Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again


Abstract
1. Introduction
1.1. Background
1.2. Unmet Medical Needs for ROP Treatment
2. Relationship between Oxygen Concentration and Retinal Neovascularization
2.1. The First ROP Epidemic: Learning from the Bedside
2.2. Advances in Respiratory Management: Reduction of Oxygen Supplementation
2.3. Establishment of the Animal Model of ROP: Learning from the Bench
3. Existing Treatments for ROP
3.1. Cryotherapy
3.2. Laser Photocoagulation
3.3. Anti-VEGF Therapy
3.3.1. Bioactivity of VEGF
3.3.2. VEGF Expression in Phase 1 and Phase 2
3.3.3. Clinical Trials with Anti-VEGF Therapy
4. Translational ROP Research: Previous and Ongoing Clinical Trials
4.1. Antioxidants
4.2. Vitamin A
4.3. Adrenocorticotropic Hormone and Steroids
4.4. Erythropoietin
4.5. Insulin-Like Growth Factor 1 and Insulin-Like Growth Factor Binding Protein 3
4.6. Non-Steroidal Anti-Inflammatory Drugs
4.7. ω-3-Polyunsaturated Fatty Acids
4.8. β-Blockers
4.9. Rho-Associated Protein Kinase
5. New Biomarkers and Candidate Targeted Molecules for ROP
5.1. Macrophage Inflammatory Protein-1β
5.2. Mast Cell Tryptase
5.3. Suppressor of Cytokine Signaling-3 and Retinoic Acid Receptor-Related Orphan Receptor Alpha
6. Clinical Trials in Preterm Infants: Differences from Adults
7. Future Prospects
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fielder, A.; Blencowe, H.; O’Connor, A.; Gilbert, C. Impact of retinopathy of prematurity on ocular structures and visual functions. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 100, F179–F184. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, C. Retinopathy of prematurity: A global perspective of the epidemics, population of babies at risk and implications for control. Early Hum. Dev. 2008, 84, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Lawn, J.E.; Vazquez, T.; Fielder, A.; Gilbert, C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr. Res. 2013, 74, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.L.; Sorita, A.; Carey, W.A.; Colby, C.E.; Murad, M.H.; Alahdab, F. Interventions to Prevent Retinopathy of Prematurity: A Meta-analysis. Pediatrics 2016, 137, e20153387. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.H.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef]
- Palmer, E.A.; Flynn, J.T.; Hardy, R.J.; Phelps, D.L.; Phillips, C.L.; Schaffer, D.B.; Tung, B.; Elsas, F.J.; Botsford, J.M.; Braune, K.W.; et al. Incidence and Early Course of Retlnonathy of Prematurity. Ophthalmology 1991, 98, 1628–1640. [Google Scholar] [CrossRef]
- Quinn, G.E.; Barr, C.; Bremer, D.; Fellows, R.; Gong, A.; Hoffman, R.; Repka, M.X.; Shepard, J.; Siatkowski, R.M.; Wade, K.; et al. Changes in course of retinopathy of prematurity from 1986 to 2013: Comparison of three studies in the United States. Ophthalmology 2016, 123, 1595–1600. [Google Scholar] [CrossRef]
- Provis, J.M. Development of the Primate Retinal Vasculature. Prog. Retin. Eye Res. 2001, 20, 799–821. [Google Scholar] [CrossRef]
- Dubis, A.M.; Costakos, D.M.; Subramaniam, C.D.; Godara, P.; Wirostko, W.J.; Carroll, J.; Provis, J.M. Evaluation of Normal Human Foveal Development Using Optical Coherence Tomography and Histologic Examination. Arch. Ophthalmol. 2012, 130, 1291–1300. [Google Scholar] [CrossRef]
- Fulton, A.B.; Hansen, R.M.; Moskowitz, A.; Akula, J.D. The neurovascular retina in retinopathy of prematurity. Prog. Retin. Eye Res. 2009, 28, 452–482. [Google Scholar] [CrossRef]
- Ecsedy, M.; Szamosi, A.; Karko, C.; Zubovics, L.; Varsanyi, B.; Nemeth, J.; Recsan, Z. A comparison of macular structure imaged by optical coherence tomog-raphy in preterm and full-term children. Investig. Ophthalmol. Vis. Sci. 2007, 48, 5207–5211. [Google Scholar] [CrossRef] [PubMed]
- Hammer, D.X.; Iftimia, N.V.; Ferguson, R.D.; Bigelow, C.E.; Ustun, T.E.; Barnaby, A.M.; Fulton, A.B. Foveal Fine Structure in Retinopathy of Prematurity: An Adaptive Optics Fourier Domain Optical Coherence Tomography Study. Investig. Opthalmol. Vis. Sci. 2008, 49, 2061–2070. [Google Scholar] [CrossRef] [PubMed]
- Fulton, A.B.; Hansen, R.M.; Moskowitz, A. The Cone Electroretinogram in Retinopathy of Prematurity. Investig. Opthalmol. Vis. Sci. 2008, 49, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Miki, A.; Yamada, Y.; Nakamura, M. The Size of the Foveal Avascular Zone Is Associated with Foveal Thickness and Structure in Premature Children. J. Ophthalmol. 2019, 2019, 8340729-5. [Google Scholar] [CrossRef]
- Ng, P.C.; Wong, S.P.S.; Chan, I.H.S.; Lam, H.S.; Lee, C.H.; Lam, C.W.K. A Prospective Longitudinal Study to Estimate the “Adjusted Cortisol Percentile” in Preterm Infants. Pediatr. Res. 2011, 69, 511–516. [Google Scholar] [CrossRef]
- Masumoto, K.; Kusuda, S.; Aoyagi, H.; Tamura, Y.; Obonai, T.; Yamasaki, C.; Sakuma, I.; Uchiyama, A.; Nishida, H.; Oda, S.; et al. Comparison of Serum Cortisol Concentrations in Preterm Infants with or Without Late-Onset Circulatory Collapse due to Adrenal Insufficiency of Prematurity. Pediatr. Res. 2008, 63, 686–690. [Google Scholar] [CrossRef]
- Ng, P.C. Adrenocortical insufficiency and refractory hypotension in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F571–F576. [Google Scholar] [CrossRef]
- Kirchner, L.; Jeitler, V.; Pollak, A.; Müllner-Eidenböck, A.; Weinzettel, R.; Kraschl, R.; Waldhör, T.; Wald, M. Must screening examinations for retinopathy of prematurity necessarily be painful? Retina 2009, 29, 586–591. [Google Scholar] [CrossRef]
- Kleberg, A.; Warren, I.; Norman, E.; Morelius, E.; Berg, A.-C.; Mat-Ali, E.; Holm, K.; Fielder, A.; Nelson, N.; Hellström-Westas, L. Lower Stress Responses After Newborn Individualized Developmental Care and Assessment Program Care During Eye Screening Examinations for Retinopathy of Prematurity: A Randomized Study. Pediatrics 2008, 121, e1267–e1278. [Google Scholar] [CrossRef]
- Arima, M.; Tsukamoto, S.; Fujiwara, K.; Murayama, M.; Fujikawa, K.; Sonoda, K.-H. Late-onset Circulatory Collapse and Continuous Positive Airway Pressure are Useful Predictors of Treatment-requiring Retinopathy of Prematurity: A 9-year Retrospective Analysis. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Heller, M.J. DNA Microarray Technology: Devices, Systems, and Applications. Annu. Rev. Biomed. Eng. 2002, 4, 129–153. [Google Scholar] [CrossRef] [PubMed]
- Mann, M.; Jensen, O.N. Proteomic analysis of post-translational modifications. Nat. Biotechnol. 2003, 21, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Ozsolak, F.; Milos, P.M. RNA sequencing: Advances, challenges and opportunities. Nat. Rev. Genet. 2010, 12, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Chari, R.V. Targeted Cancer Therapy: Conferring Specificity to Cytotoxic Drugs. Acc. Chem. Res. 2008, 41, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.M.; Hicklin, D.J. VEGF-targeted therapy: Mechanisms of anti-tumour activity. Nat. Rev. Cancer 2008, 8, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Sawyers, C.L. Targeted cancer therapy. Nat. Cell Biol. 2004, 432, 294–297. [Google Scholar] [CrossRef]
- Levy-Clarke, G.; Jabs, D.A.; Read, R.W.; Rosenbaum, J.T.; Vitale, A.; Van Gelder, R.N. Expert Panel Recommendations for the Use of Anti–Tumor Necrosis Factor Biologic Agents in Patients with Ocular Inflammatory Disorders. Ophthalmology 2014, 121, 785–796.e3. [Google Scholar] [CrossRef]
- Andreoli, C.M.; Miller, J.W. Anti-vascular endothelial growth factor therapy for ocular neovascular disease. Curr. Opin. Ophthalmol. 2007, 18, 502–508. [Google Scholar] [CrossRef]
- Gillies, M.C.; Hunyor, A.P.; Arnold, J.J.; Guymer, R.H.; Wolf, S.; Ng, P.; Pecheur, F.L.; McAllister, I.L. Effect of ranibizumab and aflibercept on best-corrected visual acuity in treat-and-extend for neovascular age-related macular degeneration: A randomized clinical trial. JAMA Ophthalmol. 2019, 137, 372–379. [Google Scholar] [CrossRef]
- Tadayoni, R.; Waldstein, S.M.; Boscia, F.; Gerding, H.; Gekkieva, M.; Barnes, E.; Das Gupta, A.; Wenzel, A.; Pearce, I. Sustained benefits of ranibizumab with or without laser in branch retinal vein occlusion: 24-month results of the BRIGHTER study. Ophthalmology 2017, 124, 1778–1787. [Google Scholar] [CrossRef]
- Heier, J.S.; Korobelnik, J.F.; Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Midena, E.; Boyer, D.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal aflibercept for diabetic macular edema: 148-week results from the VISTA and VIVID studies. Ophthalmology 2016, 123, 2376–2385. [Google Scholar] [CrossRef] [PubMed]
- Garcia Gonzalez, J.M.; Snyder, L.; Blair, M.; Rohr, A.; Shapiro, M.; Greenwald, M. Prophylactic peripheral laser and fluorescein angiography afer bevacizumab for retinopathy of prematurity. Retina 2017, 38, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Snyder, L.L.; Garcia-Gonzalez, J.M.; Shapiro, M.J.; Blair, M.P. Very Late Reactivation of Retinopathy of Prematurity After Monotherapy with Intravitreal Bevacizumab. Ophthalmic Surg. Lasers Imaging Retin. 2016, 47, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Hajrasouliha, A.R.; Garcia-Gonzales, J.M.; Shapiro, M.J.; Yoon, H.; Blair, M.P. Reactivation of Retinopathy of Prematurity Three Years After Treatment with Bevacizumab. Ophthalmic Surg. Lasers Imaging Retin. 2017, 48, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Blair, M.P.; Shapiro, M.J.; Lichtenstein, S.J.; Galasso, J.M.; Kapur, R. Reactivation of Retinopathy of Prematurity After Bevacizumab Injection. Arch. Ophthalmol. 2012, 130, 1000–1006. [Google Scholar] [CrossRef]
- Wu, W.-C.; Lien, R.; Liao, P.-J.; Wang, N.-K.; Chen, Y.-P.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C. Serum Levels of Vascular Endothelial Growth Factor and Related Factors After Intravitreous Bevacizumab Injection for Retinopathy of Prematurity. JAMA Ophthalmol. 2015, 133, 391–397. [Google Scholar] [CrossRef]
