
The Surgical Management of Brain Metastases in Non-Small Cell Lung Cancer (NSCLC): Identification of the Early Laboratory and Clinical Determinants of Survival

 ,
,  , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistics
3. Results
3.1. Patient Characteristics
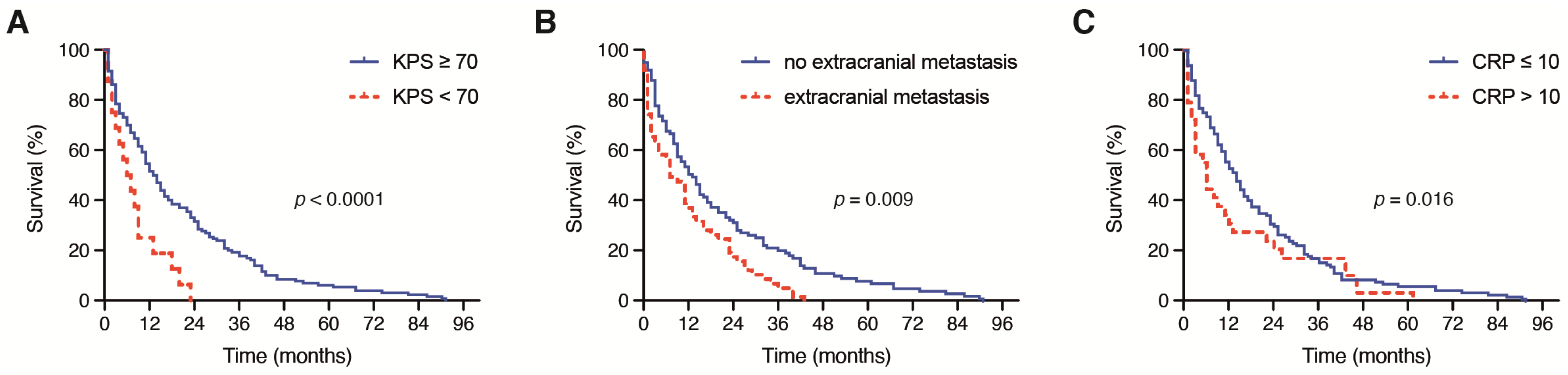
3.2. Influence of Clinical Admission Status and Tumor Stage
3.3. Influence of Preoperative Laboratory Values
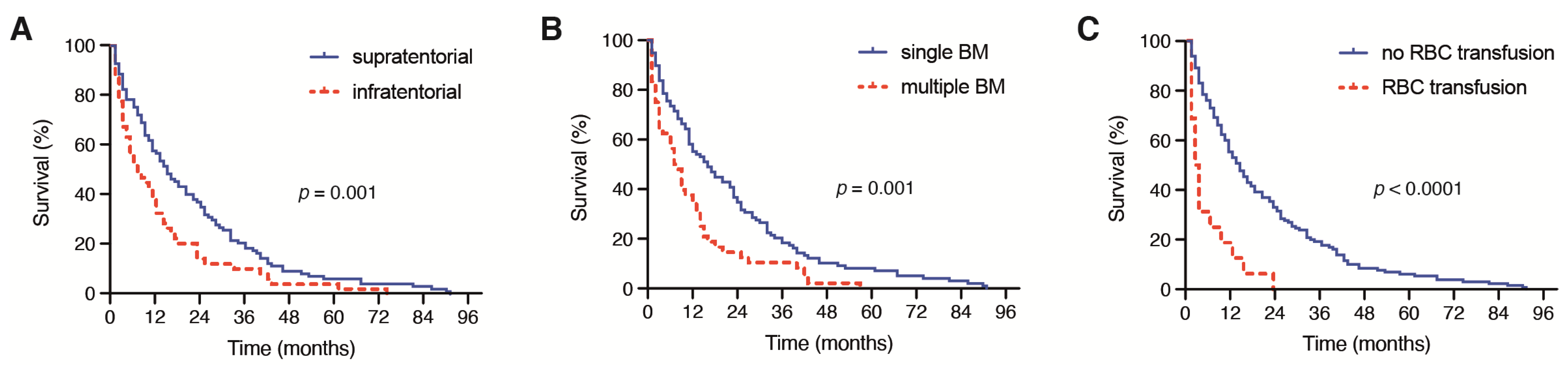
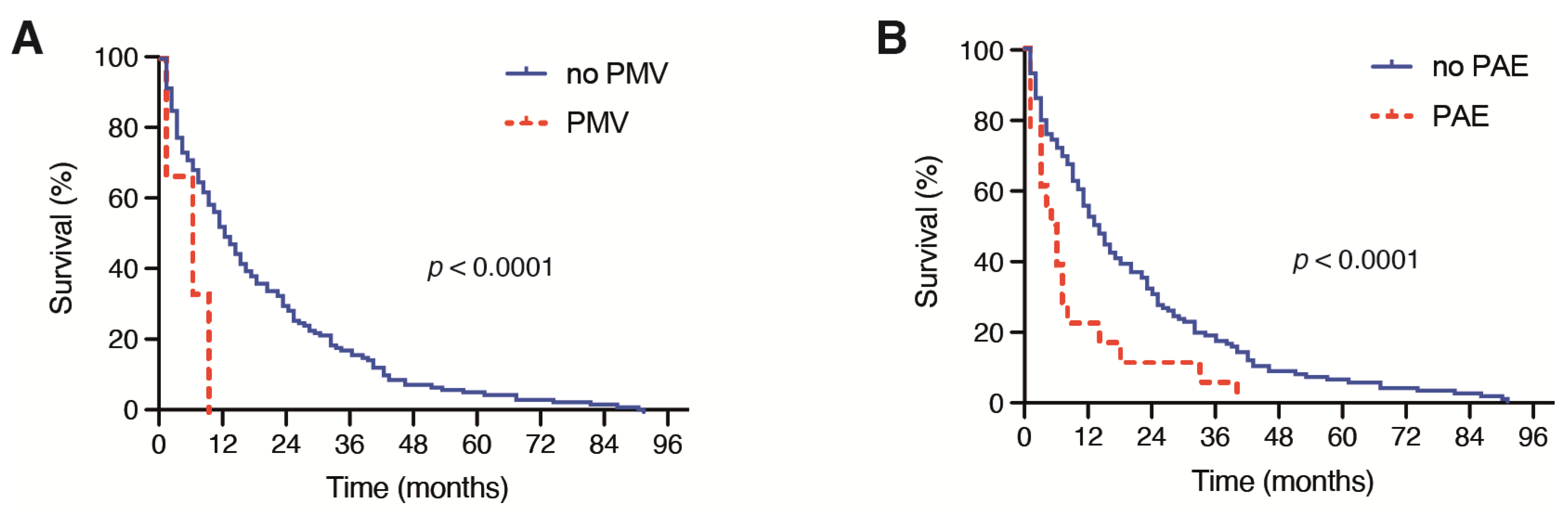
3.4. Influence of Location, Tumor Burden and Perioperative Management
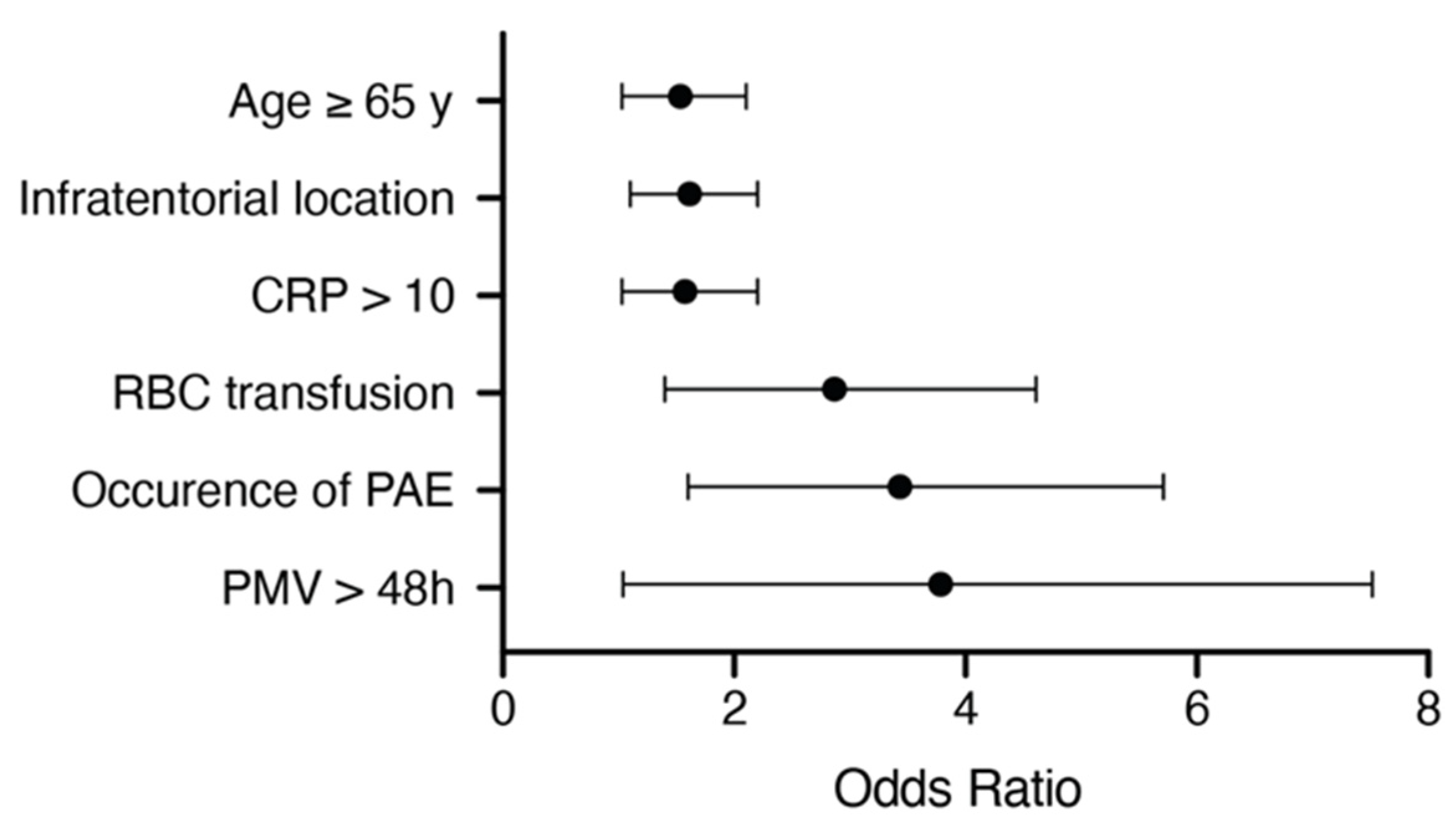
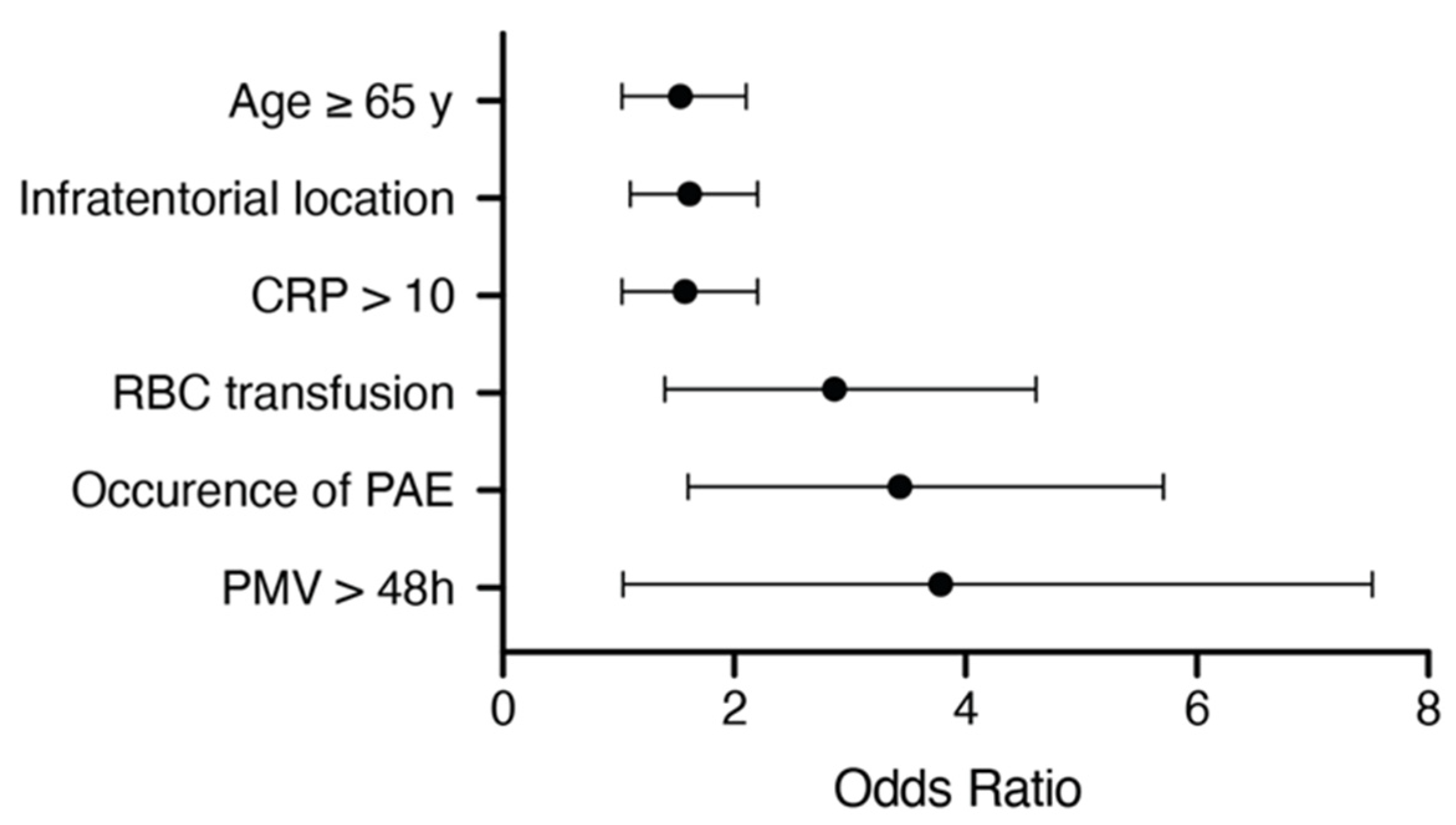
3.5. Multivariate Analysis
4. Discussion
4.1. Clinical Admission Status
4.2. Tumor Burden and Location
4.3. C-Reactive Protein
4.4. Postoperative Course
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Achrol, A.S.; Rennert, R.C.; Anders, C.; Soffietti, R.; Ahluwalia, M.S.; Nayak, L.; Peters, S.; Arvold, N.D.; Harsh, G.R.; Steeg, P.S.; et al. Brain Metastases. Nat. Rev. Dis. Primers 2019, 1, 5. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Wright, C.H.; Barnholtz-Sloan, J.S. Brain Metastases: Epidemiology. Handb. Clin. Neurol. 2018, 149, 27–42. [Google Scholar]
- Zhang, X.; Zhang, W.; Cao, W.D.; Cheng, G.; Liu, B.; Cheng, J. A Review of Current Management of Brain Metastases. Ann. Surg. Oncol. 