
An Integrated Account of Expert Perspectives on Functioning in Schizophrenia

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
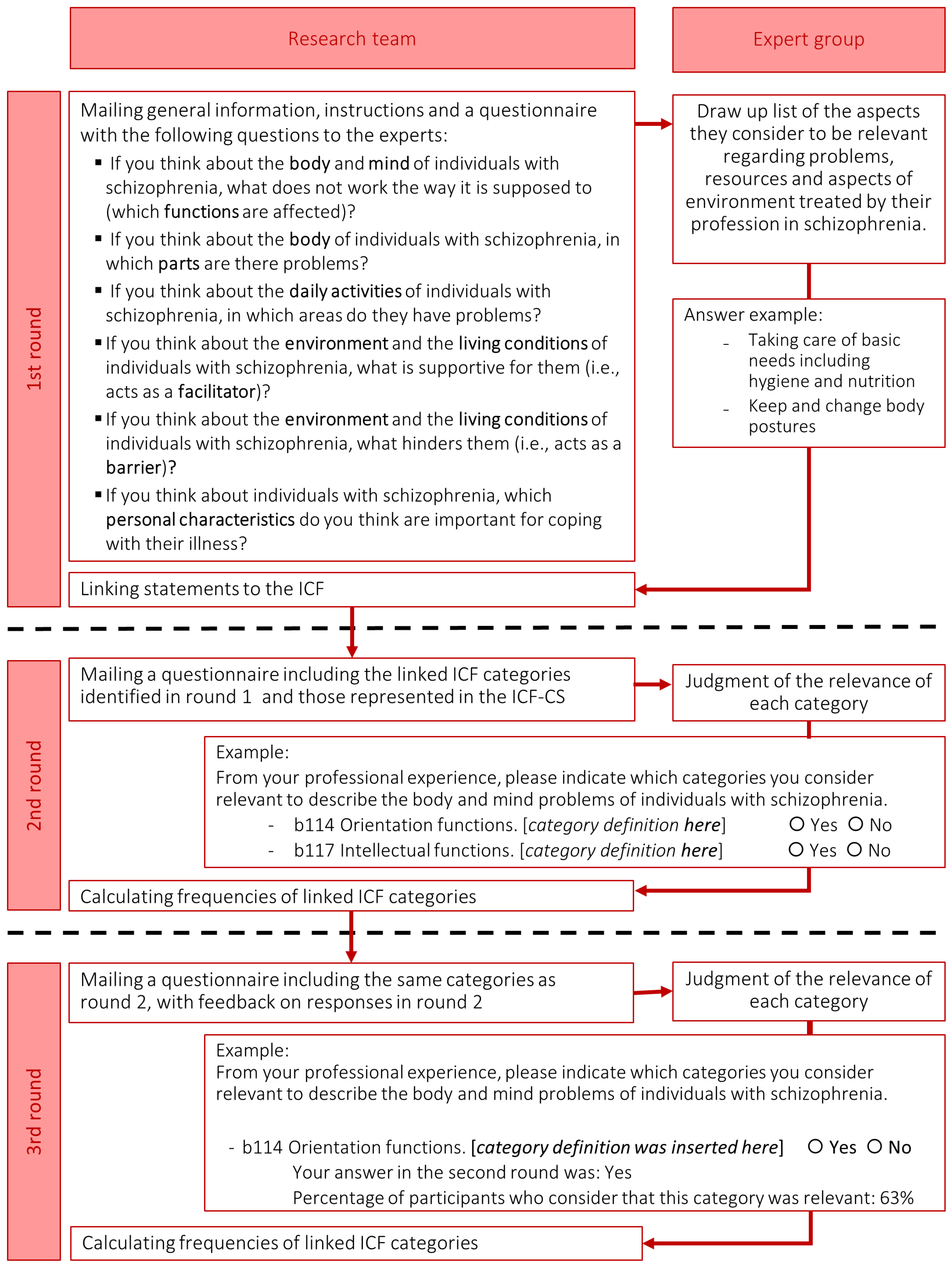
2.2. Procedure
2.3. Data Analysis
3. Results
3.1. Selected Categories from the Experts’ Perspective
3.2. Correspondence between Categories Which Reached Expert Consensus and the ICF-CSs for Schizophrenia
3.3. Personal Factors
4. Discussion
4.1. Body Functions
4.2. Body Structures
4.3. Activities and Participation
4.4. Environmental Factors
4.5. Personal Factors
4.6. Strengths, Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frese, F.J.; Knight, E.L.; Saks, E. Recovery from schizophrenia: With views of psychiatrists, psychologists, and others diagnosed with this disorder. Schizophr. Bull. 2009, 35, 370–380. [Google Scholar] [CrossRef]
- Van Eck, R.M.; Burger, T.J.; Vellinga, A.; Schirmbeck, F.; De Haan, L. The Relationship Between Clinical and Personal Recovery in Patients with Schizophrenia Spectrum Disorders: A Systematic Review and Meta-analysis. Schizophr. Bull. 2018, 44, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Vita, A.; Barlati, S. Recovery from schizophrenia. Curr. Opin. Psychiatry 2018, 31, 246–255. [Google Scholar] [CrossRef]
- Lally, J.; Ajnakina, O.; Stubbs, B.; Cullinane, M.; Murphy, K.C.; Gaughran, F.; Murray, R.M. Remission and recovery from first-episode psychosis in adults: Systematic review and meta-analysis of long-term outcome studies. Br. J. Psychiatry 2017, 211, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Kalin, M.; Kaplan, S.; Gould, F.; Pinkham, A.E.; Penn, D.L.; Harvey, P.D. Social cognition, social competence, negative symptoms and social outcomes: Inter-relationships in people with schizophrenia. J. Psychiatr. Res. 2015, 68, 254–260. [Google Scholar] [CrossRef]
- Penadés, R.; Pérez-García, H.; González-Rodríguez, A.; Catalán, R.; Bernardo, M. Treating Cognition in Schizophrenia: Searching for the Best Evidence-Based Practices. 2016. Available online: https://pdfs.semanticscholar.org/3a5f/dd2e9c2819a3cc1252a0d3b30be2317544fc.pdf (accessed on 1 July 2021).
- Fleischhacker, W.W.; Arango, C.; Arteel, P.; Barnes, T.R.E.; Carpenter, W.; Duckworth, K.; Galderisi, S.; Halpern, L.; Knapp, M.; Marder, S.R.; et al. Schizophrenia-Time to commit to policy change. Schizophr. Bull. 2014, 40, S165–S194. [Google Scholar] [CrossRef]
- Jablensky, A.; Castle, D.J.; Dark, F.; Humberstone, V.; Killackey, E.; Kulkarni, J.; McGorry, P.; Morgan, V.A.; Nielssen, O.; Tran, N.; et al. The 2016 RANZCP Guidelines for the Management of Schizophrenia and Related Disorders—What’s next? Australas. Psychiatry 2017, 25, 600–602. [Google Scholar] [CrossRef] [PubMed]
- Kendall, T.; Whittington, C.J.; Kuipers, E.; Johnson, S.; Birchwood, M.J.; Marshall, M.; Morrison, A.P. NICE vs. SIGN on psychosis and schizophrenia: Same roots, similar guidelines, different interpretations. Br. J. Psychiatry 2016, 208, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Mahone, I.H.; Maphis, C.F.; Snow, D.E. Effective Strategies for Nurses Empowering Clients with Schizophrenia: Medication Use as a Tool in Recovery. Issues Ment. Health Nurs. 2016, 37, 372–379. [Google Scholar] [CrossRef]
- Virgolesi, M.; Pucciarelli, G.; Colantoni, A.M.; D’Andrea, F.; Di Donato, B.; Giorgi, F.; Landi, L.; Salustri, E.; Turci, C.; Proietti, M.G. The effectiveness of a nursing discharge programme to improve medication adherence and patient satisfaction in the psychiatric intensive care unit. J. Clin. Nurs. 2017, 26, 4456–4466. [Google Scholar] [CrossRef]