- Wu, W.-C.; Shih, C.-P.; Lien, R.; Wang, N.-K.; Chen, Y.-P.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C. Serum vascular endothelial growth factor after bevacizumab or ranibizumab treatment for retinopathy of prematurity. Retina 2017, 37, 694–701. [Google Scholar] [CrossRef]
- Lien, R.; Yu, M.-H.; Hsu, K.-H.; Liao, P.-J.; Chen, Y.-P.; Lai, C.-C.; Wu, W.-C. Neurodevelopmental Outcomes in Infants with Retinopathy of Prematurity and Bevacizumab Treatment. PLoS ONE 2016, 11, e0148019. [Google Scholar] [CrossRef]
- Natarajan, G.; Shankaran, S.; Nolen, T.L.; Sridhar, A.; Kennedy, K.A.; Hintz, S.R.; Phelps, D.L.; DeMauro, S.B.; Carlo, W.A.; Gantz, M.G.; et al. Neurodevelopmental Outcomes of Preterm Infants with Retinopathy of Prematurity by Treatment. Pediatrics 2019, 144, e20183537. [Google Scholar] [CrossRef]
- Arima, M.; Akiyama, M.; Fujiwara, K.; Mori, Y.; Inoue, H.; Seki, E.; Nakama, T.; Tsukamoto, S.; Ochiai, M.; Ohga, S.; et al. Neurodevelopmental outcomes following intravitreal bevacizumab injection in Japanese preterm infants with type 1 retinopathy of prematurity. PLoS ONE 2020, 15, e0230678. [Google Scholar] [CrossRef]
- Wu, A.L.; Wu, W.C. Anti-VEGF for ROP and pediatric retinal diseases. Asia Pac. J. Ophthalmol. 2018, 7, 145–151. [Google Scholar] [CrossRef]
- McCourt, E.; Ying, G.-S.; Lynch, A.M.; Palestine, A.G.; Wagner, B.D.; Wymore, E.; Tomlinson, L.A.; Binenbaum, G. G-ROP Study Group Validation of the Colorado Retinopathy of Prematurity Screening Model. JAMA Ophthalmol. 2018, 136, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Pivodic, A.; Hård, A.L.; Löfqvist, C.; Smith, L.E.H.; Wu, C.; Bründer, M.C.; Lagrèze, W.A.; Stahl, A.; Holmström, G.; Albertsson-Wikland, K.; et al. Individual risk prediction for sight-threatening retinopathy of prematurity using birth characteristics. JAMA Ophthalmol. 2020, 138, 21–29. [Google Scholar] [CrossRef]
- Ying, G.-S.; Vanderveen, D.K.; Daniel, E.; Quinn, G.E.; Baumritter, A. Telemedicine Approaches to Evaluating Acute-Phase Retinopathy of Prematurity Cooperative Group Risk Score for Predicting Treatment-Requiring Retinopathy of Prematurity (ROP) in the Telemedicine Approaches to Evaluating Acute-Phase ROP Study. Ophthalmology 2016, 123, 2176–2182. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Löfqvist, C.; Andersson, E.; Sigurdsson, J.; Engström, E.; Hård, A.-L.; Niklasson, A.; Smith, L.E.H.; Hellström, A. Longitudinal Postnatal Weight and Insulin-like Growth Factor I Measurements in the Prediction of Retinopathy of Prematurity. Arch. Ophthalmol. 2006, 124, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Hellström, A.; Hård, A.-L.; Engström, E.; Niklasson, A.; Andersson, E.; Smith, L.; Löfqvist, C. Early Weight Gain Predicts Retinopathy in Preterm Infants: New, Simple, Efficient Approach to Screening. Pediatrics 2009, 123, e638–e645. [Google Scholar] [CrossRef]
- Eckert, G.U.; Filho, J.B.F.; Maia, M.; Procianoy, R.S. A predictive score for retinopathy of prematurity in very low birth weight preterm infants. Eye 2011, 26, 400–406. [Google Scholar] [CrossRef]
- Binenbaum, G.; Ying, G.-S.; Quinn, G.E.; Huang, J.; Dreiseitl, S.; Antigua, J.; Foroughi, N.; Abbasi, S. The CHOP Postnatal Weight Gain, Birth Weight, and Gestational Age Retinopathy of Prematurity Risk Model. Arch. Ophthalmol. 2012, 130, 1560–1565. [Google Scholar] [CrossRef]
- Van Sorge, A.J.; Schalij-Delfos, N.E.; Kerkhoff, F.T.; Van Rijn, L.J.; Van Hillegersberg, J.L.A.M.; Van Liempt, I.L.A.; Peer, P.G.M.; Simonsz, H.J.; Termote, J.U.M. Reduction in screening for retinopathy of prematurity through risk factor adjusted inclusion criteria. Br. J. Ophthalmol. 2013, 97, 1143–1147. [Google Scholar] [CrossRef]
- Greenwald, M.F.; Danford, I.D.; Shahrawat, M.; Ostmo, S.; Brown, J.; Kalpathy-Cramer, J.; Bradshaw, K.; Schelonka, R.; Cohen, H.S.; Chan, R.V.P.; et al. Evaluation of artificial intelligence-based telemedicine screening for retinopathy of prematurity. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2020, 160–162. [Google Scholar] [CrossRef]
- Brown, J.M.; Campbell, J.P.; Beers, A.; Chang, K.; Ostmo, S.; Chan, R.V.P.; Dy, J.; Erdoğmuş, D.; Ioannidis, S.; Kalpathy-Cramer, J.; et al. Automated Diagnosis of Plus Disease in Retinopathy of Prematurity Using Deep Convolutional Neural Networks. JAMA Ophthalmol. 2018, 136, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.F. Reflections on Errors in Neonatology: I. The “Hands-Off” Years, 1920 to 1950. J. Perinatol. 2003, 23, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, L.; Reynolds, W.E.; Chisholm, J.F.; King, M.J. The incidence and severity of retrolental fibroplasia in relation to possible causative factors*. Am. J. Ophthalmol. 1954, 38, 317–336. [Google Scholar] [CrossRef]
- Terry, T. Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Am. J. Ophthalmol. 1942, 25, 203–204. [Google Scholar] [CrossRef]
- Terry, T.L. Ocular maldevelopment in extremely premature infants. J. Am. Med. Assoc. 1945, 128, 582–585. [Google Scholar] [CrossRef]
- Owens, W.C.; Owens, E.U. Retrolental Fibroplasia in Premature Infants*: II. Studies on the Prophylaxis of the Disease: The use of Alpha Tocopheryl Acetate. Am. J. Ophthalmol. 1949, 32, 1631–1637. [Google Scholar] [CrossRef]
- Reese, A.B.; Blodi, F.C. Retrolental fibroplasia. Am. J. Ophthalmol. 1951, 34, 1–24. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- The Committee for the Classification of Retinopathy of Prematurity. An international classification of retinopathy of prematurity. Arch. Ophthalmol. 1984, 102, 1130–1134. [Google Scholar] [CrossRef]
- Szewczyk, T.S. Retrolental fibroplasia; etiology and prophylaxis. Am. J. Ophthalmol. 1952, 35, 301–311. [Google Scholar] [CrossRef]
- Ingalls, T.H.; Tedeschi, C.G.; Helpern, M.M. Congenital malformations of the eye induced in mice by maternal anoxia; with particular reference to the problem of retrolental fibroplasia in man. Am. J. Ophthalmol. 1952, 35, 311–329. [Google Scholar] [CrossRef]
- Campbell, K. Intensive oxygen therapy as a possible cause of retrolental fibroplasia: A clinical approach. Med. J. Aust. 1951, 2, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Silverman, W.A.; Blodi, F.C.; Locke, J.C.; Day, R.L.; Reese, A.B. Incidence of retrolental fibroplasia in a New York nursery. Arch. Ophthalmol. 1952, 48, 698–711. [Google Scholar] [CrossRef] [PubMed]
- Lanman, J.T.; Guy, L.P.; Dancis, J. Retrolental fibroplasia and oxygen therapy. J. Am. Med. Assoc. 1954, 155, 223–226. [Google Scholar] [CrossRef]
- Patz, A.; Hoeck, L.E.; De La Cruz, E. Studies on the Effect of High Oxygen Administration in Retrolental Fibroplasia*. Am. J. Ophthalmol. 1952, 35, 1248–1253. [Google Scholar] [CrossRef]
- Shohat, M.; Reisner, S.H.; Krikler, R.; Nissenkorn, I.; Yassur, Y.; Ben-Sira, I. Retinopathy of prematurity: Incidence and risk factors. Pediatrics 1983, 72, 159–163. [Google Scholar] [CrossRef]
- Bancalari, E.; Flynn, J.; Goldberg, R.N.; Bawol, R.; Cassady, J.; Schiffman, J.; Feuer, W.; Roberts, J.; Gillings, D.; Sim, E. Influence of transcutaneous oxygen monitoring on the incidence of retinopathy of prematurity. Pediatrics 1987, 79, 663–669. [Google Scholar]
- Kinsey, V.E.; Arnold, H.J.; Kalina, R.E.; Stern, L.; Stahlman, M.; Odell, G.; Driscoll, J.M.; Elliott, J.H.; Payne, J.; Patz, A. PaO2 levels and retrolental fibroplasia: A report of the cooperative study. Pediatrics 1977, 60, 655–668. [Google Scholar]
- Flynn, J.T.; Bancalari, E.; Bawol, R.; Goldberg, R.; Cassady, J.; Schiffman, J.; Feuer, W.; Roberts, J.; Gillings, D.; Sim, E.; et al. Retinopathy of prematurity: A randomized, prospective trial of transcutaneous oxygen monitoring. Ophthalmology 1987, 94, 630–638. [Google Scholar] [CrossRef]
- Jennis, M.S.; Peabody, J.L. Pulse oximetry: An alternative method for the assessment of oxygenation in newborn infants. Pediatrics 1987, 79, 524–528. [Google Scholar]
- Yoshiya, I.; Shimada, Y.; Tanaka, K. Spectrophotometric monitoring of arterial oxygen saturation in the fingertip. Med. Biol. Eng. Comput. 1980, 18, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Southall, D.P.; Bignall, S.; Stebbens, V.A.; Alexander, J.R.; Rivers, R.P.; Lissauer, T. Pulse oximeter and transcutaneous arterial oxygen measurements in neonatal and paediatric intensive care. Arch. Dis. Child. 1987, 62, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.T.; Bancalari, E.; Snyder, E.S.; Goldberg, R.N.; Feuer, W.; Cassady, J.; Schiffman, J.; Feldman, H.I.; Baghynski, B.; Buckley, E.; et al. A Cohort Study of Transcutaneous Oxygen Tension and the Incidence and Severity of Retinopathy of Prematurity. N. Engl. J. Med. 1992, 326, 1050–1054. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Whyte, R.K.; Asztalos, E.V.; Moddemann, D.; Poets, C.; Rabi, Y.; Solimano, A.; Roberts, R.S. Effects of targeting higher vs lower arterial oxygen saturations on death or disability in extremely preterm infants: A randomized clinical trial. JAMA 2013, 309, 2111–2120. [Google Scholar] [CrossRef]
- Phelps, D.L. Supplemental therapeutic oxygen for prethreshold retinopathy of prematurity (STOP-ROP), a randomized, controlled trial. I: Primary outcomes. Pediatrics 2000, 105, 295–310. [Google Scholar]
- Schaapveld, M.; Aleman, B.M.P.; van Eggermond, A.M.; Janus, C.P.M.; Krol, A.D.G.; van der Maazen, R.W.M.; Roesink, J.; Raemaekers, J.M.M.; de Boer, J.P.; Zijlstra, J.M.; et al. Target ranges of oxygen saturation in extremely preterm infants. N. Engl. J. Med. 2010, 362, 1959–1969. [Google Scholar]
- Askie, L.M.; Henderson-Smart, D.J.; Irwig, L.; Simpson, J.M. Oxygen-Saturation Targets and Outcomes in Extremely Preterm Infants. N. Engl. J. Med. 2003, 349, 959–967. [Google Scholar] [CrossRef]