2012, 3, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Fenske, D.C.; Price, G.L.; Hess, L.M.; John, W.J.; Kim, E.S. Systematic Review of Brain Metastases in Patients with Non-Small-Cell Lung Cancer in the United States, European Union, and Japan. Clin. Lung Cancer 2017, 6, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Stoltzfus, K.C.; Chen, H.; Louie, A.V.; Lehrer, E.J.; Horn, S.R.; Palmer, J.D.; Trifiletti, D.M.; Brown, P.D.; Zaorsky, N.G. Epidemiology of Synchronous Brain Metastases. Neurooncol. Adv. 2020, 1, vdaa041. [Google Scholar] [CrossRef]
- Naito, H.; Sasaki, M.; Kondo, K.; Gotoda, A.; Kawamura, K.; Asama, T.; Osawa, H.; Ohara, K.; Takamatsu, H.; Fukuoka, S.; et al. Radical Treatment of Brain Metastasis of Colorectal-Cancer. Oncol. Rep. 1994, 6, 1203–1205. [Google Scholar] [CrossRef]
- Davey, P. Brain Metastases: Treatment Options to Improve Outcomes. CNS Drugs 2002, 5, 325–338. [Google Scholar] [CrossRef]
- Wong, J.; Hird, A.; Kirou-Mauro, A.; Napolskikh, J.; Chow, E. Quality of Life in Brain Metastases Radiation Trials: A Literature Review. Curr. Oncol. 2008, 5, 25–45. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.; Bexelius, C.; Munk, V.; Leighl, N. The Impact of Brain Metastasis on Quality of Life, Resource Utilization and Survival in Patients with Non-Small-Cell Lung Cancer. Cancer Treat. Rev. 2016, 45, 139–162. [Google Scholar] [CrossRef]
- Hatiboglu, M.A.; Akdur, K.; Sawaya, R. Neurosurgical Management of Patients with Brain Metastasis. Neurosurg Rev. 2020, 2, 483–495. [Google Scholar] [CrossRef]
