
Prevalence and Prognostic Impact of Deranged Liver Blood Tests in COVID-19: Experience from the Regional COVID-19 Center over the Cohort of 3812 Hospitalized Patients

 , , , , , , ,
, , , , , , ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Methods
2.4. Ethical Issues
3. Results
3.1. Patients’ Characteristics
3.2. Relationship between Patients’ Characteristics and the Profile of LBTs at Admission
3.3. Relationship of LBTs with COVID-19 Severity at Admission
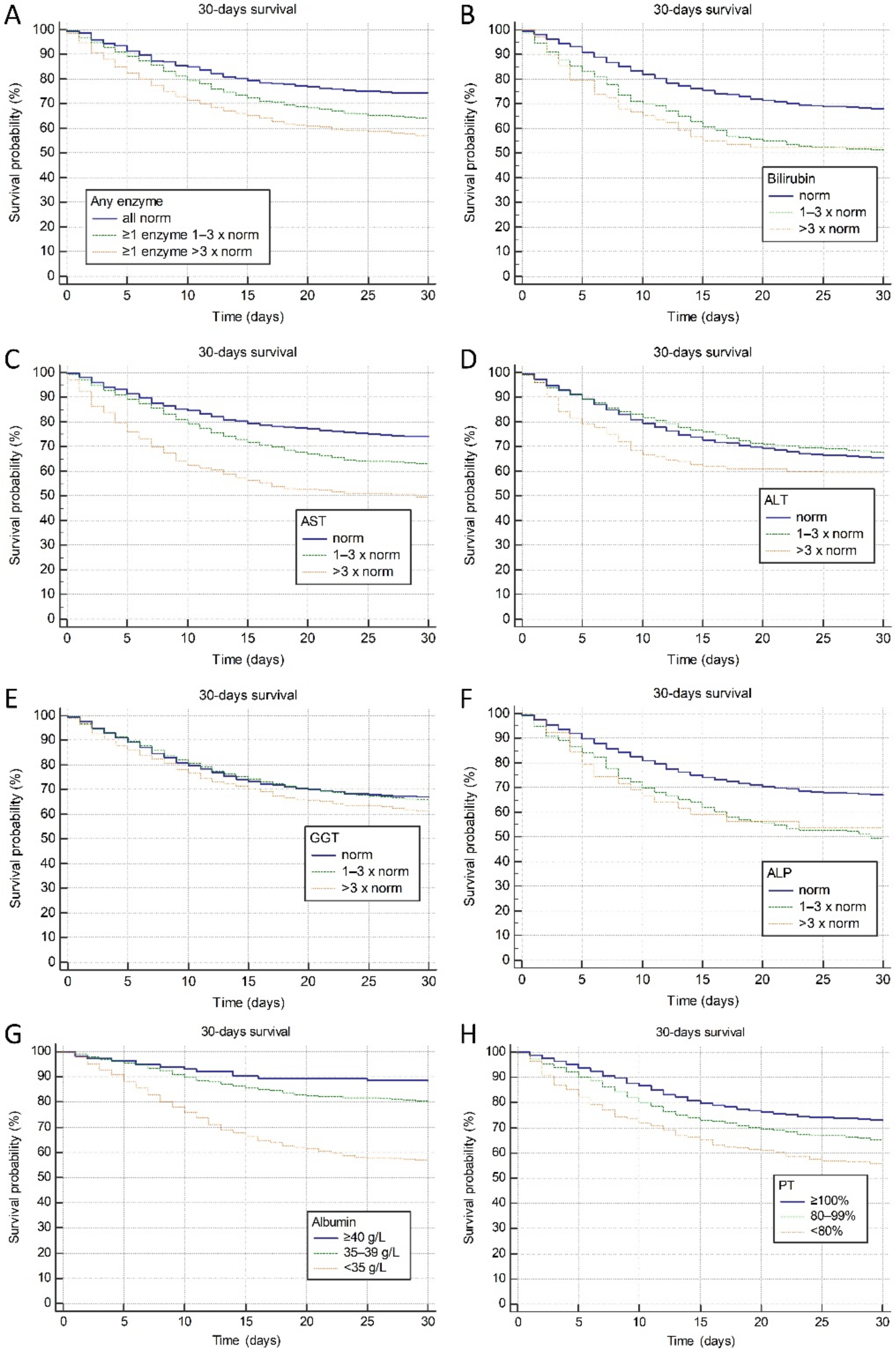
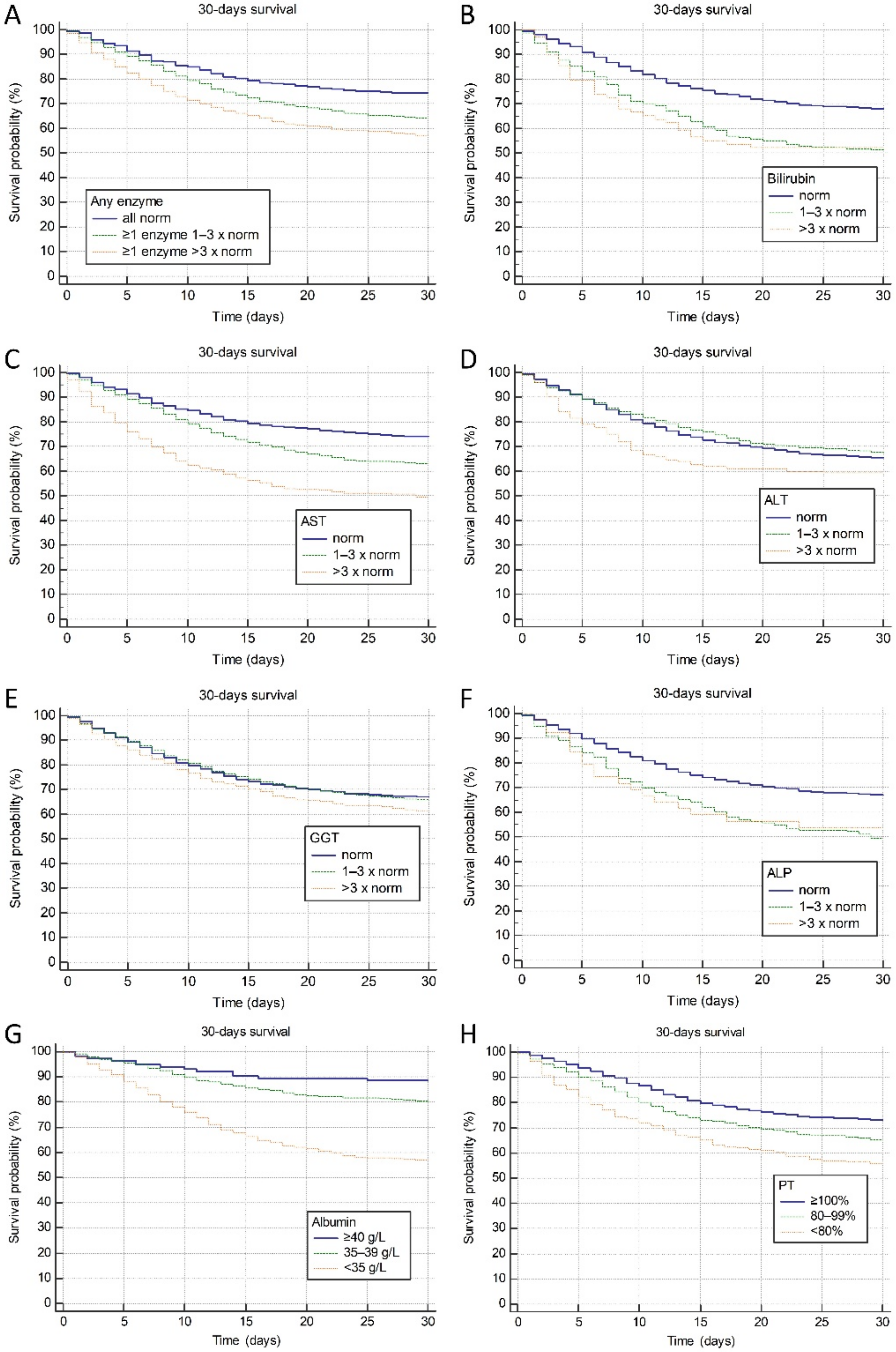
3.4. Associations between Deranged LBTs at Admission and Clinical Outcomes
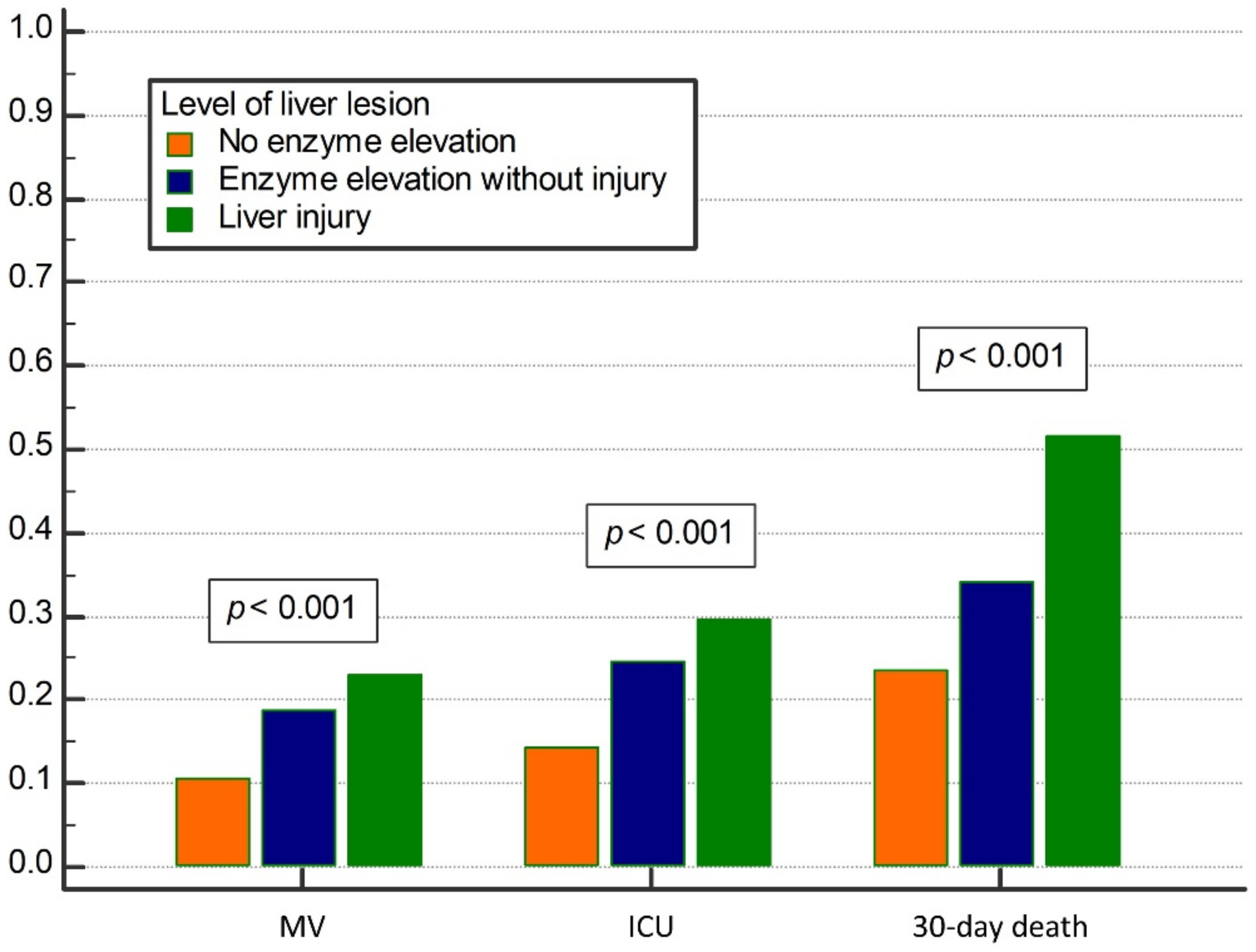
3.5. Associations between the Presence of Liver Injury at Admission and Clinical Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Bloom, P.P.; Meyerowitz, E.A.; Reinus, Z.; Daidone, M.; Gustafson, J.; Kim, A.Y.; Schaefer, E.; Chung, R.T. Liver Biochemistries in Hospitalized Patients with COVID-19. Hepatology 2021, 73, 890–900. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal liver function tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S., 4th; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Chew, M.; Tang, Z.; Radcliffe, C.; Caruana, D.; Doilicho, N.; Ciarleglio, M.M.; Deng, Y.; Garcia-Tsao, G. Significant