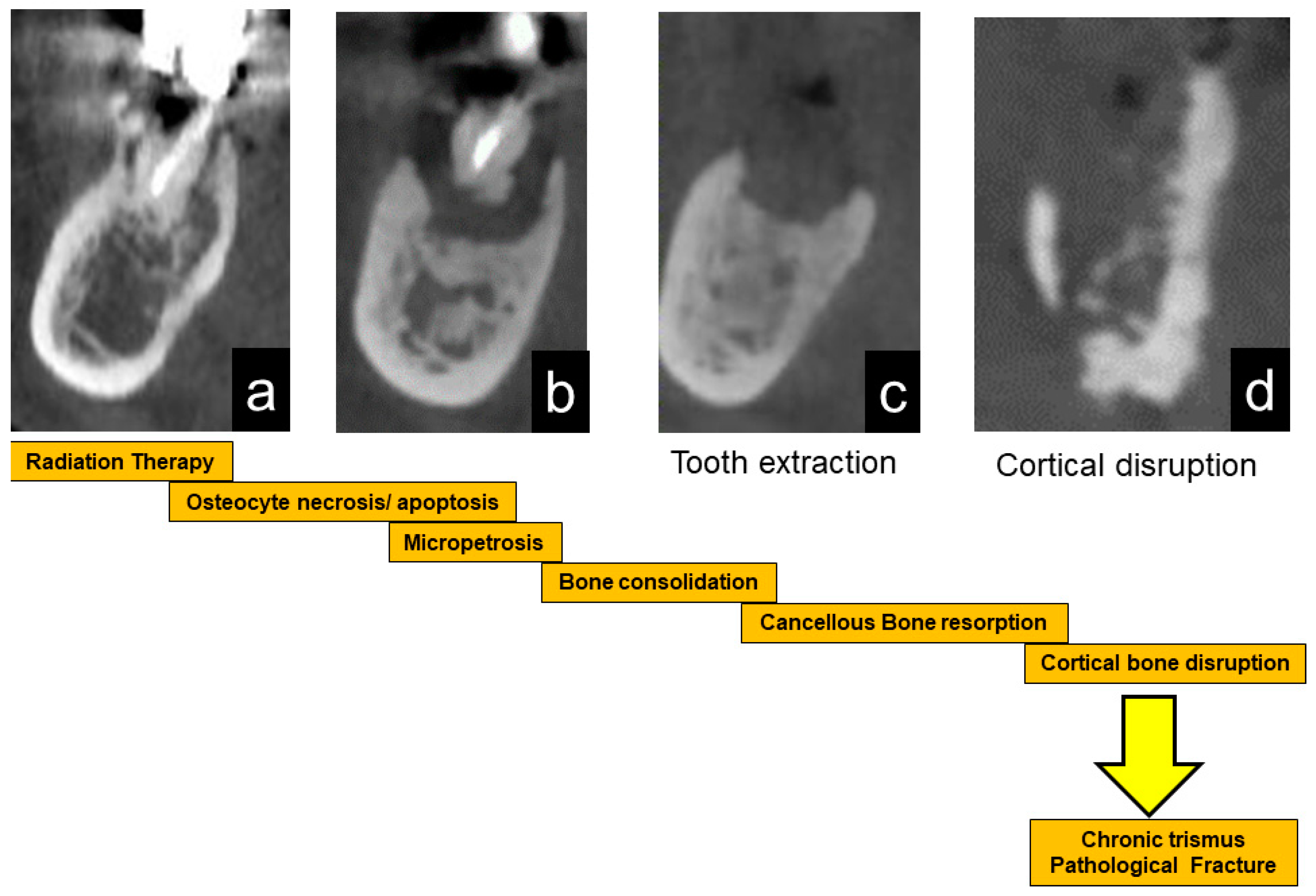
- Osteoconsolidation of cancellous bone due to irradiation with hypovascularity with reduced bone cell viabilities and bone marrow changes to fibrous or scar tissue. Bone and bone marrow are chronic inflammatory conditions.
