
Classification and Assessment of Medication Risk in the Elderly (CARE): Use of a Medication Risk Score to Inform Patients’ Readmission Likelihood after Hospital Discharge



 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Measurements
2.4. Outcomes
2.5. Statistical Analysis
3. Results
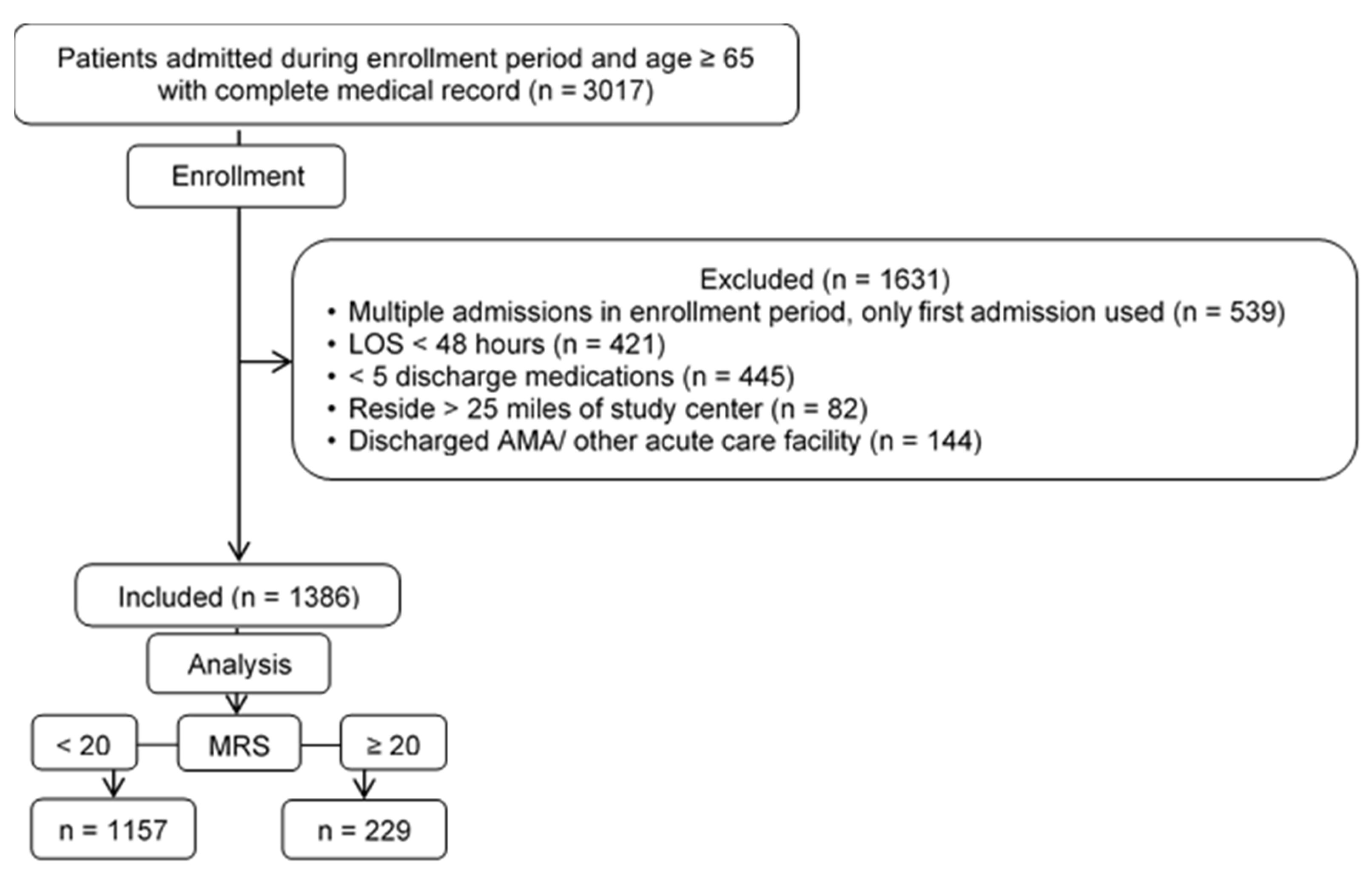
3.1. Patient Selection and Demographics
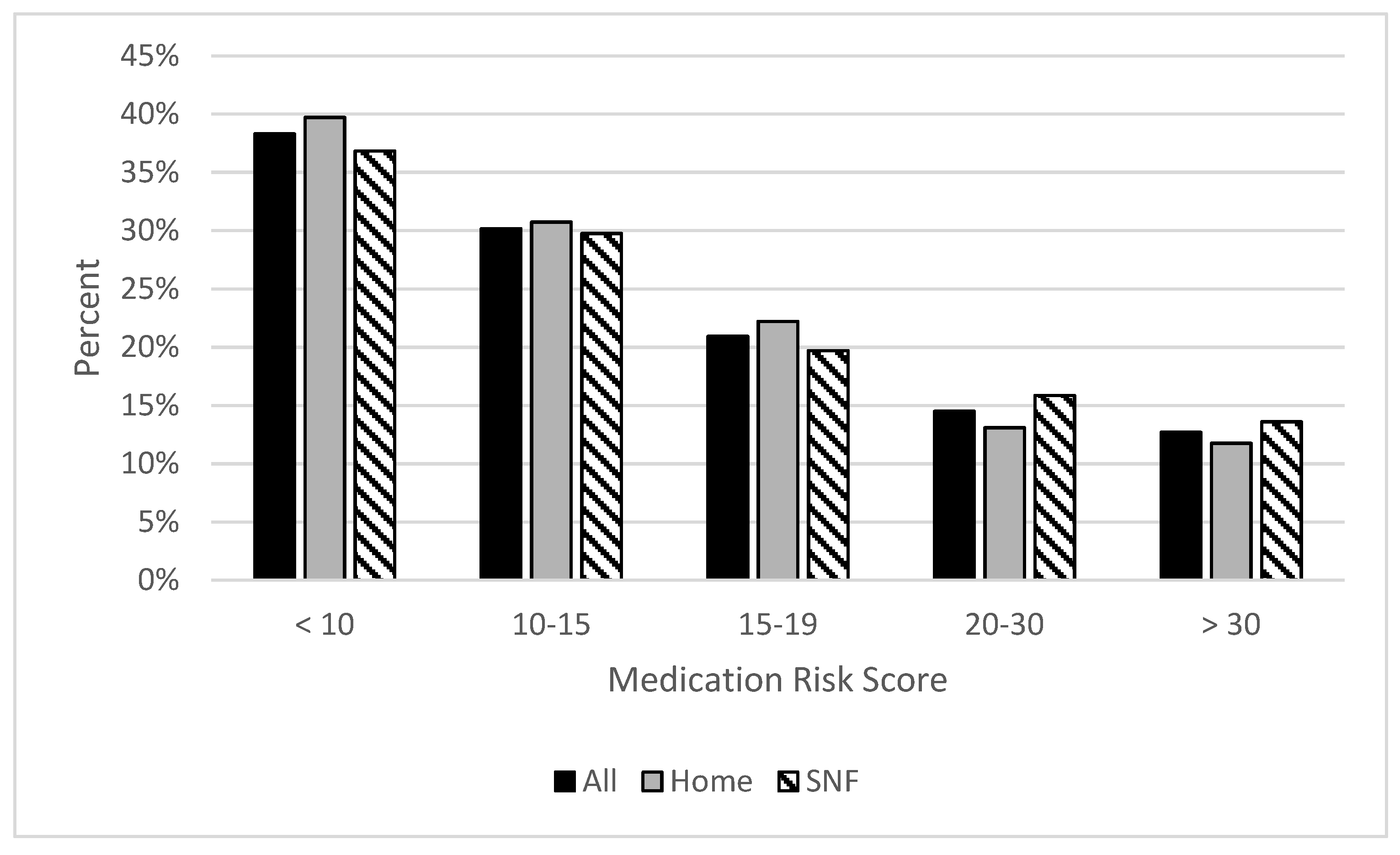
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Healthcare Cost and Utilization Project Facts and Figures 2008: Statistics on Hospital-Based Care in the United States 2008. Available online: http://www.hcup-us.ahrq.gov/reports/factsandfigures/2008/section1_TOC.jsp (accessed on 15 February 2021).
- Medicare Compare. Available online: https://www.medicare.gov/care-compare/ (accessed on 15 February 2021).
