
Analysis of Neural Interface When Using Modiolar Electrode Stimulation. Radiological Evaluation, Trans-Impedance Matrix Analysis and Effect on Listening Effort in Cochlear Implantation



Abstract
1. Introduction
2. Materials and Methods
2.1. Pitch Discrimination Method
2.2. Pupillometry Method
2.3. Radiological Study
2.4. Wrapping Factor (WF)
2.5. Intracochlear Position Index (ICPI)
2.6. Homogeneity Factor (HF)
2.7. TransImpedance Matrix (TIM)
2.8. Statistical Analysis
3. Results
3.1. Electrode Discrimination Test
3.2. Radiological Studies
3.3. Pupillometry Test
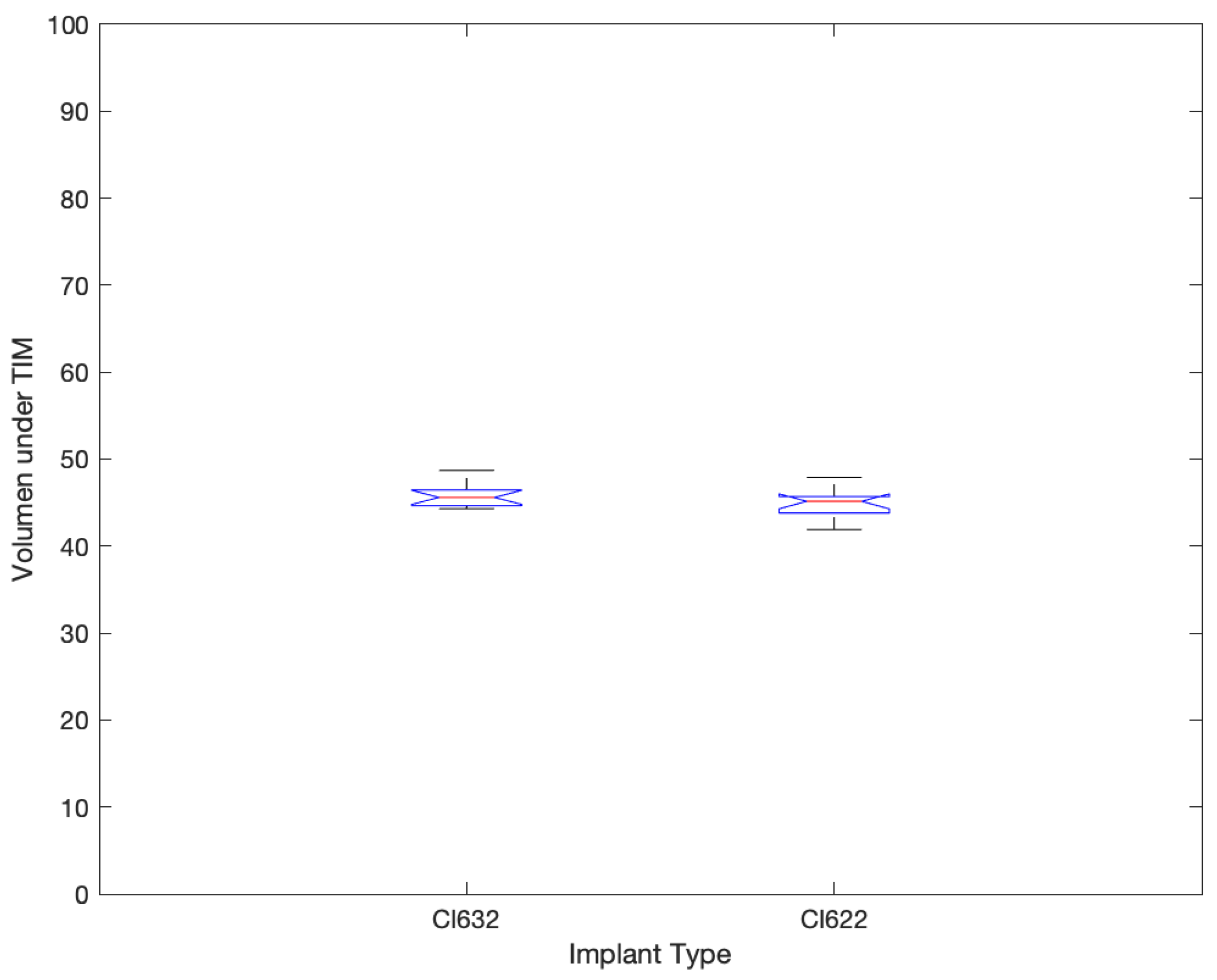
3.4. T.I.M.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saunders, E.; Cohen, L.; Aschendorff, A.; Shapiro, W.; Knight, M.; Stecker, M.; Laszig, R. Threshold, comfortable level and impedance changes as a function of electrode-modiolar distance. Ear Hear. 2002, 23, 28S–40S. [Google Scholar] [CrossRef]
- McKay, C.M.; O’Brien, A.; James, C.J. Effect of current level on electrode discrimination in electrical stimulation. Hear. Res. 1999, 136, 159–164. [Google Scholar] [CrossRef]
- Shepherd, R.K.; Hatsushika, S.; Clark, G.M. Electrical stimulation of the auditory nerve: The effect of electrode position on neural excitation. Hear. Res. 1993, 66, 108–120. [Google Scholar] [CrossRef]
- Pfingst, B.E.; Holloway, L.A.; Zwolan, T.A.; Collins, L.M. Effects of stimulus level on electrode-place discrimination in human subjects with cochlear implants. Hear. Res. 1993, 66, 108–120. [Google Scholar] [CrossRef]
- DeVries, L.; Scheperle, R.; Bierer, J.A. Assessing the elec- trode-neuron interface with the electrically evoked compound action potential, electrode position, and behavioral thresholds. J. Assoc. Res. Otolaryngol. 2016, 17, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.J.; Nogaki, G. Noise susceptibility of cochlear implant users: The role of spectral resolution and smearing. J. Assoc. Res. Otolaryngol. 2005, 6, 19–27. [Google Scholar] [CrossRef]
- Finley, C.C.; Holden, T.A.; Holden, L.K.; Whiting, B.R.; Chole, R.A.; Neely, G.J.; Hullar, T.E.; Skinner, M.W. Role of electrode placement as a contributor to variability in cochlear implant outcomes. Otol. Neurotol. 2008, 29, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Boëx, C.; de Balthasar, C.; Kós, M.I.; Pelizzone, M. Electrical field interactions in different cochlear implant systems. J. Acoust. Soc. Am. 2003, 114 (4 Pt 1), 2049–2057. [Google Scholar] [CrossRef]
- Hornsby, B.W. The effects of hearing aid use on listening effort and mental fatigue associated with sustained speech processing demands. Ear Hear. 2013, 34, 523–534. [Google Scholar] [CrossRef]