- Foruzandeh, N.; Parvin, N. Occupational therapy for inpatients with chronic schizophrenia: A pilot randomized controlled trial. Japan J. Nurs. Sci. 2013, 10, 136–141. [Google Scholar] [CrossRef]
- Shimada, T.; Ohori, M.; Inagaki, Y.; Shimooka, Y.; Ishihara, I.; Sugimura, N.; Tanaka, S.; Kobayashi, M. Effect of adding individualized occupational therapy to standard care on rehospitalization of patients with schizophrenia: A 2-year prospective cohort study. Psychiatry Clin. Neurosci. 2019, 73, 476–485. [Google Scholar] [CrossRef]
- de Saxe Zerden, L.; Lombardi, B.M.; Guan, T. Integrated Behavioral Health and Social Work: A Global Perspective. Glob. Soc. Welf. 2019, 6, 49–56. [Google Scholar] [CrossRef]
- Fraser, M.W.; Lombardi, B.M.; Wu, S.; de Saxe Zerden, L.; Richman, E.L.; Fraher, E.P. Integrated primary care and social work: A systematic review. J. Soc. Soc. Work Res. 2018, 9, 175–215. [Google Scholar] [CrossRef]
- Firth, J.; Stubbs, B.; Rosenbaum, S.; Vancampfort, D.; Malchow, B.; Schuch, F.; Elliott, R.; Nuechterlein, K.H.; Yung, A.R. Aerobic exercise improves cognitive functioning in people with schizophrenia: A systematic review and meta-analysis. Schizophr. Bull. 2017, 43, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Nyboe, L.; Stubbs, B. Physiotherapy within the Multidisciplinary Treatment of Schizophrenia. In Physiotherapy in Mental Health and Psychiatry: A Scientific and Clinical Based Approach; Probst, M., Skjaerven, L.H., Eds.; Elsevier: Edinburg, Scotland, 2017; pp. 259–263. [Google Scholar]
- Amore, K.; Howden-Chapman, P.L. Mental Health and Homelessness. In International Encyclopedia of Housing and Home; University of Otago: Wellington, New Zealand, 2012; pp. 268–273. ISBN 9780080471716. [Google Scholar] [CrossRef]
- Schöttle, D.; Schimmelmann, B.G.; Ruppelt, F.; Bussopulos, A.; Frieling, M.; Nika, E.; Nawara, L.A.; Golks, D.; Kerstan, A.; Lange, M.; et al. Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia-spectrum and bipolar I disorders: Four-year follow-up of the ACCESS II study. PLoS ONE 2018, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- She, S.; Deng, Y.; Chen, Y.; Wu, C.; Yi, W.; Lu, X.; Chen, X.; Li, J.; Li, R.; Zhang, J.; et al. Two-stage integrated care versus antipsychotic medication alone on outcomes of schizophrenia: One-year randomized controlled trial and follow-up. Psychiatry Res. 2017, 254, 164–172. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001; ISBN 9241545429. [Google Scholar]
- Selb, M.; Escorpizo, R.; Kostanjsek, N.; Stucki, G.; Üstün, T.B.; Cieza, A. A guide on how to develop an International Classification of Functioning, Disability and Health Core Set. Eur. J. Phys. Rehabil. Med. 2015, 51, 105–117. [Google Scholar] [PubMed]
- Gómez-Benito, J.; Guilera, G.; Barrios, M.; Rojo, E.; Pino, O.; Gorostiaga, A.; Balluerka, N.; Hidalgo, M.D.; Padilla, J.L.J.L.; Benítez, I.; et al. Beyond diagnosis: The Core Sets for persons with schizophrenia based on the World Health Organization’s International Classification of Functioning, Disability, and Health. Disabil. Rehabil. 2018, 40, 2756–2766. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Sandford, B.A. The Delphi Technique: Making Sense of Consensus. Pract. Assess. Res. Eval. 2007, 12, 1–8. [Google Scholar]
- Trevelyan, E.G.; Robinson, N. Delphi methodology in health research: How to do it? Eur. J. Integr. Med. 2015, 7, 423–428. [Google Scholar] [CrossRef]
