
Underdiagnosis of Major Depressive Episodes in Hemodialysis Patients: The Need for Screening and Patient Education

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Pilot Study—General Remarks
2.2. The Main Study
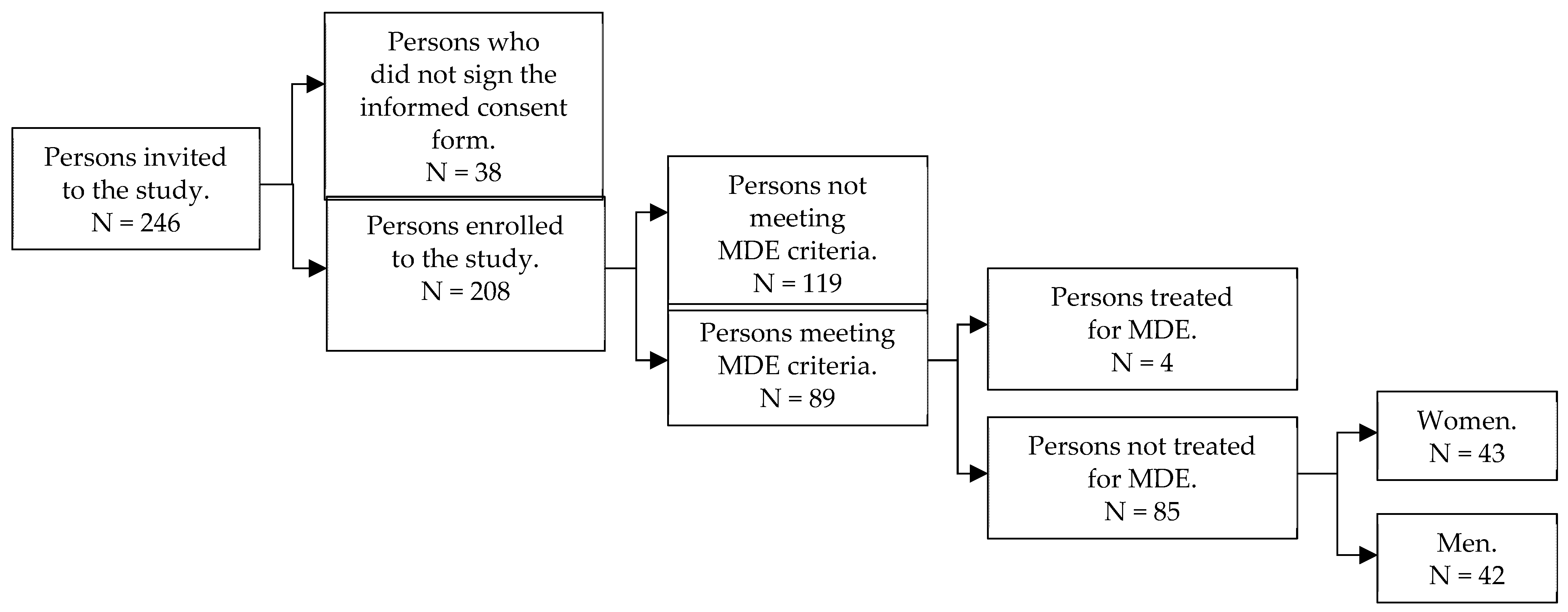
2.2.1. Study Design and Patient Characteristics
2.2.2. Methods
- The Mini-International Neuropsychiatric Interview (MINI) version 5.0.0 based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and International Classification of Diseases, Tenth Revision (ICD-10) criteria [6]. Originally, this instrument was developed as a short, structured interview to diagnose mental disorders based on the Diagnostic and Statistical Manual of Mental Disorders, Third Edition—Revised (DSM-III-R) and ICD-10 criteria. It can be used by clinicians after a short training, although nonprofessionals need a more intensive course. The psychometric properties of the original, English-language version of MINI were assessed as very high on the basis of Composite International Diagnostic Interview (CIDI) [6]. Considering the diagnosis of depression, sensitivity and specificity of the tool were 94% and 79%, respectively, and the kappa coefficient was 0.83.