- Stenson, B.J.; Tarnow-Mordi, W.O.; Darlow, B.A.; Simes, J.; Juszczak, E.; Askie, L.M.; Battin, M.R.; Bowler, U.; Broadbent, R.S.; Cairns, P.; et al. Oxygen Saturation and Outcomes in Preterm Infants. N. Engl. J. Med. 2013, 368, 2094–2104. [Google Scholar] [CrossRef]
- Tarnow-Mordi, W.; Stenson, B.; Kirby, A.; Juszczak, E.; Donoghoe, M.; Deshpande, S.; Morley, C.; King, A.; Doyle, L.W.; Fleck, B.W.; et al. Outcomes of two trials of oxygen-saturation targets in preterm infants. N. Engl. J. Med. 2016, 374, 749–760. [Google Scholar]
- Askie, L.M.; Darlow, B.A.; Finer, N.; Schmidt, B.; Stenson, B.; Tarnow-Mordi, W.; Davis, P.G.; Carlo, W.A.; Brocklehurst, P.; Davies, L.C.; et al. Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration. JAMA 2018, 319, 2190–2201. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Pas, A.T.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.J.; Polin, R.A. Committee on Fetus and Newborn Oxygen Targeting in Extremely Low Birth Weight Infants. Pediatrics 2016, 138, e20161576. [Google Scholar] [CrossRef] [PubMed]
- Kirpalani, H.; Millar, D.; Lemyre, B.; Yoder, B.A.; Chiu, A.; Roberts, R.S. A Trial Comparing Noninvasive Ventilation Strategies in Preterm Infants. N. Engl. J. Med. 2013, 369, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Davis, P.G.; Schmidt, B.; Roberts, R.S.; Doyle, L.W.; Asztalos, E.; Haslam, R.; Sinha, S.; Tin, W. Caffeine for Apnea of Prematurity Trial: Benefits May Vary in Subgroups. J. Pediatr. 2010, 156, 382–387.e3. [Google Scholar] [CrossRef] [PubMed]
- Finer, N.N.; Carlo, W.A.; Walsh, M.C.; Rich, W.; Gantz, M.G.; Laptook, A.R.; Yoder, B.A.; Faix, R.G.; Das, A.; Poole, W.K.; et al. Early CPAP versus surfactant in extremely preterm infants. N. Engl. J. Med. 2010, 362, 1970–1979. [Google Scholar] [CrossRef] [PubMed]
- Pennefather, P.M.; Tin, W.; Clarke, M.P.; Fritz, S.; Strong, N.P. Retinopathy of prematurity in a controlled trial of prophylactic surfactant treatment. Br. J. Ophthalmol. 1996, 80, 420–424. [Google Scholar] [CrossRef]
- Kinsey, V.E.; Jacobus, J.T.; Hemphill, F.M. Retrolental Fibroplasia. A.M.A. Arch. Ophthalmol. 1956, 56, 481–543. [Google Scholar] [CrossRef]
- Lucey, J.F.; Dangman, B. A reexamination of the role of oxygen in retrolental fibroplasia. Pediatrics 1984, 73, 82–96. [Google Scholar]
- Ashton, N.; Ward, B.; Serpell, G. Effect of Oxygen on Developing Retinal Vessels with Particular Reference to the Problem of Retrolental Fibroplasia. Br. J. Ophthalmol. 1954, 38, 397–432. [Google Scholar] [CrossRef]
- Ashton, N. Retinal Vascularization in Health and Disease. Am. J. Ophthalmol. 1957, 44, 7–17. [Google Scholar] [CrossRef]
- Dollery, C.T.; Hill, D.W.; Mailer, C.M.; Ramalho, P.S. High oxygen pressureand the retinal blood-vessels. Lancet 1964, 2, 291–292. [Google Scholar] [CrossRef]
- Dollery, C.T.; Bulpitt, C.J.; Kohner, E.M. Oxygen supply to the retina from the retinal and choroidal circulations at normal and increased arterial oxygen tensions. Investig. Ophthalmol. 1969, 8, 588–594. [Google Scholar]
- Wellard, J.; Lee, D.; Valter, K.; Stone, J. Photoreceptors in the rat retina are specifically vulnerable to both hypoxia and hyperoxia. Vis. Neurosci. 2005, 22, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Fulton, A.B.; Reynaud, X.; Hansen, R.M.; Lemere, C.A.; Parker, C.; Williams, T.P. Rod photoreceptors in infant rats with a history of oxygen exposure. Investig. Ophthalmol. Vis. Sci. 1999, 40, 168–174. [Google Scholar]
- Mezu-Ndubuisi, O.J.; Macke, E.L.; Kalavacherla, R.; Nwaba, A.A.; Suscha, A.; Zaitoun, I.S.; Ikeda, A.; Sheibani, N. Long-term evaluation of retinal morphology and function in a mouse model of oxygen-induced retinopathy. Mol. Vis 2020, 26, 257–276. [Google Scholar]
- Hellström, A.; Smith, L.E.H.; Dammann, O. Retinopathy of prematurity. Lancet 2013, 382, 1445–1457. [Google Scholar] [CrossRef]
- Kremer, I.; Kissun, R.; Nissenkorn, I.; Ben-Sira, I.; Garner, A. Oxygen-induced retinopathy in newborn kittens. A model for ischemic vasoproliferative retinopathy. Investig. Ophthalmol. Vis. Sci. 1987, 28, 126–130. [Google Scholar]
- Phelps, D.L. Reduced Severity of Oxygen-Induced Retinopathy in Kittens Recovered in 28% Oxygen. Pediatr. Res. 1988, 24, 106–109. [Google Scholar] [CrossRef]
- Flower, R.W.; Blake, D.A.; Wajer, S.D.; Egner, P.G.; McLeod, D.S.; Pitts, S.M. Retrolental Fibroplasia: Evidence for a Role of the Prostaglandin Cascade in the Pathogenesis of Oxygen-Induced Retinopathy in the Newborn Beagle. Pediatr. Res. 1981, 15, 1293–1302. [Google Scholar] [CrossRef]
- McLeod, D.S.; Brownstein, R.; Lutty, G.A. Vaso-obliteration in the canine model of oxygen-induced retinopathy. Investig. Ophthalmol. Vis. Sci. 1996, 37, 300–311. [Google Scholar]
- McLeod, D.S.; Crone, S.N.; Lutty, G.A. Vasoproliferation in the neonatal dog model of oxygen-induced retinopathy. Investig. Ophthalmol. Vis. Sci. 1996, 37, 1322–1333. [Google Scholar]
- McLeod, D.S.; D’Anna, S.A.; Lutty, G.A. Clinical and histopathologic features of canine oxygen-induced proliferative retinopathy. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1918–1932. [Google Scholar]
- Penn, J.S.; Henry, M.M.; Tolman, B.L. Exposure to Alternating Hypoxia and Hyperoxia Causes Severe Proliferative Retinopathy in the Newborn Rat. Pediatr. Res. 1994, 36, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Wesolowski, E.; McLellan, A.; Kostyk, S.K.; D’Amato, R.; Sullivan, R.; D’Amore, P.A. Oxygen-induced retinopathy in the mouse. Investig. Ophthalmol. Vis. Sci. 1994, 35, 101–111. [Google Scholar]
- Connor, K.M.; Krah, N.M.; Dennison, R.J.; Aderman, C.M.; Chen, J.; Guerin, K.I.; Sapieha, P.; Stahl, A.; Willett, K.L.; Smith, L.M. Quantification of oxygen-induced retinopathy in the mouse: A model of vessel loss, vessel regrowth and pathological angiogenesis. Nat. Protoc. 2009, 4, 1565–1573. [Google Scholar] [CrossRef]
- Patz, A. Oxygen Studies in Retrolental Fibroplasia. Am. J. Ophthalmol. 1954, 38, 291–308. [Google Scholar] [CrossRef]
- Ashton, N.; Blach, R. Studies on developing retinal vessels VIII. Effect of oxygen on the retinal vessels of the ratling. Br. J. Ophthalmol. 1961, 45, 321–340. [Google Scholar] [CrossRef][Green Version]
- Penn, J.S.; Tolman, B.L.; Lowery, L.A. Variable oxygen exposure causes preretinal neovascularization in the newborn rat. Investig. Ophthalmol. Vis. Sci. 1993, 34, 576–585. [Google Scholar]
- Kubota, Y.; Takubo, K.; Shimizu, T.; Ohno, H.; Kishi, K.; Shibuya, M.; Saya, H.; Suda, T. M-CSF inhibition selectively targets pathological angiogenesis and lymphangiogenesis. J. Cell Biol. 2009, 185, i6. [Google Scholar] [CrossRef]
- Tasman, W.; Brown, G.C.; Schaffer, D.B.; Quinn, G.; Naidoff, M.; Benson, W.E.; Diamond, G. Cryotherapy for Active Retinopathy of Prematurity. Ophthalmology 1986, 93, 580–585. [Google Scholar] [CrossRef]
- Ben-Sira, I.; Nissenkorn, I.; Grunwald, E.; Yassur, Y. Treatment of acute retrolental fibroplasia by cryopexy. Br. J. Ophthalmol. 1980, 64, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: Preliminary results. Pediatrics 1988, 81, 697–706. [Google Scholar]
- Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: Ophthalmological outcomes at 10 years. Arch. Ophthalmol. 2001, 119, 1110–1118. [Google Scholar] [CrossRef]
- Good, W.V.; Hardy, R.J. The multicenter study of Early Treatment for Retinopathy of Prematurity (ETROP). Ophthalmology 2001, 108, 1013–1014. [Google Scholar] [CrossRef]
- Simpson, J.L.; Melia, M.; Yang, M.B.; Buffenn, A.N.; Chiang, M.F.; Lambert, S.R. Current role of cryotherapy in retinopathy of prematurity: A report by the American academy of ophthalmology. Ophthalmology 2012, 119, 873–877. [Google Scholar] [CrossRef]
- McNamara, J.A.; Tasman, W.; Brown, G.C.; Federman, J.L. Laser Photocoagulation for Stage 3+ Retinopathy of Prematurity. Ophthalmology 1991, 98, 576–580. [Google Scholar] [CrossRef]
- Vander, J.F.; Handa, J.; McNamara, J.A.; Trese, M.; Spencer, R.; Repka, M.X.; Rubsamen, P.; Li, H.; Morse, L.S.; Tasman, W.S. Early treatment of posterior retinopathy of prematurity: A controlled trial. Ophthalmology 1997, 104, 1731–1736. [Google Scholar] [CrossRef]
- McNamara, J.A.; Tasman, W.; Vander, J.F.; Brown, G.C. Diode laser photocoagulation for retinopathy of prematurity: Preliminary results. Arch. Ophthalmol. 1992, 110, 1714–1716. [Google Scholar] [CrossRef]
- Landers, M.B.; Toth, C.A.; Semple, H.C.; Morse, L.S. Treatment of Retinopathy of Prematurity with Argon Laser Photocoagulation. Arch. Ophthalmol. 1992, 110, 44–47. [Google Scholar] [CrossRef]
- Shalev, B.; Farr, A.K.; Repka, M.X. Randomized comparison of diode laser photocoagulation versus cryotherapy for threshold retinopathy of prematurity: Seven-year outcome. Am. J. Ophthalmol. 2001, 132, 76–80. [Google Scholar] [CrossRef]
- Ng, E.Y.; Connolly, B.P.; McNamara, J.; Regillo, C.D.; Vander, J.F.; Tasman, W. A comparison of laser photocoagulation with cryotherapy for threshold retinopathy of prematurity at 10 years. Ophthalmology 2002, 109, 928–934. [Google Scholar] [CrossRef]
- Connolly, B.P.; Ng, E.Y.; McNamara, J.A.; Regillo, C.D.; Vander, J.F.; Tasman, W. A comparison of laser photocoagulation with cryotherapy for threshold retinopathy of prematurity at 10 years: Part 2. Refractive outcome. Ophthalmology 2002, 109, 936–941. [Google Scholar] [CrossRef]
- Good, W.V. Early treatment for retinopathy of prematurity cooperative group. Final results of the early treatment for retinopathy of prematurity (ETROP) randomized trial. Trans. Am. Ophthalmol. Soc. 2004, 102, 233–250. [Google Scholar] [PubMed]
- O’Connor, A.R.; Stephenson, T.; Johnson, A.; Tobin, M.J.; Moseley, M.J.; Ratib, S.; Ng, Y.; Fielder, A.R. Long-Term Ophthalmic Outcome of Low Birth Weight Children with and Without Retinopathy of Prematurity. Pediatrics 2002, 109, 12–18. [Google Scholar] [CrossRef]