- Johung, K.L.; Yeh, N.B.; Desai, T.M.; Williams, T.; Lautenschlaeger, N.D.; Arvold, M.S.; Ning, A.; Attia, C.M.; Lovly, S. Extended Survival and Prognostic Factors for Patients with Alk-Rearranged Non-Small-Cell Lung Cancer and Brain Metastasis. J. Clin. Oncol. 2016, 2, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, M.; Heimann, C.; Schaub, L.; Eichhorn, A.L.; Potthoff, F.A.; Giordano, E.; Güresir, Y.D.; Ko, J.; Landsberg, F. Comorbidity Burden and Presence of Multiple Intracranial Lesions Are Associated with Adverse Events after Surgical Treatment of Patients with Brain Metastases. Cancers 2020, 11, 3209. [Google Scholar] [CrossRef] [PubMed]
- Schuss, P.; Güresir, Á.; Schneider, M.; Velten, M.; Vatter, H.; Güresir, E. Factors Influencing Early Postoperative Complications Following Surgery for Symptomatic Spinal Metastasis: A Single-Center Series and Multivariate Analysis. Neurosurg. Rev. 2020, 1, 211–216. [Google Scholar] [CrossRef]
- Im, K.; Belle, S.H.; Schulz, R.; Mendelsohn, A.B.; Chelluri, L.; Qol-Mv Investigators. Prevalence and Outcomes of Caregiving after Prolonged (> or =48 Hours) Mechanical Ventilation in the Icu. Chest 2004, 2, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Borger, V.; Grigutsch, D.; Güresir, A.; Potthoff, Á.L.; Velten, M.; Vatter, H.; Güresir, E.; Schuss, P. Elevated Body Mass Index Facilitates Early Postoperative Complications after Surgery for Intracranial Meningioma. Neurosurg. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Ilic, I.; Potthoff, A.L.; Hamed, M.; Schäfer, N.; Velten, M.; Güresir, E.; Herrlinger, U.; Borger, V.; Vatter, H.; et al. Safety Metric Profiling in Surgery for Temporal Glioblastoma: Lobectomy as a Supra-Total Resection Regime Preserves Perioperative Standard Quality Rates. J. Neurooncol. 2020, 3, 455–461. [Google Scholar] [CrossRef]