- The Beck Depression Inventory, a tool used to assess the severity of depression. It is a self-completion questionnaire with a total score ranging from 0 to 84 points, with scores described as normal (≤9), indicating mild depression (10–18), indicating moderate depression (19–29), and indicating severe depression (≥30) [27,28]. The reliability assessment showed internal consistency—as measured by a Cronbach alpha coefficient of 0.86 for psychiatric patients and 0.81 for nonpsychiatric patients—and high agreement with clinical assessments on the Hamilton Depression Rating Scale (HDRS) [29]. BDI was used in the study for a purpose that is not the essence of this work, therefore, its results are not presented.
- The List of Explanations of Well-Being (LEWB) for persons with undiagnosed and untreated depression among patients with chronic kidney disease undergoing hemodialysis. The first version of this tool was developed for the pilot study described above. Its items were identified based on preliminary discussions with nephrologists and group interviews with dialysis patients, who were asked to determine the possible causes of their depressive symptoms and the potential obstacles to discussing these issues with medical staff. Due to the length and complexity of the original version, the newer version was modified for the current study and only statements that respondents most often referred to during the pilot study were retained. Patient responses can be classified in three categories, which means that depressive disorders may be caused by: (1) somatic diseases, (2) mental disorders, and (3) factors other than illness. The tool is a self-rating list. Patients are asked questions about their beliefs regarding the cause of their well-being. Respondents mark their answers on a 5-point Likert scale, and the predefined answers are as follows: I (1) strongly disagree, (2) would rather disagree, (3) have no opinion, (4) would rather agree, or (5) strongly agree. The questionnaire can be found in the supplementary files, see File S1.
- The Brief Measure to Assess Perception of Self-Influence on the Course of the Disease, version for hemodialysis patients [20]—a self-assessment scale consisting of 11 items to which the patient responds using a 5-point Likert scale. The reliability of the scale as measured by Cronbach alpha coefficient is 0.9, and accuracy as measured by Kendall tau coefficient is 0.6. The scale, although brief, is characterized by very high reliability and satisfactory accuracy. It assigns patients to one of the three groups according to their perception of self-influence on the course of kidney disease, i.e., (1) high (score ≤ 1.1), (2) moderate (1.1 < score ≤ 2.1), or (3) low (score > 2.1) perception of self-influence on the course of the disease.
- The Brief Method of Evaluating Coping with Disease, with versions for men and for women [30]. This is a tool used to determine the dominant style the person uses to cope with disease. The scale of 4 items tailored to the interests of both women and men corresponds with 4 different styles oriented on (1) a task, (2) searching for the best solution, (3) emotions, and (4) avoidance. The questionnaire is characterized by good reliability:
- (a)
- Cronbach alpha is 0.71 for females and 0.75 for males—for the style focused on a solution.
- (b)
- Cronbach alpha is 0.55 for females and 0.59 for males—for the style focused on searching for the best solution.
- (c)
- Cronbach alpha is 0.67 for females and 0.68 for males—for the style focused on emotions.
- (d)
- Cronbach alpha is 0.65 for females and 0.67 for males—for the style focused on avoidance.
- 6.
- The Coping Inventory for Stressful Situations (CISS) [31]—a tool used to diagnose styles of coping with stress. The results are presented on three scales: (1) focused on a task, (2) focused on emotions, and (3) focused on avoidance. It includes 2 forms of behavior: (a) engaging in surrogate activities and (b) seeking social contact. The questionnaire is characterized by high internal consistency of individual scales (Cronbach alpha coefficients within the range of 0.78–0.90) and satisfactory stability (correlation coefficients between tests at intervals of 2–3 weeks in the range of 0.73–0.80). The tool presents factor validity. It was also tested for theoretical and criterion validity (here by comparing the CISS results of various professional and clinical groups).
- 7.