Liver Injury during Hospitalization for COVID-19 Is Not Associated with Liver Insufficiency or Death. Clin. Gastroenterol. Hepatol. 2021, 19, 2182–2191.e7. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Choudhury, A.; Lau, G.K.; Zheng, M.H.; Ji, D.; Abd-Elsalam, S.; Hwang, J.; Qi, X.; Cua, I.H.; Suh, J.I.; et al. APASL COVID Task Force, APASL COVID Liver Injury Spectrum Study (APCOLIS Study-NCT 04345640). Pre-existing liver disease is associated with poor outcome in patients with SARS CoV2 infection; The APCOLIS Study (APASL COVID-19 Liver Injury Spectrum Study). Hepatol. Int. 2020, 14, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.Y.; Li, G.X.; Chen, L.; Shu, C.; Song, J.; Wang, W.; Wang, Y.W.; Chen, Q.; Jin, G.N.; Liu, T.T.; et al. Tongji Multidisciplinary Team for Treating COVID-19 (TTTC) Association of liver abnormalities with in-hospital mortality in patients with COVID-19. J. Hepatol. 2021, 74, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.S.; Tan, J.Y.; Li, X.H.; Liang, J.; Shen, J.; Zhu, L.R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Del Zompo, F.; Nesci, A.; Santopaolo, F.; Ianiro, G.; Pompili, M.; Gasbarrini, A.; “Gemelli