- Schodel, P.; Junger, S.T.; Wittersheim, M.; Reinhardt, H.C.; Schmidt, N.O.; Goldbrunner, R.; Proescholdt, M.; Grau, S. Surgical Resection of Symptomatic Brain Metastases Improves the Clinical Status and Facilitates Further Treatment. Cancer Med. 2020, 20, 7503–7510. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Potthoff, A.L.; Keil, V.C.; Güresir, Á.; Weller, J.; Borger, V.; Hamed, M.; Waha, A.; Vatter, H.; Güresir, E.; et al. Surgery for Temporal Glioblastoma: Lobectomy Outranks Oncosurgical-Based Gross-Total Resection. J. Neurooncol. 2019, 1, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Atzil, S.; Arad, M.; Glasner, A.; Abiri, N.; Avraham, R.; Greenfeld, K.; Rosenne, E.; Beilin, B.; Ben-Eliyahu, S. Blood Transfusion Promotes Cancer Progression: A Critical Role for Aged Erythrocytes. Anesthesiology 2008, 6, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Cata, J.P.; Wang, H.; Gottumukkala, V.; Reuben, J.; Sessler, D.I. Inflammatory Response, Immunosuppression, and Cancer Recurrence after Perioperative Blood Transfusions. Br. J. Anaesth. 2013, 5, 690–701. [Google Scholar] [CrossRef] [Green Version]
- Connor, J.P.; O’Shea, A.; McCool, K.; Sampene, E.; Barroilhet, L.M. Peri-Operative Allogeneic Blood Transfusion Is Associated with Poor Overall Survival in Advanced Epithelial Ovarian Cancer; Potential Impact of Patient Blood Management on Cancer Outcomes. Gynecol. Oncol. 2018, 2, 294–298. [Google Scholar] [CrossRef]