- The Metacognitions Questionnaire (MCQ) [32]—a tool that aims to examine metacognitive beliefs. The scale consists of 65 statements that create five separate dimensions within which the respondent chooses answers on a 4-point Likert-type scale. The investigated dimensions are: (1) positive beliefs on worrying (e.g., “Worrying helps me avoid problems in the future”) (Cronbach alpha = 0.87); (2) negative beliefs about not controlling one’s own thoughts, and danger (e.g., “If I let my worrying thoughts get out of control, they will end up controlling me”) (Cronbach alpha = 0.89); (3) beliefs about cognitive certainty (e.g., “I have a poor memory”) (Cronbach alpha = 0.84); (4) general negative beliefs, including responsibility, punishment, and superstition (e.g., “It is bad to think certain thoughts”) (Cronbach alpha = 0.74); and (5) cognitive self-awareness (e.g., “I monitor my thoughts”) (Cronbach alpha = 0.72).
2.2.3. Statistical Analysis
3. Results
3.1. Well-Being
3.2. Perception of Self-Influence on the Course of Kidney Disease
- A mean score ≤1.1 was a threshold for a high perception of self-influence on disease progression.
- A mean score 1.1 < X ≤ 2.1 marked a moderate perception of self-influence on disease progression.
- A mean score >2.1 indicated a low perception of self-influence on disease progression.
3.3. Styles of Coping with the Disease and Stressful Situations
3.4. Metacognitive Beliefs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Weissman, M.M.; Bland, R.; Joyce, P.R.; Newman, S.; Wells, J.E.; Wittchen, H.U. Sex differences in rates of depression: Cross-national perspectives. J. Affect. Disord. 1993, 29, 77–84. [Google Scholar] [CrossRef]
- Palmer, S.; Vecchio, M.; Craig, J.; Tonelli, M.; Johnson, D.W.; Nicolucci, A.; Pellegrini, F.; Saglimbene, V.; Logroscino, G.; Fishbane, S.; et al. Prevalence of depression in chronic kidney disease: Systematic review and meta-analysis of observational studies. Kidney Int. 2013, 84, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Kokoszka, A.; Leszczyńska, K.; Radzio, R.; Daniewska, D.; Łukasiewicz, A.; Orzechowski, W.; Piskorz, A.; Gellert, R. Prevalence of depressive and anxiety disorders in dialysis patients with chronic kidney disease. Arch. Psychiatry Psychother. 2016, 1, 8–13. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Masiak, M.; Przychoda, J.M.I.N.I. Mini International Neuropsychiatric Interview; Polish Version 5.0.0; Katedra i Klinika Psychiatrii Akademii Medycznej: Lublin, Poland, 1998. [Google Scholar]
- Klarić, M.; Letica, I.; Petrov, B.; Tomić, M.; Klarić, B.; Letica, L.; Francisković, T. Depression and anxiety in patients on chronic hemodialysis in University Clinical Hospital Mostar. Coll. Antropol. 2009, 33, 153–158. [Google Scholar]
- Saglimbene, V.; Palmer, S.; Scardapane, M.; Craig, J.C.; Ruospo, M.; Natale, P.; Gargano, L.; Leal, M.; Bednarek-Skublewska, A.; Dulawa, J.; et al. Depression and all-cause and cardiovascular mortality in patients on hemodialysis: A multinational cohort study. Nephrol. Dial. Transplant. 2017, 32, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Hedayati, S.S.; Minhajuddin, A.T.; Toto, R.D.; Morris, D.W.; Rush, A. Prevalence of major depressive episode in CKD. Am. J. Kidney Dis. 2009, 54, 424–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diefenthaeler, E.C.; Wagner, M.B.; Poli-De-Figueiredo, C.E.; Zimmermann, P.R.; Saitovitch, D. Is depression a risk factor for mortality in chronic hemodialysis patients? Rev. Bras. Psiquiatr. 2008, 30, 99–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilikiewicz, A.; Landowski, J.; Radziwiłłowicz, P. Psychiatria Repetytorium, 2nd ed.; PZWL: Warsaw, Poland, 2008. [Google Scholar]