- Progression of sclerosed cancellous bone inflammation and/or bone resorption.
- Bone invasion, such as tooth extraction, induces acute inflammation (acute osteomyelitis and ORN) and continuous bone resorption.
- Through cortical disruption or extensive bone destruction with refractory inflammation, the hard, fragile jawbone due to bone consolidation develops pathological fracture, intra-/extra-oral fistula, and soft tissue scars with trismus, which is the terminal stage of ORN, with the progression of local inflammatory bone resorption.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jacobson, A.S.; Buchbinder, D.; Hu, K.; Urken, M.L. Paradigm shifts in the management of osteoradionecrosis of the mandible. Oral Oncol. 2010, 46, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Osteoradionecrosis: A new concept of its pathophysiology. J. Oral Maxillofac. Surg. 1983, 41, 283–288. [Google Scholar] [CrossRef]
- Delanian, S.; Lefaix, J.L. Complete healing of severe osteoradionecrosis with treatment combining pentoxifylline, tocopherol and clodronate. Br. J. Radiol. 2002, 75, 467–469. [Google Scholar] [CrossRef]
- Delanian, S.; Lefaix, J.L. The radiation-induced fibroatrophic process: Therapeutic perspective via the antioxidant pathway. Radiother. Oncol. 2004, 73, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Delanian, S.; Depondt, J.; Lefaix, J.L. Major healing of refractory mandible osteoradionecrosis after treatment combining pentoxifylline and tocopherol: A phase II trial. Head Neck 2005, 27, 114–123. [Google Scholar] [CrossRef]
- Kolokythas, A.; Rasmussen, J.T.; Reardon, J.; Feng, C. Management of osteoradionecrosis of the jaws with pentoxifylline-tocopherol: A systematic review of the literature and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 173–180. [Google Scholar] [CrossRef]
- Zhang, Z.; Xiao, W.; Jia, J.; Chen, Y.; Zong, C.; Zhao, L.; Tian, L. The effect of combined application of pentoxifylline and vitamin E for the treatment of osteoradionecrosis of the jaws: A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 207–214. [Google Scholar] [CrossRef]
- Nabil, S.; Samman, N. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: A systematic review. Int. J. Oral Maxillofac. Surg. 2011, 40, 229–243. [Google Scholar] [CrossRef]
- Thorn, J.J.; Hansen, H.S.; Specht, L.; Bastholt, L. Osteoradionecrosis of the jaws: Clinical characteristics and relation to the field of irradiation. J. Oral Maxillofac. Surg. 2000, 58, 1088–1093, discussion 1093. [Google Scholar] [CrossRef]
- Marx, R.E.; Tursun, R. Suppurative osteomyelitis, bisphosphonate induced osteonecrosis, osteoradionecrosis: A blinded histopathologic comparison and its implications for the mechanism of each disease. Int. J. Oral Maxillofac. Surg. 2012, 41, 283–289. [Google Scholar] [CrossRef]
- De Antoni, C.C.; Matsumoto, M.A.; Silva, A.A.D.; Curi, M.M.; Santiago Júnior, J.F.; Sassi, L.M.; Cardoso, C.L. Medication-related osteonecrosis of the jaw, osteoradionecrosis, and osteomyelitis: A comparative histopathological study. Braz. Oral Res. 2018, 32, e23. [Google Scholar] [CrossRef] [Green Version]
