
Detection of Periodontal Pathogens in Oral Samples and Cardiac Specimens in Patients Undergoing Aortic Valve Replacement: A Pilot Study

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
- The oral bacteria or their toxins dissemination from the oral cavity into the bloodstream circulation, as a consequence of a transient or prolonged bacteremia (direct injury);
- The inflammation markers and the innate immunity system reaction to the presence of oral microorganisms, which can cause indirectly heart tissue damages (indirect systemic effect).
2. Materials and Methods
2.1. Study Design and Inclusion Criteria
2.2. Patients’ Examination
- Personal data (sex, age, smoking);
- Health status and clinical history;
- Oral hygiene habits;
- Oral conditions, with the assessment of tooth loss and periodontal evaluation of soft tissues, to establish the presence of periodontal disease; eventual presence of oral ulcerations or neoplasms.
2.2.1. Periodontal Evaluation
- Probing Pocket Depth (PPD), recorded in mm as the distance between the gingival margin and the base of the periodontal pocket;
- Bleeding on Probing (BOP), recorded as 0 (no bleeding) or 1 (bleeding) after probing for PPD, and expressed in percentage (%) for all sites;
- Visible Plaque Index (VPI), recorded as 0 (no plaque) or 1 (plaque) after probing for PPD, and expressed in % for all sites;
- Clinical Attachment Loss (CAL), recorded in mm as the distance from the cementoenamel junction (CEJ) to the location of the probe tip.
2.2.2. Plaque Samples and Aortic Valve Specimens
2.3. Microbiological Analysis
2.4. Statistical Analysis
3. Results
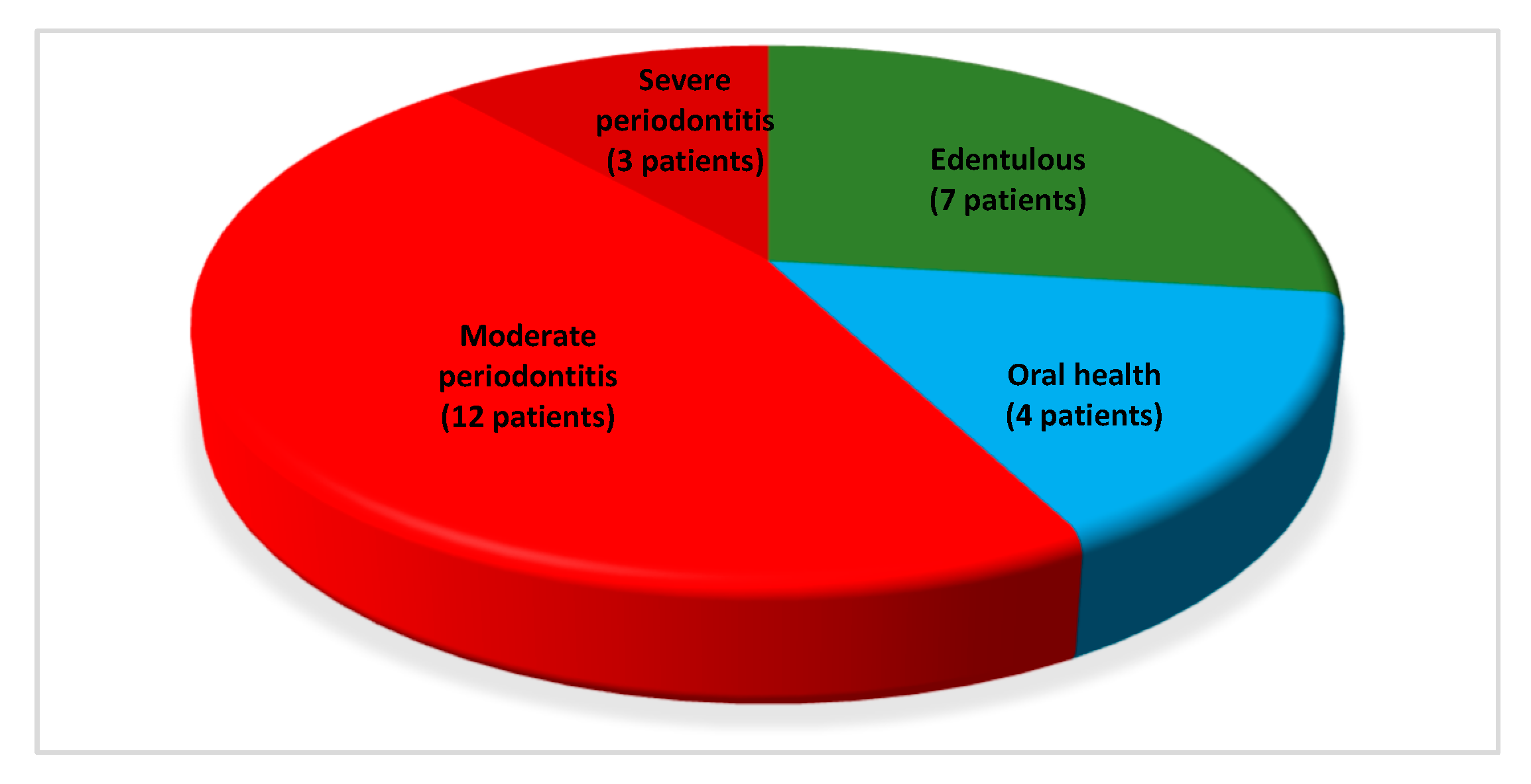
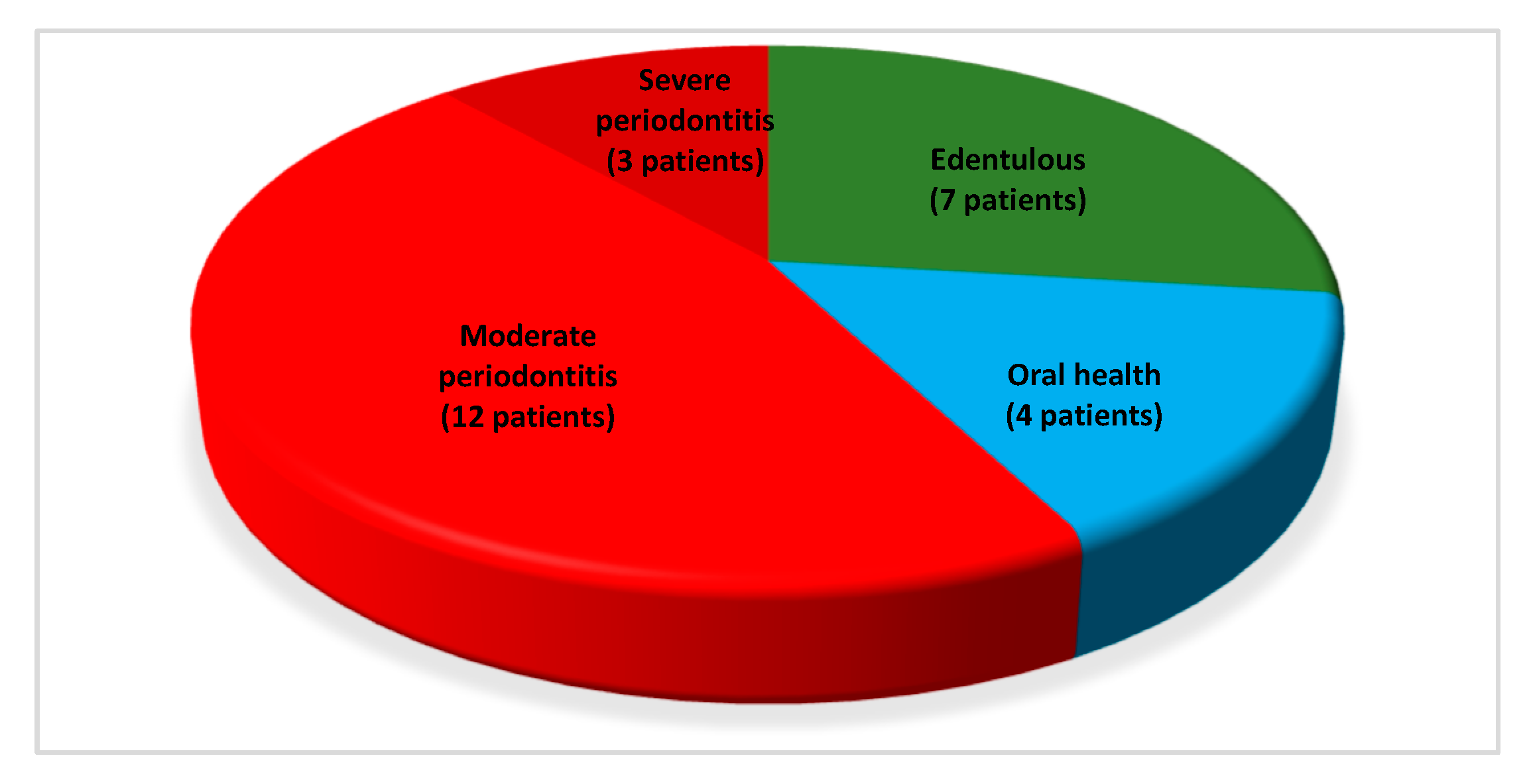
3.1. Overall Oral Conditions and Presence of Periodontal Disease
- Seven (26.92%) were edentulous and reported to had lost dentition for history of periodontal disease;
- Four dentate patients (15.39%) showed periodontally healthy conditions (oral health);
- Fifteen dentate patients (57.69%) showed periodontitis. Furthermore, the severity of active periodontal disease was registered, with 12 (46.15%) and 3 (11.54%) individuals presenting moderate and severe periodontitis, respectively.