- Yousuf, M.I. Using experts’ opinions through Delphi technique. Pract. Assess. Res. Eval. 2007, 12, 4. [Google Scholar] [CrossRef]
- Nuño, L.; Barrios, M.; Rojo, E.; Gómez-Benito, J.; Guilera, G. Validation of the ICF Core Sets for schizophrenia from the perspective of psychiatrists: An international Delphi study. J. Psychiatr. Res. 2018, 103, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Nuño, L.; Guilera, G.; Coenen, M.; Rojo, E.; Gómez-Benito, J.; Barrios, M. Functioning in schizophrenia from the perspective of psychologists: A worldwide study. PLoS ONE 2019, 14, e0217936. [Google Scholar] [CrossRef]
- Nuño, L.; Barrios, M.; Moller, M.D.; Calderón, C.; Rojo, E.; Gómez-Benito, J.; Guilera, G. An international survey of Psychiatric-Mental-Health Nurses on the content validity of the International Classification of Functioning, Disability and Health Core Sets for Schizophrenia. Int. J. Ment. Health Nurs. 2019, 28, 867–878. [Google Scholar] [CrossRef]
- Nuño, L.; Guilera, G.; Bell, M.; Rojo, E.; Gómez-Benito, J.; Calderón, C.; Barrios, M. An Occupational therapist perspective of the ICF Core Sets for Schizophrenia. Am. J. Occup. Ther. 2021, 75. [Google Scholar] [CrossRef]
- Nuño, L.; Guilera, G.; Solomon, P.; Gómez-Benito, J.; Barrios, M. The Perspective of Social Workers on Functioning for Individuals with Schizophrenia: A Delphi Study. J. Soc. Social Work Res. 2021, 12. [Google Scholar] [CrossRef]
- Nuño, L.; Barrios, M.; Vancampfort, D.; Rojo, E.; Gómez-Benito, J.; Guilera, G. Functioning in schizophrenia: A Delphi study covering the perspective of physiotherapists. Disabil. Rehabil. 2020. [Google Scholar] [CrossRef]
- Cieza, A.; Fayed, N.; Bickenbach, J.; Prodinger, B. Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil. Rehabil. 2019, 41, 574–583. [Google Scholar] [CrossRef]
- Cieza, A.; Geyh, S.; Chatterji, S.; Kostanjsek, N.; Üstün, B.; Stucki, G. ICF linking rules: An update based on lessons learned. J. Rehabil. Med. 2005, 37, 212–218. [Google Scholar] [CrossRef]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Kaech Moll, V.M.; Escorpizo, R.; Portmann Bergamaschi, R.; Finger, M.E. Validation of the Comprehensive ICF Core Set for Vocational Rehabilitation from the Perspective of Physical Therapists: International Delphi Survey. Phys. Ther. 2016, 96, 1262–1275. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0.2016; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Zipursky, R.B.; Agid, O. Recovery, not progressive deterioration, should be the expectation in schizophrenia. World Psychiatry 2015, 14, 94–96. [Google Scholar] [CrossRef]
- Nowak, I.; Sabariego, C.; Świtaj, P.; Anczewska, M. Disability and recovery in schizophrenia: A systematic review of cognitive behavioral therapy interventions. BMC Psychiatry 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Tham, X.C.; Xie, H.; Chng, C.M.L.; Seah, X.Y.; Lopez, V.; Klainin-Yobas, P. Exploring predictors of medication adherence among inpatients with schizophrenia in Singapore’s mental health settings: A non-experimental study. Arch. Psychiatr. Nurs. 2018, 32, 536–548. [Google Scholar] [CrossRef]
- Gorczynski, P.; Faulkner, G. Exercise therapy for schizophrenia. Schizophr. Bull. 2010, 36, 665–666. [Google Scholar] [CrossRef]
- Ashcroft, R.; Mcmillan, C.; Ambrose-Miller, W.; Mckee, R.; Brown, J.B. The Emerging Role of Social Work in Primary Health Care: A Survey of Social Workers in Ontario Family Health Teams. Health Soc. Work. 2018, 109–118. [Google Scholar] [CrossRef]