- Farrokhi, F. Depression among dialysis patients: Barriers to good care. Iran. J. Kidney Dis. 2012, 6, 403–406. [Google Scholar]
- Johnson, S.; Dwyer, A. Patient perceived barriers to treatment of depression and anxiety in hemodialysis patients. Clin. Nephrol. 2008, 69, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Kokoszka, A.; Jodko-Modlińska, A.; Obrębski, M.; Ostasz-Ważny, J.; Radzio, R. Psychodiabetic Kit and its application in clinical practice and research. In Type 2 Diabetes; Masuo, K., Ed.; Intech: New York, NY, USA, 2013; pp. 507–531. [Google Scholar]
- Park, C.L.; Folkman, S.; Bostrom, A. Appraisals of controllability and coping in caregivers and HIV+ men: Testing the goodness-of-fit hypothesis. J. Consult. Clin. Psychol. 2001, 69, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Dragan, M. Terapia metapoznawcza (English: Metacognitive therapy). In Psychoterapia. Szkoły i Metody (English: Psychotherapy. Schools and Methods.); Grzesiuk, W.L., Szuszek, H., Eds.; ENETEIA Wydawnictwo Psychologii i Kultury: Warsaw, Poland, 2011; pp. 211–225. [Google Scholar]
- Dragan, M.; Dragan, W. Psychometric properties of the Polish version of the Metacognitions Questionnaire-30. Psychiatr. Pol. 2011, 45, 545–553. [Google Scholar]
- Gawęda, L.; Buciński, P.; Staniszewski, K.; Słodki, Z.; Sym, A.; Kokoszka, A. Związki wglądu w chorobę, poczucia wpływu na jej przebieg, stylów radzenia sobie z chorobą z objawami psychopatologicznymi w schizofrenii (English: Relationships of insight into the disease, the sense of influence on the course of the disease, and disease coping styles, with psychopathological symptoms in schizophrenia). Psychiatria 2008, 5, 124–133. [Google Scholar]
- Kokoszka, A.; Telichowska-Leśna, A.; Radzio, R. Krótka skala poczucia wpływu na przebieg choroby: Wersja dla schizofrenii (English: The brief scale of the sense of influence on the course of the disease: Version for schizophrenia). Psychiatr. Pol. 2008, 42, 503–513. [Google Scholar]
- Endler, N.S.; Parker, J.D. Multidimensional assessment of coping: A critical evaluation. J. Pers. Soc. Psychol. 1990, 58, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Endler, N.S.; Parker, J.D.A. Assessment of multidimensional coping: Task, emotions, and avoidance strategies. Psychol. Assess. 1994, 6, 50–60. [Google Scholar] [CrossRef]
- Kokoszka, A.; Santorski, J. Psychodiabetologia dla Lekarzy: Postępowanie Psychoterapeutyczne w Cukrzycy (English: Psychodiabetology for Doctors: Psychotherapeutic Treatment in Diabetes); Marketing and Media: Warsaw, Poland, 2003. [Google Scholar]
- Wells, A.; Matthews, G. Modelling cognition in emotional disorder: The S-REF model. Behav. Res. Ther. 1996, 34, 881–888. [Google Scholar] [CrossRef]
- Wells, A.; Papageorgiou, C. Relationships between worry, obsessive-compulsive symptoms, and meta-cognitive beliefs. Behav. Res. Ther. 1998, 36, 899–913. [Google Scholar] [CrossRef]
- Wells, A.; Carter, K. Preliminary tests of a cognitive model of generalized anxiety disorder. Behav. Res. Ther. 1999, 37, 585–594. [Google Scholar] [CrossRef]
- Papageorgiou, C.; Wells, A. Positive beliefs about depressive rumination: Development and preliminary validation of a self-report scale. Behav. Ther. 2001, 32, 13–26. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Kokoszka, A.; Radzio, R.; Kot, W. Krótka metoda oceny radzenia sobie z chorobą: Wersje dla mężczyzn i kobiet (English: The brief evaluation assessment method of coping with the disease: Versions for men and women). Diabetol. Klin. 2008, 9, 1–11. [Google Scholar]
