
Check the Need–Prevalence and Outcome after Transvenous Cardiac Implantable Electric Device Extraction without Reimplantation


 , , , ,
, , , ,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. TLE and Post-Procedural Management
2.2. Decision to Reimplant
2.3. Follow-Up
2.4. Data Collection
2.5. Endpoints
2.6. Statistics
3. Results
3.1. Baseline Characteristics and TLE Procedure
3.2. Decision Not to Reimplant
3.3. Factors Favouring No Reimplantation
3.4. Follow-Up
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greenspon, A.J.; Patel, J.D.; Lau, E.; Ochoa, J.A.; Frisch, D.R.; Ho, R.T.; Pavri, B.B.; Kurtz, S.M. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. J. Am. Coll. Cardiol. 2011, 58, 1001–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.L.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.M.; Clancy, J.; Deharo, J.C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017, 14, e503–e551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the management of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Bontempi, L.; Curnis, A.; Della Bella, P.; Cerini, M.; Radinovic, A.; Inama, L.; Melillo, F.; Salghetti, F.; Marzi, A.; Gargaro, A.; et al. The MB score: A new risk stratification index to predict the need for advanced tools in lead extraction procedures. EP Eur. 2020, 22, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.; Deharo, J.C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, M.; Jones, T. How does an implantable cardioverter defibrillator (ICD) affect the lives of patients and their families? Int. J. Nurs. Pract. 2002, 8, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Al-Hijji, M.A.; Killu, A.M.; Yousefian, O.; Hodge, D.O.; Park, J.Y.; Hebsur, S.; El Sabbagh, A.; Pretorius, V.G.; Ackerman, M.J.; Friedman, P.A.; et al. Outcomes of lead extraction without subsequent device reimplantation. EP Eur. 2017, 19, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Doring, M.; Hienzsch, L.; Ebert, M.; Lucas, J.; Dagres, N.; Kuhl, M.; Hindricks, G.; Knopp, H.; Richter, S. Extraction of infected cardiac implantable electronic devices and the need for subsequent re-implantation. Int. J. Cardiol. 2020, 309, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Boyle, T.A.; Uslan, D.Z.; Prutkin, J.M.; Greenspon, A.J.; Baddour, L.M.; Danik, S.B.; Tolosana, J.M.; Le, K.; Miro, J.M.; Peacock, J.; et al. Reimplantation and repeat infection after cardiac-implantable electronic device infections: Experience from the MEDIC (multicenter electrophysiologic device infection cohort) database. Circ. Arrhythm. Electrophysiol. 2017, 10, e004822. [Google Scholar] [CrossRef] [PubMed]