against COVID-19” Group. Liver involvement is not associated with mortality: Results from a large cohort of SARS-CoV-2-positive patients. Aliment. Pharmacol. Ther. 2020, 52, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, L.; Liu, L.; Zhao, M.; Xiao, J.; Zhao, Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020, 40, 2095–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piano, S.; Dalbeni, A.; Vettore, E.; Benfaremo, D.; Mattioli, M.; Gambino, C.G.; Framba, V.; Cerruti, L.; Mantovani, A.; Martini, A.; et al. COVID-LIVER study group. Abnormal liver function tests predict transfer to intensive care unit and death in COVID-19. Liver Int. 2020, 40, 2394–2406. [Google Scholar] [CrossRef] [PubMed]
- Bangash, M.N.; Patel, J.M.; Parekh, D.; Murphy, N.; Brown, R.M.; Elsharkawy, A.M.; Mehta, G.; Armstrong, M.J.; Neil, D. SARS-CoV-2: Is the liver merely a bystander to severe disease? J. Hepatol. 2020, 73, 995–996. [Google Scholar] [CrossRef]
- Bangash, M.N.; Patel, J.; Parekh, D. COVID-19 and the liver: Little cause for concern. Lancet Gastroenterol. Hepatol. 2020, 5, 529–530. [Google Scholar] [CrossRef] [Green Version]
