
Balloon-Expandable versus Self-Expandable Valves in Transcatheter Aortic Valve Implantation: Complications and Outcomes from a Large International Patient Cohort

 , , , ,
, , , , 
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
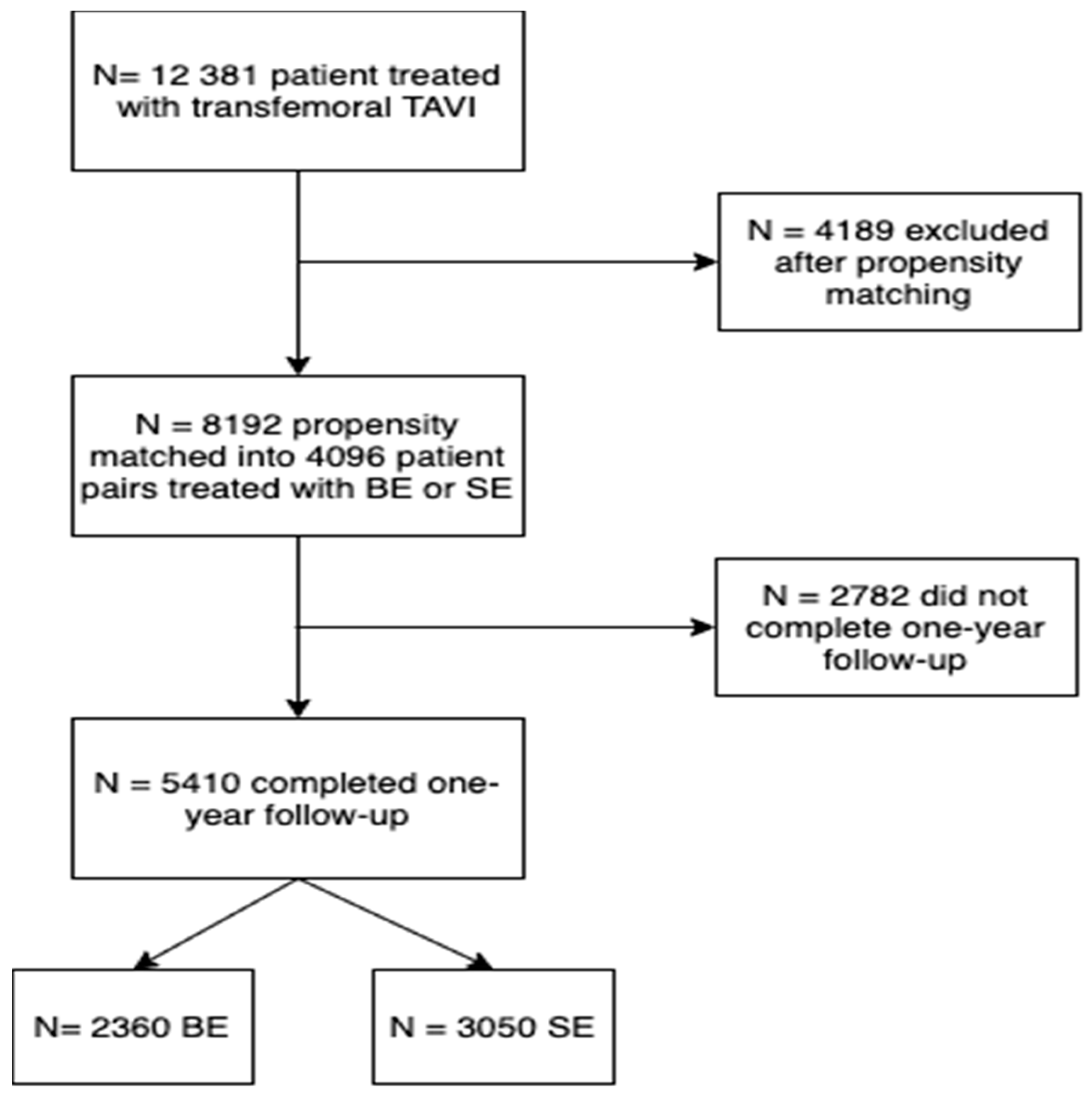
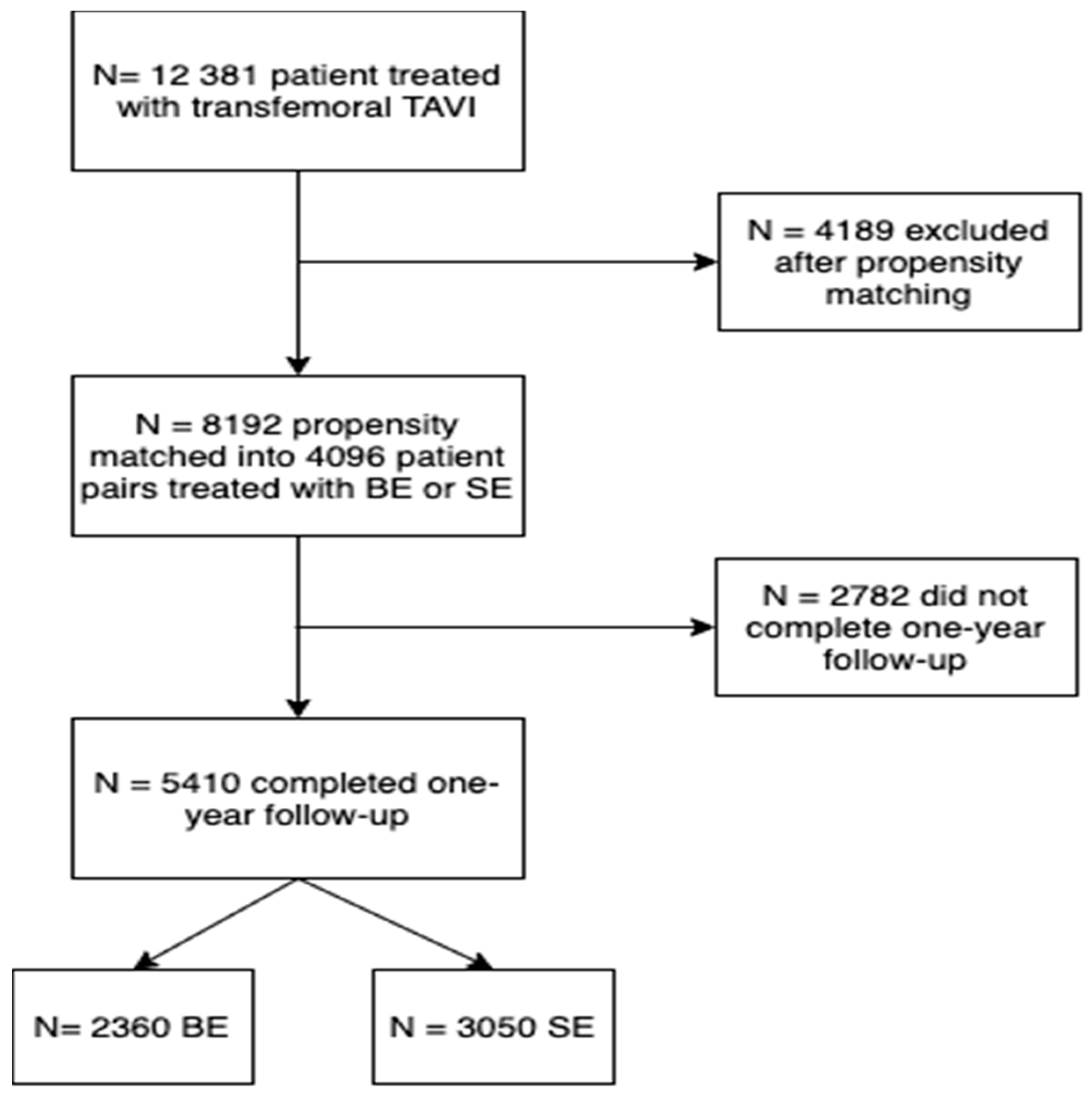
2.1. Study Design and Patient Sample
2.2. Study Endpoints
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Overall Study Population
3.2. Baseline Characteristics of the Matched Study Population
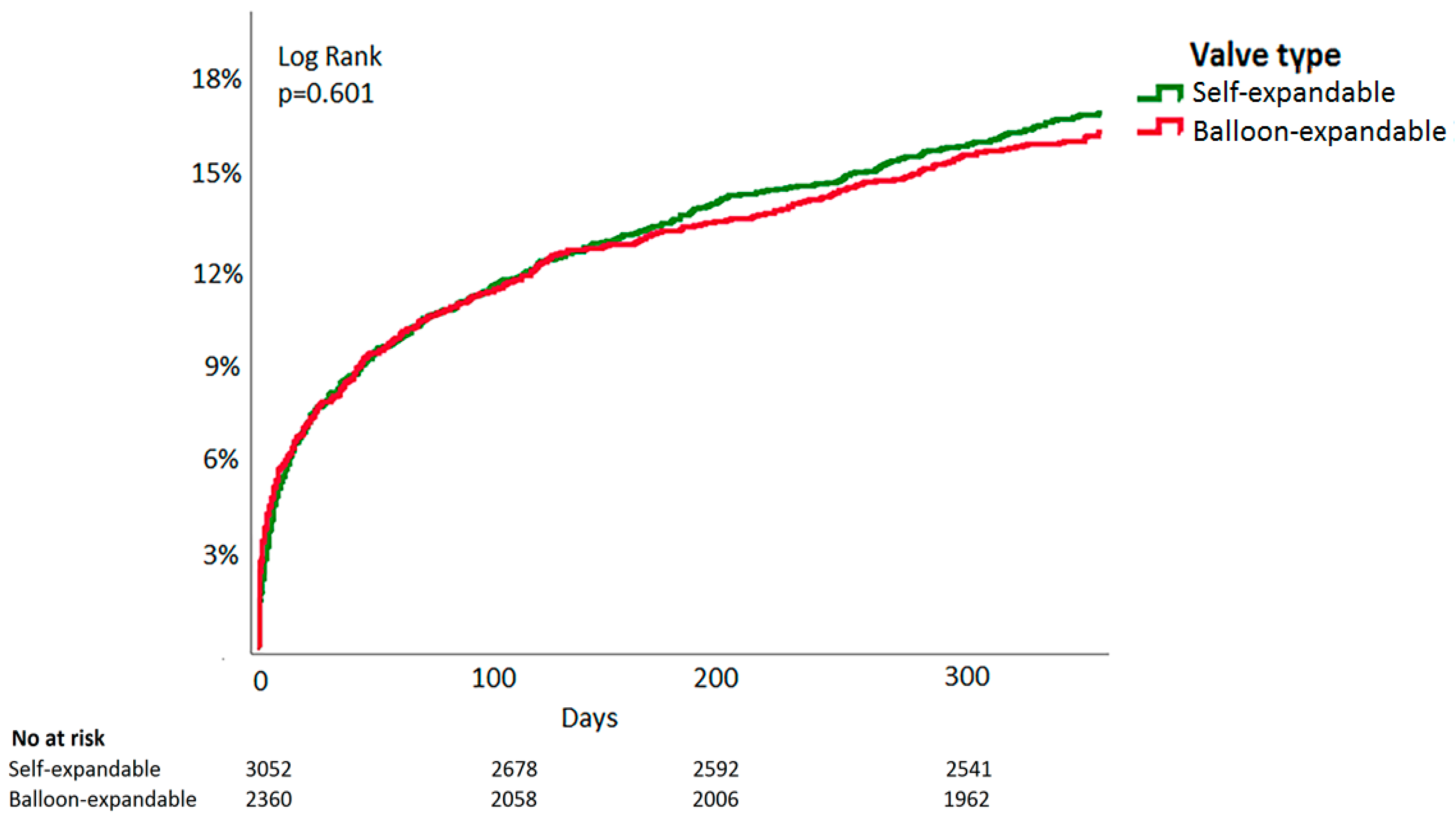
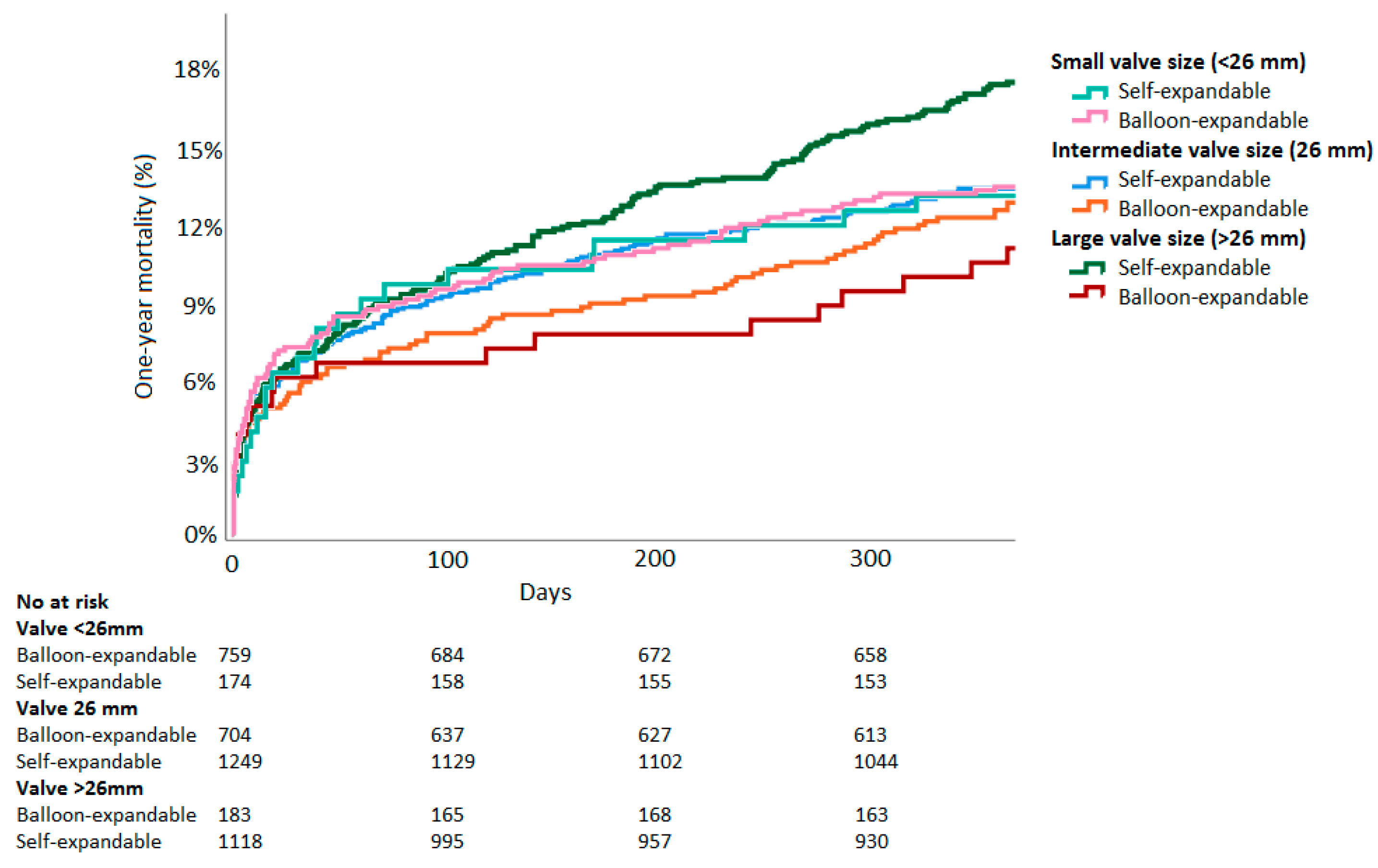
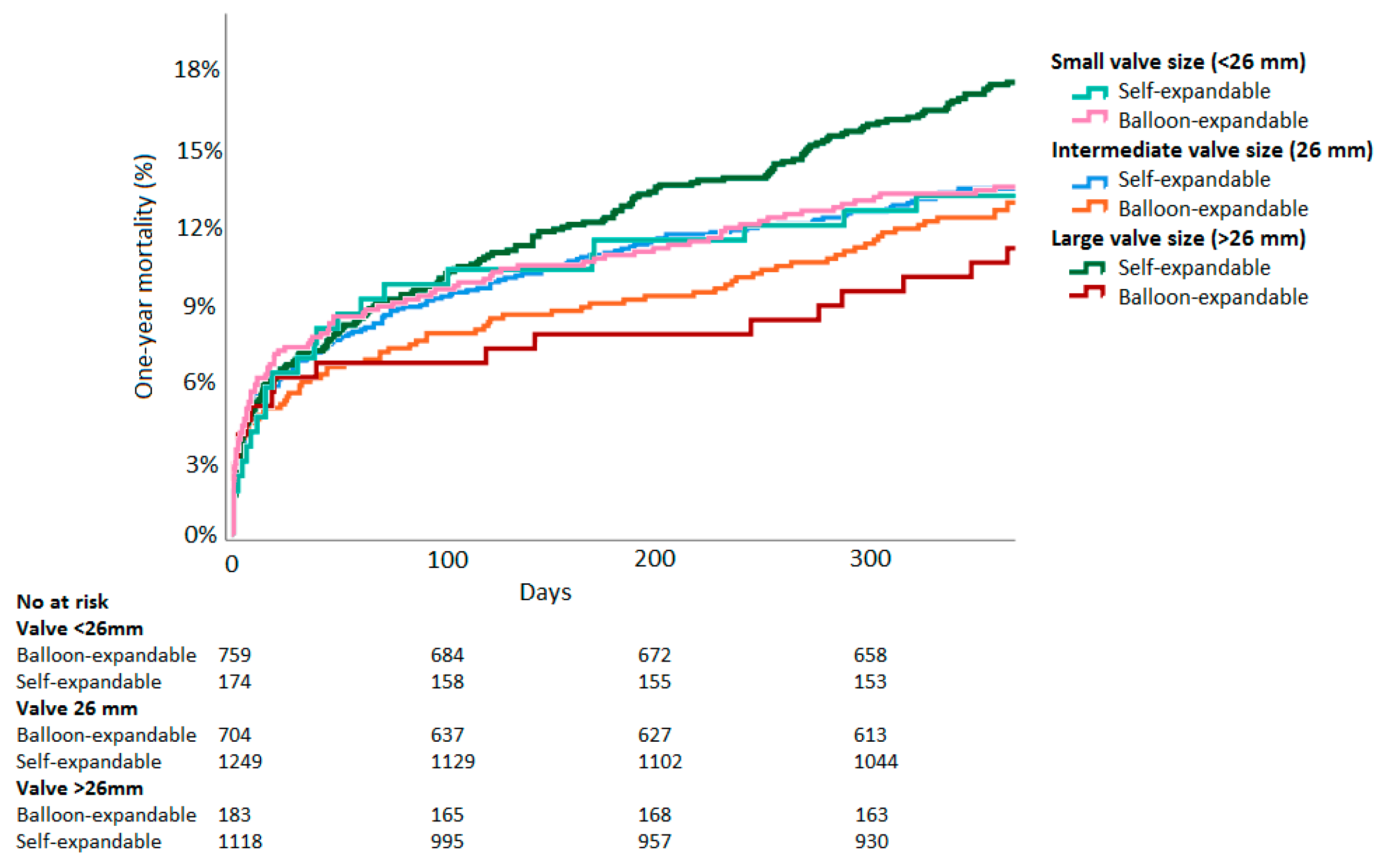
3.3. One-Year Mortality
3.4. One-Year Stroke Rates
3.5. Safety of Early Outcomes
4. Discussion
4.1. Main Findings
4.2. Mortality
4.3. Stroke
4.4. Future Perspectives
4.5. Early Safety Outcomes
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Binder, R.K.; Rodés-Cabau, J.; Wood, D.A.; Mok, M.; Leipsic, J.; De Larochellière, R.; Toggweiler, S.; Dumont, E.; Freeman, M.; Willson, A.B.; et al. Transcatheter aortic valve replacement with the SAPIEN 3: A new balloon-expandable transcatheter heart valve. JACC Cardiovasc. Interv. 2013, 6, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Popma, J.J.; Reardon, M.J.; Khabbaz, K.; Harrison, J.K.; Hughes, G.C.; Kodali, S.; George, I.; Deeb, G.M.; Chetcuti, S.; Kipperman, R.; et al. Early Clinical Outcomes After Transcatheter Aortic Valve Replacement Using a Novel Self-Expanding Bioprosthesis in Patients with Severe Aortic Stenosis Who Are Suboptimal for Surgery: Results of the Evolut R U.S. Study. JACC Cardiovasc. Interv. 