- Lum, H.D.; Studenski, S.A.; Degenholtz, H.B.; Hardy, S.E. Early hospital readmission is a predictor of one-year mortality in community-dwelling older Medicare beneficiaries. J. Gen. Intern. Med. 2012, 27, 1467–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oscanoa, T.J.; Lizaraso, F.; Carvajal, A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur. J. Clin. Pharmacol. 2017, 73, 759–770. [Google Scholar] [CrossRef]
- Parameswaran, N.N.; Chalmers, L.; Connolly, M.; Bereznicki, B.J.; Peterson, G.M.; Curtain, C.; Castelino, R.L.; Bereznicki, L.R. Prediction of Hospitalization due to Adverse Drug Reactions in Elderly Community-Dwelling Patients (The PADR-EC Score). PLoS ONE 2016, 11, e0165757. [Google Scholar] [CrossRef] [Green Version]
- Tangiisuran, B.; Scutt, G.; Stevenson, J.; Wright, J.; Onder, G.; Petrovic, M.; Davies, G. Development and validation of a risk model for predicting adverse drug reactions in older people during hospital stay: Brighton Adverse Drug Reactions Risk (BADRI) model. PLoS ONE 2014, 9, e111254. [Google Scholar] [CrossRef] [Green Version]
- Onder, G.; Petrovic, M.; Tangiisuran, B.; Meinardi, M.C.; Markito-Notenboom, W.P.; Somers, A.; van der Cammen, T.J. Development and validation of a score to assess risk of adverse drug reactions among in-hospital patients 65 years or older: The GerontoNet ADR risk score. Arch. Intern. Med. 2010, 170, 1142–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehrt, U.; Broich, K.; Larsen, J.P.; Ballard, C.; Aarsland, D. Use of drugs with anticholinergic effect and impact on cognition in Parkinson’s disease: A cohort study. J. Neurol. Neurosurg. Psychiatry 2010, 81, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Ancelin, M.L.; Artero, S.; Portet, F.; Dupuy, A.M.; Touchon, J.; Ritchie, K. Non-degenerative mild cognitive impairment in elderly people and use of anticholinergic drugs: Longitudinal cohort study. BMJ 2006, 332, 455–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Pollock, B.G.; Culp, K.R. The Anticholinergic Drug Scale as a measure of drug-related anticholinergic burden: Associations with serum anticholinergic activity. J. Clin. Pharmacol. 2006, 46, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Soto, R.; Yaldou, B. The Michigan Opioid Safety Score (MOSS): A Patient Safety and Nurse Empowerment Tool. J. Perianesth. Nurs. 2015, 30, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Webster, L.R.; Webster, R.M. Predicting aberrant behaviors in opioid-treated patients: Preliminary validation of the Opioid Risk Tool. Pain Med. 2005, 6, 432–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicali, B.M.V.; Knowlton, C.H.; Turgeon, J. Application of a novel medication-related risk stratification strategy to a self-funded employer population. Benefits Q. 2018, 2, 49–55. [Google Scholar]
- Turgeon, J.; Michaud, V.; Stephen, L.E.; Badea, G. Treatment Methods Having Reduced Drug-Related Toxicity and Methods of Identifying the Likelihood of Patient Harm from Prescribed Medications. U.S. Patent WO2017213825, 14 December 2017. [Google Scholar]
- Turgeon, J.; Michaud, V.; Cicali, B. Population-Based Medication Risk Stratification and Personalized Medication Risk Score. U.S. Patent WO2019089725, 9 May 2019. [Google Scholar]
- Ratigan, A.R.; Michaud, V.; Turgeon, J.; Bikmetov, R.; Gaona, V.G.; Anderson, H.D.; Pulver, G.; Pace, W.D. Longitudinal Association of a Medication Risk Score With Mortality Among Ambulatory Patients Acquired Through Electronic Health Record Data. J. Patient Saf. 2021, 17, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Bankes, D.L.; Jin, H.; Finnel, S.; Michaud, V.; Knowlton, C.H.; Turgeon, J.; Stein, A. Association of a Novel Medication Risk Score with Adverse Drug Events and Other Pertinent Outcomes Among Participants of the Programs of All-Inclusive Care for the Elderly. Pharmacy 2020, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Holman, C.D.; Preen, D.B.; Brameld, K. Repeat adverse drug reactions causing hospitalization in older Australians: A population-based longitudinal study 1980–2003. Br. J. Clin. Pharmacol. 2007, 63, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requirements for Long Term Care Facilities, 483.45 Pharmacy Services. Available online: https://www.law.cornell.edu/cfr/text/42/483.45 (accessed on 10 July 2021).