- Jothimani, D.; Venugopal, R.; Abedin, M.F.; Kaliamoorthy, I.; Rela, M. COVID-19 and the liver. J. Hepatol. 2020, 73, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Demirtas, C.O.; Keklikkiran, C.; Ergenc, I.; Sengel, B.E.; Eskidemir, G.; Cinel, I.; Odabasi, Z.; Korten, V.; Yilmaz, Y. Liver stiffness is associated with disease severity and worse clinical scenarios in coronavirus disease 2019: A prospective transient elastography study. Int. J. Clin. Pract. 2021, 75, e14363. [Google Scholar] [CrossRef]
- Campos-Varela, I.; Villagrasa, A.; Simon-Talero, M.; Riveiro-Barciela, M.; Ventura-Cots, M.; Aguilera-Castro, L.; Alvarez-Lopez, P.; Nordahl, E.A.; Anton, A.; Bañares, J.; et al. The role of liver steatosis as measured with transient elastography and transaminases on hard clinical outcomes in patients with COVID-19. Therap. Adv. Gastroenterol. 2021, 14, 17562848211016567. [Google Scholar] [CrossRef]
- The Ministry of Health of the Republic of Croatia. Guidelines for Treatment of Patients with COVID-19, Version 2. 2020. Available online: https://zdravlje.gov.hr/UserDocsImages//2020%20CORONAVIRUS//Smjernice%20za%20lije%C4%8Denje%20oboljelih%20od%20koronavirusne%20bolesti%202019%20(COVID-19),%20verzija%202%20od%2019.%20studenoga%202020.pdf (accessed on 15 June 2021).