2017, 10, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Vlastra, W.; Chandrasekhar, J.; Muñoz-Garcia, A.J.; Tchétché, D.; De Brito, F.S.; Barbanti, M.; Kornowski, R.; Latib, A.; D’Onofrio, A.; Ribichini, F.; et al. Comparison of balloon-expandable vs. self-expandable valves in patients undergoing transfemoral transcatheter aortic valve implantation: From the CENTER-collaboration. Eur. Heart J. 2018, 40, 456–465. [Google Scholar] [CrossRef]
- Thiele, H.; Kurz, T.; Feistritzer, H.-J.; Stachel, G.; Hartung, P.; Eitel, I.; Marquetand, C.; Nef, H.; Doerr, O.; Lauten, A.; et al. Comparison of newer generation self-expandable vs. balloon-expandable valves in transcatheter aortic valve implantation: The randomized SOLVE-TAVI trial. Eur. Heart J. 2020, 41, 1890–1899. [Google Scholar] [CrossRef]
- Reardon, M.J.; Feldman, T.E.; Meduri, C.U.; Makkar, R.R.; O’Hair, D.; Linke, A.; Kereiakes, D.J.; Waksman, R.; Babliaros, V.; Stoler, R.C.; et al. Two-Year Outcomes after Transcatheter Aortic Valve Replacement with Mechanical vs Self-expanding Valves: The REPRISE III Randomized Clinical Trial. JAMA Cardiol. 2019, 4, 223–229. [Google Scholar] [CrossRef]