- Davies, E.C.G.; Mottram, D.R.; Howe, P.H.; Pirmohamed, M. Emergency re-admissions to hospital due to adverse drug reactions within 1 year of the index admission. Br. J. Clin. Pharmacol. 2010, 70, 749–755. [Google Scholar] [CrossRef] [Green Version]
- Requirements for Long Term Care Facilities, 483.21 Comprehensive Person-Centered Care Planning. Available online: https://www.law.cornell.edu/cfr/text/42/483.21 (accessed on 10 July 2021).
- El Morabet, N.; Uitvlugt, E.B.; van den Bemt, B.J.F.; van den Bemt, P.; Janssen, M.J.A.; Karapinar-Carkit, F. Prevalence and Preventability of Drug-Related Hospital Readmissions: A Systematic Review. J. Am. Geriatr. Soc. 2018, 66, 602–608. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Characteristic No. (%) | Overall | Subgroups | |||
|---|---|---|---|---|---|
| All Patients (n = 1386) | Discharged to Home (n = 680) | Discharged to Facility (n = 706) | p | ||
| Age *, years | 65–74 | 358 (26) | 239 (35) | 119 (17) | <0.001 |
| ≥75 | 783 (74) | 441 (65) | 587 (83) | <0.001 | |
| Mean (SD) | 80 (7) | 78 (7) | 82 (7) | <0.001 | |
| Sex | Female | 784 (57) | 362 (53) | 422 (60) | 0.009 |
| Race | White | 1168 (84) | 552 (81) | 616 (88) | <0.001 |
| Black | 93 (7) | 51 (8) | 42 (6) | 0.144 | |
| Asian/Indian | 84 (6) | 53 (8) | 31 (4) | 0.002 | |
| Other | 41 (3) | 24 (4) | 40 (2) | 0.027 | |
| Ethnicity | Hispanic | 80 (6) | 40 (6) | 40 (6) | >0.99 |
| BMI | kg/m2, mean (SD) | 27.9 (7) | 28.6 (7) | 27 (7) | >0.99 |
| Charlson Comorbidity Index | ≥4 | 887 (64) | 382 (56) | 505 (72) | <0.001 |
| Length of Stay | Days, mean (SD) | 6 (4) | 4 (3) | 7 (5) | <0.001 |
| Number of Medications | Mean (SD) | 11 (5) | 10 (5) | 12 (5) | <0.001 |
| Comorbidities | Heart Failure | 454 (33) | 209 (31) | 245 (35) | 0.114 |
| Diabetes Mellitus | 449 (32) | 224 (33) | 225 (32) | 0.691 | |
| COPD | 310 (22) | 145 (21) | 165 (23) | 0.369 | |
| Dementia | 203 (15) | 46 (7) | 157 (22) | <0.001 | |
| Myocardial Infarction | 142 (10) | 75 (11) | 67 (9) | 0.214 | |
| Readmission Within 30 Days | Readmission | 194 (1) | 85 (13) | 109 (15) | 0.284 |
| Time to Readmission, mean (SD), days | 13.9 (7) | 13 (9) | 14 (9) | 0.039 | |
| By comorbidity: ** | |||||
| Heart Failure | 75 (39) | 30 (35) | 45 (41) | 0.394 | |
| Diabetes Mellitus | 70 (36) | 33 (39) | 37 (34) | 0.472 | |
| COPD | 60 (31) | 26 (31) | 34 (31) | >0.99 | |
| Dementia | 24 (12) | 4 (5) | 20 (18) | 0.006 | |
| Myocardial Infarction | 27 (14) | 12 (14) | 15 (14) | >0.99 | |
| Characteristic, No. (%) | All Patients (n = 1386) | Discharged to Home (n = 680) | Discharged to Facility (n = 706) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| MRS < 20 (n = 1157) | MRS ≥ 20 (n = 229) | p | MRS < 20 (n = 582) | MRS ≥ 20 (n = 98) | p | MRS < 20 (n = 575) | MRS ≥ 20 (n = 131) | p | ||