- Santiago Restrepo, C.; Giménez, C.R.; McCarthy, K. Imaging of osteomyelitis and musculoskeletal soft tissue infections: Current concepts. Rheum. Dis. Clin. N. Am. 2003, 29, 89–109. [Google Scholar] [CrossRef]
- Kaneda, T.; Minami, M.; Ozawa, K.; Akimoto, Y.; Utsunomiya, T.; Yamamoto, H.; Suzuki, H.; Sasaki, Y. Magnetic resonance imaging of osteomyelitis in the mandible. Comparative study with other radiologic modalities. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1995, 79, 634–640. [Google Scholar] [CrossRef]
- Reinert, S.; Widlitzek, H.; Venderink, D.J. The value of magnetic resonance imaging in the diagnosis of mandibular osteomyelitis. Br. J. Oral Maxillofac. Surg. 1999, 37, 459–463. [Google Scholar] [CrossRef]
- Madrid, C.; Abarca, M.; Bouferrache, K. Osteoradionecrosis: An update. Oral Oncol. 2010, 46, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Nadella, K.R.; Kodali, R.M.; Guttikonda, L.K.; Jonnalagadda, A. Osteoradionecrosis of the jaws: Clinico-therapeutic management: A literature review and update. J. Maxillofac. Oral Surg. 2015, 14, 891–901. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Liu, Z.; Tian, Z.; Dai, T.; Qiu, W.; Zhang, Z. Retrospective analysis of osteoradionecrosis of the mandible: Proposing a novel clinical classification and staging system. Int. J. Oral Maxillofac. Surg. 2015, 44, 1547–1557. [Google Scholar] [CrossRef]
- Chronopoulos, A.; Zarra, T.; Ehrenfeld, M.; Otto, S. Osteoradionecrosis of the jaws: Definition, epidemiology, staging and clinical and radiological findings. A concise review. Int. Dent. J. 2018, 68, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Støre, G.; Larheim, T.A. Mandibular osteoradionecrosis: A comparison of computed tomography with panoramic radiography. Dentomaxillofac. Radiol. 1999, 28, 295–300. [Google Scholar] [CrossRef]
- Støre, G.; Boysen, M. Mandibular osteoradionecrosis: Clinical behaviour and diagnostic aspects. Otolaryngol. Allied Sci. 2000, 25, 378–384. [Google Scholar] [CrossRef]
- Ariji, Y.; Izumi, M.; Gotoh, M.; Naitoh, M.; Katoh, M.; Kuroiwa, Y.; Obayashi, N.; Kurita, K.; Shimozato, K.; Ariji, E. MRI features of mandibular osteomyelitis: Practical criteria based on an association with conventional radiography features and clinical classification. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Alhilali, L.; Reynolds, A.R.; Fakhran, S. Osteoradionecrosis after radiation therapy for head and neck cancer: Differentiation from recurrent disease with CT and PET/CT imaging. AJNR Am. J. Neuroradiol. 2014, 35, 1405–1411. [Google Scholar] [CrossRef] [Green Version]
- Regaud, C. Sur la necrose des os attenté par un processus cancereux et traites par les radiaions. Compt. Rend. Soc. Biol. 1922, 87, 427. [Google Scholar]
- Eiving, J. Radiation osteitis. Acta Radiol. 1926, 6, 399–412. [Google Scholar] [CrossRef] [Green Version]
- Wendt, T.G.; Grabenbauer, G.G.; Rödel, C.M.; Thiel, H.J.; Aydin, H.; Rohloff, R.; Wustrow, T.P.; Iro, H.; Popella, C.; Schalhorn, A. Simultaneous radiochemotherapy versus radiotherapy alone in advanced head and neck cancer: A randomized multicenter study. J. Clin. Oncol. 1998, 16, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J.; MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Oikawa, H.; Nakamura, R.; Nakasato, T.; Nishimura, K.; Sato, H.; Ehara, S. Radiotherapy and concomitant intra-arterial docetaxel combined with systemic 5-fluorouracil and cisplatin for oropharyngeal cancer: A preliminary report--improvement of locoregional control of oropharyngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 338–342. [Google Scholar] [CrossRef]