- Strelau, J.; Jaworowska, A. Kwestionariusz Radzenia Sobie w Sytuacjach Stresowych CISS: Podręcznik do Polskiej Normalizacji (English: CISS—Coping with Stress Questionnaire. A Manual for Polish Standardization); Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2005. [Google Scholar]
- Cartwright-Hatton, S.; Wells, A. Beliefs about worry and intrusions: The meta-cognitions questionnaire and its correlates. J. Anxiety Disord. 1997, 11, 279–296. [Google Scholar] [CrossRef]
- Cypryańska, M.; Bedyńska, S. Porównanie dwóch grup: Testy t-Studenta i ich nieparametryczne odpowiedniki. (English: Comparison of two groups: Student’s t tests and their non-parametric counterparts.). In Statystyczny Drogowskaz. Praktyczny Poradnik Analizy Danych w Naukach Społecznych na Przykładach z Psychologii (English: Statistical Signpost. A Practical Guide to Data Analysis in Social Sciences Based on Examples from Psychology), 1st ed.; Bedyńska, S., Brzezicka, A., Eds.; Academica Wydawnictwo SWPS: Warsaw, Poland, 2007; pp. 184–207. [Google Scholar]
- Krejtz, K.; Krejtz, I. Dwuczynnikowa analiza wariancji w schemacie międzygrupowym. (English: Bivariate analysis of variance in a between-groups design.). In Statystyczny Drogowskaz. Praktyczny Poradnik Analizy Danych w Naukach Społecznych na Przykładach z Psychologii (English: Statistical Signpost. A Practical Guide to Data Analysis in Social Sciences Based on Examples from Psychology), 1st ed.; Bedyńska, S., Brzezicka, A., Eds.; Academica Wydawnictwo SWPS: Warsaw, Poland, 2007; pp. 231–252. [Google Scholar]
- Rycielski, P.; Brzezicka, A. Wnioskowanie statystyczne na danych jakościowych: Testy oparte na rozkładzie chi-kwadrat. (English: Statistical inference on qualitative data: Tests based on the chi-square distribution). In Statystyczny Drogowskaz. Praktyczny Poradnik Analizy Danych w Naukach Społecznych na Przykładach z Psychologii (English: Statistical Signpost. A Practical Guide to Data Analysis in Social Sciences Based on Examples from Psychology), 1st ed.; Bedyńska, S., Brzezicka, A., Eds.; Academica Wydawnictwo SWPS: Warsaw, Poland, 2007; pp. 162–183. [Google Scholar]
- Ścibor-Rylski, M. Miary związku pomiędzy zmiennymi—Współczynniki korelacji. (English: Measures of the relationship between variables—correlation coefficients). In Statystyczny Drogowskaz. Praktyczny Poradnik Analizy Danych w Naukach Społecznych na Przykładach z Psychologii (English: Statistical Signpost. A Practical Guide to Data Analysis in Social Sciences Based on Examples from Psychology), 1st ed.; Bedynska, S., Brzezicka, A., Eds.; Academica Wydawnictwo SWPS: Warsaw, Poland, 2007; pp. 94–115. [Google Scholar]
- Górniak, J. Zastosowanie analizy korespondencji w badaniach społecznych i marketingowych (English: Application of correspondence analysis in social and marketing Research). ASK 2000, 9, 115–134. [Google Scholar]
- Orzechowski, W.M.; Fiderkiewicz, B. Krótka metoda oceny poczucia wpływu pacjenta na przebieg choroby—wersja dla hemodializowanych (English: The brief evaluation assessment method of patient’s sense of influence on the course of the disease—version for hemodialysis). Prz. Lek. 2016, 73, 20–24. [Google Scholar]
- Arroll, B.; Khin, N.; Kerse, N. Screening for depression in primary care with two verbally asked questions: Cross sectional study. BMJ 2003, 327, 1144–1146. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- PHQ-9 Screener. Available online: https://www.phqscreeners.com/select-screener (accessed on 27 August 2021).