- Kypta, A.; Blessberger, H.; Kammler, J.; Lambert, T.; Lichtenauer, M.; Brandstaetter, W.; Gabriel, M.; Steinwender, C. Leadless cardiac pacemaker implantation after lead extraction in patients with severe device infection. J. Cardiovasc. Electrophysiol. 2016, 27, 1067–1071. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, H.; Richardson, T.D.; Montgomery, J.A.; Crossley, G.H.; Ellis, C.R. Comparison of leadless pacing and temporary externalized pacing following cardiac implanted device extraction. J. Innov. Card. Rhythm. Manag. 2019, 10, 3930–3936. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Population (n = 223) | Reimplantation (n = 190) | No Reimplantation (n = 33) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 70 (58–76) | 70 (58–76) | 73 (57–78) | 0.703 |
| Female gender | 22.0% (n = 49) | 23.2% (n = 44) | 15.2% (n = 5) | 0.369 |
| Comorbidities | ||||
| Hypertension | 53.4% (n = 119) | 52.6% (n = 100) | 57.6% (n = 19) | 0.706 |
| Diabetes mellitus | 22.0% (n = 49) | 20.5% (n = 39) | 30.3% (n = 10) | 0.254 |
| eGFR | 69.7 ± 27.7 | 68.7 ± 27.2 | 75.3 ± 30.0 | 0.245 |
| eGFR < 60 mL/min | 37.7% (n = 84) | 38.4% (n = 73) | 33.3% (n = 11) | 0.698 |
| LVEF | 0.043 | |||
| 35–50% | 28.7% (n = 64) | 29.0% (n = 55) | 27.3% (n = 9) | |
| <35% | 34.5% (n = 77) | 37.4% (n = 71) | 18.2% (n = 6) | |
| Atrial fibrillation | 0.613 | |||
| paroxysmal | 22.9% (n = 51) | 22.1% (n = 42) | 27.3% (n = 9) | |
| permanent | 11.7% (n = 26) | 11.1% (n = 21) | 1.52% (n = 5) | |
| Anticoagulation | 31.4% (n = 70) | 32.1% (n = 61) | 27.3% (n = 9) | 0.686 |
| Antiplatelets | 33.2% (n = 74) | 34.7% (n = 66) | 24.2% (n = 8) | 0.317 |
| Device details | ||||
| Device type | 0.590 | |||
| CRT-D | 40.4% (n = 90) | 41.6% (n = 79) | 33.3% (n = 11) | |
| PM | 31.4% (n = 70) | 31.6% (n = 60) | 30.3% (n = 10) | |
| ICD | 26.9% (n = 60) | 25.3% (n = 48) | 36.4% (n = 12) | |
| CRT-P | 1.4% (n = 3) | 1.6% (n = 3) | 0% (n = 0) | |
| Indication for implant | 0.004 | |||
| Non-ischemic CMP | 38.1% (n = 85) | 37.9% (n = 72) | 39.4% (n = 13) | |
| Ischemic CMP | 29.6% (n = 66) | 32.1% (n = 61) | 15.2% (n = 5) | |
| AV block | 12.6% (n = 28) | 14.2% (n = 27) | 3.0% (n = 1) | |
| Sick sinus syndrome | 11.2% (n = 25) | 8.4% (n = 16) | 27.3% (n = 9) | |
| Inherited cardiac disease | 5.4% (n = 12) | 4.7% (n = 9) | 9.1% (n = 3) | |
| other | 3.1% (n = 7) | 2.6% (n = 5) | 6.1% (n = 2) | |
| Implant for secondary prevention † | 15.5% (n= 16) | 17.2% (n = 15) | 6.3% (n = 1) | 0.456 |
| Indication for explant | 0.003 | |||
| infection | 55.6% (n = 124) | 51.1% (n = 97) | 81.8% (n = 27) | |
| malfunction | 35.9% (n = 80) | 39.5% (n = 75) | 15.2% (n = 5) | |
| system upgrade | 6.7% (n = 15) | 7.9% (n = 15) | 0% (n = 0) | |
| other causes | 1.8% (n = 4) | 1.6% (n = 3) | 3.0% (n = 1) | |
| Number of leads | 2 (2–3) | 2 (2–3) | 2 (2–3) | 0.943 |
| Number of leads to be removed | 2 (1–3) | 2 (1–3) | 2 (2–3) | 0.033 |
| Age of device (months) | 54 (21–85) | 50 (21–84) | 68 (20–92) | 0.633 |
| Age of leads (months) | 68 (31–100) | 62 (30–99) | 78 (45–104) | 0.432 |
| Parameter | p Value (Univariable) | OR (95% CI) | p Value (Multivariable) |
|---|---|---|---|
| Details regarding CIED indication | |||