- Robbins, K.T.; Kumar, P.; Harris, J.; McCulloch, T.; Cmelak, A.; Sofferman, R.; Levine, P.; Weisman, R.; Wilson, W.; Weymuller, E.; et al. Supradose intra-arterial cisplatin and concurrent radiation therapy for the treatment of stage IV head and neck squamous cell carcinoma is feasible and efficacious in a multi-institutional setting: Results of Radiation Therapy Oncology Group Trial 9615. J. Clin. Oncol. 2005, 23, 1447–1454. [Google Scholar] [CrossRef]
- Quon, H.; Vapiwala, N.; Forastiere, A.; Kennedy, E.B.; Adelstein, D.J.; Boykin, H.; Califano, J.A.; Holsinger, F.C.; Nussenbaum, B.; Rosenthal, D.I.; et al. Radiation therapy for oropharyngeal squamous cell carcinoma: American society of clinical oncology endorsement of the American Society for Radiation Oncology evidence-based clinical practice guideline. J. Clin. Oncol. 2017, 35, 4078–4090. [Google Scholar] [CrossRef]
- Kuhnt, T.; Becker, A.; Bloching, M.; Schubert, J.; Klautke, G.; Fietkau, R.; Dunst, J. Phase II trial of a simultaneous radiochemotherapy with cisplatinum and paclitaxel in combination with hyperfractionated-accelerated radiotherapy in locally advanced head and neck tumors. Med. Oncol. 2006, 23, 325–333. [Google Scholar] [CrossRef]
- Hehr, T.; Classen, J.; Welz, S.; Ganswindt, U.; Scheithauer, H.; Koitschev, A.; Bamberg, M.; Budach, W. Hyperfractionated, accelerated chemoradiation with concurrent mitomycin-C and cisplatin in locally advanced head and neck cancer, a phase I/II study. Radiother. Oncol. 2006, 80, 33–38. [Google Scholar] [CrossRef]
- Reuther, T.; Schuster, T.; Mende, U.; Kübler, A. Osteoradionecrosis of the jaws as a side effect of radiotherapy of head and neck tumor patients--a report of a thirty year retrospective review. Int. J. Oral Maxillofac. Surg. 2003, 32, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Sugimoto, M.; Kotoura, Y.; Sasai, K.; Oka, M.; Yamamuro, T. Long-term changes in the haversian systems following high-dose irradiation. An ultrastructural and quantitative histomorphological study. J. Bone Joint Surg. Am. 1994, 76, 722–738. [Google Scholar] [CrossRef] [PubMed]
- Busse, B.; Djonic, D.; Milovanovic, P.; Hahn, M.; Püschel, K.; Ritchie, R.O.; Djuric, M.; Amling, M. Decrease in the Osteocyte Lacunar Density Accompanied by occlusion reveals failure and delay of remodeling in aged human bone. Aging Cell 2010, 9, 1065–1075. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, I.; Ishikawa, A.; Morimoto, Y.; Takahashi, T. Potential risk of asymptomatic osteomyelitis around mandibular third molar tooth for aged people: A computed tomography and histopathologic study. PLoS ONE 2013, 8, e73897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost, H.M. Micropetrosis. J. Bone Joint Surg. Am. 1960, 42, 144–150. [Google Scholar] [CrossRef]