- Fielder, A.R.; Quinn, G.E. Myopia of prematurity: Nature, nurture, or disease? Br. J. Ophthalmol. 1997, 81, 2–3. [Google Scholar] [CrossRef]
- Houston, S.K.; Wykoff, C.C.; Berrocal, A.M.; Hess, D.J.; Murray, T.G. Laser treatment for retinopathy of prematurity. Lasers Med. Sci. 2013, 28, 683–692. [Google Scholar] [CrossRef]
- Yang, C.-S.; Wang, A.-G.; Shih, Y.-F.; Hsu, W.-M. Long-term biometric optic components of diode laser-treated threshold retinopathy of prematurity at 9 years of age. Acta Ophthalmol. 2013, 91, e276–e282. [Google Scholar] [CrossRef]
- Senger, D.R.; Galli, S.J.; Dvorak, A.M.; Perruzzi, C.A.; Harvey, V.S.; Dvorak, H.F. Tumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science 1983, 219, 983–985. [Google Scholar] [CrossRef]
- Ferrara, N.; Henzel, W.J. Pituitary follicular cells secrete a novel heparin-binding growth factor specific for vascular endothelial cells. Biochem. Biophys. Res. Commun. 1989, 161, 851–858. [Google Scholar] [CrossRef]
- Keck, P.J.; Hauser, S.D.; Krivi, G.; Sanzo, K.; Warren, T.; Feder, J.; Connolly, D.T. Vascular permeability factor, an endothelial cell mitogen related to PDGF. Science 1989, 246, 1309–1312. [Google Scholar] [CrossRef]
- Leung, D.W.; Cachianes, G.; Kuang, W.J.; Goeddel, D.V.; Ferrara, N. Vascular endothelial growth factor is a secreted angiogenic mitogen. Science 1989, 246, 1306–1309. [Google Scholar] [CrossRef] [PubMed]
- Aiello, L.M.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular Endothelial Growth Factor in Ocular Fluid of Patients with Diabetic Retinopathy and Other Retinal Disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Kusaka, S.; Shimojo, H.; Fujikado, T. Simultaneous Analyses of Vitreous Levels of 27 Cytokines in Eyes with Retinopathy of Prematurity. Ophthalmology 2009, 116, 2165–2169. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, E.; Achen, M.G.; Breier, G.; Risau, W. Hypoxia-induced Transcriptional Activation and Increased mRNA Stability of Vascular Endothelial Growth Factor in C6 Glioma Cells. J. Biol. Chem. 1995, 270, 19761–19766. [Google Scholar] [CrossRef]
- Damert, A.; Ikeda, E.; Risau, W. Activator-protein-1 binding potentiates the hypoxia-induciblefactor-1-mediated hypoxia-induced transcriptional activation of vascular-endothelial growth factor expression in C6 glioma cells. Biochem. J. 1997, 327, 419–423. [Google Scholar] [CrossRef]
- Wang, G.L.; Semenza, G.L. Purification and Characterization of Hypoxia-inducible Factor 1. J. Biol. Chem. 1995, 270, 1230–1237. [Google Scholar] [CrossRef]
- Semenza, G.L. Life with Oxygen. Science 2007, 318, 62–64. [Google Scholar] [CrossRef]
- Pugh, C.W.; Ratcliffe, P.J. Regulation of angiogenesis by hypoxia: Role of the HIF system. Nat. Med. 2003, 9, 677–684. [Google Scholar] [CrossRef]
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell 2019, 176, 1248–1264. [Google Scholar] [CrossRef]
- Ferrara, N. Vascular Endothelial Growth Factor: Basic Science and Clinical Progress. Endocr. Rev. 2004, 25, 581–611. [Google Scholar] [CrossRef]
- Shibuya, M.; Claesson-Welsh, L. Signal transduction by VEGF receptors in regulation of angiogenesis and lymphangiogenesis. Exp. Cell Res. 2006, 312, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N. Molecular and biological properties of vascular endothelial growth factor. J. Mol. Med. 1999, 77, 527–543. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, K.; Economides, D.; Soothill, P. Blood gases, pH, and lactate in appropriate- and small-for-gestational-age fetuses. Am. J. Obstet. Gynecol. 1989, 161, 996–1001. [Google Scholar] [CrossRef]
- Stone, J.; Itin, A.; Alon, T.; Pe’Er, J.; Gnessin, H.; Chan-Ling, T.; Keshet, E. Development of retinal vasculature is mediated by hypoxia-induced vascular endothelial growth factor (VEGF) expression by neuroglia. J. Neurosci. 1995, 15, 4738–4747. [Google Scholar] [CrossRef] [PubMed]
- Alon, T.; Hemo, I.; Itin, A.; Pe’Er, J.; Stone, J.; Keshet, E. Vascular endothelial growth factor acts as a survival factor for newly formed retinal vessels and has implications for retinopathy of prematurity. Nat. Med. 1995, 1, 1024–1028. [Google Scholar] [CrossRef]
- Pierce, E.A.; Avery, R.L.; Foley, E.D.; Aiello, L.P.; Smith, L.E. Vascular endothelial growth factor/vascular permeability factor expression in a mouse model of retinal neovascularization. Proc. Natl. Acad. Sci. USA 1995, 92, 905–909. [Google Scholar] [CrossRef]
- Hoppe, G.; Yoon, S.; Gopalan, B.; Savage, A.R.; Brown, R.; Case, K.; Vasanji, A.; Chan, E.R.; Silver, R.B.; Sears, J. Comparative systems pharmacology of HIF stabilization in the prevention of retinopathy of prematurity. Proc. Natl. Acad. Sci. USA 2016, 113, E2516–E2525. [Google Scholar] [CrossRef]
- Kusaka, S.; Shima, C.; Wada, K.; Arahori, H.; Shimojyo, H.; Sato, T.; Fujikado, T. Efficacy of intravitreal injection of bevacizumab for severe retinopathy of prematurity: A pilot study. Br. J. Ophthalmol. 2008, 92, 1450–1455. [Google Scholar] [CrossRef]
- Lalwani, G.A.; Berrocal, A.M.; Murray, T.G.; Buch, M.; Cardone, S.; Hess, D.; Johnson, R.A.; Puliafito, C.A. Off-label use of intravitreal bevacizumab (avastin) for salvage treatment in progressive threshold retinopathy of prematurity. Retina 2008, 28, S13–S18. [Google Scholar] [CrossRef]
- Dalma-Weiszhausz, J.; Martinez-Castellanos, M.A.; Hernandez-Rojas, M.L.; Salazar-Teran, N.; Chan, R.V.P. Antiangiogenic therapy with intravitreal bevacizumab for retinopathy of prematurity. Retina 2008, 28, S19–S25. [Google Scholar] [CrossRef]
- Honda, S.; Hirabayashi, H.; Tsukahara, Y.; Negi, A. Acute contraction of the proliferative membrane after an intravitreal injection of bevacizumab for advanced retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 1061–1063. [Google Scholar] [CrossRef] [PubMed]
- Mintz-Hittner, H.A.; Kennedy, K.A.; Chuang, A.Z. Efficacy of Intravitreal Bevacizumab for Stage 3+ Retinopathy of Prematurity. N. Engl. J. Med. 2011, 364, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.K.; Hubbard, G.B.; Hutchinson, A.K.; Lambert, S.R. Outcomes after intravitreal bevacizumab versus laser photocoagulation for retinopathy of prematurity: A 5-year retrospective analysis. Ophthalmology 2015, 122, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Lepore, D.; Quinn, G.E.; Molle, F.; Baldascino, A.; Orazi, L.; Sammartino, M.; Purcaro, V.; Giannantonio, C.; Papacci, P.; Romagnoli, C. Intravitreal Bevacizumab versus Laser Treatment in Type 1 Retinopathy of Prematurity. Ophthalmology 2014, 121, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Stahl, A.; Lepore, D.; Fielder, A.; Fleck, B.; Reynolds, J.D.; Chiang, M.F.; Li, J.; Liew, M.; Maier, R.; Zhu, Q.; et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): An open-label randomised controlled trial. Lancet 2019, 394, 1551–1559. [Google Scholar] [CrossRef]
- Geloneck, M.M.; Chuang, A.Z.; Clark, W.L.; Hunt, M.G.; Norman, A.A.; Packwood, E.A.; Tawansy, K.A.; Mintz-Hittner, H.A. Refractive Outcomes Following Bevacizumab Monotherapy Compared with Conventional Laser Treatment. JAMA Ophthalmol. 2014, 132, 1327–1333. [Google Scholar] [CrossRef]
- Recchia, F.M.; Capone, A. Contemporary understanding and management of retinopathy of prematurity. Retina 2004, 24, 283–292. [Google Scholar] [CrossRef]
- Wallace, D.K.; Dean, T.W.; Hartnett, M.E.; Kong, L.; Smith, L.E.; Hubbard, G.B.; McGregor, M.L.; Jordan, C.O.; Mantagos, I.S.; Bell, E.F.; et al. A dosing study of bevacizumab for retinopathy of prematurity: Late recurrences and additional treatments. Ophthalmology 2018, 125, 1961–1966. [Google Scholar] [CrossRef]
- Morin, J.; Luu, T.M.; Superstein, R.; Ospina, L.H.; Lefebvre, F.; Simard, M.-N.; Shah, V.; Shah, P.S.; Mb, E.N.K. The Canadian Neonatal Network and the Canadian Neonatal Follow-Up Network Investigators Neurodevelopmental Outcomes Following Bevacizumab Injections for Retinopathy of Prematurity. Pediatrics 2016, 137, e20153218. [Google Scholar] [CrossRef]
- Fan, Y.Y.; Huang, Y.S.; Huang, C.Y.; Hsu, J.F.; Shih, C.P.; Hwang, Y.S.; Yao, T.C.; Lai, C.C.; Wu, W.C. Neurodevelopmental outcomes after intravitreal bevacizumab therapy for retinopathy of prematurity: A prospective case-control study. Ophthalmology 2019, 4, 1–11. [Google Scholar] [CrossRef]
- Rodriguez, S.H.; Peyton, C.; Lewis, K.; Andrews, B.; Greenwald, M.J.; Schreiber, M.D.; Msall, M.E.; Blair, M.P. Neurodevelopmental Outcomes Comparing Bevacizumab to Laser for Type 1 ROP. Ophthalmic Surg. Lasers Imaging Retin. 2019, 50, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Eichmann, A.; Thomas, J.-L. Molecular Parallels between Neural and Vascular Development. Cold Spring Harb. Perspect. Med. 2012, 3, a006551. [Google Scholar] [CrossRef][Green Version]
- Rosenstein, J.M.; Krum, J.M.; Ruhrberg, C. VEGF in the nervous system. Organogenesis 2010, 6, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Zhang, Q.; Fei, P.; Xu, Y.; Lyu, J.; Ji, X.; Peng, J.; Li, Y.; Zhao, P. Ranibizumab injection as primary treatment in patients with retinopathy of prematurity: Anatomic outcomes and influencing factors. Ophthalmology 2017, 124, 1156–1164. [Google Scholar] [CrossRef]
- Vanderveen, D.K.; Melia, M.; Yang, M.B.; Hutchinson, A.K.; Wilson, L.B.; Lambert, S.R. Anti-Vascular Endothelial Growth Factor Therapy for Primary Treatment of Type 1 Retinopathy of Prematurity. Ophthalmology 2017, 124, 619–633. [Google Scholar] [CrossRef]
- Papadopoulos, N.; Martin, J.; Ruan, Q.; Rafique, A.; Rosconi, M.P.; Shi, E.; Pyles, E.A.; Yancopoulos, G.D.; Stahl, N.; Wiegand, S.J. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis 2012, 15, 171–185. [Google Scholar] [CrossRef]