- Shih, C.Y.; Hung, M.C.; Lu, H.M.; Chen, L.; Huang, S.J.; Wang, J.D. Incidence, Life Expectancy and Prognostic Factors in Cancer Patients under Prolonged Mechanical Ventilation: A Nationwide Analysis of 5.138 Cases During 1998–2007. Crit. Care 2013, 4, R144. [Google Scholar] [CrossRef] [Green Version]
- Churilla, T.M.; Chowdhury, I.H.; Handorf, E.; Collette, L.; Collette, S.; Dong, Y.; Alexander, B.M.; Kocher, M.; Soffietti, R.; Claus, E.B.; et al. Comparison of Local Control of Brain Metastases with Stereotactic Radiosurgery Vs Surgical Resection: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2019, 2, 243–247. [Google Scholar] [CrossRef]
- Chirieac, L.R. Tumor Cell Proliferation, Proliferative Index and Mitotic Count in Lung Cancer. Transl. Lung Cancer Res. 2016, 5, 554–556. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.; Paesmans, M.; Mascaux, C.; Berghmans, T.; Lothaire, P.; Meert, A.P.; Lafitte, J.J.; Sculier, J.P. Ki-67 Expression and Patients Survival in Lung Cancer: Systematic Review of the Literature with Meta-Analysis. Br. J. Cancer 2004, 12, 2018–2025. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.N.; Sorensen, J.B. Clinical Impact of Ki-67 Labeling Index in Non-Small Cell Lung Cancer. Lung Cancer 2013, 1, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Warth, A.; Cortis, A.; Soltermann, M.; Meister, J.; Budczies, A.; Stenzinger, B.; Goeppert, M.; Thomas, F.J.; Herth, P. Tumour