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.N.; Cramb, R.; Davison, S.M.; Dillon, J.F.; Foulerton, M.; Godfrey, E.M.; Hall, R.; Harrower, U.; Hudson, M.; Langford, A.; et al. Guidelines on the management of abnormal liver blood tests. Gut 2018, 67, 6–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hundt, M.A.; Deng, Y.; Ciarleglio, M.M.; Nathanson, M.H.; Lim, J.K. Abnormal Liver Tests in COVID-19: A Retrospective Observational Cohort Study of 1,827 Patients in a Major U.S. Hospital Network. Hepatology 2020, 72, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Altayar, O.; Siddique, S.M.; Davitkov, P.; Feuerstein, J.D.; Lim, J.K.; Falck-Ytter, Y.; El-Serag, H.B.; AGA Institute. AGA Institute Rapid Review of the Gastrointestinal and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology 2020, 159, 320–334.e27. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Zhao, X.; Wang, Y.; Zhu, J.; Ma, C.; Feng, X.; Ma, Y.; Zheng, Y.; Yang, L.; Han, G.; et al. Abnormal Liver Function Tests Were Associated with Adverse Clinical Outcomes: An Observational Cohort Study of 2912 Patients with COVID-19. Front. Med. 2021, 8, 639855. [Google Scholar] [CrossRef] [PubMed]
- Pirola, C.J.; Sookoian, S. SARS-CoV-2 virus and liver expression of host receptors: Putative mechanisms of liver involvement in COVID-19. Liver Int. 2020, 40, 2038–2040. [Google Scholar] [CrossRef]
- Sonzogni, A.; Previtali, G.; Seghezzi, M.; Grazia Alessio, M.; Gianatti, A.; Licini, L.; Morotti, D.; Zerbi, P.; Carsana, L.; Rossi, R.; et al. Liver histopathology in severe COVID 19 respiratory failure is suggestive of vascular alterations. Liver Int. 2020, 40, 2110–2116. [Google Scholar] [CrossRef] [PubMed]
- Nie, X.; Qian, L.; Sun, R.; Huang, B.; Dong, X.; Xiao, Q.; Zhang, Q.; Lu, T.; Yue, L.; Chen, S.; et al. Multi-organ proteomic landscape of COVID-19 autopsies. Cell 2021, 184, 775–791.e14. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, S.; Liu, H.; Li, W.; Lin, F.; Jiang, L.; Li, X.; Xu, P.; Zhang, L.; Zhao, L.; et al. SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19. J. Hepatol. 2020, 73, 807–816. [Google Scholar] [CrossRef]
- Roth, N.C.; Kim, A.; Vitkovski, T.; Xia, J.; Ramirez, G.; Bernstein, D.; Crawford, J.M. Post-COVID-19 Cholangiopathy: A Novel Entity. Am. J. Gastroenterol. 2021, 116, 1077–1082. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| N (%), Median (IQR) | |
|---|---|
| Total number of patients | 3812 |
| Age (years) | 74 (64–82) |
| Sex | |
| Female | 1664 (43.7%) |
| Male | 2148 (56.3%) |
| Arterial hypertension | |
| Yes | 2658 (69.7%) |
| No | 1154 (30.3%) |
| Diabetes mellitus | |
| Yes | 1154 (30.3%) |
| No | 2658 (69.7%) |
| Obesity (Body mass index ≥ 30 kg/m2) | |
| Yes | 1023 (28.6%) |
| No | 2554 (71.4%) |
| Congestive heart failure | |
| Yes | 617 (16.2%) |
| No | 3195 (82.8%) |