- Ogura, I.; Sasaki, Y.; Sue, M.; Oda, T.; Kameta, A.; Hayama, K. Tc-99 m hydroxymethylene diphosphonate scintigraphy, computed tomography, and magnetic resonance imaging of osteonecrosis in the mandible: Osteoradionecrosis versus medication-related osteonecrosis of the jaw. Imaging Sci. Dent. 2019, 49, 53–58. [Google Scholar] [CrossRef]
- Obinata, K.; Shirai, S.; Ito, H.; Nakamura, M.; Carrozzo, M.; Macleod, I.; Carr, A.; Yamazaki, Y.; Tei, K. Image findings of bisphosphonate related osteonecrosis of jaws comparing with osteoradionecrosis. Dentomaxillofac. Radiol. 2017, 46, 20160281. [Google Scholar] [CrossRef]
- Chong, J.; Hinckley, L.K.; Ginsberg, L.E. Masticator space abnormalities associated with mandibular osteoradionecrosis: MR and CT findings in five patients. AJNR Am. J. Neuroradiol. 2000, 21, 175–178. [Google Scholar]
- Hakim, S.G.; Bruecker, C.W.R.; Jacobsen, H.C.; Hermes, D.; Lauer, I.; Eckerle, S.; Froehlich, A.; Sieg, P. The value of FDG-PET and bone scintigraphy with SPECT in the primary diagnosis and follow-up of patients with chronic osteomyelitis of the mandible. Int. J. Oral Maxillofac. Surg. 2006, 35, 809–816. [Google Scholar] [CrossRef]
- Meerwein, C.M.; Nakadate, M.; Stolzmann, P.; Vital, D.; Morand, G.B.; Zweifel, D.F.; Huber, G.F.; Huellner, M.W. Contrast-Enhanced 18 F-FDG-PET/CT for Differentiating Tumor and Radionecrosis in Head and Neck Cancer: Our Experience in 37 Patients. Clin. Otolaryngol. 2018, 43, 1594–1599. [Google Scholar] [CrossRef]
- Toshima, H.; Ogura, I. Assessment of inflammatory jaw pathologies using bone SPECT/CT maximum standardized uptake value. Dentomaxillofac. Radiol. 2020, 49, 20200043. [Google Scholar] [CrossRef]
- Beech, N.M.; Porceddu, S.; Batstone, M.D. Radiotherapy-associated dental extractions and osteoradionecrosis. Head Neck 2017, 39, 128–132. [Google Scholar] [CrossRef]
- Chang, D.T.; Sandow, P.R.; Morris, C.G.; Hollander, R.; Scarborough, L.; Amdur, R.J.; Mendenhall, W.M. Do pre-irradiation dental extractions reduce the risk of osteoradionecrosis of the mandible? Head Neck 2007, 29, 528–536. [Google Scholar] [CrossRef]
- Smith, R.M.; Hassan, A.; Robertson, C.E. Numb Chin Syndrome. Curr. Pain Headache Rep. 2015, 19, 44. [Google Scholar] [CrossRef]
- Leonzio, F.; Massimo, A.; Michele, S.; Francesco, B.; Selene, B.; Amerigo, G. Numb chin syndrome: A reflection of malignancy or a harbinger of MRONJ? A multicenter experience. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 389–394. [Google Scholar]
- Willaert, R.; Nevens, D.; Laenen, A.; Batstone, M.; Politis, C.; Nuyts, S. Does intensity-modulated radiation therapy lower the risk of osteoradionecrosis of the jaw? A long-term comparative analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, F.J.; Phan, T.T.T.; van den Hoogen, F.J.A.; Kaanders, J.H.A.M.; Merkx, M.A.W. The efficacy of hyperbaric oxygen therapy related to the clinical stage of osteoradionecrosis of the mandible. Int. J. Oral Maxillofac. Surg. 2017, 46, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Sultan, A.; Hanna, G.J.; Margalit, D.N.; Chau, N.; Goguen, L.A.; Marty, F.M.; Rabinowits, G.; Schoenfeld, J.D.; Sonis, S.T.; Thomas, T.; et al. The use of hyperbaric oxygen for the prevention and management of osteoradionecrosis of the jaw: A Dana-Farber/Brigham and Women’s Cancer Center Multidisciplinary Guideline. Oncologist 2017, 22, 343–350. [Google Scholar] [CrossRef] [Green Version]