- Chapman, L.R.; Hallowell, B. A novel pupillometric method for indexing word difficulty in individuals with and without aphasia. J. Speech Lang. Hear. Res. 2015, 58, 1508–1520. [Google Scholar] [CrossRef]
- Blamey, P.; Artieres, F.; Baskent, D.; Bergeron, F.; Beynon, A.; Burke, E.; Govaerts, P.J. Factors affecting audi-tory performance of postlinguistically deaf adults using cochlear implants: An update with 2251 patients. Audiol. Neurotol. 2013, 18, 36–47. [Google Scholar] [CrossRef]
- Killion, M.C.; Niquette, P.A.; Gudmundsen, G.I.; Revit, L.J.; Banerjee, S. Development of a quick speech- in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. J. Acoust. Soc. Am. 2004, 116, 2395–2405. [Google Scholar] [CrossRef] [PubMed]
- Hess, E.H.; Polt, J.M. Pupil size in relation to mental activity during simple problem-solving. Science 1964, 143, 1190–1192. [Google Scholar] [CrossRef] [PubMed]
- Borghini, G.; Hazan, V. Listening effort during sentence processing is increased for non-native listeners: A pupillometry study. Front. Neurosci. 2018, 12, 152. [Google Scholar] [CrossRef]
- Piquado, T.; Isaacowitz, D.; Wingfield, A. Pupillometry as a measure of cognitive effort in younger and older adults. Psychophysiology 2010, 47, 560–569. [Google Scholar] [CrossRef]
- Hey, M.; Böhnke, B.; Dillier, N.; Hoppe, U.; Eskilsson, G.; Löwgren, K.; Müller-Deile, J. The Intra-Cochlear Impedance-Matrix (IIM) test for the Nucleus® cochlear implant. Biomed. Eng./Biomed. Tech. 2015, 60, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Klabbers, T.M.; Huinck, W.J.; Heutink, F.; Verbist, B.M.; Mylanus, E.A.M. Transimpedance Matrix (TIM) Measurement for the Detection of Intraoperative Electrode Tip Foldover Using the Slim Modiolar Electrode: A Proof of Concept Study. Otol. Neurotol. 2021, 42, e124–e129. [Google Scholar] [CrossRef]
- Whiting, B.R.; Holden, T.A.; Brunsden, B.S.; Finley, C.C.; Skinner, M.W. Use of computed tomography scans for cochlear implants. J. Digit. Imaging 2008, 21, 323–328. [Google Scholar] [CrossRef]
- Henry, B.A.; McKay, C.M.; McDermott, H.J.; Clark, G.M. The relation-ship between speech perception and electrode discrimination in cochlear implantees. J. Acoust. Soc. Am. 2000, 108, 1269–1280. [Google Scholar] [CrossRef] [PubMed]
- Vickers, D.; Degun, A.; Canas, A.; Stainsby, T.; Vanpoucke, F. Deactivating cochlear implant electrodes based on pitch information for users of the ACE strategy. Adv. Exp. Med. Biol. 2016, 894, 115–123. [Google Scholar]
