
A Network Analysis of Drug Combinations Associated with Acute Generalized Exanthematous Pustulosis (AGEP)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
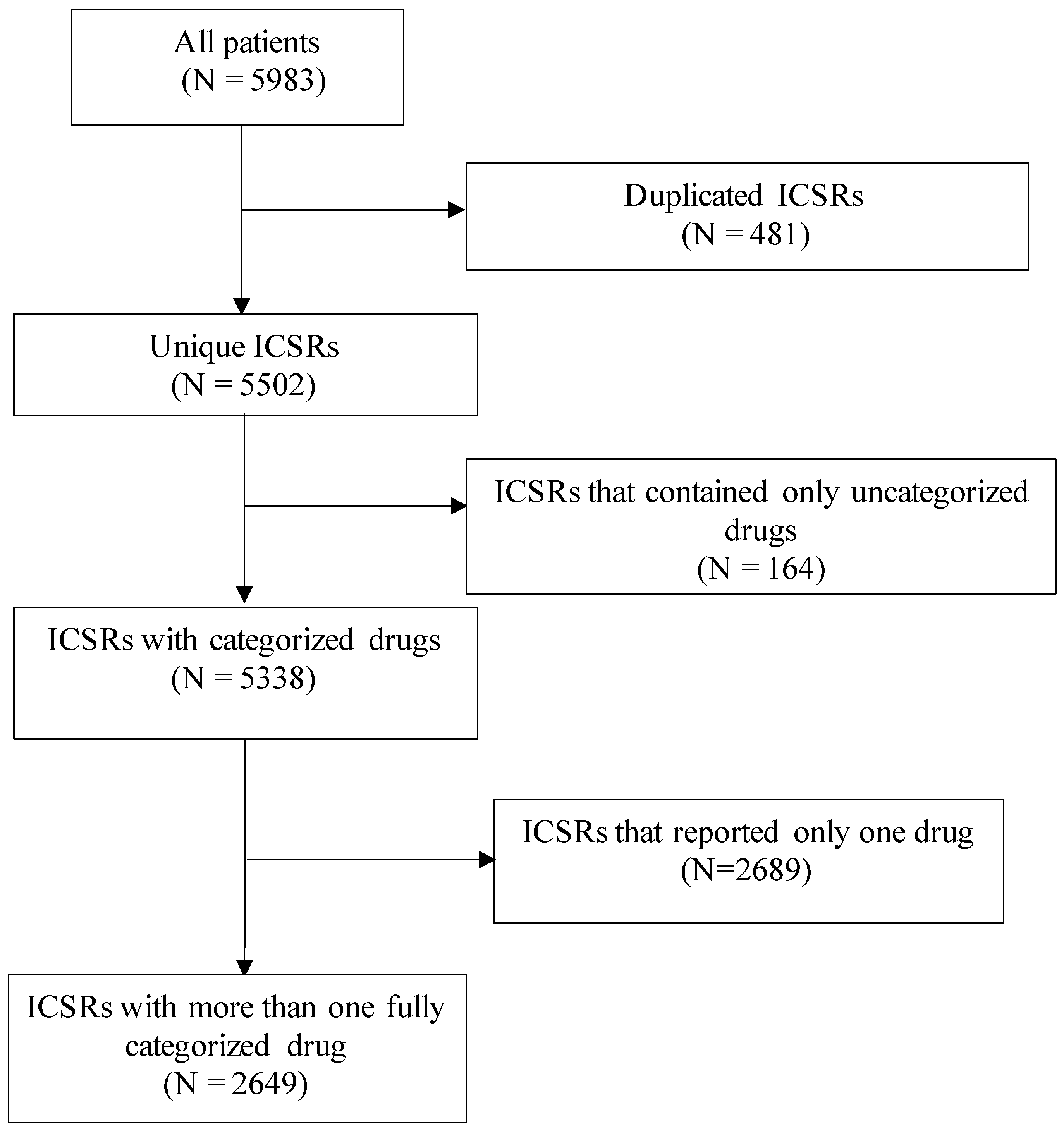
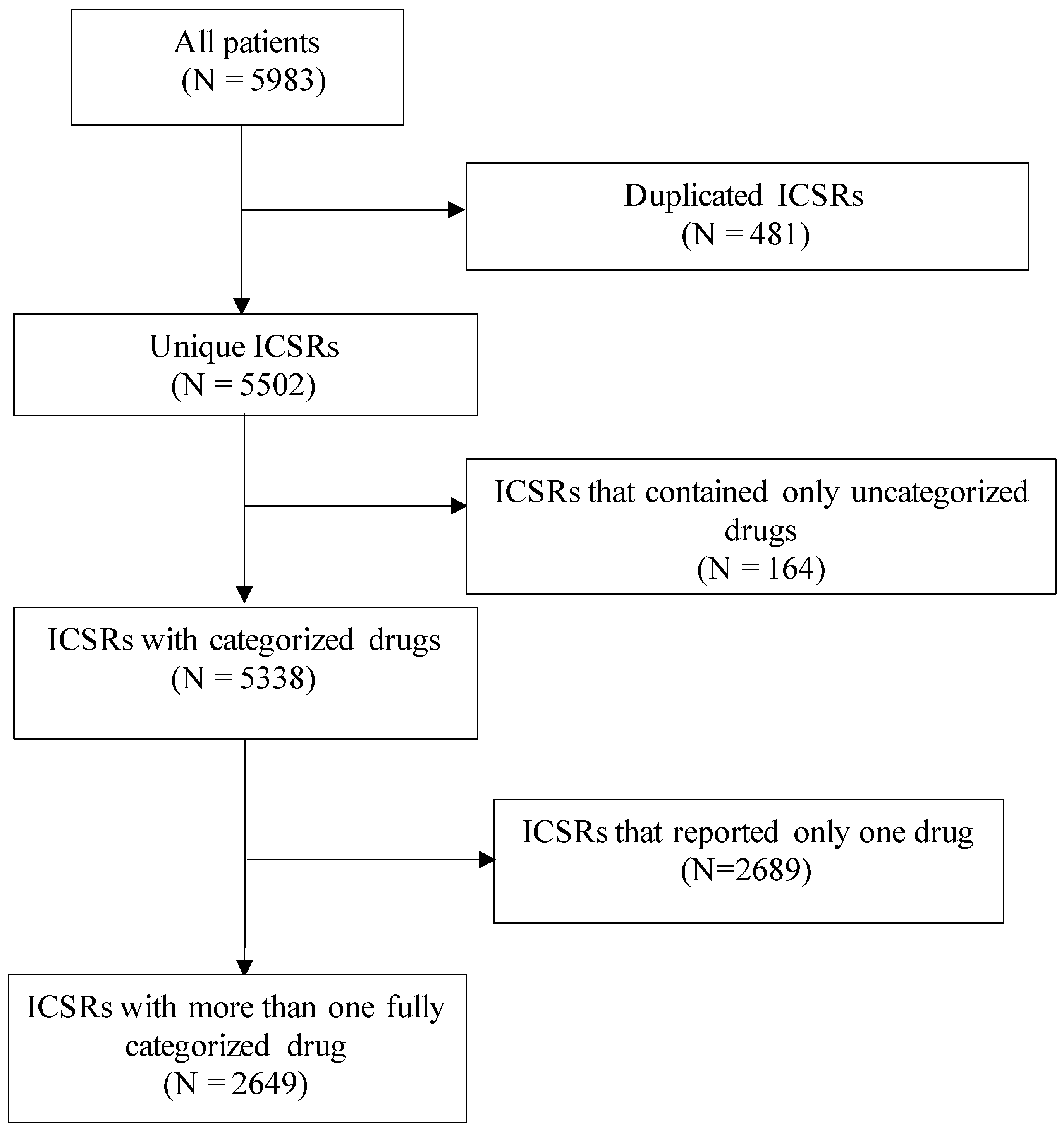
2.1. Data Source and Patient Population
2.2. Analysis
3. Results
Descriptive Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sidoroff, A.; Halevy, S.; Bavinck, J.N.B.; Vaillant, L.; Roujeau, J.C. Acute Generalized Exanthematous Pustulosis (AGEP)—A Clinical Reaction Pattern. J. Cutan. Pathol. 2001, 28, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Duman, H.; Topal, I.O.; Kocaturk, E.; Cure, K.; Mansuroglu, I. Acute Generalized Exanthematous Pustulosis Induced by Hydroxychloroquine: A Case with Atypical Clinical Presentation. An. Bras. Dermatol. 2017, 92, 404–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bostan, E.; Yalcin, H.B.; Akdogan, N.; Ozdemir, D.A.; Karaduman, A. Acute Generalized Exanthematous Pustulosis Induced by Iron Carboxymaltose Infusion: A Case Report. Dermatol. Ther. 2020, 33, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Roujeau, J.C.; Bioulac-Sage, P.; Bourseau, C.; Guillaume, J.C.; Bernard, P.; Lok, C.; Plantin, P.; Claudy, A.; Delavierre, C.; Vaillant, L. Acute Generalized Exanthematous Pustulosis. Analysis of 63 Cases. Arch. Dermatol. 1991, 127, 1333–1338. [Google Scholar] [CrossRef]