Cell Proliferation (Ki-67) in Non-Small Cell Lung Cancer: A Critical Reappraisal of Its Prognostic Role. Br. J. Cancer 2014, 6, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, E.; Le Teuff, G.; Marguet, S.; Lantuejoul, S.; Dunant, A.; Graziano, S.; Pirker, R.; Douillard, J.Y.; Le Chevalier, T. Prognostic Effect of Tumor Lymphocytic Infiltration in Resectable Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 11, 1223–1230. [Google Scholar] [CrossRef]
- Al-Alao, B.S.; Gately, K.; Nicholson, S.; McGovern, E.; Young, V.K.; O’Byrne, K.J. Prognostic Impact of Vascular and Lymphovascular Invasion in Early Lung Cancer. Asian Cardiovasc. Thorac. Ann. 2014, 1, 55–64. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | N of Patients (n = 154) |
|---|---|
| Median age at surgery | 63 (range 40–86) |
| Female sex | 74 (48%) |
| Median preoperative KPS | 80 (range 30–100) |
| ASA ≥ 3 | 89 (58%) |
| Age-adjusted CCI > 10 | 79 (51%) |
| Multiple BM | 54 (35%) |
| Infratentorial location of BM | 54 (35%) |
| Admission CRP > 10 mg/dL | 33 (21%) |
| Admission WBC > 12 G/L | 93 (60%) |
| Postoperative PMV ≥ 48 h | 7 (5%) |
| Perioperative RBC transfusion(within 5 days) | 19 (12%) |
| Occurrence of PAE | 13 (8%) |
| 12 months of mortality | 83 (54%) |
| Median OS (mo) | 11 (95% CI 8.2–13.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneider, M.; Schäfer, N.; Bode, C.; Eichhorn, L.; Giordano, F.A.; Güresir, E.; Heimann, M.; Ko, Y.-D.; Landsberg, J.; Lehmann, F.; et al. The Surgical Management of Brain Metastases in Non-Small Cell Lung Cancer (NSCLC): Identification of the Early Laboratory and Clinical Determinants of Survival. J. Clin. Med. 2021, 10, 4013. https://doi.org/10.3390/jcm10174013