- Best, M.W.; Bowie, C.R. A review of cognitive remediation approaches for schizophrenia: From top-down to bottom-up, brain training to psychotherapy. Expert Rev. Neurother. 2017, 17, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Vita, A.; Barlati, S.; Ceraso, A.; Nibbio, G.; Ariu, C.; Deste, G.; Wykes, T. Effectiveness, Core Elements, and Moderators of Response of Cognitive Remediation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Psychiatry 2021, 78, 848–858. [Google Scholar] [CrossRef]
- Kani, A.S.; Shinn, A.K.; Lewandowski, K.E.; Öngür, D. Converging effects of diverse treatment modalities on frontal cortex in schizophrenia: A review of longitudinal functional magnetic resonance imaging studies. J. Psychiatr. Res. 2017, 84, 256–276. [Google Scholar] [CrossRef][Green Version]
- Shimada, T.; Nishi, A.; Yoshida, T.; Tanaka, S.; Kobayashi, M. Development of an Individualized Occupational Therapy Programme and its Effects on the Neurocognition, Symptoms and Social Functioning of Patients with Schizophrenia. Occup. Ther. Int. 2016, 23, 425–435. [Google Scholar] [CrossRef]
- Díaz-Caneja, C.M.; Morón-Nozaleda, M.G.; Vicente-Moreno, R.P.; Rodríguez-Toscano, E.; Pina-Camacho, L.; de la Serna, E.; Sugranyes, G.; Baeza, I.; Romero, S.; Sánchez-Gistau, V.; et al. Temperament in child and adolescent offspring of patients with schizophrenia and bipolar disorder. Eur. Child Adolesc. Psychiatry 2018, 27, 1459–1471. [Google Scholar] [CrossRef]
- Rettew, D.C.; McKee, L. Temperament and Its Role in Developmental Psychopathology. Harv. Rev. Psychiatry 2005, 13, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Sevilla-Llewellyn-Jones, J.; Cano-Domínguez, P.; De-Luis-Matilla, A.; Espina-Eizaguirre, A.; Moreno-Küstner, B.; Ochoa, S. Personality traits in recent-onset-of-psychosis patients compared to a control sample by gender. Schizophr. Res. 2017, 195, 86–92. [Google Scholar] [CrossRef]
- Manu, P.; Dima, L.; Shulman, M.; Vancampfort, D.; De Hert, M.; Correll, C.U. Weight gain and obesity in schizophrenia: Epidemiology, pathobiology, and management. Acta Psychiatr. Scand. 2015, 132, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Gurusamy, J.; Gandhi, S.; Damodharan, D.; Ganesan, V.; Palaniappan, M. Exercise, diet and educational interventions for metabolic syndrome in persons with schizophrenia: A systematic review. Asian J. Psychiatr. 2018, 36, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Koychev, I.; El-Deredy, W.; Mukherjee, T.; Haenschel, C.; Deakin, J.F.W. Core dysfunction in schizophrenia: Electrophysiology trait biomarkers. Acta Psychiatr. Scand. 2012, 126, 59–71. [Google Scholar] [CrossRef]
- Chan, S.K.W.; Hui, C.L.M.; Chang, W.C.; Lee, E.H.M.; Chen, E.Y.H. Ten-year follow up of patients with first-episode schizophrenia spectrum disorder from an early intervention service: Predictors of clinical remission and functional recovery. Schizophr. Res. 2019, 204, 65–71. [Google Scholar] [CrossRef]
- Fitzsimmons, J.; Kubicki, M.; Shenton, M.E. Review of functional and anatomical brain connectivity findings in schizophrenia. Curr. Opin. Psychiatry 2013, 26, 172–187. [Google Scholar] [CrossRef]
- Ira, E.; Zanoni, M.; Ruggeri, M.; Dazzan, P.; Tosato, S.; Ira, E. COMT, neuropsychological function and brain structure in schizophrenia: A systematic review and neurobiological interpretation. J. Psychiatry Neurosci. 2013, 38, 366–380. [Google Scholar] [CrossRef]