- Fernando, S.L. Acute Generalised Exanthematous Pustulosis. Australas. J. Dermatol. 2012, 53, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Roujeau, J. Clinical Heterogeneity of Drug Hypersensitivity. Toxicology 2005, 209, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Paolino, A.; Walsh, S.; Basu, T.; Creamer, D. Severe Drug-Induced Kidney Injury in Acute Generalized Exanthematous Pustulosis. Clin. Exp. Dermatol. 2018, 43, 323–324. [Google Scholar] [CrossRef]
- Belhadjali, H.; Mandhouj, S.; Amri, M.; Zakhama, A. Mercury-Induced Acute Generalized Exanthematous Pustulosis Misdiagnosed as a Drug-Related Case. Contact Dermat. 2008, 59, 52–54. [Google Scholar] [CrossRef]
- Ameur, K.; Youssef, M.; Belhadjali, H.; Soua, Y.; Korbi, M.; Henchi, M.A.; Zili, J. Occupational Acute Generalized Exanthematous Pustulosis Induced by Disperse Dyes in a Textile. Contact Dermat. 2019, 80, 411–412. [Google Scholar] [CrossRef]
- Rouchouse, B.; Bonnefoy, M.; Pallot, B.; Jacquelin, L.; Dimoux-Dime, G.; Claudy, A. Acute Generalized Exanthematous Pustular Dermatitis and Viral Infection. Dermatology 1986, 173, 180–184. [Google Scholar] [CrossRef]
- Sidoroff, A.; Dunant, A.; Viboud, C.; Halevy, S.; Bavinck, J.N.B.; Naldi, L.; Mockenhaupt, M.; Fagot, J.-P.; Roujeau, J.-C. Risk Factors for Acute Generalized Exanthematous Pustulosis (AGEP)-Results of a Multinational Case-Control Study (EuroSCAR). Br. J. Dermatol. 2007, 157, 989–996. [Google Scholar] [CrossRef]
- European Medicines Agency. PRAC Recommendations on Signals; European Medicines Agency: Amsterdam, The Netherlands, 2016. [Google Scholar]
- European Medicines Agency. PRAC Recommendations on Signals; European Medicines Agency: Amsterdam, The Netherlands, 2017. [Google Scholar]
- European Medicines Agency. PRAC Recommendations on Signals; European Medicines Agency: Amsterdam, The Netherlands, 2018. [Google Scholar]
- European Medicines Agency. PRAC Recommendations on Signals; European Medicines Agency: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Food and Drug Administration. October–December 2018|Potential Signals of Serious Risks/New Safety Information Identified by the FDA Adverse Event Reporting System (FAERS); Food and Drug Administration: Silver Spring, MD, USA, 2019.