- Cichon, E.; Kiejna, A.; Kokoszka, A.; Gondek, T.M.; Radzio, R.; Jastrzębski, A.; Andrzejewska, B.E.; Alosaimi, F.D.; Lloyd, C.E.; Sartorius, N. People with diabetes need a lower cut-off than others for depression screening with PHQ-9. PLoS ONE 2020, 15, e0240209. [Google Scholar] [CrossRef]
- WHO—Regional Office for Europe. Wellbeing Measures in Primary Health Care/The Depcare Project; WHO Regional Office for Europe: Copenhagen, Denmark; Geneva, Switzerland, 1998; Available online: https://www.euro.who.int/__data/assets/pdf_file/0016/130750/E60246.pdf (accessed on 27 August 2021).
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Cichoń, E.; Kiejna, A.; Kokoszka, A.; Gondek, T.; Rajba, B.; Lloyd, C.E.; Sartorius, N. Validation of the Polish version of WHO-5 as a screening instrument for depression in adults with diabetes. Diabetes Res. Clin. Pract. 2019, 159, 107970. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, Y.; Zerbinati, L.; Martino, E.; Piazza, G.; Massarenti, S.; Storari, A.; Grassi, L. Psychosocial dimensions in hemodialysis patients on kidney transplant waiting list: Preliminary data. Transplantology 2020, 1, 12. [Google Scholar] [CrossRef]
- Porcelli, P.; Rafanelli, C. Criteria for psychosomatic research (DCPR) in the medical setting. Curr. Psychiatry Rep. 2010, 12, 246–254. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Values | |
|---|---|---|
| Age | 68.26 1 (14.19) 2 years old | |
| Dialysis duration | 70.63 1 (75.26) 2 months | |
| Total | N (%) | |
| Attitude to treatment of depression (N = 89) | Treated | 4 (4.5%) |
| Untreated | 85 (95.5%) | |
| Patient’s sex | Female | 43 (50.6%) |
| Male | 42 (49.4%) | |
| Patient’s education level | Primary school | 13 (19.7%) |
| Vocational | 13 (19.7%) | |
| Secondary school | 25 (37.9%) | |
| High | 15 (22.7%) | |
| Time of hemodialysis | Morning | 43 (50.6%) |
| Afternoon | 22 (25.9%) | |
| Evening | 20 (23.5%) | |
| Hemodialysis center | Dpt. of Nephrology, Dialysis, and Int. Medicine, Medical Univ. of Warsaw, Central Teaching Hospital | 24 (28.2%) |
| Dpt. of Int. Medicine, Nephrology and Transplantology, Central Clinical Hospital of the Ministry of Interior and Administration | 29 (34.1%) | |
| Dpt. of Nephrology and Int. Medicine, Centre for Postgraduate Medical Education, Bielanski Hospital | 32 (37.6%) | |
| Risk of suicidal behavior | Low | 75 (88.2%) |
| Moderate | 10 (11.8%) | |
| Current diagnosed comorbidities | Hypomanic episode | 1 (1.2%) |
| Panic disorder | 5 (5.9%) | |
| Panic disorder with agoraphobia | 7 (8.2%) | |
| Agoraphobia | 5 (5.9%) | |
| Social phobia | 6 (7.1%) | |
| Obsessive-compulsive disorder | 3 (3.5%) | |
| Acute stress disorder | 1 (1.2%) | |
| My Well-Being Is: | Agree 1 | Disagree 2 | ||
|---|---|---|---|---|
| N | % | N | % | |
| A symptom of kidney failure | 36 | 42.3 | 43 | 50.6 |
| Affected by hemodialysis | 42 | 49.4 | 39 | 45.9 |
| Related to my other diseases and/or conditions | 47 | 55.3 | 37 | 43.5 |