- van den Heuvel, M.P.; Fornito, A. Brain Networks in Schizophrenia. Neuropsychol. Rev. 2014, 24, 32–48. [Google Scholar] [CrossRef]
- Hutcheson, N.L.; Sreenivasan, K.R.; Deshpande, G.; Reid, M.A.; Hadley, J.; White, D.M.; Ver Hoef, L.; Lahti, A.C. Effective connectivity during episodic memory retrieval in schizophrenia participants before and after antipsychotic medication. Hum. Brain Mapp. 2015, 36, 1442–1457. [Google Scholar] [CrossRef]
- Chang, Y.-T.; Tao, S.-G.; Lu, C.-L. Qualitative inquiry into motivators for maintaining medication adherence among Taiwanese with schizophrenia. Int. J. Ment. Health Nurs. 2013, 22, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Morton, N.K.; Zubek, D. Adherence challenges and long-acting injectable antipsychotic treatment in patients with schizophrenia. J. Psychosoc. Nurs. Ment. Health Serv. 2013, 51, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Cella, M.; Preti, A.; Edwards, C.; Dow, T.; Wykes, T. Cognitive remediation for negative symptoms of schizophrenia: A network meta-analysis. Clin. Psychol. Rev. 2017, 52, 43–51. [Google Scholar] [CrossRef]
- Kurtz, M.M.; Richardson, C.L. Social cognitive training for schizophrenia: A meta-analytic investigation of controlled research. Schizophr. Bull. 2012, 38, 1092–1104. [Google Scholar] [CrossRef]
- Roder, V.; Mueller, D.R.; Schmidt, S.J. Effectiveness of integrated psychological therapy (IPT) for schizophrenia patients: A research update. Schizophr. Bull. 2011, 37, S71–S79. [Google Scholar] [CrossRef]
- Mason, L.; Peters, E.R.; Dima, D.; Williams, S.C.; Kumari, V. Cognitive behavioral therapy normalizes functional connectivity for social threat in psychosis. Schizophr. Bull. 2016, 42, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Penadés, R.; Pujol, N.; Catalán, R.; Massana, G.; Rametti, G.; García-Rizo, C.; Bargalló, N.; Gastó, C.; Bernardo, M.; Junqué, C. Brain effects of cognitive remediation therapy in schizophrenia: A structural and functional neuroimaging study. Biol. Psychiatry 2013, 73, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Probst, M.; De Hert, M.; Soundy, A.; Stubbs, B.; Stroobants, M.; De Herdt, A. Neurobiological effects of physical exercise in schizophrenia: A systematic review. Disabil. Rehabil. 2014, 36, 1749–1754. [Google Scholar] [CrossRef]
- Cordeiro, K.; Foroughe, M.; Mastorakos, T. Primary Mental Health Care in the Family Health Team Setting: Tracking Patient Care from Referral to Outcome. Can. J. Community Ment. Heal. 2015, 34, 51–65. [Google Scholar] [CrossRef]
- Lindenmayer, J.-P.; McGurk, S.R.; Khan, A.; Kaushik, S.; Thanju, A.; Hoffman, L.; Valdez, G.; Wance, D.; Herrmann, E. Improving social cognition in schizophrenia: A pilot intervention combining computerized social cognition training with cognitive remediation. Schizophr. Bull. 2013, 39, 507–517. [Google Scholar] [CrossRef]
- Mueller, D.R.; Schmidt, S.J.; Roder, V. One-year randomized controlled trial and follow-up of integrated neurocognitive therapy for schizophrenia outpatients. Schizophr. Bull. 2015, 41, 604–616. [Google Scholar] [CrossRef]