| Chronic kidney disease | |
| Yes | 474 (12.4%) |
| No | 3338 (87.6%) |
| Chronic liver disease | |
| Yes | 106 (2.8%) |
| No | 3706 (97.2%) |
| Liver cirrhosis | |
| Yes | 49 (1.3%) |
| No | 3763 (98.7%) |
| Charlson comorbidity index | 4 IQR (3–6) |
| Alcohol use | |
| Yes | 207 (5.4%) |
| No | 3605 (94.6%) |
| Smoking | |
| Yes | 434 (11.4%) |
| No | 3378 (88.6%) |
| Number of drugs in chronic therapy | 5 (3–8) |
| Statin use | |
| Yes | 911 (23.9%) |
| No | 2901 (76.1%) |
| Antibiotic therapy before admission | |
| Yes | 1285 (33.7%) |
| No | 2527 (66.3%) |
| Oral anticoagulant therapy | |
| Yes | 1049 (27.5%) |
| No | 2763 (72.5%) |
| AST (U/L) | 41 (28–64) |
| ALT (U/L) | 31 (19–52) |
| GGT (U/L) | 42 (24–81) |
| ALP (U/L) | 72 (56–97) |
| Total bilirubin (umol/L) | 11.4 (8.6–15.9) |
| Albumin (g/L) | 32 (28–35) |
| Prothrombin time (%, Quick) * | 100% (89–109%) |
| Liver blood tests (any) | |
| Normal level | 958 (25.1%) |
| Deranged | 2854 (74.9%) |
| White blood cell count (×109/L) | 8 (5.8–11.2) |
| Hemoglobin (g/L) | 128 (113–141) |
| Platelets (×109/L) | 221 (163–297) |
| C-reactive protein (mg/L) | 88.7 (39.5–151) |
| Ferritin (ug/L) | 711 (386–1289) |
| D-dimers (mg/L) | 1.42 (0.73–3.6) |
| Day of disease on admission | 5 (1–9) |
| ECOG status | 3 (1–4) |
| Pneumonia | |
| Yes | 3390 (88.9%) |
| No | 422 (11.1%) |
| Oxygen therapy | |
| Yes | 3136 (82.3%) |
| No | 676 (17.7%) |
| MEWS severity | |
| Mild | 392 (10.3%) |
| Moderate | 196 (5.1%) |
| Severe | 2652 (69.6%) |
| Critical | 572 (15%) |
| ICU admission | |
| Yes | 881 (23.1%) |
| No | 2931 (76.9%) |
| Mechanical ventilation | |
| Yes | 659 (17.3%) |
| No | 3153 (82.7%) |
| 30-day mortality | |
| Yes | 1315 (34.5%) |
| No | 2497 (65.5%) |
| Overall/Any Enzyme | AST (U/L) | ALT (U/L) | GGT (U/L) | ALP (U/L) | Bilirubin (umol/L) | Albumin (g/L) | PT (%, Quick) | |
|---|---|---|---|---|---|---|---|---|
| Length of hospitalization | 10 IQR (6–16) | Rho = 0; p = 0.852 | Rho = −0.01; p = 0.516 | Rho = 0.03; p = 0.111 | Rho = 0; p = 0.965 | Rho = −0.02; p = 0.141 | Rho = −0.06; p = 0.008 * | Rho = 0.01; p = 0.534 |
| Intensive care unit | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 879 (23.1%) | 47.5 | 34 | 47 | 72 | 11.7 | 30 | 100% |
| No | 2933 (76.9%) | 39 | 29 | 40 | 72 | 11.3 | 32 | 101% |
| p < 0.001 * | p < 0.001 * | p < 0.001 * | p = 0.486 | p = 0.022 * | p < 0.001 * | p = 0.283 | ||
| High-flow oxygenation | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 758 (19.9%) | 49 | 35 | 51 | 72 | 11.5 | 31 | 102% |
| No | 3054 (80.1%) | 39 | 29 | 40 | 72 | 11.3 | 32 | 101% |
| p < 0.001 * | p < 0.001 * | p < 0.001 * | p = 0.829 | p = 0.481 | p < 0.001 * | p = 0.528 | ||
| Mechanical ventilation | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 660 (17.3%) | 48 | 34 | 49 | 73 | 11.8 | 30 | 101% |