- Annane, D.; Depondt, J.; Aubert, P.; Villart, M.; Géhanno, P.; Gajdos, P.; Chevret, S. Hyperbaric oxygen therapy for radionecrosis of the jaw: A randomized, placebo-controlled, double-blind trial from the ORN96 study group. J. Clin. Oncol. 2004, 22, 4893–4900. [Google Scholar] [CrossRef] [PubMed]
- van Merkesteyn, J.P.; Balm, A.J.; Bakker, D.J.; Borgmeyer-Hoelen, A.M. Hyperbaric Oxygen Treatment of Osteoradionecrosis of the fracture. Report of a case. Oral Surg. Oral Med. Oral Pathol. 1994, 77, 461–464. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Numbers of Patients (%) | |
|---|---|---|
| Gender | Male | 36 (80%) |
| Female | 9 (20%) | |
| Age Mean (range) | 68.6 (39–85) years | |
| Maxilla/mandible | 9 (18.8%)/39 (81.2%) | |
| Primary tumor | Oropharyngeal | 19 (42.2%) |
| Tongue | 11 (24.4%) | |
| Gingival | 4 (8.9%) | |
| Parotid gland | 2 (4.4%) | |
| Hard palate | 2 (4.4%) | |
| Buccal mucosa | 2 (4.4%) | |
| floor of the mouth | 2 (4.4%) | |
| Nasal cavity | 1 (2.2%) | |
| Maxillary sinus | 1 (2.2%) | |
| Histology | Squamous cell carcinoma | 37 (82.2%) |
| Adenoid cystic carcinoma | 1 (2.2%) | |
| Undifferentiated carcinoma | 1 (2.2%) | |
| Malignant lymphoma | 1 (2.2%) | |
| Lymphoepithelial tumor | 1 (2.2%) | |
| Plasmacytoma | 1 (2.2%) | |
| No data | 3 (6.7%) | |
| Mean radiation dose (range) | 64.3 (40–95) Gy | |
| Chemotherapy | (+) | 37 (82.2%) |
| including 13 (28.9%) patients treated with super-selective arterial chemotherapy | ||
| (−) | 6 (13.3%) | |
| No data | 2 (4.4%) | |
| Tumor stage | Stage I | 2 (4.4%) |
| Stage II | 1 (2.2%) | |
| Stage III | 4 (8.9%) | |
| Stage IV | 26 (57.8%) | |
| Other | 3 (6.7%) | |
| No data | 9 (20.0%) | |
| Initial events of osteoradionecrosis | Local bone exposure | 19 (39.6%) |
| Periodontal infection | 14 (29.2%) | |
| Tooth extraction | 9 (18.8%) | |
| Dental implant placement | 1 (2.1%) | |
| Bone surgery | 1 (2.1%) | |
| Unknown cause | 4 (8.3%) |
| ORN Stage | Number of Patients (%) |
|---|---|
| Stage 0 | n = 4 (8.3%) |
| B0 S0: No evident signs or only osteolytic images on radiography; however, the patient suffers from typical ORN-related symptoms (bone exposure or pain). | 100% |
| Stage I | n = 15 (31.3%) → 13 (27.1%) |
| B1 S0: The maximum diameter of the lesion on radiography is <2 cm, and there is no mucosa or skin defect. | n = 3 (6.3%) |
| B1 S1: The maximum diameter of the lesion on radiography is <2 cm, and there is an intraoral mucosa defect or external skin fistula alone. | n = 12(25.0%) → 10 (20.8%) |
| B1 S2: The maximum diameter of the lesion on radiography is <2 cm, and there is a through-and-through defect. | n = 0 (0%) |
| Stage II | n = 25 (52.1%) |
| B2 S0: The maximum diameter of the lesion on radiography is >2 cm, and there is no mucosa or skin defect. | n = 2 (4.2%) |
| B2 S1: The maximum diameter of the lesion on radiography is >2 cm, and there is an intraoral mucosa defect or external skin fistula alone. | n = 20 (41.7%) |