- Pinkham, A.E.; Harvey, P.D. Future directions for social cognitive interventions in schizophrenia. Schizophr. Bull. 2013, 39, 499–500. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Quee, P.J.; Stiekema, A.P.M.; Wigman, J.T.W.; Schneider, H.; van der Meer, L.; Maples, N.J.; van den Heuvel, E.R.; Velligan, D.I.; Bruggeman, R. Improving functional outcomes for schizophrenia patients in the Netherlands using Cognitive Adaptation Training as a nursing intervention—A pilot study. Schizophr. Res. 2014, 158, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Bowie, C.R.; McGurk, S.R.; Mausbach, B.; Patterson, T.L.; Harvey, P.D. Combined cognitive remediation and functional skills training for schizophrenia: Effects on cognition, functional competence, and real-world behavior. Am. J. Psychiatry 2012, 169, 710–718. [Google Scholar] [CrossRef]
- Harvey, P.D.; Bellack, A.S. Toward a terminology for functional recovery in schizophrenia: Is functional remission a viable concept? Schizophr. Bull. 2009, 35, 300–306. [Google Scholar] [CrossRef]
- Slade, M.; Longden, E. Empirical evidence about recovery and mental health. BMC Psychiatry 2015, 15, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bailey, K.P. Choosing between atypical antipsychotics: Weighing the risks and benefits. Arch. Psychiatr. Nurs. 2002, 16, S2–S11. [Google Scholar] [CrossRef] [PubMed]
- Kern, R.S.; Glynn, S.M.; Horan, W.P.; Marder, S.R. Psychosocial treatments to promote functional recovery in Schizophrenia. Schizophr. Bull. 2009, 35, 347–361. [Google Scholar] [CrossRef]
- Adams, J.R.; Drake, R.E. Shared decision-making and evidence-based practice. Community Ment. Health J. 2006, 42, 87–105. [Google Scholar] [CrossRef]
- Ashcroft, R.; Kourgiantakis, T.; Fearing, G.; Robertson, T.; Brown, J.B. Social Work’s Scope of Practice in Primary Mental Health Care: A Scoping Review. Br. J. Soc. Work 2019, 49, 318–334. [Google Scholar] [CrossRef]
- Morris, K.; Reid, G.; Spencer, S. Occupational therapy delivered by specialists versus non-specialists for people with schizophrenia. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Juntapim, S.; Nuntaboot, K. Care of patients with schizophrenia in the community. Arch. Psychiatr. Nurs. 2018, 32, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.A.; Weisman de Mamani, A. The mediating effect of family cohesion in reducing patient symptoms and family distress in a culturally informed family therapy for schizophrenia: A parallel-process latent-growth model. J. Consult. Clin. Psychol. 2018, 86, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Niendam, T.A.; Tully, L.M.; Iosif, A.-M.; Kumar, D.; Nye, K.E.; Denton, J.C.; Zakskorn, L.N.; Fedechko, T.L.; Pierce, K.M. Enhancing early psychosis treatment using smartphone technology: A longitudinal feasibility and validity study. J. Psychiatr. Res. 2018, 96, 239–246. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, W.R. Family Interventions for Schizophrenia and the Psychoses: A Review. Fam. Process. 2016, 55, 460–482. [Google Scholar] [CrossRef]
- Okpokoro, U.; Adams, C.E.; Sampson, S. Family intervention (brief) for schizophrenia. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Fox, J.; Ramon, S.; Morant, N. Exploring the Meaning of Recovery for Carers: Implications for Social Work Practice. Br. J. Soc. Work 2015, 45, i117–i134. [Google Scholar] [CrossRef]
- Gurak, K.; De Mamani, A.W. Risk and protective factors, perceptions of family environment, ethnicity, and schizophrenia symptoms. J. Nerv. Ment. Dis. 2016, 204, 570–577. [Google Scholar] [CrossRef]
- O’Donoghue, B.; Lyne, J.; Madigan, K.; Lane, A.; Turner, N.; O’Callaghan, E.; Clarke, M. Environmental factors and the age at onset in first episode psychosis. Schizophr. Res. 2015, 168, 106–112. [Google Scholar] [CrossRef]