| Absence of ischemic CMP | 0.062 | 3.1 (1.1–10.4) | 0.047 * |
| Absence of AV block | 0.089 | 14.6 (2.5–281.7) | 0.014 * |
| Sick sinus syndrome | 0.004 * | 1.6 (0.5–5.2) | 0.425 |
| Clinical details | |||
| LVEF (per 10% increase) | 0.019 * | 1.5 (1.1–2.3) | 0.024 * |
| Details regarding CIED explant | |||
| Absence of lead malfunction | 0.006 * | 2.2 (0.3–14.4) | 0.416 |
| Number of explanted leads, per lead | 0.033 * | 1.3 (0.8–2.2) | 0.243 |
| CIED infection | 0.001 * | 2.3 (0.4–18.5) | 0.373 |
| Reimplantation (n = 190) | No Reimplantation (n = 33) | p Value | |
|---|---|---|---|
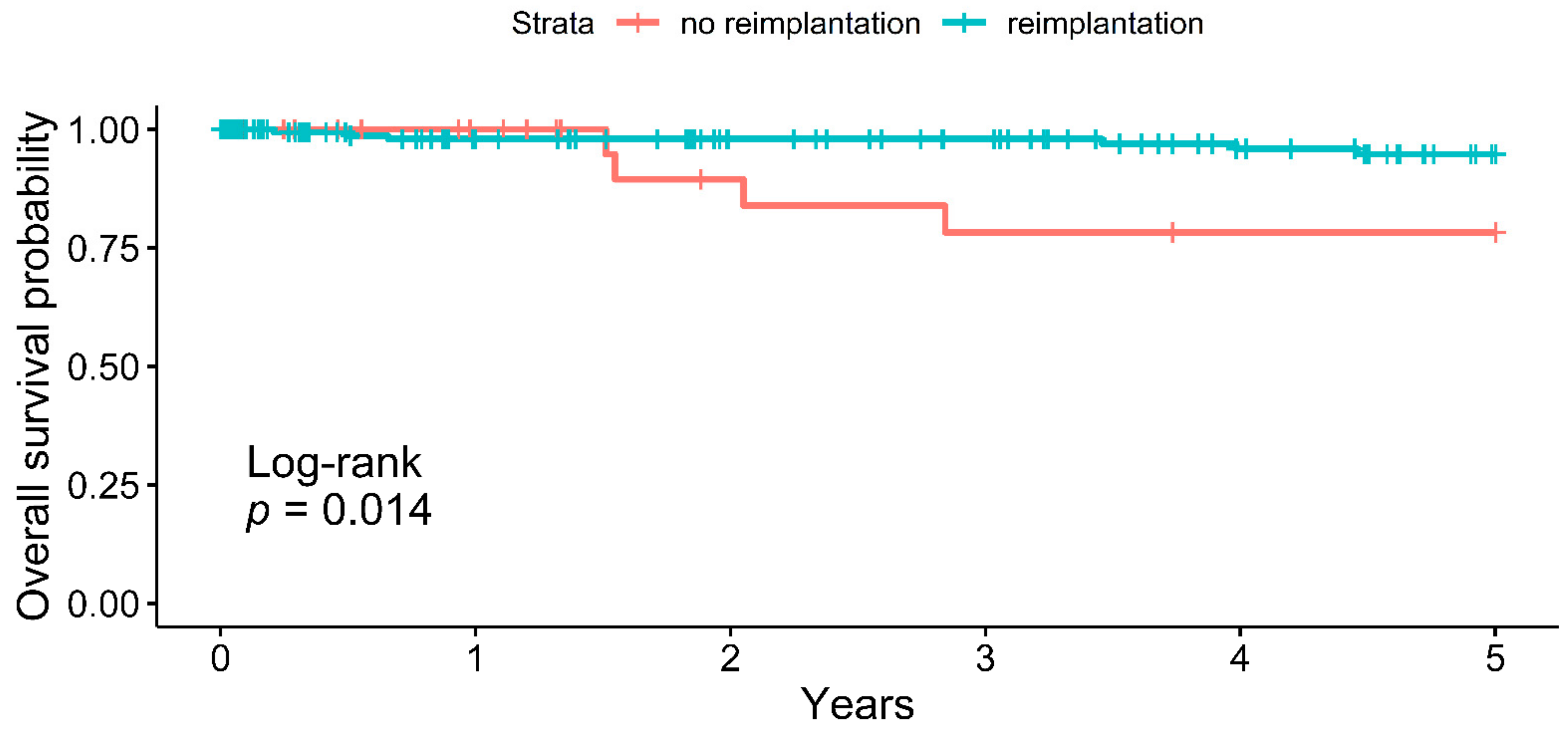
| Follow-up duration, months | 44 (7–76) | 23 (11–80) | 0.883 |
| 1-year cumulative survival (NaR) | 98.0% (131) | 100.0% (23) | 0.500 |
| 5-year cumulative survival (NaR) | 94.7% (73) | 78.3% (13) | 0.014 * |
| late reimplantation or device revision | 11.1% (n = 21) | 12.1% (n = 4) | 0.771 |
| “Reimplantation”-specific events | N/A | N/A | |
| any device-related hospitalisation | 11.1% (n = 21) | ||
| lead failure/dislocation | 7.9% (n = 15) | ||
| pocket revision | 2.1% (n = 4) | ||
| device recall | 1.1% (n = 2) | ||
| device infection | 0.5% (n = 1) | ||
| repeat extraction procedure | 3.2% (n = 6) | ||
| “No reimplantation”-specific events Reimplantation | N/A | 12.1% (n = 4) | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Angelo, G.; Zweiker, D.; Fierro, N.; Marzi, A.; Paglino, G.; Gulletta, S.; Matta, M.; Melillo, F.; Bisceglia, C.; Limite, L.R.; et al. Check the Need–Prevalence and Outcome after Transvenous Cardiac Implantable Electric Device Extraction without Reimplantation. J. Clin. Med. 2021, 10, 4043. https://doi.org/10.3390/jcm10184043
D’Angelo G, Zweiker D, Fierro N, Marzi A, Paglino G, Gulletta S, Matta M, Melillo F, Bisceglia C, Limite LR, et al. Check the Need–Prevalence and Outcome after Transvenous Cardiac Implantable Electric Device Extraction without Reimplantation. Journal of Clinical Medicine. 2021; 10(18):4043. https://doi.org/10.3390/jcm10184043
Chicago/Turabian StyleD’Angelo, Giuseppe, David Zweiker, Nicolai Fierro, Alessandra Marzi, Gabriele Paglino, Simone Gulletta, Mario Matta, Francesco Melillo, Caterina Bisceglia, Luca Rosario Limite, and et al. 2021. "Check the Need–Prevalence and Outcome after Transvenous Cardiac Implantable Electric Device Extraction without Reimplantation" Journal of Clinical Medicine 10, no. 18: 4043. https://doi.org/10.3390/jcm10184043
APA StyleD’Angelo, G., Zweiker, D., Fierro, N., Marzi, A., Paglino, G., Gulletta, S., Matta, M., Melillo, F., Bisceglia, C., Limite, L. R., Cireddu, M., Vergara, P., Bosica, F., Falasconi, G., Pannone, L., Brugliera, L., Oloriz, T., Sala, S., Radinovic, A., ... Mazzone, P. (2021). Check the Need–Prevalence and Outcome after Transvenous Cardiac Implantable Electric Device Extraction without Reimplantation. Journal of Clinical Medicine, 10(18), 4043. https://doi.org/10.3390/jcm10184043