- Abdel-Wahab, M.; Neumann, F.J.; Mehilli, J.; Frerker, C.; Richardt, D.; Landt, M.; Jose, J.; Toelg, R.; Kuck, K.H.; Massberg, S.; et al. 1-year outcomes after transcatheter aortic valve replacement with balloon-expandable versus self-expandable valves: Results from the CHOICE randomized clinical trial. J Am. Coll. Cardiol. 2015, 66, 791–800. [Google Scholar] [CrossRef] [Green Version]
- Van Belle, E.; Vincent, F.; Labreuche, J.; Auffret, V.; Debry, N.; Lefèvre, T.; Eltchaninoff, H.; Manigold, T.; Gilard, M.; Verhoye, J.P.; et al. Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Replacement: A Propensity-Matched Comparison From the FRANCE-TAVI Registry. Circulation 2020, 141, 243–259. [Google Scholar] [CrossRef]
- Deharo, P.; Bisson, A.; Herbert, J.; Lacour, T.; Saint Etienne, C.; Grammatico-Guillon, L.; Porto, A.; Collart, F.; Bourguignon, T.; Cuisset, T.; et al. Impact of Sapien 3 Balloon-Expandable Versus Evolut R Self-Expandable Transcatheter Aortic Valve Implantation in Patients with Aortic Stenosis: Data from a Nationwide Analysis. Circulation 2020, 141, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. EuroIntervention 2012, 8, 782–795. [Google Scholar] [CrossRef] [Green Version]
- Tamburino, C.; Barbanti, M.; D’Errigo, P.; Ranucci, M.; Onorati, F.; Covello, R.D.; Santini, F.; Rosato, S.; Santoro, G.; Fusco, D.; et al. 1-year outcomes after transfemoral transcatheter or surgical aortic valve replacement: Results from the Italian OBSERVANT study. J. Am. Coll. Cardiol. 