
Complex Rearrangement of the Entire Retinal Posterior Pole in Patients with Relapsing Remitting Multiple Sclerosis

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic and Clinical Variables
3.2. OCT Variables
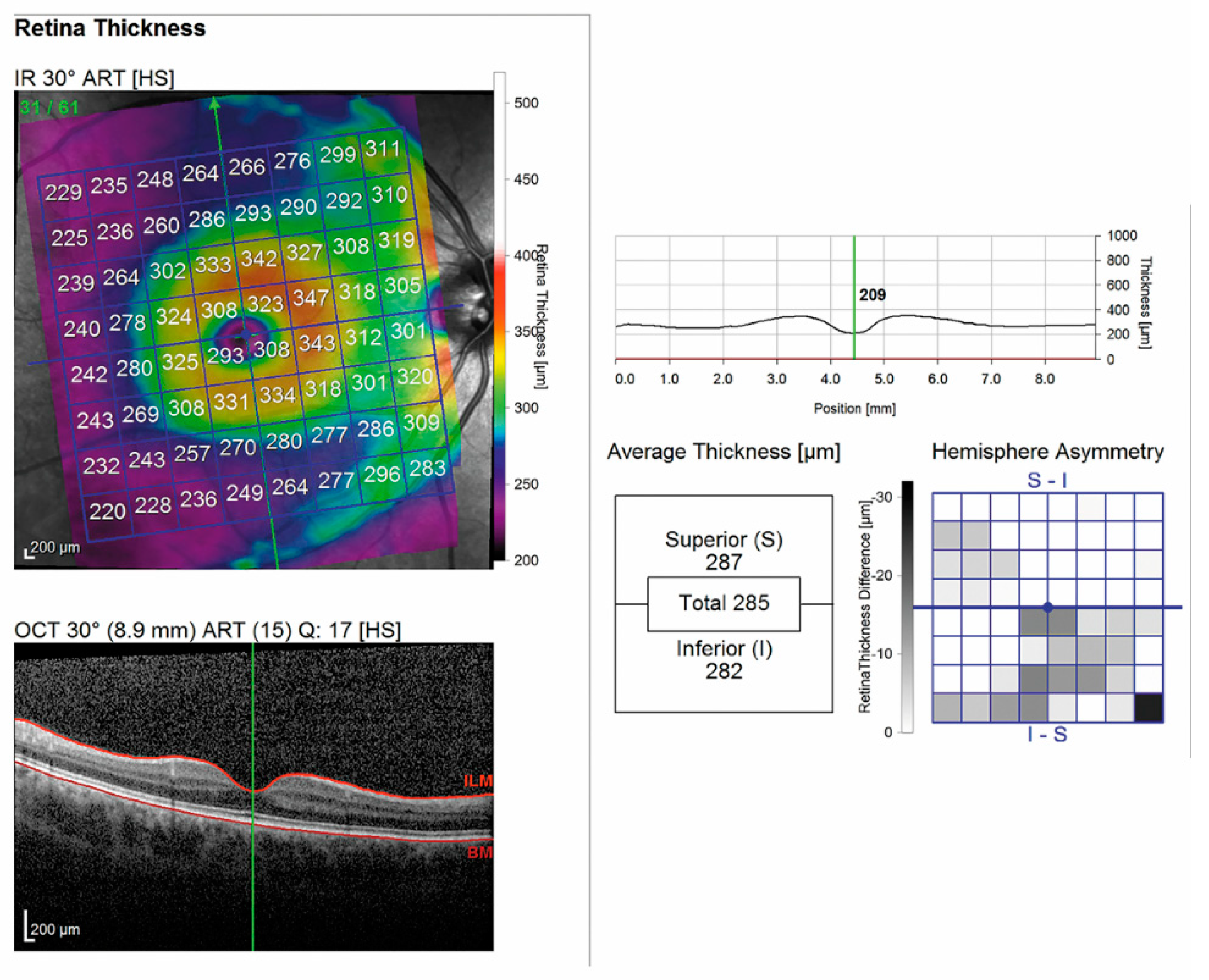
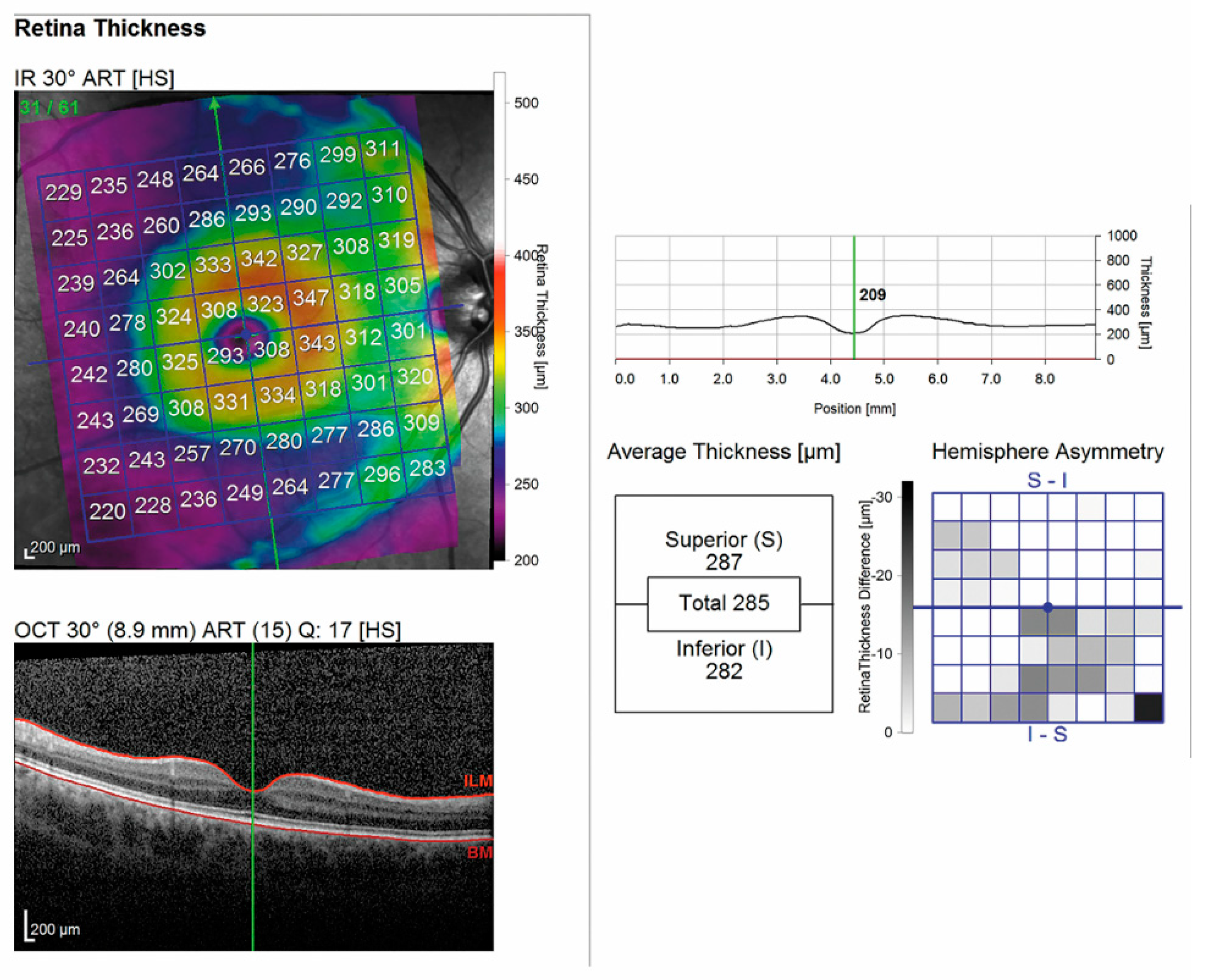
3.2.1. Mean Thickness of the Retinal Posterior Pole by Layers
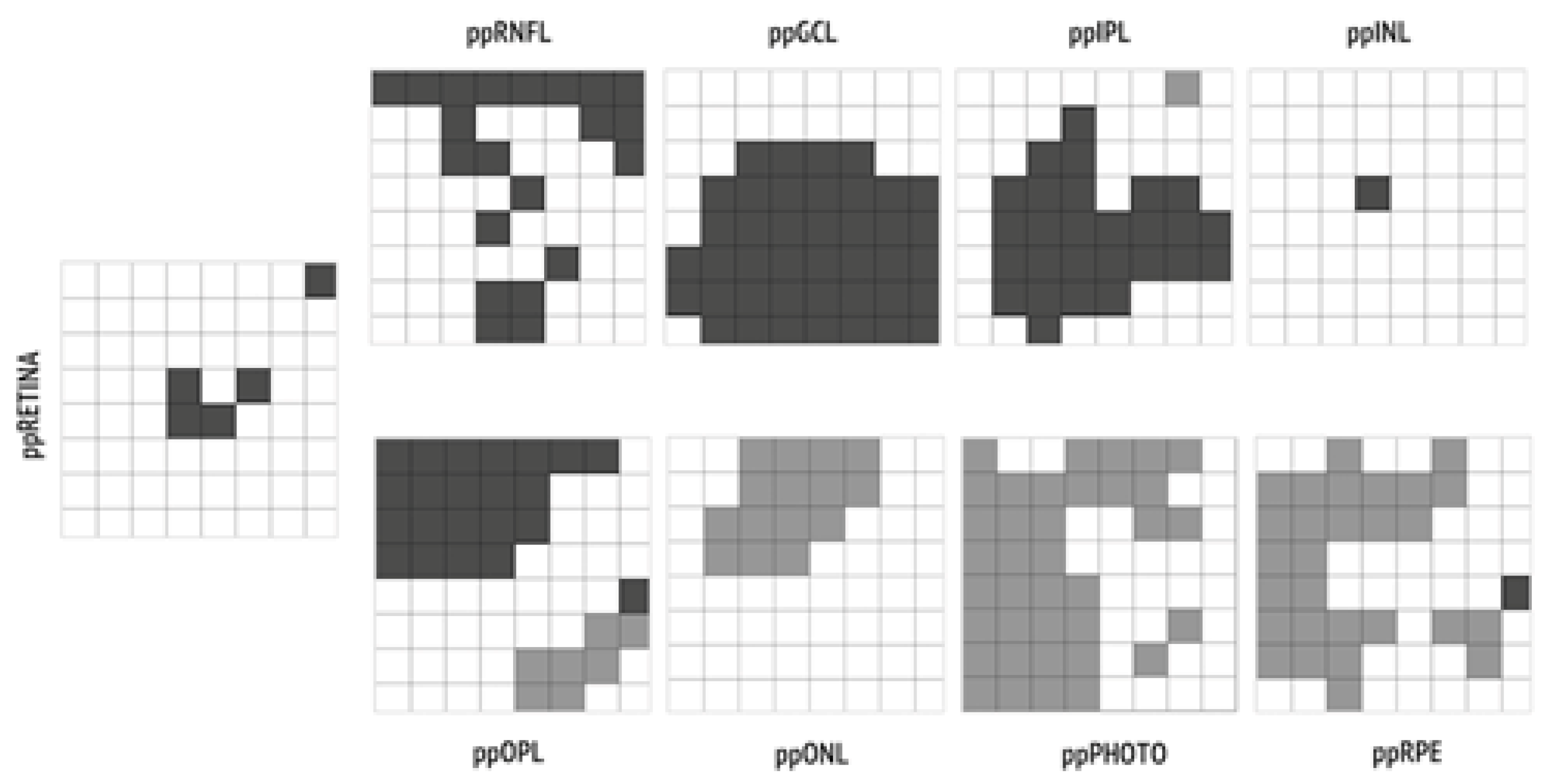
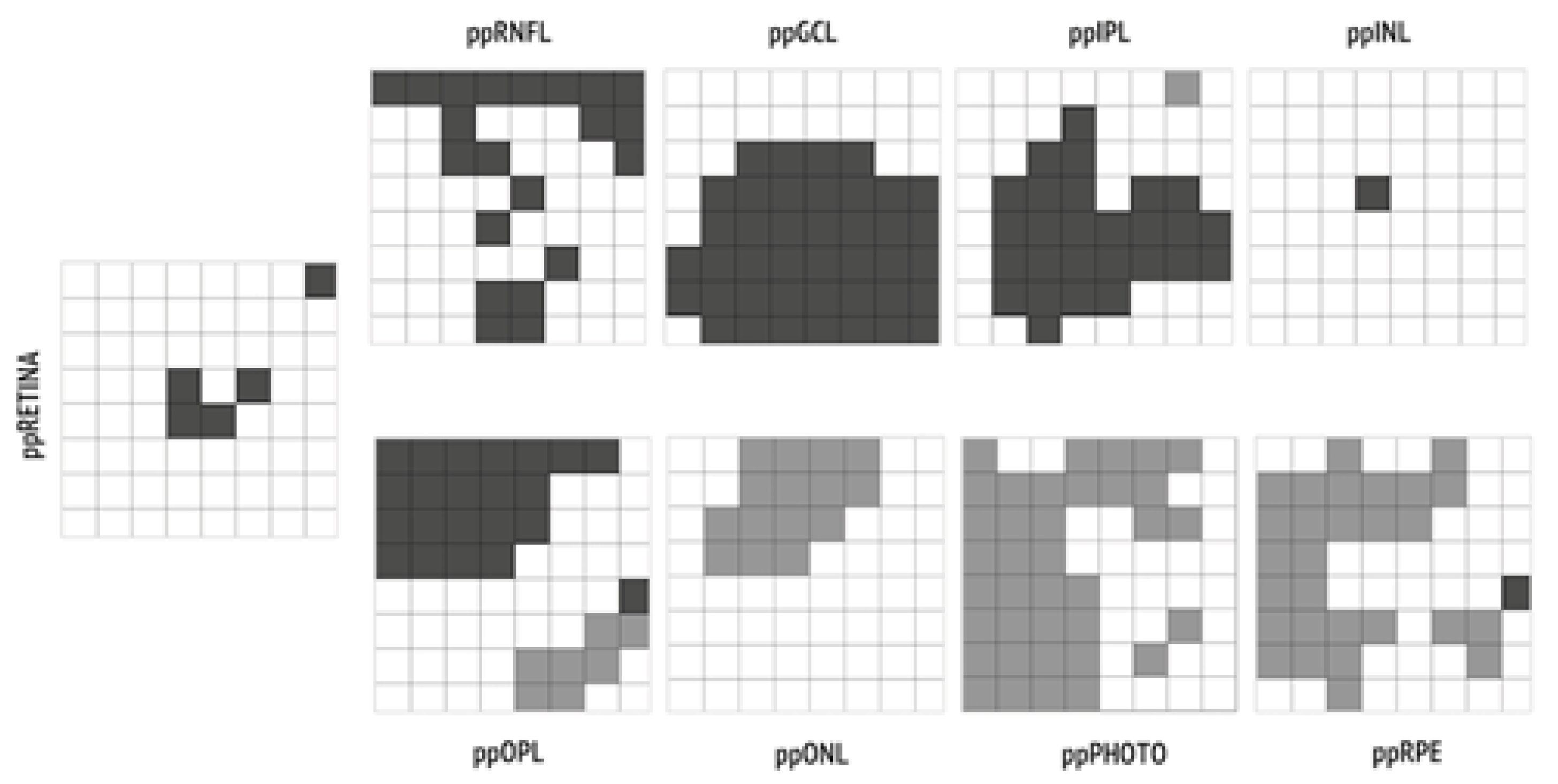
3.2.2. Mean Thickness of the Retinal Posterior Pole by Layers and Regions
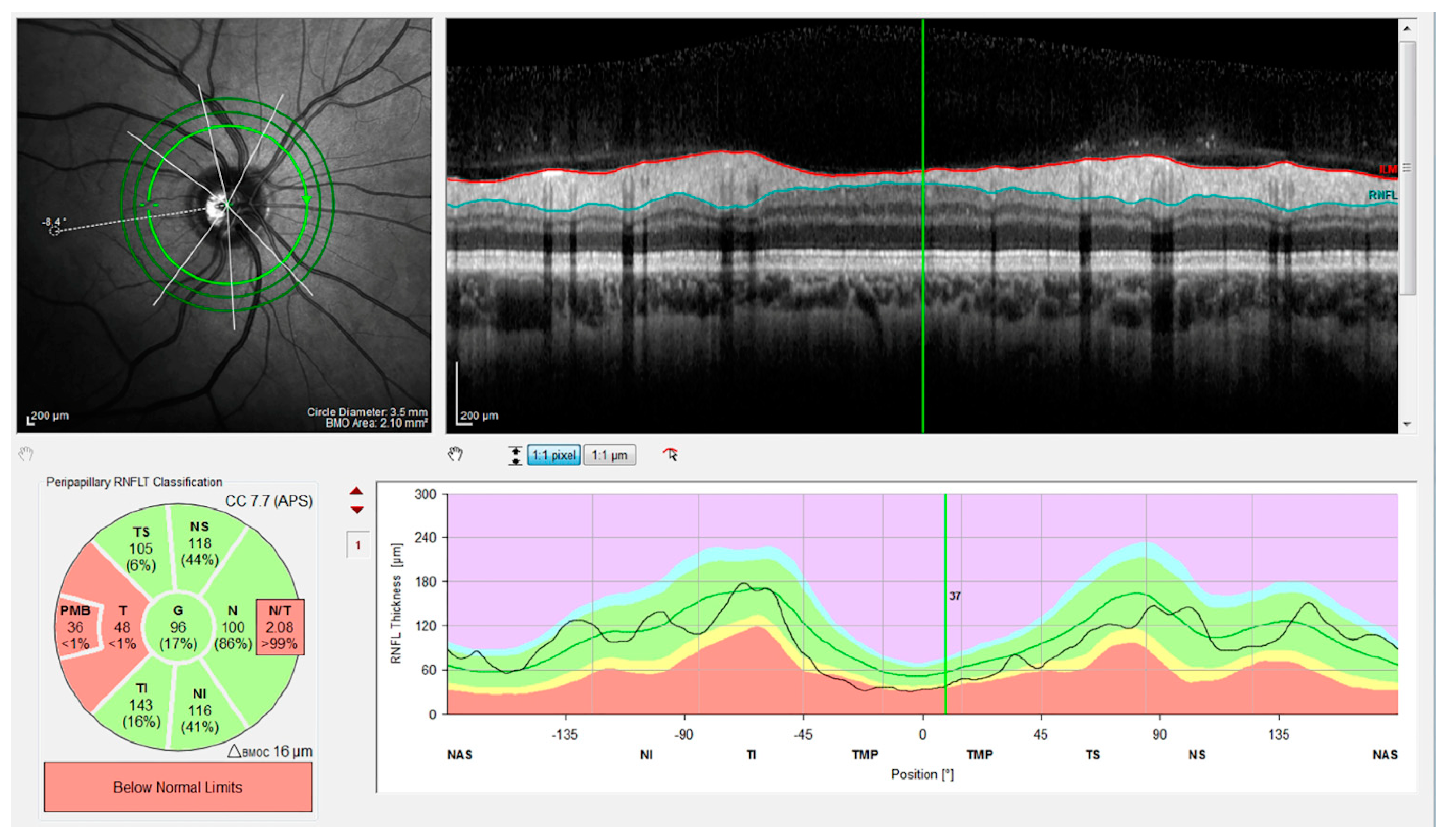
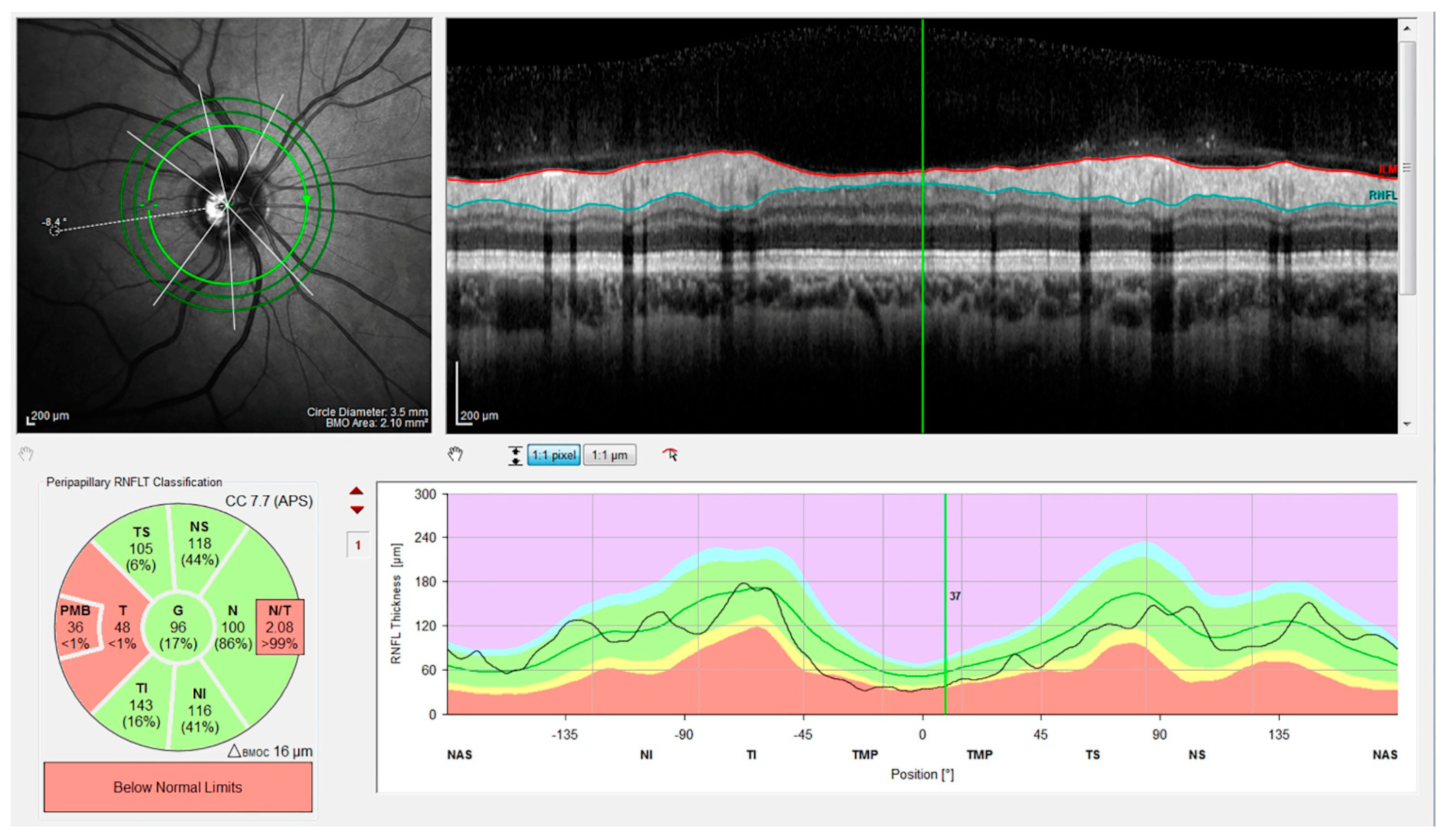
3.2.3. Mean Thickness of the Optic Disk by Quadrants
3.3. Correlations between OCT Parameters and Clinical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petzold, A.; Balcer, L.J.; Calabresi, P.A.; Costello, F.; Frohman, T.C.; Frohman, E.M.; Martinez-Lapiscina, E.H.; Green, A.J.; Kardon, R.; Outteryck, O. Retinal layer segmentation in multiple sclerosis: A systematic review and meta-analysis. Lancet Neurol. 2017, 16, 797–812. [Google Scholar] [CrossRef] [Green Version]