- Zwolan, T.A.; Collins, L.M.; Wakefield, G.H. Electrode discrimination and speech recognition in postlingually deafened adult cochlear implant subjects. J. Acoust. Soc. Am. 1997, 102, 3673–3685. [Google Scholar] [CrossRef] [PubMed]
- Huarte, A. The Castilian Spanish Hearing in Noise Test. Int. J. Audiol. 2008, 47, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Ramos Macias, A.; Perez Zaballos, M.T.; Ramos de Miguel, A.; Cervera Paz, J. Importance of Perimodiolar Electrode Position for Psychoacoustic Discrimination in Cochlear Implantation. Otol. Neurotol. 2017, 38, e429–e437. [Google Scholar] [CrossRef] [PubMed]
- Cushing, S.L.; Daly, M.J.; Treaba, C.G.; Chan, H.; Irish, J.C.; Blaser, S.; Papsin, B.C. High-resolution Cone-Beam computed tomography: A potential tool to improve atraumatic electrode design and position. Acta Otolaryngol. 2012, 132, 361–368. [Google Scholar] [CrossRef] [PubMed]
- de Miguel, Á.R.; Durmo, I.; González, J.C.; Barreiro, S.B.; Macías, A.R. Evaluation of Intracochlear Position of a Slim Modiolar Electrode Array, by Using Different Radiological Analyses. Otol. Neurotol. 2019, 40 (5S Suppl. 1), S10–S17. [Google Scholar] [CrossRef]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open- set word recognition in adults with cochlear implants. Hear. Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef] [PubMed]
- Vanpoucke, F.J.; Boermans, P.P.B.; Frijns, J.H. Assessing the Placement of a Cochlear Electrode Array by Multidimensional Scaling. IEEE Trans. Biomed. Eng. 2012, 59, 307. [Google Scholar] [CrossRef] [PubMed]
- Ruivo, J.; Mermuys, K.; Bacher, K.; Kuhweide, R.; Offeciers, E.; Casselman, J.W. Cone beam computed tomography, a low-dose imaging technique in the postoperative assessment of cochlear implantation. Otol. Neurotol. 2009, 30, 299–303. [Google Scholar] [CrossRef]
- Pfingst, B.E.; Burkholder-Juhasz, R.A.; Zwolan, T.A.; Xu, L. Psychophysical assessment of stimulation sites in auditory pros- thesis electrode arrays. Hear. Res. 2008, 242, 172–183. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Skinner, M.W.; Holden, T.A.; Whiting, B.R.; Voie, A.H.; Brunsden, B.; Neely, J.G.; Finley, C.C. In vivo estimates of the position of advanced bionics electrode arrays in the human cochlea. Ann. Otol. Rhinol. Laryngol. 2007, 197, 2–24. [Google Scholar] [CrossRef]