- Food and Drug Administration. July–September 2019|Potential Signals of Serious Risks/New Safety Information Identified by the FDA Adverse Event Reporting System (FAERS); Food and Drug Administration: Silver Spring, MD, USA, 2020.
- Food and Drug Administration. April–June 2016|Potential Signals of Serious Risks/New Safety Information Identified by the FDA Adverse Event Reporting System (FAERS); Food and Drug Administration: Silver Spring, MD, USA, 2020.
- Barbaud, A.; Collet, E.; Milpied, B.; Assier, H.; Staumont, D.; Avenel-Audran, M.; Grange, A.; Amarger, S.; Girardin, P.; Guinnepain, M.-T.; et al. A Multicentre Study to Determine the Value and Safety of Drug Patch Tests for the Three Main Classes of Severe Cutaneous Adverse Drug Reactions. Br. J. Dermatol. 2013, 168, 555–562. [Google Scholar] [CrossRef]
- Zheng, J.; Gao, Y.; Yi, X.; Ding, Y. A Case of Ceftriaxone-Induced Acute Generalized Exanthematous Pustulosis/Generalized Pustular Psoriasis Overlap. Case Rep. Dermatol. 2018, 10, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaabane, A.; Aouam, K.; Gassab, L.; Njim, L.; Boughattas, N.A. Acute Generalized Exanthematous Pustulosis (AGEP) Induced by Cefotaxime. Fundam. Clin. Pharmacol. 2010, 24, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Nacaroglu, H.T.; Celegen, M.; Ozek, G.; Umac, O.; Karkiner, C.S.U.; Yildirim, H.T.; Can, D. Acute Generalized Exanthematous Pustulosis Induced by Ceftriaxone Use. Postepy Dermatol. Alergol. 2014, 31, 269–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bate, A.; Evans, S.J.W. Quantitative Signal Detection Using Spontaneous ADR Reporting. Pharmacoepidemiol. Drug Saf. 2009, 18, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Smeets, T.J.L.; Jessurun, N.; Härmark, L.; Kardaun, S.H. Clindamycin-Induced Acute Generalised Exanthematous Pustulosis: Five Cases and a Review of the Literature. Neth. J. Med. 2016, 74, 421–428. [Google Scholar]
- Janier, M.; Froidevaux, D.; Lons-Danic, D.; Daniel, F. Acute Generalized Exanthematous Pustulosis Due to the Combination of Chloroquine and Proguanil. Dermatology 1998, 196, 271. [Google Scholar] [CrossRef]
- Ogoshi, M.; Yamada, Y.; Tani, M. Acute Generalized Exanthematic Pustulosis Induced by Cefaclor and Acetazolamide. Dermatology 1992, 184, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Kovács, I.A.; Barabási, A.-L. Network-Based Prediction of Drug Combinations. Nat. Commun. 2019, 10, 1197. [Google Scholar] [CrossRef]
- Botsis, T.; Ball, R. Network Analysis of Possible Anaphylaxis Cases Reported to the US Vaccine Adverse Event Reporting System after H1N1 Influenza Vaccine. Stud. Health Technol. Inform. 2011, 169, 564–568. [Google Scholar] [PubMed]
- Davazdahemami, B.; Delen, D. A Chronological Pharmacovigilance Network Analytics Approach for Predicting Adverse Drug Events. J. Am. Med Inform. Assoc. 2018, 25, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, M. VigiBase, the WHO Global ICSR Database System: Basic Facts. Drug Inf. J. 2008, 42, 409–419. [Google Scholar] [CrossRef]