- Cesareo, M.; Ciuffoletti, E.; Martucci, A.; Balducci, C.; Cusumano, A.; Ricci, F.; Sorge, R. Automatic Segmentation of Posterior Pole Retinal Layers in Patients with Early Stage Glaucoma Using Spectral Domain Optical Coherence Tomography. J. Clin. Exp. Ophthalmol. 2016, 7, 538. [Google Scholar] [CrossRef] [Green Version]
- Cesareo, M.; Ciuffoletti, E.; Martucci, A.; Sebastiani, J.; Sorge, R.P.; Lamantea, E.; Garavaglia, B.; Ricci, F.; Cusumano, A.; Nucci, C. Assessment of the retinal posterior pole in dominant optic atrophy by spectral-domain optical coherence tomography and microperimetry. PLoS ONE 2017, 12, e0174560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martucci, A.; Toschi, N.; Cesareo, M.; Giannini, C.; Pocobelli, G.; Garaci, F.; Mancino, R.; Nucci, C. Spectral Domain Optical Coherence Tomography Assessment of Macular and Optic Nerve Alterations in Patients with Glaucoma and Correlation with Visual Field Index. J. Ophthalmol. 2018, 2018, 6581846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chorostecki, J.; Seraji-Bozorgzad, N.; Shah, A.; Bao, F.; Bao, G.; George, E.; Gorden, V.; Caon, C.; Frohman, E.; Bhatti, M.T. Characterization of retinal architecture in Parkinson’s disease. J. Neurol. Sci. 2015, 355, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Murphy, O.C.; Kalaitzidis, G.; Vasileiou, E.; Filippatou, A.G.; Lambe, J.; Ehrhardt, H.; Pellegrini, N.; Sotirchos, E.S.; Luciano, N.J.; Liu, Y. Optical Coherence Tomography and Optical Coherence Tomography Angiography Findings After Optic Neuritis in Multiple Sclerosis. Front Neurol. 2020, 11, 618879. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuman, J.S.; Pedut-Kloizman, T.; Hertzmark, E.; Hee, M.R.; Wilkins, J.R.; Coker, J.G.; Puliafito, C.A.; Fujimoto, J.G.; Swanson, E.A. Reproducibility of nerve fiber layer thickness measurements using optical coherence tomography. Ophthalmology. 1996, 103, 1889–1898. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Martin, E.; Polo, V.; Larrosa, J.M.; Marques, M.L.; Herrero, R.; Martin, J.; Ara, J.R.; Fernandez, J.; Pablo, L.E. Retinal layer segmentation in patients with multiple sclerosis using spectral domain optical coherence tomography. Ophthalmology 2014, 121, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Britze, J.; Pihl-Jensen, G.; Frederiksen, J.L. Retinal ganglion cell analysis in multiple sclerosis and optic neuritis: A systematic review and meta-analysis. J. Neurol. 