- de Miguel, Á.R.; Argudo, A.A.; Barreiro, S.A.; González, J.C.; Macías, A.R. Imaging evaluation of electrode placement and effect on electrode discrimination on different cochlear implant electrode arrays. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Garaycochea, O.; Manrique-Huarte, R.; Lazaro, C.; Huarte, A.; Prieto, C.; de Linera-Alperi, M.A.; Manrique, M. Comparative study of two different perimodiolar and a straight cochlear implant electrode array: Surgical and audiological outcomes. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.H.; Labadie, R.F.; Gifford, R.H.; Dawant, B.M. Image—Guidance enables new methods for customizing cochlear implant stimulation strategies. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 820–829. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Type of Implant | Sex | Age (Years) | Prosthesis Use (Month) | Tinnitus | Number of Active Electrodes | Preop. Deafness Duration (Years) | Disyllabics % | Implant Ear |
|---|---|---|---|---|---|---|---|---|---|
| S1 | CI622 | F | 64 | 16 | No | 22 | 4 | 92 | R |
| S2 | CI622 | F | 26 | 29 | No | 22 | 7 | 76 | R |
| S3 | CI622 | M | 53 | 48 | No | 22 | 5 | 72 | R |
| S4 | CI622 | M | 70 | 20 | Yes | 22 | 6 | 80 | L |
| S5 | CI622 | F | 52 | 34 | No | 22 | 5 | 80 | R |
| S6 | CI622 | M | 34 | 27 | No | 22 | 8 | 84 | L |
| S7 | CI622 | M | 75 | 43 | No | 22 | 9 | 96 | L |
| S8 | CI622 | F | 66 | 16 | No | 22 | 12 | 96 | L |
| S9 | CI622 | M | 60 | 30 | No | 22 | 6 | 92 | R |
| S10 | CI622 | M | 32 | 36 | Yes | 22 | 1 | 76 | R |
| S11 | CI622 | M | 49 | 43 | No | 22 | 4 | 80 | L |
| S12 | CI622 | F | 57 | 48 | No | 22 | 11 | 92 | R |
| S13 | CI632 | M | 58 | 31 | No | 22 | 3 | 68 | L |
| S14 | CI632 | F | 56 | 12 | No | 22 | 9 | 96 | L |
| S15 | CI632 | F | 47 | 21 | No | 22 | 11 | 88 | R |
| S16 | CI632 | M | 30 | 17 | No | 22 | 1 | 92 | L |
| S17 | CI632 | M | 58 | 58 | No | 22 | 6 | 96 | L |
| S18 | CI632 | F | 28 | 22 | No | 22 | 3 | 88 | L |
| S19 | CI632 | M | 50 | 38 | Yes | 22 | 15 | 96 | R |
| S20 | CI632 | F | 75 | 27 | Yes | 22 | 9 | 88 | R |
| S21 | CI632 | M | 66 | 40 | No | 22 | 11 | 84 | L |
| S22 | CI632 | M | 70 | 20 | No | 22 | 3 | 88 | R |
| S23 | CI632 | M | 49 | 13 | No | 22 | 5 | 92 | L |
| S24 | CI632 | M | 47 | 12 | No | 22 | 2 | 88 | L |
| Subject | Implant | WF | ICPI | HF | Electrode Discrimination (%) | Pupil Dilatation (%) | Volume under TIM Surface |
|---|---|---|---|---|---|---|---|
| S1 | CI622 | 0.94 | 0.60 | 0.29 | 46 | 28 | 46.7 |
| S2 | CI622 | 0.77 | 0.62 | 0.28 | 64 | 28 | 45.4 |
| S3 | CI622 | 0.87 | 0.61 | 0.29 | 66 | 19 | 46.0 |
| S4 | CI622 | 0.81 | 0.62 | 0.28 | 69 | 25 | 45.4 |
| S5 | CI622 | 0.89 | 0.62 | 0.29 | 11 | 24 | 42.4 |
| S6 | CI622 | 0.80 | 0.61 | 0.28 | 29 | 31 | 45.4 |
| S7 | CI622 | 0.91 | 0.61 | 0.28 | 46 | 34 | 44.3 |
| S8 | CI622 | 0.87 | 0.63 | 0.28 | 46 | 34 | 44.0 |
| S9 | CI622 | 0.84 | 0.59 | 0.29 | 45 | 19 | 43.6 |
| S10 | CI622 | 0.79 | 0.61 | 0.27 | 66 | 26 | 44.9 |