3.2. Microbiological Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LPS | Lipopolysaccharide |
| AHA | American Heart Association |
| OPT | Orthopanoramic radiograph |
| PPD | Probing Pocket Depth |
| BOP | Bleeding on Probing |
| VPI | Visible Plaque Index |
| CAL | Clinical Attachment Loss |
| CEJ | Cementoenamel junction |
| PCR | Polymerase Chain Reaction |
| SD | Standard deviation |
| iqr | Interquartile range |
| ANOVA | One-way analysis of variance |
| P. gingivalis | Porphyromonas gingivalis |
| P. intermedia | Prevotella intermedia |
| T. denticola | Treponema denticola |
| T. forsythia | Tannerella forsythia |
| A. actinomycetemcomitans | Aggregatibacter actinomycetemcomitans |
| A. naeslundii | Actinomyces naeslundii |
| S. mutans | Streptococcus mutans |
| S. periodonticum | Streptococcus periodonticum |
| S. sinensis | Streptococcus sinensis |
| S. infantis | Streptoccoccus infantis |
| S. parasanguinis | Streptococcus parasanguinis |
| F. nucleatum | Fusobacterium nucleatum |
| F. periodonticum | Fusobacterium periodonticum |
| P. pasteri | Porphyromonas pasteri |
| A. segnis | Aggregatibacter segnis |
References
- Nakano, K.; Inaba, H.; Nomura, R.; Nemoto, H.; Takeda, M.; Yoshioka, H.; Matsue, H.; Takahashi, T.; Taniguchi, K.; Amano, A.; et al. Detection of cariogenic Streptococcus mutans in extirpated heart valve and atheromatous plaque specimens. J. Clin. Microbiol. 2006, 44, 3313–3317. [Google Scholar] [CrossRef] [Green Version]
- Nakano, K.; Nemoto, H.; Nomura, R.; Inaba, H.; Yoshioka, H.; Taniguchi, K.; Amano, A.; Ooshima, T. Detection of oral bacteria in cardiovascular specimens. Oral. Microbiol. Immunol. 2009, 24, 64–68. [Google Scholar] [CrossRef]
- Seymour, G.J.; Ford, P.J.; Cullinan, M.P.; Leishman, S.; Yamazaki, K. Relationship between periodontal infections and systemic disease. Clin. Microbiol. Infect. 2007, 13, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunwald, E. Valvular heart diseases. In Heart Disease. A Textbook of Cardiovascular Medicine, 6th ed.; Braunwald, E., Zipes, D.P., Libby, P., Eds.; WB Saunders: Philadelphia, PA, USA, 2001; pp. 1643–1722. [Google Scholar]
- Chalupova, M.; Skalova, A.; Hajek, T.; Geigerova, L.; Kralova, D.; Liska, P.; Hecova, H.; Molacek, J.; Hrabak, J. Bacterial DNA detected on pathologically changed heart valves using 16S rRNA gene amplification. Folia Microbiol. (Praha) 2018, 63, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev. 2000, 13, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, P.B.; Brennan, M.T.; Sasser, H.C.; Fox, P.C.; Paster, B.J.; Bahrani-Mougeot, F.K. Bacteremia associated with toothbrushing and dental extraction. Circulation 2008, 117, 3118–3125. [Google Scholar] [CrossRef] [Green Version]
- Lockhart, P.B.; Bolger, A.F.; Papapanou, P.N.; Osinbowale, O.; Trevisan, M.; Levison, M.E.; Taubert, K.A.; Newburger, J.W.; Gornik, H.L.; Gewitz, M.H.; et al. American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, Council on Epidemiology and Prevention, Council on Peripheral Vascular Disease, and Council on Clinical Cardiology. Periodontal disease and atherosclerotic vascular disease: Does the evidence support an independent association?: A scientific statement from the American Heart Association. Circulation 2012, 125, 2520–2544. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Jahn, C.; Pegel, J.; Semper-Pinnecke, E.; Mausberg, R.F.; Waldmann-Beushausen, R.; Schöndube, F.A.; Danner, B.C. Periodontal bacteria DNA findings in human cardiac tissue—Is there a link of periodontitis to heart valve disease? Int. J. Cardiol. 2018, 251, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, L.; Santangelo, R.; Falchetti, P.; Galluccio, F.; Luciani, N.; Anselmi, A.; Nowzari, H.; Verdugo, F.; Fadda, G.; D’Addona, A. Examination of periodontal pathogens in stenotic valve specimens and in whole blood samples in patients affected by aortic valve stenosis and chronic periodontitis. Int. J. Immunopathol. Pharmacol. 2010, 23, 561–566. [Google Scholar] [CrossRef]