- Schäfer, I.; Kaduszkiewicz, H.; Wagner, H.-O.; Schön, G.; Scherer, M.; van den Bussche, H. Reducing Complexity: A Visualisation of Multimorbidity by Combining Disease Clusters and Triads. BMC Public Health 2014, 14, 1285. [Google Scholar] [CrossRef] [Green Version]
- Scott, J. Social Network Analysis. Sociology 1988, 22, 109–127. [Google Scholar] [CrossRef]
- Dehmer, M.; Basak, S.C. Statistical and Machine Learning Approaches for Network Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2012; ISBN 978-1-118-34698-3. [Google Scholar]
- Blondel, V.D.; Guillaume, J.-L.; Lambiotte, R.; Lefebvre, E. Fast Unfolding of Communities in Large Networks. J. Stat. Mech. 2008, 2008, P10008. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.E. Finding Community Structure in Networks Using the Eigenvectors of Matrices. Phys. Rev. E 2006, 74, 036104. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Bastian, M.; Heymann, S.; Jacomy, M. Gephi: An Open Source Software for Exploring and Manipulating Networks. In Proceedings of the International AAAI Conference on Web and Social Media, San Jose, CA, USA, 17–20 May 2009; Volume 3. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.Y.; Thirumoorthy, T.; Pang, S.M. Acute Generalized Exanthematous Pustulosis (AGEP) in Singapore. Clin. Transl. Allergy 2014, 4, P90. [Google Scholar] [CrossRef] [Green Version]
- Ball, R.; Botsis, T. Can Network Analysis Improve Pattern Recognition among Adverse Events Following Immunization Reported to VAERS? Clin. Pharmacol. Ther. 2011, 90, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.G.; Jeong, C.R.; Kim, H.J.; Kim, J.H.; Song, Y.K.; Kim, K.I.; Ji, E.; Yoon, S.S.; Koh, Y.; Cho, Y.S.; et al. Network Analysis of Drug-Related Problems in Hospitalized Patients with Hematologic Malignancies. Supportive Care Cancer 2018, 26, 2737–2742. [Google Scholar] [CrossRef] [PubMed]
- Feldmeyer, L.; Heidemeyer, K.; Yawalkar, N. Acute Generalized Exanthematous Pustulosis: Pathogenesis, Genetic Background, Clinical Variants and Therapy. Int. J. Mol. Sci. 2016, 17, 1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libby, P.; Lichtman, A.H.; Hansson, G.K. Immune Effector Mechanisms Implicated in Atherosclerosis: From Mice to Humans. Immunity 2013, 38, 1092–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rader, D.J.; Daugherty, A. Translating Molecular Discoveries into New Therapies for Atherosclerosis. Nature 2008, 451, 904–913. [Google Scholar] [CrossRef]
- Burkhart, K.K.; Abernethy, D.; Jackson, D. Data Mining FAERS to Analyze Molecular Targets of Drugs Highly Associated with Stevens-Johnson Syndrome. J. Med. Toxicol. 2015, 11, 265–273. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Overall | Female | Male | |||||
|---|---|---|---|---|---|---|---|
| (n = 2649) | (n = 1571) | (n = 1020) | |||||
| n | % | n | % | n | % | p-Value | |