| Sex | Female | 637 (55) | 147 (64) | 0.011 | 297 (51) | 65 (66) | 0.006 | 340 (59) | 82 (63) | 0.528 |
| Age * | Years, mean (SD) | 80 (7) | 80 (7) | 1 | 78 (7) | 79 (7) | 0.430 | 82 (6.8) | 81 (7) | 0.148 |
| BMI | kg/m2, mean (SD), | 27.7 (7) | 28.9 (7) | 0.018 | 28.5 (7) | 29.4 (7) | 0.239 | 26.8 (7) | 28.6 (8) | 0.021 |
| CCI | >4 | 718 (62) | 169 (74) | <0.001 | 317 (54) | 65 (66) | 0.027 | 401 (70) | 104 (80) | 0.032 |
| Length of Stay | Days, mean (SD) | 6 (5) | 7 (5) | 0.312 | 4 (3) | 5 (3) | 0.013 | 7 (5) | 8 (5) | 0.218 |
| Number of Medications | 5–6 | 247 (21) | 2 (0.9) | <0.001 | 149 (26) | 2 (2) | <0.001 | 98 (17) | 0 (0) | <0.001 |
| 7–14 | 750 (65) | 71 (31) | <0.001 | 415 (61) | 35 (36) | 0.090 | 370 (64) | 36 (27) | <0.001 | |
| ≥15 | 160 (14) | 156 (68) | <0.001 | 53 (9) | 61 (62) | <0.001 | 107 (19) | 95 (73) | <0.001 | |
| Mean (SD) | 10 (14) | 17 (6) | <0.001 | 9 (4) | 17 (6) | <0.001 | 11 (4) | 18 (6) | <0.001 | |
| Comorbidities | Heart Failure | 368 (32) | 86 (38) | 0.078 | 169 (29) | 40 (41) | 0.017 | 199 (35) | 46 (35) | >0.99 |
| Diabetes Mellitus | 372 (32) | 77 (34) | 0.554 | 190 (33) | 34 (35) | 0.698 | 182 (32) | 43 (33) | 0.825 | |
| COPD | 248 (21) | 62 (27) | 0.045 | 117 (20) | 28 (29) | 0.044 | 131 (23) | 34 (26) | 0.465 | |
| Dementia | 156 (13) | 47 (21) | 0.002 | 34 (6) | 12 (12) | <0.001 | 122 (21) | 35 (27) | 0.135 | |
| Myocardial Infarction | 120 (10) | 22 (10) | >0.99 | 61 (10) | 14 (14) | 0.234 | 59 (10) | 8 (6) | 0.154 | |
| Readmission Within 30 days | Readmission | 158 (13) | 36 (16) | 0.412 | 66 (10) | 19 (19) | 0.009 | 92 (16) | 17 (13) | 0.424 |
| Time to Readmission, mean (SD), days | 14 (9) | 12 (10) | 0.221 | 14 (8) | 12 (9) | 0.17 | 14 (9) | 14 (10) | 0.387 | |
| By comorbidity: ** | ||||||||||
| Heart Failure | 64 (41) | 11 (31) | 0.267 | 23 (35) | 7 (37) | 0.872 | 41 (45) | 4 (24) | 0.107 | |
| Diabetes Mellitus | 56 (35) | 14 (39) | 0.651 | 25 (38) | 8 (42) | 0.753 | 31 (34) | 6 (35) | 0.936 | |
| COPD | 47 (30) | 13 (36) | 0.483 | 20 (30) | 6 (32) | 0.867 | 27 (29) | 7 (41) | 0.325 | |
| Dementia | 19 (12) | 5 (14) | 0.742 | 3 (5) | 1 (5) | >0.99 | 16 (17) | 4 (24) | 0.491 | |
| Myocardial Infarction | 23 (15) | 4 (11) | 0.536 | 9 (14) | 3 (16) | 0.827 | 14 (15) | 1 (6) | <0.001 | |
| Parameter | Univariate | Multivariable | |||
|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | ||
| All Patients | MRS ≥ 20 | 1.18 (0.8–1.75) | 0.411 | 1.06 (0.71–1.58) | 0.787 |
| Age | 1.00 (0.78–1.02) | 0.846 | |||
| Sex (male) | 0.87 (0.64–1.18) | 0.370 | |||
| BMI ≤ 24.9 | 1.52 (1.12–2.06) | 0.008 | |||
| Length of Stay | 1.07 (1.04–1.10) | <0.001 | 1.06 (1.03–1.09) | <0.001 | |
| CCI > 4 | 2.25 (1.57–3.23) | <0.001 | 2.14 (1.48–3.08) | 0.001 | |