- Carmeliet, P.; Moons, L.; Luttun, A.; Vincenti, V.; Compernolle, V.; De Mol, M.; Wu, Y.; Bono, F.; Devy, L.; Beck, H.; et al. Synergism between vascular endothelial growth factor and placental growth factor contributes to angiogenesis and plasma extravasation in pathological conditions. Nat. Med. 2001, 7, 575–583. [Google Scholar] [CrossRef]
- Takahashi, H.; Shibuya, M. The vascular endothelial growth factor (VEGF)/VEGF receptor system and its role under physiological and pathological conditions. Clin. Sci. 2005, 109, 227–241. [Google Scholar] [CrossRef]
- Sukgen, E.A.; Koçluk, Y. Comparison of clinical outcomes of intravitreal ranibizumab and aflibercept treatment for retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 257, 49–55. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Lien, R.; Wang, N.-K.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C.; Wu, W.-C. Changes in systemic vascular endothelial growth factor levels after intravitreal injection of aflibercept in infants with retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 479–487. [Google Scholar] [CrossRef]
- Owens, W.C.; Owens, E.U. Retrolental Fibroplasia in Premature Infants*. Am. J. Ophthalmol. 1949, 32, 1–21. [Google Scholar] [CrossRef]
- Hittner, H.M.; Godio, L.B.; Rudolph, A.J.; Adams, J.M.; Garcia-Prats, J.A.; Friedman, Z.; Kautz, J.A.; Monaco, W.A. Retrolental Fibroplasia: Efficacy of Vitamin E in a Double-Blind Clinical Study of Preterm Infants. N. Engl. J. Med. 1981, 305, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Phelps, D.L.; Rosenbaum, A.L.; Isenberg, S.J.; Leake, R.D.; Dorey, F.J. Tocopherol efficacy and safety for preventing retinopathy of prematurity: A randomized, controlled, double-masked trial. Pediatrics 1987, 79, 489–500. [Google Scholar] [PubMed]
- Brion, L.P.; Bell, E.F.; Raghuveer, T.S. Vitamin E supplementation for prevention of morbidity and mortality in preterm infants. Cochrane Database Syst. Rev. 2003, CD003665. [Google Scholar] [CrossRef] [PubMed]
- Raju, T.N.; Langenberg, P.; Bhutani, V.; Quinn, G.E. Vitamin E prophylaxis to reduce retinopathy of prematurity: A reappraisal of published trials. J. Pediatr. 1997, 131, 844–850. [Google Scholar] [CrossRef]
- Johnson, L.; Quinn, G.E.; Abbasi, S.; Otis, C.; Goldstein, D.; Sacks, L.; Porat, R.; Fong, E.; Delivoria-Papadopoulos, M.; Peckham, G.; et al. Effect of sustained pharmacologic vitamin E levels on incidence and severity of retinopathy of prematurity: A controlled clinical trial. J. Pediatr. 1989, 114, 827–838. [Google Scholar] [CrossRef]
- Finer, N.N.; Peters, K.L.; Hayek, Z.; Merkel, C.L. Vitamin E and necrotizing enterocolitis. Pediatrics 1984, 73, 387–393. [Google Scholar]
- Gu, X.; El-Remessy, A.B.; Brooks, S.E.; Al-Shabrawey, M.; Tsai, N.-T.; Caldwell, R.B. Hyperoxia induces retinal vascular endothelial cell apoptosis through formation of peroxynitrite. Am. J. Physiol. Physiol. 2003, 285, C546–C554. [Google Scholar] [CrossRef]
- Okuno, Y.; Nakamura-Ishizu, A.; Otsu, K.; Suda, T.; Kubota, Y. Pathological neoangiogenesis depends on oxidative stress regulation by ATM. Nat. Med. 2012, 18, 1208–1216. [Google Scholar] [CrossRef]
- Kojima, H.; Otani, A.; Oishi, A.; Makiyama, Y.; Nakagawa, S.; Yoshimura, N. Granulocyte colony-stimulating factor attenuates oxidative stress–induced apoptosis in vascular endothelial cells and exhibits functional and morphologic protective effect in oxygen-induced retinopathy. Blood 2011, 117, 1091–1100. [Google Scholar] [CrossRef]
- Kim, Y.-W.; Byzova, T.V. Oxidative stress in angiogenesis and vascular disease. Blood 2014, 123, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Nassi, P.; Ponziani, V.; Becatti, M.; Galvan, P.; Donzelli, G. Anti-oxidant enzymes and related elements in term and preterm newborns. Pediatr. Int. 2009, 51, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Buhimschi, I.A.; Buhimschi, C.S.; Pupkin, M.; Weiner, C.P. Beneficial impact of term labor: Nonenzymatic antioxidant reserve in the human fetus. Am. J. Obstet. Gynecol. 2003, 189, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Muller, D.P.R. Vitamin E therapy in retinopathy of prematurity. Eye 1992, 6, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Soghier, L.M.; Brion, L.P. Cysteine, cystine or N-acetylcysteine supplementation in parenterally fed neonates. Cochrane Database Syst. Rev. 2006, CD004869. [Google Scholar] [CrossRef] [PubMed]
- Manzoni, P.; Guardione, R.; Bonetti, P.; Priolo, C.; Maestri, A.; Mansoldo, C.; Mostert, M.; Anselmetti, G.; Sardei, D.; Bellettato, M.; et al. Lutein and Zeaxanthin Supplementation in Preterm Very Low-Birth-Weight Neonates in Neonatal Intensive Care Units: A Multicenter Randomized Controlled Trial. Am. J. Perinatol. 2012, 30, 025–032. [Google Scholar] [CrossRef]
- Reynolds, J.D.; Hardy, R.J.; Kennedy, K.A.; Spencer, R.; Van Heuven, W.; Fielder, A.R. Lack of Efficacy of Light Reduction in Preventing Retinopathy of Prematurity. N. Engl. J. Med. 1998, 338, 1572–1576. [Google Scholar] [CrossRef]
- Qureshi, M.J.; Kumar, M. D-Penicillamine for preventing retinopathy of prematurity in preterm infants. Cochrane Database Syst. Rev. 2013, 2013, CD001073. [Google Scholar] [CrossRef]
- Tandon, M.; Dutta, S.; Dogra, M.R.; Brar, G.S. Oral D-penicillamine for the prevention of retinopathy of prematurity in very low birth weight infants: A randomized, placebo-controlled trial. Acta Paediatr. 2010, 99, 1324–1328. [Google Scholar] [CrossRef]
- Parad, R.B.; Allred, E.N.; Rosenfeld, W.N.; Davis, J.M. Reduction of Retinopathy of Prematurity in Extremely Low Gestational Age Newborns Treated with Recombinant Human Cu/Zn Superoxide Dismutase. Neonatology 2012, 102, 139–144. [Google Scholar] [CrossRef]
- Beharry, K.D.; Cai, C.L.; Siddiqui, F.; Chowdhury, S.; D’Agrosa, C.; Valencia, G.B.; Aranda, J.V. Comparative Effects of Coenzyme Q10 or n-3 Polyunsaturated Fatty Acid Supplementation on Retinal Angiogenesis in a Rat Model of Oxygen-Induced Retinopathy. Antioxidants 2018, 7, 160. [Google Scholar] [CrossRef] [PubMed]
- Akdogan, M.; Polat, O. Clinical Efficacy of Topical CoQ10 and Vitamin-E Eye-drop in Retinopathy of Prematurity. Med. Hypothesis. Discov. Innov. Ophthalmol. 2019, 8, 291–297. [Google Scholar] [PubMed]
- L’Abbe, M.R.; Friel, J.K. Superoxide Dismutase and Glutathione Peroxidase Content of Human Milk from Mothers of Premature and Full-Term Infants During the First 3 Months of Lactation. J. Pediatr. Gastroenterol. Nutr. 2000, 31, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Friel, J.K.; Martin, S.M.; Langdon, M.; Herzberg, G.R.; Buettner, G.R. Milk from Mothers of Both Premature and Full-Term Infants Provides Better Antioxidant Protection than Does Infant Formula. Pediatr. Res. 2002, 51, 612–618. [Google Scholar] [CrossRef]
- Mactier, H.; Weaver, L.T. Vitamin A and preterm infants: What we know, what we don’t know, and what we need to know. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, 103–108. [Google Scholar] [CrossRef]
- Shenai, J.P.; Chytil, F.; Stahlman, M.T. Liver Vitamin A Reserves of Very Low Birth Weight Neonates. Pediatr. Res. 1985, 19, 892–893. [Google Scholar] [CrossRef]
- Shenai, J.P.; Chytil, F.; Jhaveri, A.; Stahlman, M.T. Plasma vitamin A and retinol-binding protein in premature and term neonates. J. Pediatr. 1981, 99, 302–305. [Google Scholar] [CrossRef]
- Garofoli, F.; Barillà, D.; Angelini, M.; Mazzucchelli, I.; De Silvestri, A.; Guagliano, R.; Decembrino, L.; Tzialla, C. Oral vitamin A supplementation for ROP prevention in VLBW preterm infants. Ital. J. Pediatr. 2020, 46, 77. [Google Scholar] [CrossRef]
- Sun, H.; Cheng, R.; Wang, Z. Early vitamin a supplementation improves the outcome of retinopathy of prematurity in extremely preterm infants. Retina 2020, 40, 1176–1184. [Google Scholar] [CrossRef]
- Biesalski, H.K.; Nohr, D. Importance of vitamin-A for lung function and development. Mol. Asp. Med. 2003, 24, 431–440. [Google Scholar] [CrossRef]
- Tyson, J.E.; Wright, L.L.; Oh, W.; Kennedy, K.A.; Mele, L.; Ehrenkranz, R.A.; Stoll, B.J.; Lemons, J.A.; Stevenson, D.K.; Bauer, C.R.; et al. Vitamin A Supplementation for Extremely-Low-Birth-Weight Infants. N. Engl. J. Med. 1999, 340, 1962–1968. [Google Scholar] [CrossRef] [PubMed]
- Shenai, J.P.; Kennedy, K.A.; Chytil, F.; Stahlman, M.T. Clinical trial of vitamin A supplementation in infants susceptible to bronchopulmonary dysplasia. J. Pediatr. 1987, 111, 269–277. [Google Scholar] [CrossRef]
- Araki, S.; Kato, S.; Namba, F.; Ota, E. Vitamin A to prevent bronchopulmonary dysplasia in extremely low birth weight infants: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0207730. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.U.; Miras-Baldo, M.; Jerez-Calero, A.; Narbona-López, E. Effectiveness of Vitamin A in the Prevention of Complications of Prematurity. Pediatr. Neonatol. 2014, 55, 358–362. [Google Scholar] [CrossRef]
- Lingen, M.W.; Polverini, P.J.; Bouck, N.P. Inhibition of squamous cell carcinoma angiogenesis by direct interaction of retinoic acid with endothelial cells. Lab. Investig. 1996, 74, 476–483. [Google Scholar]
- Hoffmann, S.; Rockenstein, A.; Ramaswamy, A.; Celik, I.; Wunderlich, A.; Lingelbach, S.; Hofbauer, L.C.; Zielke, A. Retinoic acid inhibits angiogenesis and tumor growth of thyroid cancer cells. Mol. Cell. Endocrinol. 2007, 264, 74–81. [Google Scholar] [CrossRef]
- Ozkan, H.; Duman, N.; Kumral, A.; Kasap, B.; Ozer, E.A.; Lebe, B.; Yaman, A.; Berk, T.; Yilmaz, O.; Ozer, E. Inhibition of vascular endothelial growth factor-induced retinal neovascularization by retinoic acid in experimental retinopathy of prematurity. Physiol. Res. 2005, 55, 267–275. [Google Scholar]