| Mean age (SD) | 57.32 | (21.80) | 59.33 | (21.34) | 54.27 | (22.14) | <0.001 |
| Age Groups | <0.001 | ||||||
| <16 | 114 | (4.3) | 41 | (2.6) | 72 | (7.1) | |
| 16–44 | 542 | (20.5) | 327 | (20.8) | 213 | (20.9) | |
| 45–64 | 723 | (27.3) | 405 | (25.8) | 317 | (31.1) | |
| 65–84 | 853 | (32.2) | 538 | (34.2) | 308 | (30.2) | |
| 85+ | 190 | (7.2) | 144 | (9.2) | 46 | (4.5) | |
| Unknown | 227 | (8.6) | 116 | (7.4) | 64 | (6.3) | |
| Region of Report | <0.001 | ||||||
| Europe | 1585 | (59.8) | 1005 | (64.0) | 563 | (55.2) | |
| Asia | 619 | (23.4) | 339 | (21.6) | 274 | (26.9) | |
| Africa | 26 | (1.0) | 10 | (0.6) | 16 | (1.6) | |
| North America | 374 | (14.1) | 190 | (12.1) | 151 | (14.8) | |
| Oceania | 35 | (1.3) | 19 | (1.2) | 14 | (1.4) | |
| South America | 10 | (0.4) | 8 | (0.5) | 2 | (0.2) | |
| Reporter Type | 0.037 | ||||||
| Physician | 1739 | (83.3) | 1067 | (85.4) | 642 | (81.3) | |
| Other Health Professional | 296 | (14.2) | 157 | (12.6) | 124 | (15.7) | |
| Nonhealth Professional | 53 | (2.5) | 25 | (2.0) | 24 | (3.0) | |
| Seriousness (Yes) | 2179 | (91.9) | 1315 | (92.2) | 813 | (91.2) | 0.452 |
| Death | 66 | (2.5) | 33 | (2.1) | 27 | (2.6) | 0.441 |
| Number of reported Drugs | |||||||
| Mean (SD) | 4.22 | (3.24) | 4.27 | (3.20) | 4.15 | (3.32) | 0.361 |
| Median (IQR) | 3.00 | (2.00– 5.00) | 3.00 | (2.00– 5.00) | 3.00 | (2.00–5.00) | 0.359 |
| Individual Drugs | Drug-Drug Pairs | Drug Triads | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Drug 1 | n | Prevalence | Drug 1 | Drug 2 | n | Prevalence | Expected Prevalence | O/E Ratio | Drug 1 | Drug 2 | Drug 3 | n | Prevalence | Expected Prevalence | O/E Ratio |
| amoxicillin | 573 | 21.63% | paracetamol | amoxicillin | 109 | 4.11% | 3.24% | 1.27 | ibuprofen | amoxicillin | paracetamol | 17 | 0.64% | 0.12% | 5.14 |
| paracetamol | 397 | 14.99% | amoxicillin | furosemide | 57 | 2.15% | 1.61% | 1.34 | enoxaparin | amoxicillin | paracetamol | 16 | 0.60% | 0.14% | 4.18 |
| ceftriaxone | 234 | 8.83% | ceftriaxone | metronidazole | 53 | 2.00% | 0.50% | 4.00 | ASA | furosemide | amoxicillin | 15 | 0.57% | 0.11% | 4.93 |
| vancomycin | 219 | 8.27% | paracetamol | enoxaparin | 47 | 1.77% | 0.67% | 2.66 | furosemide | bisoprolol | amoxicillin | 15 | 0.57% | 0.07% | 8.63 |
| furosemide | 197 | 7.44% | atorvastatin | ASA | 46 | 1.74% | 0.27% | 6.51 | ASA | amoxicillin | paracetamol | 14 | 0.53% | 0.23% | 2.28 |
| ASA | 189 | 7.13% | amoxicillin | ASA | 45 | 1.70% | 1.54% | 1.10 | ASA | metformin | amlodipine | 13 | 0.49% | 0.01% | 41.64 |
| clindamycin | 181 | 6.83% | ceftriaxone | amoxicillin | 45 | 1.70% | 1.91% | 0.89 | ASA | clopidogrel | atorvastatin | 13 | 0.49% | 0.00% | 103.73 |
| piperacillin | 157 | 5.93% | bisoprolol | furosemide | 44 | 1.66% | 0.30% | 5.48 | ASA | amlodipine | atorvastatin | 12 | 0.45% | 0.01% | 35.72 |
| metronidazole | 150 | 5.66% | paracetamol | omeprazole | 42 | 1.59% | 0.78% | 2.05 | ASA | furosemide | bisoprolol | 11 | 0.42% | 0.02% | 19.20 |