| Heart Failure | 1.35 (0.99–1.85) | 0.059 | |||
| Diabetes | 1.21 (0.88–1.68) | 0.237 | |||
| CKD Stage 3 or Worse | 1.62 (1.18–2.22) | <0.001 | |||
| MELD 20+ | 2.14 (0.75–6.12) | 0.157 | |||
| Discharged Home | MRS ≥ 20 | 1.88 (1.07–3.30) | 0.028 | 1.81 (1.02–3.21) | 0.042 |
| Age | 1.01 (0.98–1.04) | 0.533 | |||
| Sex (male) | 1.23 (0.78–1.94) | 0.384 | |||
| BMI ≤ 24.9 | 1.65 (1.04–2.63) | 0.034 | 1.72 (1.07–2.75) | 0.024 | |
| Length of Stay | 1.01 (0.94–1.09) | 0.752 | |||
| CCI > 4 | 2.04 (1.24–3.33) | 0.005 | 1.99 (1.21–3.27) | 0.007 | |
| Heart Failure | 1.27 (0.79–2.05) | 0.331 | |||
| Diabetes | 1.34 (0.84–2.15) | 0.219 | |||
| CKD Stage 3 or Worse | 1.25 (0.76–2.06) | 0.377 | |||
| MELD 20+ | 1.33 (0.24–7.34) | 0.741 | |||
| Discharged to a Facility | MRS ≥ 20 | 0.78 (0.45–1.37) | 0.388 | 0.67 (0.38–1.19) | 0.171 |
| Age | 0.99 (0.96–1.02) | 0.372 | |||
| Sex (male) | 0.64 (0.42–0.96) | 0.032 | |||
| BMI ≤ 24.9 | 1.40 (0.93–2.10) | 0.111 | |||
| Length of Stay | 1.08 (1.04–1.12) | <0.001 | 1.08 (1.04–1.12) | <0.001 | |
| CCI > 4 | 2.41 (1.40–4.16) | 0.002 | 2.20 (1.24–3.90) | 0.007 | |
| Heart Failure | 1.40 (0.92–2.12) | 0.118 | |||
| Diabetes | 1.12 (0.73–1.72) | 0.613 | |||
| CKD Stage 3 or Worse | 1.91 (1.26–2.89) | 0.002 | 1.55 (1.01–2.40) | 0.047 | |
| MELD 20+ | 3.14 (0.80–12.4) | 0.102 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
SanFilippo, S.; Michaud, V.; Wei, J.; Bikmetov, R.; Turgeon, J.; Brunetti, L. Classification and Assessment of Medication Risk in the Elderly (CARE): Use of a Medication Risk Score to Inform Patients’ Readmission Likelihood after Hospital Discharge. J. Clin. Med. 2021, 10, 3947. https://doi.org/10.3390/jcm10173947
SanFilippo S, Michaud V, Wei J, Bikmetov R, Turgeon J, Brunetti L. Classification and Assessment of Medication Risk in the Elderly (CARE): Use of a Medication Risk Score to Inform Patients’ Readmission Likelihood after Hospital Discharge. Journal of Clinical Medicine. 2021; 10(17):3947. https://doi.org/10.3390/jcm10173947
Chicago/Turabian StyleSanFilippo, Savanna, Veronique Michaud, Juanqin Wei, Ravil Bikmetov, Jacques Turgeon, and Luigi Brunetti. 2021. "Classification and Assessment of Medication Risk in the Elderly (CARE): Use of a Medication Risk Score to Inform Patients’ Readmission Likelihood after Hospital Discharge" Journal of Clinical Medicine 10, no. 17: 3947. https://doi.org/10.3390/jcm10173947
APA StyleSanFilippo, S., Michaud, V., Wei, J., Bikmetov, R., Turgeon, J., & Brunetti, L. (2021). Classification and Assessment of Medication Risk in the Elderly (CARE): Use of a Medication Risk Score to Inform Patients’ Readmission Likelihood after Hospital Discharge. Journal of Clinical Medicine, 10(17), 3947. https://doi.org/10.3390/jcm10173947