- Pal, S.; Iruela-Arispe, M.; Harvey, V.; Zeng, H.; Nagy, J.A.; Dvorak, H.F.; Mukhopadhyay, D. Retinoic Acid Selectively Inhibits the Vascular Permeabilizing Effect of VPF/VEGF, an Early Step in the Angiogenic Cascade. Microvasc. Res. 2000, 60, 112–120. [Google Scholar] [CrossRef]
- Reese, A.B.; Blodi, F.C.; Locke, J.C.; Silverman, W.A.; Day, R.L. Results of use of corticotropin (ACTH) in treatment of retrolental fibroplasia. Arch. Ophthalmol. 1952, 47, 551–555. [Google Scholar] [CrossRef]
- Gilstrap, L.C. Effect of corticosteroids for fetal maturation on perinatal outcomes. NIH consensus development panel on the effect of corticosteroids for fetal maturation on perinatal outcomes. JAMA 1995, 273, 413–418. [Google Scholar] [CrossRef]
- Mesiano, S.; Jaffe, R.B. Developmental and Functional Biology of the Primate Fetal Adrenal Cortex. Endocr. Rev. 1997, 18, 378–403. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, E.; Montman, R.; Watterberg, K. ACTH and cortisol response to critical illness in term and late preterm newborns. J. Perinatol. 2008, 28, 797–802. [Google Scholar] [CrossRef]
- Niwa, F.; Kawai, M.; Kanazawa, H.; Iwanaga, K.; Matsukura, T.; Shibata, M.; Hasegawa, T.; Heike, T. Limited response to CRH stimulation tests at 2 weeks of age in preterm infants born at less than 30 weeks of gestational age. Clin. Endocrinol. 2013, 78, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M. Late-onset circulatory collapse of prematurity. Pediatr. Int. 2017, 59, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Thompson, E. Gene regulation by the glucocorticoid receptor: Structure:function relationship. J. Steroid Biochem. Mol. Biol. 2005, 94, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Jonat, C.; Rahmsdorf, H.J.; Park, K.-K.; Cato, A.C.; Gebel, S.; Ponta, H.; Herrlich, P. Antitumor promotion and antiinflammation: Down-modulation of AP-1 (Fos/Jun) activity by glucocorticoid hormone. Cell 1990, 62, 1189–1204. [Google Scholar] [CrossRef]
- Tsurufuji, S.; Sugio, K.; Takemasa, F. The role of glucocorticoid receptor and gene expression in the anti-inflammatory action of dexamethasone. Nat. Cell Biol. 1979, 280, 408–410. [Google Scholar] [CrossRef]
- Hoekstra, M.; Ye, D.; Hildebrand, R.B.; Zhao, Y.; Lammers, B.; Stitzinger, M.; Kuiper, J.; Van Berkel, T.J.C.; Van Eck, M. Scavenger receptor class B type I-mediated uptake of serum cholesterol is essential for optimal adrenal glucocorticoid production. J. Lipid Res. 2009, 50, 1039–1046. [Google Scholar] [CrossRef]
- Console, V.; Gagliardi, L.; De Giorgi, A.; De Ponti, E. Retinopathy of prematurity and antenatal corticosteroids. The Italian ROP Study Group. Acta. Biomed. Ateneo. Parm. 1997, 68, 75–79. [Google Scholar]
- Higgins, R.D.; Mendelsohn, A.L.; Defeo, M.J.; Ucsel, R.; Hendricks-Munoz, K.D. Antenatal dexamethasone and decreased severity of retinopathy of prematurity. Arch. Ophthalmol. 1998, 116, 601–605. [Google Scholar] [CrossRef]
- Doyle, L.W.; Cheong, J.L.; Ehrenkranz, R.A.; Halliday, H.L. Late (>7 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst. Rev. 2017, 10, CD001145. [Google Scholar] [CrossRef]
- Doyle, L.W.; Cheong, J.L.; Ehrenkranz, R.A.; Halliday, H.L. Early (<8 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst. Rev. 2017, 10, CD001146. [Google Scholar] [CrossRef]
- Baud, O.; Maury, L.; LeBail, F.; Ramful, D.; El Moussawi, F.; Nicaise, C.; Zupan-Simunek, V.; Coursol, A.; Beuchée, A.; Bolot, P.; et al. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): A double-blind, placebo-controlled, multicentre, randomised trial. Lancet 2016, 387, 1827–1836. [Google Scholar] [CrossRef]
- Jelkmann, W. Erythropoietin: Structure, control of production, and function. Physiol. Rev. 1992, 72, 449–489. [Google Scholar] [CrossRef]
- Watanabe, D.; Suzuma, K.; Matsui, S.; Kurimoto, M.; Kiryu, J.; Kita, M.; Suzuma, I.; Ohashi, H.; Ojima, T.; Murakami, T.; et al. Erythropoietin as a Retinal Angiogenic Factor in Proliferative Diabetic Retinopathy. N. Engl. J. Med. 2005, 353, 782–792. [Google Scholar] [CrossRef]
- Semenza, G.L.; Wang, G.L. A nuclear factor induced by hypoxia via de novo protein synthesis binds to the human erythropoietin gene enhancer at a site required for transcriptional activation. Mol. Cell. Biol. 1992, 12, 5447–5454. [Google Scholar] [CrossRef]
- Rex, T.S.; Allocca, M.; Domenici, L.; Surace, E.M.; Maguire, A.M.; Lyubarsky, A.; Cellerino, A.; Bennett, J.; Auricchio, A. Systemic but not intraocular Epo Gene Transfer Protects the Retina from Light-and Genetic-Induced Degeneration. Mol. Ther. 2004, 10, 855–861. [Google Scholar] [CrossRef]
- Junk, A.K.; Mammis, A.; Savitz, S.I.; Singh, M.; Roth, S.; Malhotra, S.; Rosenbaum, P.S.; Cerami, A.; Brines, M.; Rosenbaum, D.M. Erythropoietin administration protects retinal neurons from acute ischemia-reperfusion injury. Proc. Natl. Acad. Sci. USA 2002, 99, 10659–10664. [Google Scholar] [CrossRef]
- Anagnostou, A.; Lee, E.S.; Kessimian, N.; Levinson, R.; Steiner, M. Erythropoietin has a mitogenic and positive chemotactic effect on endothelial cells. Proc. Natl. Acad. Sci. USA 1990, 87, 5978–5982. [Google Scholar] [CrossRef]
- Chen, J.; Connor, K.M.; Aderman, C.M.; Smith, L. Erythropoietin deficiency decreases vascular stability in mice. J. Clin. Investig. 2008, 118, 526–533. [Google Scholar] [CrossRef]
- Chen, J.; Connor, K.M.; Aderman, C.M.; Willett, K.L.; Aspegren, O.P.; Smith, L.E.H. Suppression of Retinal Neovascularization by Erythropoietin siRNA in a Mouse Model of Proliferative Retinopathy. Investig. Opthalmol. Vis. Sci. 2009, 50, 1329–1335. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, H.; Jiang, Y.; Hartnett, M.E. VEGFA activates erythropoietin receptor and enhances VEGFR2-mediated pathological angiogenesis. Am. J. Pathol. 2014, 184, 1230–1239. [Google Scholar] [CrossRef]
- Suk, K.K.; Dunbar, J.A.; Liu, A.; Daher, N.S.; Leng, C.K.; Leng, J.K.; Lim, P.; Weller, S.; Fayard, E. Human recombinant erythropoietin and the incidence of retinopathy of prematurity: A multiple regression model. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2008, 12, 233–238. [Google Scholar] [CrossRef]
- Brown, M.S.; Barón, A.E.; France, E.K.; Hamman, R.F. Association Between Higher Cumulative Doses of Recombinant Erythropoietin and Risk for Retinopathy of Prematurity. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2006, 10, 143–149. [Google Scholar] [CrossRef]
- Romagnoli, C.; Zecca, E.; Gallini, F.; Girlando, P.; Zuppa, A.A. Do recombinant human erythropoietin and iron supplementation increase the risk of retinopathy of prematurity? Eur. J. Nucl. Med. Mol. Imaging 2000, 159, 627–628. [Google Scholar] [CrossRef]
- Ohls, R.K.; Christensen, R.D.; Kamath-Rayne, B.D.; Rosenberg, A.; Wiedmeier, S.E.; Roohi, M.; Lacy, C.B.; Lambert, D.K.; Burnett, J.J.; Pruckler, B.; et al. A Randomized, Masked, Placebo-Controlled Study of Darbepoetin Alfa in Preterm Infants. Pediatrics 2013, 132, e119–e127. [Google Scholar] [CrossRef]
- Juul, S.E.; Comstock, B.A.; Wadhawan, R.; Mayock, D.E.; Courtney, S.E.; Robinson, T.; Ahmad, K.A.; Bendel-Stenzel, E.; Baserga, M.; LaGamma, E.F.; et al. A Randomized Trial of Erythropoietin for Neuroprotection in Preterm Infants. N. Engl. J. Med. 2020, 382, 233–243. [Google Scholar] [CrossRef]
- Ohlsson, A.; Aher, S.M. Early erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst. Rev. 2014, 26, CD004863. [Google Scholar] [CrossRef]
- Aher, S.M.; Ohlsson, A. Late erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst. Rev. 2014, 23, CD004868. [Google Scholar] [CrossRef]
- Smith, L.E.H.; Kopchick, J.J.; Chen, W.; Knapp, J.; Kinose, F.; Daley, D.; Foley, E.; Smith, R.G.; Schaeffer, J.M. Essential Role of Growth Hormone in Ischemia-Induced Retinal Neovascularization. Science 1997, 276, 1706–1709. [Google Scholar] [CrossRef]
- Smith, L.E.H.; Shen, W.; Perruzzi, C.; Soker, S.; Kinose, F.; Xu, X.; Robinson, G.; Driver, S.; Bischoff, J.; Zhang, B.; et al. Regulation of vascular endothelial growth factor-dependent retinal neovascularization by insulin-like growth factor-1 receptor. Nat. Med. 1999, 5, 1390–1395. [Google Scholar] [CrossRef]
- Hellstrom, A.; Perruzzi, C.; Ju, M.; Engström, E.; Hård, A.-L.; Liu, J.-L.; Albertsson-Wikland, K.; Carlsson, B.; Niklasson, A.; Sjödell, L.; et al. Low IGF-I suppresses VEGF-survival signaling in retinal endothelial cells: Direct correlation with clinical retinopathy of prematurity. Proc. Natl. Acad. Sci. USA 2001, 98, 5804–5808. [Google Scholar] [CrossRef]
- Löfqvist, C.; Chen, J.; Connor, K.M.; Smith, A.C.H.; Aderman, C.M.; Liu, N.; Pintar, J.E.; Ludwig, T.; Hellström, A.; Smith, L.E.H. IGFBP3 suppresses retinopathy through suppression of oxygen-induced vessel loss and promotion of vascular regrowth. Proc. Natl. Acad. Sci. USA 2007, 104, 10589–10594. [Google Scholar] [CrossRef]
- Hansen-Pupp, I.; Hellström-Westas, L.; Cilio, C.M.; Andersson, S.; Fellman, V.; Ley, D. Inflammation at birth and the insulin-like growth factor system in very preterm infants. Acta Paediatr. Int. J. Paediatr. 2007, 96, 830–836. [Google Scholar] [CrossRef]
- Ley, D.; Hansen-Pupp, I.; Niklasson, A.; Domellöf, M.; Friberg, L.E.; Borg, J.; Löfqvist, C.; Hellgren, G.; Smith, L.E.H.; Hård, A.-L.; et al. Longitudinal infusion of a complex of insulin-like growth factor-I and IGF-binding protein-3 in five preterm infants: Pharmacokinetics and short-term safety. Pediatr. Res. 2013, 73, 68–74. [Google Scholar] [CrossRef]
- Sugioka, K.; Saito, A.; Kusaka, S.; Kuniyoshi, K.; Shimomura, Y. Identification of vitreous proteins in retinopathy of prematurity. Biochem. Biophys. Res. Commun. 2017, 488, 483–488. [Google Scholar] [CrossRef]
- Wang, Z.; Dabrosin, C.; Yin, X.; Fuster, M.M.; Arreola, A.; Rathmell, W.K.; Generali, D.; Nagaraju, G.P.; El-Rayes, B.; Ribatti, D.; et al. Broad targeting of angiogenesis for cancer prevention and therapy. Semin. Cancer Biol. 2015, 35, S224–S243. [Google Scholar] [CrossRef]