| omeprazole | 137 | 5.17% | paracetamol | ibuprofen | 41 | 1.55% | 0.58% | 2.68 | metronidazole | vancomycin | ceftriaxone | 11 | 0.42% | 0.04% | 10.04 |
| amlodipine | 126 | 4.76% | paracetamol | furosemide | 41 | 1.55% | 1.11% | 1.39 | warfarin | furosemide | bisoprolol | 10 | 0.38% | 0.00% | 94.23 |
| pristinamycin | 124 | 4.68% | piperacillin | vancomycin | 40 | 1.51% | 0.49% | 3.08 | ASA | furosemide | atorvastatin | 10 | 0.38% | 0.02% | 19.04 |
| pantoprazole | 121 | 4.57% | furosemide | ASA | 39 | 1.47% | 0.53% | 2.77 | ASA | atorvastatin | amoxicillin | 10 | 0.38% | 0.06% | 6.55 |
| prednisolone | 120 | 4.53% | levetiracetam | valproic acid | 37 | 1.40% | 0.07% | 20.60 | warfarin | furosemide | amoxicillin | 10 | 0.38% | 0.02% | 17.76 |
| enoxaparin | 118 | 4.45% | ceftriaxone | vancomycin | 36 | 1.36% | 0.73% | 1.86 | furosemide | amoxicillin | allopurinol | 10 | 0.38% | 0.06% | 6.76 |
| esomeprazole | 116 | 4.38% | amlodipine | ASA | 35 | 1.32% | 0.34% | 3.89 | furosemide | bisoprolol | allopurinol | 10 | 0.38% | 0.01% | 35.85 |
| ciprofloxacin | 116 | 4.38% | clindamycin | vancomycin | 35 | 1.32% | 0.56% | 2.34 | esomeprazole | enoxaparin | paracetamol | 10 | 0.38% | 0.03% | 12.91 |
| bisoprolol | 108 | 4.08% | amoxicillin | ibuprofen | 35 | 1.32% | 0.83% | 1.59 | ASA | furosemide | paracetamol | 10 | 0.38% | 0.08% | 4.75 |
| sulfamethoxazole | 106 | 4.00% | paracetamol | ASA | 34 | 1.28% | 1.07% | 1.20 | amoxicillin | ceftriaxone | paracetamol | 10 | 0.38% | 0.29% | 1.32 |
| ibuprofen | 102 | 3.85% | bisoprolol | ASA | 33 | 1.25% | 0.29% | 4.28 | furosemide | amoxicillin | paracetamol | 10 | 0.38% | 0.24% | 1.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-De la Torre, A.; van Weenen, E.; Kraus, M.; Weiler, S.; Feuerriegel, S.; Burden, A.M. A Network Analysis of Drug Combinations Associated with Acute Generalized Exanthematous Pustulosis (AGEP). J. Clin. Med. 2021, 10, 4486. https://doi.org/10.3390/jcm10194486
Martinez-De la Torre A, van Weenen E, Kraus M, Weiler S, Feuerriegel S, Burden AM. A Network Analysis of Drug Combinations Associated with Acute Generalized Exanthematous Pustulosis (AGEP). Journal of Clinical Medicine. 2021; 10(19):4486. https://doi.org/10.3390/jcm10194486
Chicago/Turabian StyleMartinez-De la Torre, Adrian, Eva van Weenen, Mathias Kraus, Stefan Weiler, Stefan Feuerriegel, and Andrea M. Burden. 2021. "A Network Analysis of Drug Combinations Associated with Acute Generalized Exanthematous Pustulosis (AGEP)" Journal of Clinical Medicine 10, no. 19: 4486. https://doi.org/10.3390/jcm10194486
APA StyleMartinez-De la Torre, A., van Weenen, E., Kraus, M., Weiler, S., Feuerriegel, S., & Burden, A. M. (2021). A Network Analysis of Drug Combinations Associated with Acute Generalized Exanthematous Pustulosis (AGEP). Journal of Clinical Medicine, 10(19), 4486. https://doi.org/10.3390/jcm10194486