2017, 264, 1837–1853. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.Y.; Cringle, S.J.; Balaratnasingam, C.; Morgan, W.H.; Yu, P.K.; Su, E.N. Retinal ganglion cells: Energetics, compartmentation, axonal transport, cytoskeletons and vulnerability. Prog. Retin. Eye Res. 2013, 36, 217–246. [Google Scholar] [CrossRef] [PubMed]
- Campbell, G.; Licht-Mayer, S.; Mahad, D. Targeting mitochondria to protect axons in progressive MS. Neurosci. Lett. 2019, 710, 134258. [Google Scholar] [CrossRef] [PubMed]
- Parisi, V.; Manni, G.; Spadaro, M.; Colacino, G.; Restuccia, R.; Marchi, S.; Pierelli, F. Correlation between morphological and functional retinal impairment in multiple sclerosis patients. Investig. Ophthalmol. Vis. Sci. 1999, 40, 2520–2527. [Google Scholar]
- Saidha, S.; Al-Louzi, O.; Ratchford, J.N.; Bhargava, P.; Oh, J.; Newsome, S.D.; Prince, J.L.; Pham, D.; Roy, S.; van Zijl, P. Optical coherence tomography reflects brain atrophy in multiple sclerosis: A four-year study. Ann. Neurol. 2015, 78, 801–813. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, D.; Cheng, H.; Bonem, K.N.; Saenz, R.; Tang, R.A.; Frishman, L.J. Tracking changes over time in retinal nerve fiber layer and ganglion cell-inner plexiform layer thickness in multiple sclerosis. Mult. Scler. 2014, 20, 1331–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelfand, J.M.; Goodin, D.S.; Boscardin, W.J.; Nolan, R.; Cuneo, A.; Green, A.J. Retinal axonal loss begins early in the course of multiple sclerosis and is similar between progressive phenotypes. PLoS ONE 2012, 7, e36847. [Google Scholar] [CrossRef] [PubMed]
- Manogaran, P.; Samardzija, M.; Schad, A.N.; Wicki, C.A.; Walker-Egger, C.; Rudin, M.; Grimm, C.; Schippling, S. Retinal pathology in experimental optic neuritis is characterized by retrograde degeneration and gliosis. Acta Neuropathol. Commun. 2019, 7, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhe, R.; Pearson, R.A. Rebuilding the Retina: Prospects for Müller Glial-mediated Self-repair. Curr. Eye Res. 2020, 45, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Ziccardi, L.; Barbano, L.; Boffa, L.; Albanese, M.; Grzybowski, A.; Centonze, D.; Parisi, V. Morphological Outer Retina Findings in Multiple Sclerosis Patients with or Without Optic Neuritis. Front. Neurol. 2020, 11, 858. [Google Scholar] [CrossRef] [PubMed]