- Bhalla, I.P.; Stefanovics, E.A.; Rosenheck, R.A. Mental health multimorbidity and poor quality of life in patients with schizophrenia. Schizophr. Res. 2018, 201, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, Z.; Burton, C.Z.; Vella, L.; Twamley, E.W. Neuropsychological predictors of performance-based measures of functional capacity and social skills in individuals with severe mental illness. J. Psychiatr. Res. 2018, 102, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Kendler, K.S.; Ohlsson, H.; Keefe, R.S.E.; Sundquist, K.; Sundquist, J. The joint impact of cognitive performance in adolescence and familial cognitive aptitude on risk for major psychiatric disorders: A delineation of four potential pathways to illness. Mol. Psychiatry 2018, 23, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.E.; Martin, A.S.; Tu, X.; Palmer, B.W.; Jeste, D.V. Childhood Adversity and Schizophrenia: The Protective Role of Resilience in Mental and Physical Health and Metabolic Markers. J. Clin. Psychiatry 2018, 79. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. The Impact of Childhood Adversity on the Clinical Features of Schizophrenia. Schizophr. Res. Treatment 2015, 2015, 532082. [Google Scholar] [CrossRef]
- Torgalsbøen, A.-K.; Fu, S.; Czajkowski, N. Resilience trajectories to full recovery in first-episode schizophrenia. Eur. Psychiatry 2018, 52, 54–60. [Google Scholar] [CrossRef] [PubMed]
- van Erp, T.G.M.; Walton, E.; Hibar, D.P.; Schmaal, L.; Jiang, W.; Glahn, D.C.; Pearlson, G.D.; Yao, N.; Fukunaga, M.; Hashimoto, R.; et al. Cortical Brain Abnormalities in 4474 Individuals with Schizophrenia and 5098 Control Subjects via the Enhancing Neuro Imaging Genetics through Meta Analysis (ENIGMA) Consortium. Biol. Psychiatry 2018, 84, 644–654. [Google Scholar] [CrossRef]
- Goghari, V.M. Personality dimensions in schizophrenia: A family study. Psychiatry Res. 2017, 251, 162–167. [Google Scholar] [CrossRef]
- Leeson, V.C.; Sharma, P.; Harrison, M.; Ron, M.A.; Barnes, T.R.E.; Joyce, E.M. IQ trajectory, cognitive reserve, and clinical outcome following a first episode of psychosis: A 3-year longitudinal study. Schizophr. Bull. 2011, 37, 768–777. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Borgwardt, S.; Bechdolf, A.; Addington, J.; Riecher-Rössler, A.; Schultze-Lutter, F.; Keshavan, M.; Wood, S.; Ruhrmann, S.; Seidman, L.J.; et al. The psychosis high-risk state: A comprehensive state-of-the-art review. JAMA 2013, 70, 107–120. [Google Scholar] [CrossRef] [PubMed]
- DeVylder, J.E. Preventing Schizophrenia and Severe Mental Illness: A Grand Challenge for Social Work. Res. Soc. Work Pract. 2016, 26, 449–459. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Professional Ambit | Round 1 n(%) | Women n (%) | Age Average (Rank) | Years of Experience Average (Rank) | WHO Region | Countries n | Treated Population g | Round 3 n (%) h | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| African a n (%) | Americas b n (%) | Eastern Mediterranean c n (%) | European d n (%) | South-East Asia e n (%) | Western Pacific f n (%) | Acute n (%) | Chronic n (%) | Rural n (%) | Urban n (%) | |||||||
| Psychiatry | 352 (44.5) | 99 (28.1) | 47.6 (29–81) | 19.5 (4–55) | 26 (7.4) | 72 (20.4) | 17 (4.8) | 82 (23.3) | 77 (21.9) | 78 (22.2) | 63 | 325 (92.3) | 315 (89.5) | 207 (58.8) | 303 (86.1) | 303 (86.1) |
| Psychology | 175 (22.2) | 110 (62.9) | 41.8 (24–67) | 11.7 (1–42) | 11 (6.3) | 47 (26.9) | 21 (12.0) | 63 (36.0) | 20 (11.4) | 13 (7.4) | 46 | 92 (52.6) | 149 (85.1) | 60 (34.3) | 130 (74.3) | 137 (78.3) |