- Nakao, S.; Kuwano, T.; Tsutsumi-Miyahara, C.; Ueda, S.; Kimura, Y.N.; Hamano, S.; Sonoda, K.; Saijo, Y.; Nukiwa, T.; Strieter, R.M.; et al. Infiltration of COX-2-expressing macrophages is a prerequisite for IL-1 beta-induced neovascularization and tumor growth. J. Clin. Investig. 2005, 115, 2979–2991. [Google Scholar] [CrossRef]
- Simmons, D.L.; Botting, R.M.; Hla, T. Cyclooxygenase Isozymes: The Biology of Prostaglandin Synthesis and Inhibition. Pharmacol. Rev. 2004, 56, 387–437. [Google Scholar] [CrossRef]
- Hyde, C.; Missailidis, S. Inhibition of arachidonic acid metabolism and its implication on cell proliferation and tumour-angiogenesis. Int. Immunopharmacol. 2009, 9, 701–715. [Google Scholar] [CrossRef]
- Nandgaonkar, B.N.; Rotschild, T.; Yu, K.; Higgins, R.D. Indomethacin improves oxygen-induced retinopathy in the mouse. Pediatr. Res. 1999, 46, 184–188. [Google Scholar] [CrossRef][Green Version]
- Sennlaub, F.; Valamanesh, F.; Vazquez-Tello, A.; El-Asrar, A.; Checchin, D.; Brault, S.; Gobeil, F.; Beauchamp, M.; Mwaikambo, B.; Courtois, Y.; et al. Cyclooxygenase-2 in Human and Experimental Ischemic Proliferative Retinopathy. Circulation 2003, 108, 198–204. [Google Scholar] [CrossRef]
- Yanni, S.E.; Barnett, J.M.; Clark, M.L.; Penn, J.S. The Role of PGE2Receptor EP4in Pathologic Ocular Angiogenesis. Investig. Opthalmol. Vis. Sci. 2009, 50, 5479–5486. [Google Scholar] [CrossRef]
- Gersony, W.M.; Peckham, G.J.; Ellison, R.C.; Miettinen, O.S.; Nadas, A.S. Effects of indomethacin in premature infants with patent ductus arteriosus: Results of a national collaborative study. J. Pediatr. 1983, 102, 895–906. [Google Scholar] [CrossRef]
- Bandstra, E.S.; Montalvo, B.M.; Goldberg, R.N.; Pacheco, I.; Ferrer, P.L.; Flynn, J.; Gregorios, J.B.; Bancalari, E. Prophylactic indomethacin for prevention of intraventricular hemorrhage in premature infants. Pediatrics 1988, 82, 533–542. [Google Scholar]
- Bolling, J.; Feman, S.S.; Mellander, M.; Cotton, R. The Influence of Indomethacin on Retinopathy of Prematurity. Am. J. Ophthalmol. 1983, 96, 254–255. [Google Scholar] [CrossRef]
- Schmidt, B.; Davis, P.; Moddemann, D.; Ohlsson, A.; Roberts, R.S.; Saigal, S.; Solimano, A.; Vincer, M.; Wright, L.L. Long-Term Effects of Indomethacin Prophylaxis in Extremely-Low-Birth-Weight Infants. N. Engl. J. Med. 2001, 344, 1966–1972. [Google Scholar] [CrossRef]
- Jegatheesan, P.; Ianus, V.; Buchh, B.; Yoon, G.; Chorne, N.; Ewig, A.; Lin, E.; Fields, S.; Moon-Grady, A.; Tacy, T.; et al. Increased Indomethacin Dosing for Persistent Patent Ductus Arteriosus in Preterm Infants: A Multicenter, Randomized, Controlled Trial. J. Pediatr. 2008, 153, 183–189. [Google Scholar] [CrossRef]
- Aranda, J.V.; Clyman, R.; Cox, B.; Van Overmeire, B.; Wozniak, P.; Sosenko, I.; Carlo, W.A.; Ward, R.M.; Shalwitz, R.; Baggs, G.; et al. A Randomized, Double-Blind, Placebo-Controlled Trial on Intravenous Ibuprofen L-Lysine for the Early Closure of Nonsymptomatic Patent Ductus Arteriosus within 72 Hours of Birth in Extremely Low-Birth-Weight Infants. Am. J. Perinatol. 2008, 26, 235–245. [Google Scholar] [CrossRef]
- Clyman, R.I.; Liebowitz, M.; Kaempf, J.; Erdeve, O.; Bulbul, A.; Håkansson, S.; Lindqvist, J.; Farooqi, A.; Katheria, A.; Sauberan, J.; et al. PDA-TOLERATE Trial: An Exploratory Randomized Controlled Trial of Treatment of Moderate-to-Large Patent Ductus Arteriosus at 1 Week of Age. J. Pediatr. 2019, 205, 41–48. [Google Scholar] [CrossRef]
- Dani, C.; Bertini, G.; Reali, M.F.; Murru, P.; Fabris, C.; Vangi, V.; Rubaltelli, F.F. Prophylaxis of patent ductus arteriosus with ibuprofen in preterm infants. Acta Paediatr. 2000, 89, 1369–1374. [Google Scholar] [CrossRef] [PubMed]
- Avila-Vazquez, M.; Maffrand, R.; Sosa, M.; Franco, M.; De Alvarez, B.V.; Cafferata, M.L.; Bergel, E. Treatment of Retinopathy of Prematurity with topical ketorolac tromethamine: A preliminary study. BMC Pediatr. 2004, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Giannantonio, C.; Papacci, P.; Purcaro, V.; Cota, F.; Tesfagabir, M.G.; Molle, F.; Lepore, D.; Baldascino, A.; Romagnoli, C. Effectiveness of Ketorolac Tromethamine in Prevention of Severe Retinopathy of Prematurity. J. Pediatr. Ophthalmol. Strabismus 2010, 48, 247–251. [Google Scholar] [CrossRef] [PubMed]
- SanGiovanni, J.P.; Chew, E.Y. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog. Retin. Eye Res. 2005, 24, 87–138. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Polyunsaturated fatty acids and inflammation. Prostaglandins Leukot. Essent. Fat. Acids 2006, 75, 197–202. [Google Scholar] [CrossRef]
- Connor, K.M.; SanGiovanni, J.P.; Lofqvist, C.; Aderman, C.M.; Chen, J.; Higuchi, A.; Hong, S.; Pravda, E.A.; Majchrzak, S.; Carper, D.; et al. Increased dietary intake of ω-3-polyunsaturated fatty acids reduces pathological retinal angiogenesis. Nat. Med. 2007, 13, 868–873. [Google Scholar] [CrossRef]
- Sapieha, P.; Stahl, A.; Chen, J.; Seaward, M.R.; Willett, K.L.; Krah, N.M.; Dennison, R.J.; Connor, K.M.; Aderman, C.M.; Liclican, E.; et al. 5-Lipoxygenase metabolite 4-HDHA is a mediator of the antiangiogenic effect of ω-3 polyunsaturated fatty acids. Sci. Transl. Med. 2011, 3, 69ra12. [Google Scholar] [CrossRef]
- Beken, S.; Dilli, D.; Fettah, N.D.; Kabataş, E.U.; Zenciroǧlu, A.; Okumuş, N. The influence of fish-oil lipid emulsions on retinopathy of prematurity in very low birth weight infants: A randomized controlled trial. Early Hum. Dev. 2014, 90, 27–31. [Google Scholar] [CrossRef]
- Khalesi, N.; Bordbar, A.; Khosravi, N.; Kabirian, M.; Karimi, A. The Efficacy of Omega-3 Supplement on Prevention of Retinopathy of Prematurity in Premature Infants: A Randomized Double-blinded Controlled trial. Curr. Pharm. Des. 2018, 24, 1845–1848. [Google Scholar] [CrossRef]
- Pawlik, D.; Lauterbach, R.; Walczak, M.; Hurkała, J.; Sherman, M.P. Fish-oil fat emulsion supplementation reduces the risk of retinopathy in very low birth weight infants: A prospective, randomized study. J. Parenter. Enter. Nutr. 2014, 38, 711–716. [Google Scholar] [CrossRef]
- Najm, S.; Löfqvist, C.; Hellgren, G.; Engström, E.; Lundgren, P.; Hård, A.-L.; Lapillonne, A.; Sävman, K.; Nilsson, A.K.; Andersson, M.X.; et al. Effects of a lipid emulsion containing fish oil on polyunsaturated fatty acid profiles, growth and morbidities in extremely premature infants: A randomized controlled trial. Clin. Nutr. ESPEN 2017, 20, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Löfqvist, C.A.; Najm, S.; Hellgren, G.; Engström, E.; Sävman, K.; Nilsson, A.K.; Andersson, M.X.; Hård, A.-L.; Smith, L.E.H.; Hellström, A. Association of retinopathy of prematurity with low levels of arachidonic acid. JAMA Ophthalmol. 2018, 136, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Ricci, B.; Calogero, G.; Caprilli, A.; Quaranta-Leoni, F.M. Reduced severity of oxygen-induced retinopathy in the newborn rat after topical administration of timolol maleate—A preliminary study. Doc. Ophthalmol. 1991, 77, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Ricci, B.; Minicucci, G.; Manfredi, A.; Santo, A. Oxygen-induced retinopathy in the newborn rat: Effects of hyperbarism and topical administration of timolol maleate. Graefe’s Arch. Clin. Exp. Ophthalmol. 1995, 233, 226–230. [Google Scholar] [CrossRef]
- Lutgendorf, S.K.; Cole, S.; Costanzo, E.; Bradley, S.; Coffin, J.; Jabbari, S.; Rainwater, K.; Ritchie, J.M.; Yang, M.; Sood, A.K. Stress-related mediators stimulate vascular endothelial growth factor secretion by two ovarian cancer cell lines. Clin. Cancer Res. 2003, 9, 4514–4521. [Google Scholar]
- Léauté-Labrèze, C.; De La Roque, E.D.; Hubiche, T.; Boralevi, F.; Thambo, J.-B.; Taieb, A. Propranolol for Severe Hemangiomas of Infancy. N. Engl. J. Med. 2008, 358, 2649–2651. [Google Scholar] [CrossRef]
- Weil, J.; Benndorf, R.; Fredersdorf, S.; Griese, D.P.; Eschenhagen, T. Norepinephrine Upregulates Vascular Endothelial Growth Factor in Rat Cardiac Myocytes by a Paracrine Mechanism. Angiogenesis 2003, 6, 303–309. [Google Scholar] [CrossRef]
- Yang, E.V.; Sood, A.K.; Chen, M.; Li, Y.; Eubank, T.D.; Marsh, C.B.; Jewell, S.; Flavahan, N.A.; Morrison, C.; Yeh, P.-E.; et al. Norepinephrine Up-regulates the Expression of Vascular Endothelial Growth Factor, Matrix Metalloproteinase (MMP)-2, and MMP-9 in Nasopharyngeal Carcinoma Tumor Cells. Cancer Res. 2006, 66, 10357–10364. [Google Scholar] [CrossRef]
- Martini, D.; Monte, M.D.; Ristori, C.; Cupisti, E.; Mei, S.; Fiorini, P.; Filippi, L.; Bagnoli, P. Antiangiogenic effects of β2-adrenergic receptor blockade in a mouse model of oxygen-induced retinopathy. J. Neurochem. 2011, 119, 1317–1329. [Google Scholar] [CrossRef]
- Ristori, C.; Filippi, L.; Monte, M.D.; Martini, D.; Cammalleri, M.; Fortunato, P.; La Marca, G.; Fiorini, P.; Bagnoli, P. Role of the Adrenergic System in a Mouse Model of Oxygen-Induced Retinopathy: Antiangiogenic Effects of β-Adrenoreceptor Blockade. Investig. Opthalmol. Vis. Sci. 2011, 52, 155–170. [Google Scholar] [CrossRef]
- Ozturk, M.A.; Korkmaz, L. The efficacy of propranolol in very preterm infants at the risk of retinopathy of prematurity: Which newborn and when? Int. Ophthalmol. 2018, 39, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, L.; Baştuğ, O.; Ozdemir, A.; Korkut, S.; Karaca, C.; Akin, M.A.; Gunes, T.; Kurtoglu, S.; Ozturk, M.A. The Efficacy of Propranolol in Retinopathy of Prematurity and its Correlation with the Platelet Mass Index. Curr. Eye Res. 2016, 42, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Makhoul, I.R.; Peleg, O.; Miller, B.; Bar-Oz, B.; Kochavi, O.; Mechoulam, H.; Mezer, E.; Ulanovsky, I.; Smolkin, T.; Yahalom, C.; et al. Oral propranolol versus placebo for retinopathy of prematurity: A pilot, randomised, double-blind prospective study. Arch. Dis. Child. 2013, 98, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Bancalari, A.; Schade, R.; Muñoz, T.; Lazcano, C.; Parada, R.; Peña, R. Oral propranolol in early stages of retinopathy of prematurity. J. Périnat. Med. 2016, 44, 499–503. [Google Scholar] [CrossRef]