| B2 S2: The maximum diameter of the lesion on radiography is >2 cm, and there is a through-and-through defect. | n = 3 (6.3%) |
| Stage III | n = 4 (8.3%) → 6 (12.5%) |
| B3 S0: A pathological fracture is identified on radiography, and there is no mucosa or skin defect. | n = 1 (2.1%) |
| B3 S1: A pathological fracture is identified on radiography, and there is an intraoral mucosa defect or external skin fistula alone. | n = 0 (0%) → 2 (4.2%) |
| B3 S2: A pathological fracture is identified on radiography, and there is a through-and-through defect. | n = 3 (6.3%) |
| ORN Stage | Mean Duration ± Standard Deviation (Months) |
|---|---|
| Stage 0 (n = 4) | 90 ± 25.8 |
| Stage I (n = 15) | 40.1 ± 44.0 |
| Stage II (n = 25) | 64.8 ± 42.9 |
| Stage III (n = 4) | 14 ± 16.7 |
| Overall (n = 48) | 54.9 ± 44.1 |
| ORN Stage | Number of Patients (%) |
|---|---|
| Stage 0 | 1/4 (25%) |
| Stage I | 2/13 (15%) |
| Stage II | 11/25 (44%) |
| Stage III | 5/6 (83%) |
| Overall | 19/48 (39.6%) |
| Modality | Findings | Number of Patients (%) | |
|---|---|---|---|
| CT | Bone mineral condition | No bone resorption | n = 2 (4.2%) |
| Cancellous homogeneous Bone sclerosis | n = 10 (20.8%) | ||
| Cancellous heterogeneous Bone sclerosis | n = 30 (62.5%) | ||
| Bone resorption | n = 6 (12.5%) | ||
| Periosteum reaction | (+) n = 4 (8.3%) | ||
| (−) n = 44 (91.7%) | |||
| MRI | Bone marrow viability | T1 hypo-intensity | n = 42 (100%) |
| T2 homogeneous intensity | n = 30 (71.4%) | ||
| T2 heterogeneous intensity | n = 11 (26.2%) | ||
| T2 hypo-intensity | n = 1 (2.4%) | ||
| PET/CT | Glucose metabolic activity | Active | (+) n = 30 (85.7%) |
| mean SUVmax = 7.69 (n = 14) | |||
| Non-active | (−) n = 5 (14.3%) | ||
| Bone scintigraphy/SPECT | Bone metabolic activity | Active | (+) n = 17 (94.4%) |
| Non-active | (−) n = 1 (5.6%) |
| Treatment Outcome | Number of Patients (%) |
|---|---|
| Resolved | n = 8 (16.7%) |
| Improved | n = 22 (45.8%) |
| Stable | n = 15 (31.3%) |
| Progressed | n = 3 (6.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyamoto, I.; Tanaka, R.; Kogi, S.; Yamaya, G.; Kawai, T.; Ohashi, Y.; Takahashi, N.; Izumisawa, M.; Yamada, H. Clinical Diagnostic Imaging Study of Osteoradionecrosis of the Jaw: A Retrospective Study. J. Clin. Med. 2021, 10, 4704. https://doi.org/10.3390/jcm10204704
Miyamoto I, Tanaka R, Kogi S, Yamaya G, Kawai T, Ohashi Y, Takahashi N, Izumisawa M, Yamada H. Clinical Diagnostic Imaging Study of Osteoradionecrosis of the Jaw: A Retrospective Study. Journal of Clinical Medicine. 2021; 10(20):4704. https://doi.org/10.3390/jcm10204704
Chicago/Turabian StyleMiyamoto, Ikuya, Ryoichi Tanaka, Shintaro Kogi, Genki Yamaya, Tadashi Kawai, Yu Ohashi, Noriaki Takahashi, Mitsuru Izumisawa, and Hiroyuki Yamada. 2021. "Clinical Diagnostic Imaging Study of Osteoradionecrosis of the Jaw: A Retrospective Study" Journal of Clinical Medicine 10, no. 20: 4704. https://doi.org/10.3390/jcm10204704
APA StyleMiyamoto, I., Tanaka, R., Kogi, S., Yamaya, G., Kawai, T., Ohashi, Y., Takahashi, N., Izumisawa, M., & Yamada, H. (2021). Clinical Diagnostic Imaging Study of Osteoradionecrosis of the Jaw: A Retrospective Study. Journal of Clinical Medicine, 10(20), 4704. https://doi.org/10.3390/jcm10204704