| Nursing | 101 (12.8) | 64 (63.3) | 45.8 (24–74) | 20.7 (2–54) | 5 (4.9) | 25 (24.7) | 9 (8.9) | 31 (30.6) | 13 (12.7) | 18 (17.8) | 30 | 82 (81.2) | 89 (88.2) | 45 (44.6) | 69 (68.3) | 79 (78.2) |
| Occupational therapy | 92 (11.6) | 76 (82.6) | 37.7 (23–67) | 9.9 (1–44) | 13 (14.1) | 16 (17.4) | 7 (7.6) | 42 (45.7) | 5 (5.4) | 9 (9.8) | 29 | 49 (53.3) | 79 (85.9) | 31 (33.7) | 60 (65.2) | 73 (79.3) |
| Social work | 57 (7.2) | 39 (68.4) | 45.1 (26–72) | 10.3 (1–27) | 2 (3.5) | 17 (29.8) | 1 (1.8) | 13 (22.8) | 11 (19.3) | 13 (22.8) | 20 | 28 (49.1) | 53 (93.0) | 24 (42.1) | 43 (75.4) | 36 (63.2) |
| Physiotherapy | 13 (1.6) | 7 (53.8) | 43.2 (32–62) | 10.5 (1–30) | 0 | 2 (15.4) | 0 | 7 (53.8) | 1 (7.7) | 3 (23.1) | 8 | 7 (53.8) | 12 (92.3) | 3 (23.1) | 7 (53.8) | 10 (76.9) |
| Total | 790 | 307 (48.1) | 45.5 (23–81) | 15.8 (1–55) | 57 (7.2) | 179 (22.6) | 55 (7.0) | 238 (30.1) | 127 (16.1) | 134 (17.0) | 85 | 583 (73.8) | 697 (88.2) | 370 (46.8) | 612 (77.5) | 638 (80.8) |
| Number of Categories | Body Functions | Body Structures | Activities and Participation | Environmental Factors | Total |
|---|---|---|---|---|---|
| Categories that achieved consensus from at least one professional perspective | 21 | 2 | 50 | 40 | 113 |
| Categories in the ICF-CS for schizophrenia | 17 | 0 | 48 | 32 | 97 |
| Categories that achieved expert consensus a | 17 | 1 | 39 | 33 | 90 |
| ICF-CS categories for which expert consensus was achieved | 16 | 0 | 39 | 32 | 87 |
| ICF Component | ICF Category | Perspectives from Achieving Consensus | Number of Perspectives from Which Achieved Consensus | |
|---|---|---|---|---|
| Categories that achieved expert consensus a and are not present in the ICF-CS | Body functions | b126 Temperament and personality functions | All | 6 |
| Body structures | s110 Structure of brain | All | 6 | |
| Environmental factors | e135 Products and technology for employment | PC, PS, NS, OT | 4 | |
| ICF-CS categories for schizophrenia that did not achieve expert consensus | Body functions | b530 Weight maintenance functions | PC, NS, PH | 3 |
| Activities and Participation | d330 Speaking | SW, PH | 2 | |
| d475 Driving | OT, PH | 2 | ||
| d510 Washing oneself | OT, SW | 2 | ||
| d540 Dressing | NS, OT | 2 | ||
| d166 Reading | PH | 1 | ||
| d210 Undertaking a single task | OT | 1 | ||
| d470 Using transportation | OT | 1 | ||
| d860 Basic economic transactions | OT | 1 | ||
| d930 Religion and spirituality | OT | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuño, L.; Guilera, G.; Rojo, E.; Gómez-Benito, J.; Barrios, M. An Integrated Account of Expert Perspectives on Functioning in Schizophrenia. J. Clin. Med. 2021, 10, 4223. https://doi.org/10.3390/jcm10184223
Nuño L, Guilera G, Rojo E, Gómez-Benito J, Barrios M. An Integrated Account of Expert Perspectives on Functioning in Schizophrenia. Journal of Clinical Medicine. 2021; 10(18):4223. https://doi.org/10.3390/jcm10184223
Chicago/Turabian StyleNuño, Laura, Georgina Guilera, Emilio Rojo, Juana Gómez-Benito, and Maite Barrios. 2021. "An Integrated Account of Expert Perspectives on Functioning in Schizophrenia" Journal of Clinical Medicine 10, no. 18: 4223. https://doi.org/10.3390/jcm10184223
APA StyleNuño, L., Guilera, G., Rojo, E., Gómez-Benito, J., & Barrios, M. (2021). An Integrated Account of Expert Perspectives on Functioning in Schizophrenia. Journal of Clinical Medicine, 10(18), 4223. https://doi.org/10.3390/jcm10184223