2015, 66, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.; Landt, M.; Neumann, F.J.; Massberg, S.; Frerker, C.; Kurz, T.; Kaur, J.; Toelg, R.; Sachse, S.; Jochheim, D.; et al. 5-Year Outcomes After TAVR With Balloon-Expandable Versus Self-Expanding Valves: Results from the CHOICE Randomized Clinical Trial. JACC Cardiovasc. Interv. 2020, 13, 1071–1082. [Google Scholar] [CrossRef] [PubMed]
- Feistritzer, H.-J.; Kurz, T.; Stachel, G.; Hartung, P.; Lurz, P.; Eitel, I.; Marquetand, C.; Nef, H.; Doerr, O.; Vigelius-Rauch, U.; et al. Impact of Anesthesia Strategy and Valve Type on Clinical Outcomes After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2021, 77, 2204–2215. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R.; Rich, J.B.; Zoghbi, W.A.; Mack, M.J. The Heart Team of Cardiovascular Care. J. Am. Coll. Cardiol. 2013, 61, 903–907. [Google Scholar] [CrossRef] [Green Version]
- Giannini, C.; Petronio, A.S.; Mehilli, J.; Sartori, S.; Chandrasekhar, J.; Faggioni, M.; Lefèvre, T.; Presbitero, P.; Capranzano, P.; Tchetche, D.; et al. Edwards SAPIEN Versus Medtronic Aortic Bioprosthesis in Women Undergoing Transcatheter Aortic Valve Implantation (from the Win-TAVI Registry). Am. J. Cardiol. 2019, 125, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Rogers, T.; Steinvil, A.; Gai, J.; Torguson, R.; Koifman, E.; Kiramijyan, S.; Negi, S.; Lee, S.Y.; Okubagzi, P.; Satler, L.F.; et al. Choice of Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Impacts Hemodynamics Differently According to Aortic Annular Size. Am. J. Cardiol. 2016, 119, 900–904. [Google Scholar] [CrossRef]