| Related to factors other than illness, e.g., family problems, unemployment, etc. | 52 | 61.2 | 31 | 36.5 |
| Inherently related to a disease like mine (kidney disease) | 64 | 75.3 | 18 | 21.2 |
| A symptom of depression | 60 | 70.6 | 16 | 18.8 |
| Not related to my current health state | 8 | 7.2 | 76 | 89.4 |
| Low | Moderate | High |
|---|---|---|
| N = 55 | N = 19 | N = 11 |
| 64.7% | 22.4% | 12.9% |
| Task-Oriented Coping | Best Solution-Oriented Coping | Emotion-Oriented Coping | Avoidance-Oriented Coping | ||||
|---|---|---|---|---|---|---|---|
| N = 13 | N = 9 | N = 36 | N = 27 | ||||
| 15.3% | 10.6% | 42.4% | 31.8% | ||||
| F 1 | M 2 | F | M | F | M | F | M |
| N = 4 | N = 9 | N = 6 | N = 3 | N = 24 | N = 12 | N = 9 | N = 18 |
| 4.7% | 10.6% | 7.1% | 3.5% | 28.2% | 14.1% | 10.6% | 21.2% |
| Task-Oriented | Emotion-Oriented | Avoidance-Oriented | Two Styles More Apparent than the Third Style |
|---|---|---|---|
| N = 17 | N = 48 | N = 3 | N = 14 |
| 20.7% | 58.5% | 3.7% | 17.1% |
| Beliefs | M 1 | P 2 | SD 3 | Median |
|---|---|---|---|---|
| Positive worry beliefs | 26.95 | 35% | 10.23 | 23.00 |
| Negative beliefs about not controlling one’s own thoughts and danger | 41.54 | 65% | 12.97 | 43.00 |
| Beliefs about cognitive confidence | 19.25 | 48% | 8.44 | 17.00 |
| General negative beliefs about thoughts, including a sense of responsibility, superstition, and expectation of punishment | 23.51 | 45% | 5.20 | 25.00 |
| Beliefs about cognitive self-awareness | 15.84 | 57% | 8.09 | 13.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orzechowski, W.; Buczek, W.; Szczerba, J.E.; Gellert, R.; Rydzewski, A.; Fiderkiewicz, B.; Żebrowski, P.; Daniewska, D.; Kokoszka, A. Underdiagnosis of Major Depressive Episodes in Hemodialysis Patients: The Need for Screening and Patient Education. J. Clin. Med. 2021, 10, 4109. https://doi.org/10.3390/jcm10184109
Orzechowski W, Buczek W, Szczerba JE, Gellert R, Rydzewski A, Fiderkiewicz B, Żebrowski P, Daniewska D, Kokoszka A. Underdiagnosis of Major Depressive Episodes in Hemodialysis Patients: The Need for Screening and Patient Education. Journal of Clinical Medicine. 2021; 10(18):4109. https://doi.org/10.3390/jcm10184109
Chicago/Turabian StyleOrzechowski, Wojciech, Wiktor Buczek, Joanna Emma Szczerba, Ryszard Gellert, Andrzej Rydzewski, Bartosz Fiderkiewicz, Paweł Żebrowski, Dorota Daniewska, and Andrzej Kokoszka. 2021. "Underdiagnosis of Major Depressive Episodes in Hemodialysis Patients: The Need for Screening and Patient Education" Journal of Clinical Medicine 10, no. 18: 4109. https://doi.org/10.3390/jcm10184109
APA StyleOrzechowski, W., Buczek, W., Szczerba, J. E., Gellert, R., Rydzewski, A., Fiderkiewicz, B., Żebrowski, P., Daniewska, D., & Kokoszka, A. (2021). Underdiagnosis of Major Depressive Episodes in Hemodialysis Patients: The Need for Screening and Patient Education. Journal of Clinical Medicine, 10(18), 4109. https://doi.org/10.3390/jcm10184109