- Filippi, L.; Cavallaro, G.; Bagnoli, P.; Monte, M.D.; Fiorini, P.; Donzelli, G.; Tinelli, F.; Araimo, G.; Cristofori, G.; La Marca, G.; et al. Oral Propranolol for Retinopathy of Prematurity: Risks, Safety Concerns, and Perspectives. J. Pediatr. 2013, 163, 1570–1577.e6. [Google Scholar] [CrossRef]
- Filippi, L.; Cavallaro, G.; Bagnoli, P.; Monte, M.D.; Fiorini, P.; Berti, E.; Padrini, L.; Donzelli, G.; Araimo, G.; Cristofori, G.; et al. Propranolol 0.1% eye micro-drops in newborns with retinopathy of prematurity: A pilot clinical trial. Pediatr. Res. 2017, 81, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Cavallaro, G.; Berti, E.; Padrini, L.; Araimo, G.; Regiroli, G.; Raffaeli, G.; Bozzetti, V.; Tagliabue, P.; Tomasini, B.; et al. Propranolol 0.2% Eye Micro-Drops for Retinopathy of Prematurity: A Prospective Phase IIB Study. Front. Pediatr. 2019, 7, 180. [Google Scholar] [CrossRef]
- Matsui, T.; Amano, M.; Yamamoto, T.; Chihara, K.; Nakafuku, M.; Ito, M.; Nakano, T.; Okawa, K.; Iwamatsu, A.; Kaibuchi, K. Rho-associated kinase, a novel serine/threonine kinase, as a putative target for small GTP binding protein Rho. EMBO J. 1996, 15, 2208–2216. [Google Scholar] [CrossRef]
- Kishi, T.; Hirooka, Y.; Masumoto, A.; Ito, K.; Kimura, Y.; Inokuchi, K.; Tagawa, T.; Shimokawa, H.; Takeshita, A.; Sunagawa, K. Rho-Kinase Inhibitor Improves Increased Vascular Resistance and Impaired Vasodilation of the Forearm in Patients with Heart Failure. Circulation 2005, 111, 2741–2747. [Google Scholar] [CrossRef]
- Mueller, B.K.; Mack, H.; Teusch, N. Rho kinase, a promising drug target for neurological disorders. Nat. Rev. Drug Discov. 2005, 4, 387–398. [Google Scholar] [CrossRef]
- Kinoshita, S.; Koizumi, N.; Ueno, M.; Okumura, N.; Imai, K.; Tanaka, H.; Yamamoto, Y.; Nakamura, T.; Inatomi, T.; Bush, J.; et al. Injection of Cultured Cells with a ROCK Inhibitor for Bullous Keratopathy. N. Engl. J. Med. 2018, 378, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Rothschild, P.-R.; Salah, S.; Berdugo, M.; Gélizé, E.; Delaunay, K.; Naud, M.-C.; Klein, C.; Moulin, A.; Savoldelli, M.; Bergin, C.; et al. ROCK-1 mediates diabetes-induced retinal pigment epithelial and endothelial cell blebbing: Contribution to diabetic retinopathy. Sci. Rep. 2017, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hollanders, K.; Van Hove, I.; Sergeys, J.; Van Bergen, T.; Lefevere, E.; Kindt, N.; Castermans, K.; Vandewalle, E.; Van Pelt, J.; Moons, L.; et al. AMA0428, A Potent Rock Inhibitor, Attenuates Early and Late Experimental Diabetic Retinopathy. Curr. Eye Res. 2016, 42, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Kita, T.; Hata, Y.; Arita, R.; Kawahara, S.; Miura, M.; Nakao, S.; Mochizuki, Y.; Enaida, H.; Goto, Y.; Shimokawa, H.; et al. Role of TGF-beta in proliferative vitreoretinal diseases and ROCK as a therapeutic target. Proc. Natl. Acad. Sci. USA 2008, 105, 17504–17509. [Google Scholar] [CrossRef]
- Arima, M.; Nakao, S.; Yamaguchi, M.; Feng, H.; Fujii, Y.; Shibata, K.; Wada, I.; Kaizu, Y.; Ahmadieh, H.; Ishibashi, T.; et al. Claudin-5 Redistribution Induced by Inflammation Leads to Anti-VEGF–Resistant Diabetic Macular Edema. Diabetes 2020, 69, 981–999. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Nakao, S.; Arita, R.; Kaizu, Y.; Arima, M.; Zhou, Y.; Kita, T.; Yoshida, S.; Kimura, K.; Isobe, T.; et al. Vascular Normalization by ROCK Inhibitor: Therapeutic Potential of Ripasudil (K-115) Eye Drop in Retinal Angiogenesis and Hypoxia. Investig. Opthalmol. Vis. Sci. 2016, 57, 2264. [Google Scholar] [CrossRef]
- Zandi, S.; Nakao, S.; Chun, K.-H.; Fiorina, P.; Sun, D.; Arita, R.; Zhao, M.; Kim, E.; Schueller, O.; Campbell, S.; et al. ROCK-Isoform-Specific Polarization of Macrophages Associated with Age-Related Macular Degeneration. Cell Rep. 2015, 10, 1173–1186. [Google Scholar] [CrossRef]
- Zhou, Y.; Yoshida, S.; Nakao, S.; Yoshimura, T.; Kobayashi, Y.; Nakama, T.; Kubo, Y.; Miyawaki, K.; Yamaguchi, M.; Ishikawa, K.; et al. M2 Macrophages Enhance Pathological Neovascularization in the Mouse Model of Oxygen-Induced Retinopathy. Investig. Opthalmol. Vis. Sci. 2015, 56, 4767–4777. [Google Scholar] [CrossRef]
- Nakao, S.; Arima, M.; Ishikawa, K.; Kohno, R.; Kawahara, S.; Miyazaki, M.; Yoshida, S.; Enaida, H.; Hafezi-Moghadam, A.; Kono, T.; et al. Intravitreal Anti-VEGF Therapy Blocks Inflammatory Cell Infiltration and Re-Entry into the Circulation in Retinal Angiogenesis. Investig. Opthalmol. Vis. Sci. 2012, 53, 4323–4328. [Google Scholar] [CrossRef]
- Ishikawa, K.; Yoshida, S.; Kadota, K.; Nakamura, T.; Niiro, H.; Arakawa, S.; Yoshida, A.; Akashi, K.; Ishibashi, T. Gene Expression Profile of Hyperoxic and Hypoxic Retinas in a Mouse Model of Oxygen-Induced Retinopathy. Investig. Opthalmol. Vis. Sci. 2010, 51, 4307–4319. [Google Scholar] [CrossRef]
- Ishikawa, K.; Yoshida, S.; Nakao, S.; Sassa, Y.; Asato, R.; Kohno, R.; Arima, M.; Kita, T.; Yoshida, A.; Ohuchida, K.; et al. Bone marrow-derived monocyte lineage cells recruited by MIP-1β promote physiological revascularization in mouse model of oxygen-induced retinopathy. Lab. Investig. 2011, 92, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Soucek, L.; Lawlor, E.R.; Soto, D.; Shchors, K.; Swigart, L.B.; Evan, G.I. Mast cells are required for angiogenesis and macroscopic expansion of Myc-induced pancreatic islet tumors. Nat. Med. 2007, 13, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Muramatsu, M.; Katada, J.; Hayashi, I.; Majima, M. Chymase as a Proangiogenic Factor. J. Biol. Chem. 2000, 275, 5545–5552. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, K.; Okamoto, N.; Kondo, M.; Arkwright, P.D.; Karasawa, K.; Ishizaka, S.; Yokota, S.; Matsuda, A.; Jung, K.; Oida, K.; et al. Mast cell hyperactivity underpins the development of oxygen-induced retinopathy. J. Clin. Investig. 2017, 127, 3987–4000. [Google Scholar] [CrossRef] [PubMed]
- Rao, N.; Lee, Y.F.; Ge, R. Novel endogenous angiogenesis inhibitors and their therapeutic potential. Acta Pharmacol. Sin. 2015, 36, 1177–1190. [Google Scholar] [CrossRef]
- Stahl, A.; Joyal, J.-S.; Chen, J.; Sapieha, P.; Juan, A.M.; Hatton, C.J.; Pei, D.T.; Hurst, C.G.; Seaward, M.R.; Krah, N.M.; et al. SOCS3 is an endogenous inhibitor of pathologic angiogenesis. Blood 2012, 120, 2925–2929. [Google Scholar] [CrossRef]
- Starr, R.; Willson, T.A.; Viney, E.M.; Murray, L.J.L.; Rayner, J.R.; Jenkins, B.J.; Gonda, T.J.; Alexander, W.S.; Metcalf, D.; Nicola, N.A.; et al. A family of cytokine-inducible inhibitors of signalling. Nat. Cell Biol. 1997, 387, 917–921. [Google Scholar] [CrossRef]
- Sun, Y.; Ju, M.; Lin, Z.; Fredrick, T.W.; Evans, L.P.; Tian, K.T.; Saba, N.J.; Morss, P.C.; Pu, W.T.; Chen, J.; et al. SOCS3 in retinal neurons and glial cells suppresses VEGF signaling to prevent pathological neovascular growth. Sci. Signal. 2015, 8, ra94. [Google Scholar] [CrossRef]
- Sun, Y.; Liu, C.-H.; SanGiovanni, J.P.; Evans, L.P.; Tian, K.T.; Zhang, B.; Stahl, A.; Pu, W.T.; Kamenecka, T.M.; Solt, L.A.; et al. Nuclear receptor RORα regulates pathologic retinal angiogenesis by modulating SOCS3-dependent inflammation. Proc. Natl. Acad. Sci. USA 2015, 112, 10401–10406. [Google Scholar] [CrossRef]
- Isenberg, S.J.; Apt, L.; Mccarty, J.; Cooper, L.L.; Lim, L.; Del Signore, M. Development of tearing in preterm and term neonates. Arch. Ophthalmol. 1998, 116, 773–776. [Google Scholar] [CrossRef]
- Kusari, A.; Ba, A.M.H.; Virgen, C.A.; Matiz, C.; Rasmussen, M.; Friedlander, S.F.; Eichenfield, D.Z. Evidence-based skin care in preterm infants. Pediatr. Dermatol. 2018, 36, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Salaets, T.; Turner, M.A.; Short, M.; Ward, R.M.; Hokuto, I.; Ariagno, R.L.; Klein, A.; Beauman, S.; Wade, K.; Thomson, M.; et al. Development of a neonatal adverse event severity scale through a Delphi consensus approach. Arch. Dis. Child. 2019, 104, 1167–1173. [Google Scholar] [CrossRef] [PubMed]



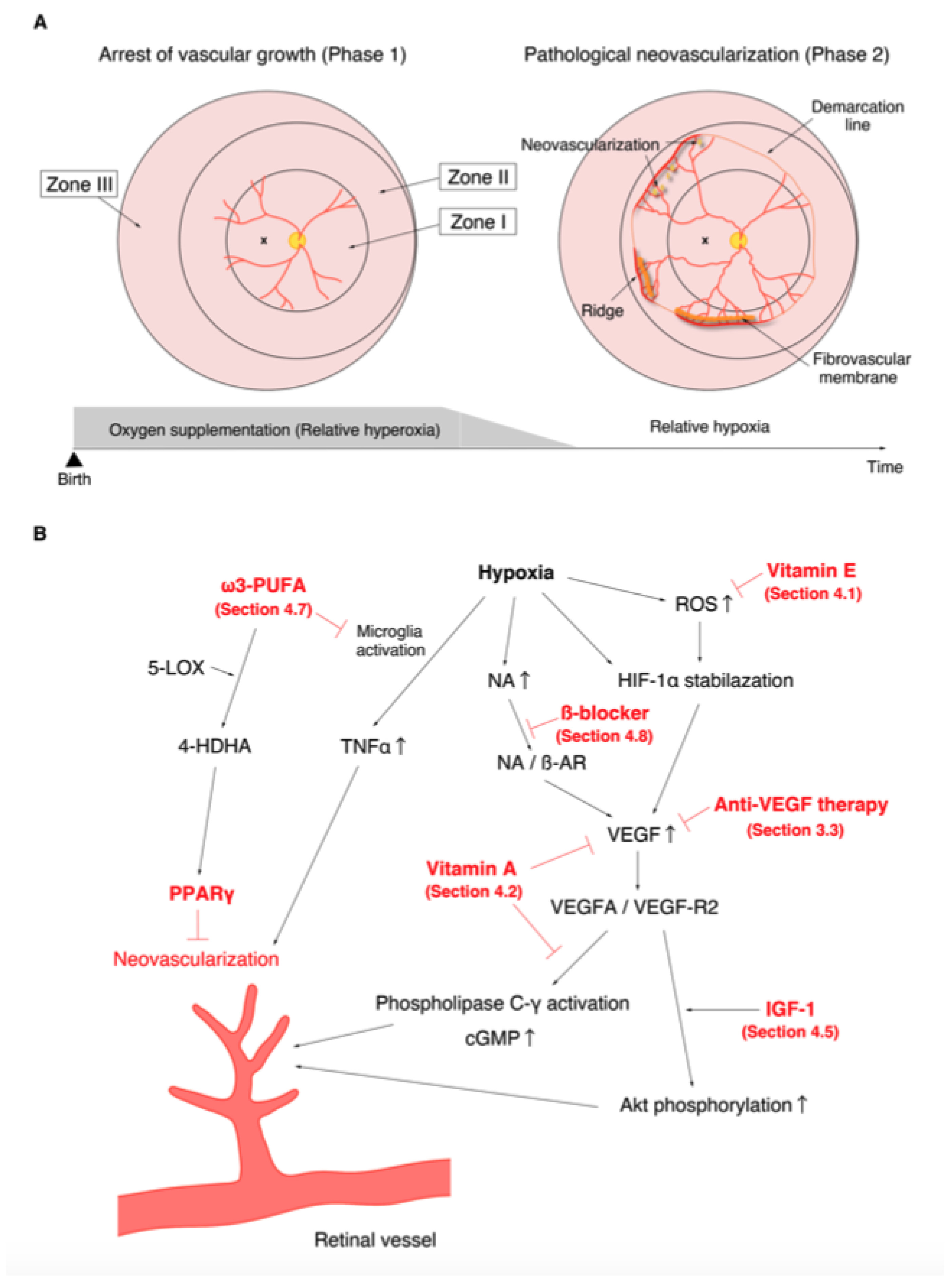{kind=link}
{kind=link}
| Location (see Figure 1) | Zone I | Circle centered on the optic disc with the radius of twice the distance from the optic disc to the fovea. |
| Zone II | Circle centered on the optic disc with the distance to the nasal ora serrata as the radius, excluding Zone I | |
| Zone III | Residual retina anterior to Zone II. | |
| Severity | Stage 1 | Demarcation line |
| Stage 2 | Ridge | |
| Stage 3 | Ridge with extra retinal fibrovascular proliferation | |
| Stage 4 | Subtotal retinal detachment | |
| Stage 5 | Total retinal detachment | |
| Plus disease | Venous dilation and arterial tortuosity of the posterior pole vessels |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arima, M.; Fujii, Y.; Sonoda, K.-H. Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again. J. Clin. Med. 2021, 10, 331. https://doi.org/10.3390/jcm10020331
Arima M, Fujii Y, Sonoda K-H. Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again. Journal of Clinical Medicine. 2021; 10(2):331. https://doi.org/10.3390/jcm10020331
Chicago/Turabian StyleArima, Mitsuru, Yuya Fujii, and Koh-Hei Sonoda. 2021. "Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again" Journal of Clinical Medicine 10, no. 2: 331. https://doi.org/10.3390/jcm10020331
APA StyleArima, M., Fujii, Y., & Sonoda, K.-H. (2021). Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again. Journal of Clinical Medicine, 10(2), 331. https://doi.org/10.3390/jcm10020331