| No | 3152 (82.7%) | 40 | 30 | 40 | 72 | 11.3 | 32 | 101% |
| p < 0.001 * | p < 0.001 * | p < 0.001 * | p = 0.606 | p = 0.109 | p < 0.001 * | p = 0.698 | ||
| Venous thrombosis | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 207 (5.4%) | 38 | 30 | 46 | 75 | 11.9 | 30.5 | 94% |
| No | 3605 (94.6%) | 41 | 31 | 42 | 72 | 11.3 | 32 | 101% |
| p = 0.011 * | p = 0.608 | p = 0.665 | p = 0.035 * | p = 0.214 | p = 0.009 * | p < 0.001 * | ||
| Arterial thrombosis | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 213 (5.6%) | 42.5 | 29 | 36 | 74 | 11.8 | 32 | 100% |
| No | 3599 (94.4%) | 41 | 31 | 42 | 72 | 11.4 | 32 | 101% |
| p = 0.688 | p = 0.204 | p = 0.061 | p = 0.461 | p = 0.664 | p = 0.225 | p = 0.848 | ||
| Bleeding | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 304 (8%) | 39 | 29 | 41 | 75 | 11.3 | 30 | 98% |
| No | 3508 (92%) | 41 | 31 | 42 | 72 | 11.4 | 32 | 101% |
| p = 0.310 | p = 0.085 | p = 0.210 | p = 0.042 * | p = 0.835 | p < 0.001 * | p = 0.018 * | ||
| 30-day death | Median | Median | Median | Median | Median | Median | Median | |
| Yes | 1315 (34.5%) | 48 | 30 | 43 | 77.5 | 12.3 | 30 | 97.5% |
| No | 2497 (65.5%) | 38 | 31 | 41 | 69 | 11 | 33 | 102% |
| p < 0.001 * | p = 0.812 | p = 0.199 | p < 0.001 * | p < 0.001 * | p < 0.001 * | p < 0.001 * |
| LBT | × ULN | 30-Day Survival (%) | Hazard Ratio vs. Normal (95% CI) | p for Trend | p for Difference |
|---|---|---|---|---|---|
| AST (U/L) | N | 74 | Reference | <0.001 | <0.001 |
| 1–3 | 63 | 1.5 (1.33–1.68) | |||
| >3 | 50 | 2.42 (1.97–2.98) | |||
| ALT (U/L) | N | 66 | Reference | 0.631 | 0.021 |
| 1–3 | 68 | 0.92 (0.82–1.04) | |||
| >3 | 59 | 1.32 (0.99–1.74) | |||
| GGT (U/L) | N | 67 | Reference | 0.034 | 0.056 |
| 1–3 | 66 | 1.03 (0.92–1.17) | |||
| >3 | 61 | 1.23 (1.03–1.47) | |||
| ALP (U/L) | N | 67 | Reference | <0.001 | <0.001 |
| 1–3 | 50 | 1.72 (1.37–2.14) | |||
| >3 | 54 | 1.61 (0.91–2.85) | |||
| Bilirubin (umol/L) | N | 68 | Reference | <0.001 | <0.001 |
| 1–3 | 52 | 1.73 (1.42–2.09) | |||
| >3 | 52 | 1.79 (1.15–2.78) | |||
| Albumin (g/L) | >40 | 89 | Reference | <0.001 | <0.001 |
| 35–40 | 80 | 1.77 (1.29–2.43) | |||
| <35 | 57 | 4.55 (3.39–6.12) | |||
| PT (%, Quick) | ≥100 | 73 | Reference | <0.001 | <0.001 |
| 80–99 | 66 | 1.36 (1.19–1.57) | |||
| <80 | 56 | 1.92 (1.52–2.43) |
| Covariate | p | HR | 95% CI for HR |
|---|---|---|---|
| Age (years) | <0.001 * | 1.0311 | 1.0207 to 1.0416 |
| Male sex | 0.137 | 1.1593 | 0.9542 to 1.4086 |
| Obesity | 0.796 | 1.0272 | 0.8385 to 1.2582 |
| Charlson comorbidity index | <0.001 * | 1.1270 | 1.0831 to 1.1727 |
| COVID severity severe vs. mild | <0.001 * | 13.1424 | 4.1771 to 41.3497 |
| COVID severity critical vs. mild | <0.001 * | 28.2629 | 8.8608 to 90.1489 |
| AST 1–3 × elevated vs. normal | <0.001 * | 1.5081 | 1.2089 to 1.8814 |