- Rodés-Cabau, J.; Pibarot, P.; Suri, R.M.; Kodali, S.; Thourani, V.H.; Szeto, W.Y.; Svensson, L.G.; Dumont, E.; Xu, K.; Hahn, R.T.; et al. Impact of aortic annulus size on valve hemodynamics and clinical outcomes after transcatheter and surgical aortic valve replacement insights from the PARTNER trial. Circ. Cardiovasc. Interv. 2014, 7, 701–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelghani, M.; Mankerious, N.; Allali, A.; Landt, M.; Kaur, J.; Sulimov, D.S.; Merten, C.; Sachse, S.; Mehilli, J.; Neumann, F.J.; et al. Bioprosthetic Valve Performance After Transcatheter Aortic Valve Replacement With Self-Expanding Versus Balloon-Expandable Valves in Large Versus Small Aortic Valve Annuli: Insights From the CHOICE Trial and the CHOICE-Extend Registry. JACC Cardiovasc. Interv. 2018, 11, 2507–2518. [Google Scholar] [CrossRef] [PubMed]
- Van Mieghem, N.M.; El Faquir, N.; Rahhab, Z.; Rodríguez-Olivares, R.; Wilschut, J.; Ouhlous, M.; Galema, T.W.; Geleijnse, M.L.; Kappetein, A.P.; Schipper, M.E.; et al. Incidence and predictors of debris embolizing to the brain during transcatheter aortic valve implantation. JACC Cardiovasc. Interv. 2015, 8, 718–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muntané-Carol, G.; Urena, M.; Munoz-Garcia, A.; Padrón, R.; Gutiérrez, E.; Regueiro, A.; Serra, V.; Capretti, G.; Himbert, D.; Moris, C.; et al. Late Cerebrovascular Events Following Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 872–881. [Google Scholar] [CrossRef] [PubMed]