| S11 | CI622 | 0.91 | 0.61 | 0.28 | 30 | 16 | 41.9 |
| S12 | CI622 | 0.82 | 0.62 | 0.28 | 44 | 17 | 47.9 |
| S13 | CI632 | 0.47 | 0.11 | 0.11 | 78 | 14 | 47.0 |
| S14 | CI632 | 0.43 | 0.02 | 0.03 | 67 | 15 | 45.9 |
| S15 | CI632 | 0.66 | 0.03 | 0.04 | 59 | 10 | 45.9 |
| S16 | CI632 | 0.57 | 0.06 | 0.03 | 93 | 16 | 44.5 |
| S17 | CI632 | 0.56 | 0.05 | 0.06 | 78 | 18 | 48.0 |
| S18 | CI632 | 0.66 | 0.06 | 0.03 | 71 | 24 | 45.7 |
| S19 | CI632 | 0.62 | 0.11 | 0.10 | 85 | 12 | 44.5 |
| S20 | CI632 | 0.60 | 0.10 | 0.09 | 72 | 1 | 48.7 |
| S21 | CI632 | 0.58 | 0.07 | 0.04 | 81 | 8 | 45.5 |
| S22 | CI632 | 0.56 | 0.07 | 0.05 | 74 | 22 | 44.8 |
| S23 | CI632 | 0.51 | 0.03 | 0.03 | 68 | 7 | 45.4 |
| S24 | CI632 | 0.48 | 0.05 | 0.04 | 64 | 10 | 44.3 |
| CI622 | Mean | 0.8517 | 0.6125 | 0.2825 | 46.83 | 25.08 | 44.82 |
| Std. Dev. | 0.0546 | 0.0106 | 0.0062 | 17.6318 | 6.2879 | 1.7121 | |
| CI632 | Mean | 0.5583 | 0.0633 | 0.0542 | 74.16 | 13.0833 | 45.85 |
| Std. Dev. | 0.0736 | 0.0306 | 0.0294 | 9.466 | 6.5012 | 1.4003 | |
| Anova Test | p | 1.77−10 | 1.06−25 | 3.93−18 | 0.0001 | 0.0001 | 0.1227 |
| F | 123.01 | 2464.17 | 693.98 | 22.39 | 21.12 | 2.58 | |
| Degrees of freedom | 1 | 1 | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-de-Miguel, A.; Falcón-González, J.C.; Ramos-Macias, A. Analysis of Neural Interface When Using Modiolar Electrode Stimulation. Radiological Evaluation, Trans-Impedance Matrix Analysis and Effect on Listening Effort in Cochlear Implantation. J. Clin. Med. 2021, 10, 3962. https://doi.org/10.3390/jcm10173962
Ramos-de-Miguel A, Falcón-González JC, Ramos-Macias A. Analysis of Neural Interface When Using Modiolar Electrode Stimulation. Radiological Evaluation, Trans-Impedance Matrix Analysis and Effect on Listening Effort in Cochlear Implantation. Journal of Clinical Medicine. 2021; 10(17):3962. https://doi.org/10.3390/jcm10173962
Chicago/Turabian StyleRamos-de-Miguel, Angel, Juan Carlos Falcón-González, and Angel Ramos-Macias. 2021. "Analysis of Neural Interface When Using Modiolar Electrode Stimulation. Radiological Evaluation, Trans-Impedance Matrix Analysis and Effect on Listening Effort in Cochlear Implantation" Journal of Clinical Medicine 10, no. 17: 3962. https://doi.org/10.3390/jcm10173962
APA StyleRamos-de-Miguel, A., Falcón-González, J. C., & Ramos-Macias, A. (2021). Analysis of Neural Interface When Using Modiolar Electrode Stimulation. Radiological Evaluation, Trans-Impedance Matrix Analysis and Effect on Listening Effort in Cochlear Implantation. Journal of Clinical Medicine, 10(17), 3962. https://doi.org/10.3390/jcm10173962