| AST >3 × elevated vs. normal | <0.001 * | 2.1315 | 1.3957 to 3.2552 |
| ALT 1–3 × elevated vs. normal | <0.001 * | 0.6432 | 0.5042 to 0.8206 |
| ALT >3 × elevated vs. normal | 0.053 | 0.5762 | 0.3296 to 1.0072 |
| GGT 1–3 × elevated vs. normal | 0.236 | 1.1393 | 0.9185 to 1.4131 |
| GGT >3 × elevated vs. normal | 0.727 | 1.0735 | 0.7207 to 1.5990 |
| ALP 1–3 × elevated vs. normal | 0.142 | 1.3301 | 0.9088 to 1.9467 |
| ALP >3 × elevated vs. normal | 0.129 | 2.0607 | 0.8090 to 5.2489 |
| Total bilirubin 1–3 × elevated vs. normal | 0.066 | 1.3087 | 0.9819 to 1.7443 |
| Total bilirubin >3 × elevated vs. normal | 0.881 | 1.0668 | 0.4577 to 2.4863 |
| Albumin 35–39 g/L vs. ≥40 g/L | 0.759 | 1.1403 | 0.4915 to 2.6459 |
| Albumin <35 g/L g/L vs. ≥40 g/L | 0.351 | 1.4787 | 0.6503 to 3.3624 |
| PT 80–89% vs. ≥100% | 0.388 | 1.0933 | 0.8929 to 1.3387 |
| PT < 80% vs. ≥100% | 0.056 | 1.3417 | 0.9920 to 1.8148 |
| Chronic liver disease | 0.246 | 0.5553 | 0.2057 to 1.4990 |
| Liver cirrhosis | 0.610 | 1.4051 | 0.3798 to 5.1976 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paštrovic, F.; Lucijanic, M.; Atic, A.; Stojic, J.; Barisic Jaman, M.; Tjesic Drinkovic, I.; Zelenika, M.; Milosevic, M.; Medic, B.; Loncar, J.; et al. Prevalence and Prognostic Impact of Deranged Liver Blood Tests in COVID-19: Experience from the Regional COVID-19 Center over the Cohort of 3812 Hospitalized Patients. J. Clin. Med. 2021, 10, 4222. https://doi.org/10.3390/jcm10184222
Paštrovic F, Lucijanic M, Atic A, Stojic J, Barisic Jaman M, Tjesic Drinkovic I, Zelenika M, Milosevic M, Medic B, Loncar J, et al. Prevalence and Prognostic Impact of Deranged Liver Blood Tests in COVID-19: Experience from the Regional COVID-19 Center over the Cohort of 3812 Hospitalized Patients. Journal of Clinical Medicine. 2021; 10(18):4222. https://doi.org/10.3390/jcm10184222
Chicago/Turabian StylePaštrovic, Frane, Marko Lucijanic, Armin Atic, Josip Stojic, Mislav Barisic Jaman, Ida Tjesic Drinkovic, Marko Zelenika, Marko Milosevic, Barbara Medic, Jelena Loncar, and et al. 2021. "Prevalence and Prognostic Impact of Deranged Liver Blood Tests in COVID-19: Experience from the Regional COVID-19 Center over the Cohort of 3812 Hospitalized Patients" Journal of Clinical Medicine 10, no. 18: 4222. https://doi.org/10.3390/jcm10184222
APA StylePaštrovic, F., Lucijanic, M., Atic, A., Stojic, J., Barisic Jaman, M., Tjesic Drinkovic, I., Zelenika, M., Milosevic, M., Medic, B., Loncar, J., Mijic, M., Filipec Kanizaj, T., Kralj, D., Lerotic, I., Virovic Jukic, L., Ljubicic, N., Luetic, K., Grgic, D., Majerovic, M., ... Grgurevic, I. (2021). Prevalence and Prognostic Impact of Deranged Liver Blood Tests in COVID-19: Experience from the Regional COVID-19 Center over the Cohort of 3812 Hospitalized Patients. Journal of Clinical Medicine, 10(18), 4222. https://doi.org/10.3390/jcm10184222