- Damgaard, C.; Reinholdt, J.; Enevold, C.; Fiehn, N.E.; Nielsen, C.H.; Holmstrup, P. Immunoglobulin G antibodies against Porphyromonas gingivalis or Aggregatibacter actinomycetemcomitans in cardiovascular disease and periodontitis. J. Oral. Microbiol. 2017, 9, 1374154. [Google Scholar] [CrossRef] [Green Version]
- Boillot, A.; Demmer, R.T.; Mallat, Z.; Sacco, R.L.; Jacobs, D.R.; Benessiano, J.; Tedgui, A.; Rundek, T.; Papapanou, P.N.; Desvarieux, M. Periodontal microbiota and phospholipases: The Oral Infections and Vascular Disease Epidemiology Study (INVEST). Atherosclerosis 2015, 242, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Söder, P.O.; Söder, B.; Nowak, J.; Jogestrand, T. Early carotid atherosclerosis in subjects with periodontal diseases. Stroke 2005, 36, 1195–1200. [Google Scholar] [CrossRef] [Green Version]
- Atarbashi-Moghadam, F.; Havaei, S.R.; Havaei, S.A.; Hosseini, N.S.; Behdadmehr, G.; Atarbashi-Moghadam, S. Periopathogens in atherosclerotic plaques of patients with both cardiovascular disease and chronic periodontitis. ARYA Atheroscler. 2018, 14, 53–57. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. ACC/AHA Task Force Members. 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef]
- Lindhe, J.; Karring, T.; Lang, N.P. Clinical Periodontology and Implant Dentistry, 6th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2015; p. 1480. [Google Scholar]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Signoretto, C.; Marchi, A.; Bertoncelli, A.; Burlacchini, G.; Milli, A.; Tessarolo, F.; Caola, I.; Papetti, A.; Pruzzo, C.; Zaura, E.; et al. Effects of mushroom and chicory extracts on the shape, physiology and proteome of the cariogenic bacterium Streptococcus mutans. BMC Complement. Altern. Med. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- García, L.; Tercero, J.C.; Legido, B.; Ramos, J.A.; Alemany, J.; Sanz, M. Rapid detection of Actinobacillus actinomycetemcomitans, Prevotella intermedia and Porphyromonas gingivalis by multiplex PCR. J. Periodontal. Res. 1998, 33, 59–64. [Google Scholar] [CrossRef]
- Chun, Y.H.; Chun, K.R.; Olguin, D.; Wang, H.L. Biological foundation for periodontitis as a potential risk factor for atherosclerosis. J. Periodontal. Res. 2005, 40, 87–95. [Google Scholar] [CrossRef]
- Aimetti, M.; Romano, F.; Nessi, F. Microbiologic analysis of periodontal pockets and carotid atheromatous plaques in advanced chronic periodontitis patients. J. Periodontol. 2007, 78, 1718–1723. [Google Scholar] [CrossRef]
- Sfyroeras, G.S.; Roussas, N.; Saleptsis, V.G.; Argyriou, C.; Giannoukas, A.D. Association between periodontal disease and stroke. J. Vasc. Surg. 2012, 55, 1178–1184. [Google Scholar] [CrossRef] [Green Version]
- Mattila, K.J.; Asikainen, S.; Wolf, J.; Jousimies-Somer, H.; Valtonen, V.; Nieminen, M. Age, dental infections, and coronary heart disease. J. Dent. Res. 2000, 79, 756–760. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Mattila, K.J.; Nieminen, M.S.; Valtonen, V.V.; Rasi, V.P.; Kesäniemi, Y.A.; Syrjälä, S.L.; Jungell, P.S.; Isoluoma, M.; Hietaniemi, K.; Jokinen, M.J. Association between dental health and acute myocardial infarction. BMJ 1989, 298, 779–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoyama, N.; Kobayashi, N.; Hanatanii, T. Periodontal condition in Japanese coronary heart disease patients: A comparison between coronary and non-coronary heart disease. J. Periodont. Res. 2019, 54, 259–265. [Google Scholar] [CrossRef]