- Nuschke, A.C.; Farrell, S.R.; Levesque, J.M.; Chauhan, B.C. Assessment of retinal ganglion cell damage in glaucomatous optic neuropathy: Axon transport, injury and soma loss. Exp. Eye Res. 2015, 141, 111–124. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| RRMS | CONTROLS | |
|---|---|---|
| Eyes (n) | 97 | 106 |
| Age (years), mean, SD | 37.4 ± 10.1 | 36.11 ± 12.94 |
| Sex (F), n, % | 73 F (76.2%) | 72 F (67.9%) |
| EDSS | 1.9 ± 1.3 | - |
| Disease duration (months) | 43.2 ± 66.7 | - |
| Group | Thickness (µn) | Retina | RNFL | GCL | IPL | INL | OPL | ONL | PHOTO | RPE |
|---|---|---|---|---|---|---|---|---|---|---|
| MS | Mean | 291.6 | 41.6 | 31.4 | 27.2 | 30.8 | 27.1 | 56.3 | 77.6 | 13.5 |
| SD | 12.2 | 5.2 | 2.6 | 2 | 1.6 | 2 | 6.3 | 2.2 | 1 | |
| CTRL | Mean | 293.2 | 42.8 | 32.7 | 26.7 | 30.7 | 27.3 | 55.5 | 76.8 | 13.1 |
| SD | 12.7 | 4.5 | 1.9 | 1.6 | 1.7 | 2.1 | 5.4 | 2.1 | 1.1 | |
| p | 0.3 | 0.072 | 0.001 | 0.074 | 0.7 | 0.7 | 0.3 | 0.001 | 0.014 | |
| Group | Thickness (µn) | PMB | TI | T | TS | NI | N | NS | G | N/T |
|---|---|---|---|---|---|---|---|---|---|---|