- Fischer, Q.; Urena, M.; Bouleti, C.; Abtan, J.; Brochet, E.; Carrasco, J.-L.; Iung, B.; Vahanian, A.; Himbert, D. Performing optimal transcatheter aortic valve implantation: The need for tailored use of transcatheter valves. Arch. Cardiovasc. Dis. 2019, 112, 512–522. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Balloon-Expandable (n = 2360) | Self-Expandable (n = 3050) | p-Value | |
|---|---|---|---|
| Age (years) | 81.3 ± 7.1 | 81.3 ± 6.9 | 0.89 |
| Female gender | 1417 (60%) | 1822 (60%) | 0.82 |
| Body mass index (kg/m2) | 27.1 ± 4.8 | 27.1 ± 4.9 | 0.83 |
| Previous CVA or TIA | 236 (10%) | 333 (11%) | 0.28 |
| Previous MI | 317 (13%) | 423 (14%) | 0.64 |
| Previous PCI | 507 (22%) | 672 (22%) | 0.62 |
| Previous CABG | 289 (12%) | 379 (12%) | 0.84 |
| Diabetes Mellitus | 742 (31%) | 994 (33%) | 0.37 |
| Hypertension | 1895 (80%) | 2430 (80%) | 0.57 |
| Dyslipidaemia | 1324 (56%) | 1722 (57%) | 0.79 |
| Peripheral artery disease | 354 (15%) | 441 (15%) | 0.58 |
| Coronary artery disease | 954 (40%) | 1230 (40%) | 0.94 |
| Atrial Fibrillation | 622 (26%) | 845 (28%) | 0.27 |
| GFR < 30 mL/min | 358 (15%) | 451 (15%) | 0.70 |
| Aortic max gradient (mmHg) | 78.2 ± 23.1 | 80.5 ± 24.3 | 0.002 |
| Aortic mean gradient (mmHg) | 49.2 ± 16.6 | 50.7 ± 17.1 | 0.001 |
| Aortic valve area (cm2) | 0.67 ± 0.20 | 0.64 ± 0.20 | <0.001 |