Schneider M, Schäfer N, Bode C, Eichhorn L, Giordano FA, Güresir E, Heimann M, Ko Y-D, Landsberg J, Lehmann F, et al. The Surgical Management of Brain Metastases in Non-Small Cell Lung Cancer (NSCLC): Identification of the Early Laboratory and Clinical Determinants of Survival. Journal of Clinical Medicine. 2021; 10(17):4013. https://doi.org/10.3390/jcm10174013
Chicago/Turabian StyleSchneider, Matthias, Niklas Schäfer, Christian Bode, Lars Eichhorn, Frank A. Giordano, Erdem Güresir, Muriel Heimann, Yon-Dschun Ko, Jennifer Landsberg, Felix Lehmann, and et al. 2021. "The Surgical Management of Brain Metastases in Non-Small Cell Lung Cancer (NSCLC): Identification of the Early Laboratory and Clinical Determinants of Survival" Journal of Clinical Medicine 10, no. 17: 4013. https://doi.org/10.3390/jcm10174013
APA StyleSchneider, M., Schäfer, N., Bode, C., Eichhorn, L., Giordano, F. A., Güresir, E., Heimann, M., Ko, Y.-D., Landsberg, J., Lehmann, F., Radbruch, A., Schaub, C., Schwab, K. S., Weller, J., Herrlinger, U., Vatter, H., & Schuss, P. (2021). The Surgical Management of Brain Metastases in Non-Small Cell Lung Cancer (NSCLC): Identification of the Early Laboratory and Clinical Determinants of Survival. Journal of Clinical Medicine, 10(17), 4013. https://doi.org/10.3390/jcm10174013