| MS | Mean | 49.8 | 146.6 | 65.7 | 125 | 112.6 | 83.6 | 113.4 | 97.2 | 1.3 |
| SD | 8.9 | 21.5 | 12.2 | 22.6 | 23.3 | 21.8 | 24.4 | 12.6 | 0.5 | |
| CTRL | Mean | 54.3 | 150.4 | 71.1 | 127.7 | 110.1 | 82.9 | 116.6 | 99.1 | 1.19 |
| SD | 6.9 | 17.2 | 9.8 | 17.3 | 23.3 | 11.1 | 19.8 | 8.0 | 0.24 | |
| p | 0.0001 | 0.162 | 0.001 | 0.343 | 0.439 | 0.783 | 0.311 | 0.193 | 0.017 | |
| Retina | RNFL | GCL | PMB | TI | T | TS | G | ||
|---|---|---|---|---|---|---|---|---|---|
| Disease duration | R | −0.390 | −0.423 | −0.365 | −0.501 | −0.317 | −0.463 | −0.231 | −0.316 |
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.002 | 0.001 | 0.020 | 0.020 | |
| EDSS | R | −0.388 | −0.267 | −0.245 | 0.345 | −0.280 | −0.264 | ||
| p | 0.001 | 0.008 | 0.016 | 0.001 | 0.005 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martucci, A.; Landi, D.; Cesareo, M.; Di Carlo, E.; Di Mauro, G.; Sorge, R.P.; Albanese, M.; Gabri Nicoletti, C.; Mataluni, G.; Mercuri, N.B.; et al. Complex Rearrangement of the Entire Retinal Posterior Pole in Patients with Relapsing Remitting Multiple Sclerosis. J. Clin. Med. 2021, 10, 4693. https://doi.org/10.3390/jcm10204693