| Third generation valve | 614 (26%) | 791 (26%) | 0.90 |
| Valve in valve | 42 (2%) | 90 (3%) | 0.002 |
| Valve size (mm) | 26 (23–26) | 26 (26–29) | <0.001 |
| Year of procedure | 2012 (2011–2014) | 2012 (2010–2014) | <0.001 |
| Balloon-Expandable | Self-Expandable | |
|---|---|---|
| 20 mm | 4 (0.2%) | - |
| 23 mm | 755 (46%) | 174 (7%) |
| 26 mm | 704 (43%) | 1249 (49%) |
| 29 mm | 183 (12%) | 1022 (40%) |
| 31 mm | - | 93 (4%) |
| 34 mm | - | 3 (0.1%) |
| Balloon-Expandable (n = 2369) | Self-Expandable (n = 3050) | Relative Risk (95%CI) | p-Value | |
|---|---|---|---|---|
| Conversion to open heart surgery | 22 (1.0%) | 20 (0.7%) | 0.70 (0.39–1.29) | 0.25 |
| Device Success | 1831 (95.5%) | 2161 (91.3%) | 0.96 (0.94–0.97) | <0.001 |
| Stroke | 67 (2.8%) | 94 (3.1%) | 1.09 (0.80–1.48) | 0.60 |
| Myocardial infarction | 23 (1.1%) | 22 (0.8%) | 0.73 (0.41–1.30) | 0.28 |
| Major or life-threatening bleeding | 143 (6.9%) | 179 (6.5%) | 0.95 (0.77–1.18) | 0.65 |
| Permanent pacemaker implantation | 170 (7.4%) | 606 (20.2%) | 2.73 (2.32–3.21) | <0.001 |
| Length of hospital stay | 7 (5–11) | 7 (5–11) | - | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Nieuwkerk, A.C.; Santos, R.B.; Andraka, L.; Tchetche, D.; de Brito, F.S.; Barbanti, M.; Kornowski, R.; Latib, A.; D’Onofrio, A.; Ribichini, F.; et al. Balloon-Expandable versus Self-Expandable Valves in Transcatheter Aortic Valve Implantation: Complications and Outcomes from a Large International Patient Cohort. J. Clin. Med. 2021, 10, 4005. https://doi.org/10.3390/jcm10174005