Martucci A, Landi D, Cesareo M, Di Carlo E, Di Mauro G, Sorge RP, Albanese M, Gabri Nicoletti C, Mataluni G, Mercuri NB, et al. Complex Rearrangement of the Entire Retinal Posterior Pole in Patients with Relapsing Remitting Multiple Sclerosis. Journal of Clinical Medicine. 2021; 10(20):4693. https://doi.org/10.3390/jcm10204693
Chicago/Turabian StyleMartucci, Alessio, Doriana Landi, Massimo Cesareo, Emiliano Di Carlo, Giovanni Di Mauro, Roberto Pietro Sorge, Maria Albanese, Carolina Gabri Nicoletti, Giorgia Mataluni, Nicola Biagio Mercuri, and et al. 2021. "Complex Rearrangement of the Entire Retinal Posterior Pole in Patients with Relapsing Remitting Multiple Sclerosis" Journal of Clinical Medicine 10, no. 20: 4693. https://doi.org/10.3390/jcm10204693
APA StyleMartucci, A., Landi, D., Cesareo, M., Di Carlo, E., Di Mauro, G., Sorge, R. P., Albanese, M., Gabri Nicoletti, C., Mataluni, G., Mercuri, N. B., Di Marino, M., Aiello, F., Centonze, D., Nucci, C., Marfia, G. A., & Mancino, R. (2021). Complex Rearrangement of the Entire Retinal Posterior Pole in Patients with Relapsing Remitting Multiple Sclerosis. Journal of Clinical Medicine, 10(20), 4693. https://doi.org/10.3390/jcm10204693