van Nieuwkerk AC, Santos RB, Andraka L, Tchetche D, de Brito FS, Barbanti M, Kornowski R, Latib A, D’Onofrio A, Ribichini F, et al. Balloon-Expandable versus Self-Expandable Valves in Transcatheter Aortic Valve Implantation: Complications and Outcomes from a Large International Patient Cohort. Journal of Clinical Medicine. 2021; 10(17):4005. https://doi.org/10.3390/jcm10174005
Chicago/Turabian Stylevan Nieuwkerk, Astrid C., Raquel B Santos, Leire Andraka, Didier Tchetche, Fabio S. de Brito, Marco Barbanti, Ran Kornowski, Azeem Latib, Augusto D’Onofrio, Flavio Ribichini, and et al. 2021. "Balloon-Expandable versus Self-Expandable Valves in Transcatheter Aortic Valve Implantation: Complications and Outcomes from a Large International Patient Cohort" Journal of Clinical Medicine 10, no. 17: 4005. https://doi.org/10.3390/jcm10174005
APA Stylevan Nieuwkerk, A. C., Santos, R. B., Andraka, L., Tchetche, D., de Brito, F. S., Barbanti, M., Kornowski, R., Latib, A., D’Onofrio, A., Ribichini, F., Ten, F., Dumonteil, N., Baan, J., Piek, J. J., Abizaid, A., Sartori, S., D’Errigo, P., Tarantini, G., Lunardi, M., ... Delewi, R. (2021). Balloon-Expandable versus Self-Expandable Valves in Transcatheter Aortic Valve Implantation: Complications and Outcomes from a Large International Patient Cohort. Journal of Clinical Medicine, 10(17), 4005. https://doi.org/10.3390/jcm10174005