- Kumar, P.S. From focal sepsis to periodontal medicine: A century of exploring the role of the oral microbiome in systemic disease. J. Physiol. 2017, 595, 465–476. [Google Scholar] [CrossRef]
- Gaetti-Jardim, E.; Marcelino, S.L.; Feitosa, A.C.R.; Romito, G.A.; Avila-Campos, M.J. Quantitative detection of periodontopathic bacteria in atherosclerotic plaques from coronary arteries. J. Med. Microbiol. 2009, 58, 1568–1575. [Google Scholar] [CrossRef]
- Ishihara, K.; Nabuchi, A.; Ito, R.; Miyachi, K.; Kuramitsu, H.K.; Okuda, K. Correlation between detection rates of periodontopathic bacterial DNA in coronary stenotic artery plaque [corrected] and in dental plaque samples. J. Clin. Microbiol. 2004, 42, 1313–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahrani-Mougeot, F.K.; Paster, B.J.; Coleman, S.; Ashar, J.; Barbuto, S.; Lockhart, P.B. Diverse and novel oral bacterial species in blood following dental procedures. J. Clin. Microbiol. 2008, 46, 2129–2132. [Google Scholar] [CrossRef] [Green Version]
- Zaremba, M.; Górska, R.; Suwalski, P.; Kowalski, J. Evaluation of the incidence of periodontitis-associated bacteria in the atherosclerotic plaque of coronary blood vessels. J. Periodontol. 2007, 78, 322–327. [Google Scholar] [CrossRef]
- Pucar, A.; Milasin, J.; Lekovic, V.; Vukadinovic, M.; Ristic, M.; Putnik, S.; Kenney, E.B. Correlation between atherosclerosis and periodontal putative pathogenic bacterial infections in coronary and internal mammary arteries. J. Periodontol. 2007, 78, 677–682. [Google Scholar] [CrossRef]
- Szulc, M.; Kustrzycki, W.; Janczak, D.; Michalowska, D.; Baczynska, D.; Radwan-Oczko, M. Presence of periodontopathic bacteria DNA in atheromatous plaques from coronary and carotid arteries. Biomed. Res. Int. 2015, 2015, 825397. [Google Scholar] [CrossRef] [Green Version]
- Haraszthy, V.I.; Zambon, J.J.; Trevisan, M.; Zeid, M.; Genco, R.J. Identification of periodontal pathogens in atheromatous plaques. J. Periodontol. 2000, 71, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Sánchez-Beltrán, M.; Cuesta-Frechoso, S.; Tejerina, J.M.; del Castro, J.A.; Gutiérrez, J.M.; Herrera, D.; Sanz, M. Detection of periodontal bacteria in atheromatous plaque by nested polymerase chain reaction. J. Periodontol. 2011, 82, 1469–1477. [Google Scholar] [CrossRef] [Green Version]
- Pussinen, P.J.; Mattila, K. Periodontal infections and atherosclerosis: Mere associations? Curr. Opin. Lipidol. 2004, 15, 583–588. [Google Scholar] [CrossRef]
- Li, L.; Messas, E.; Batista, E.L., Jr.; Levine, R.A.; Amar, S. Porphyromonas gingivalis infection accelerates the progression of atherosclerosis in a heterozygous apolipoprotein E-deficient murine model. Circulation 2002, 105, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Schenkein, H.A.; Loos, B.G. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J. Periodontol. 2013, 40, S51–S69. [Google Scholar] [CrossRef]
- Cairo, F.; Gaeta, C.; Dorigo, W.; Oggioni, M.R.; Pratesi, C.; Pini Prato, G.P.; Pozzi, G. Periodontal pathogens in atheromatous plaques. A controlled clinical and laboratory trial. J. Periodontal. Res. 2004, 39, 442–446. [Google Scholar] [CrossRef]
- Romano, F.; Barbui, A.; Aimetti, M. Periodontal pathogens in periodontal pockets and in carotid atheromatous plaques. Minerva Stomatol. 2007, 56, 169–179. [Google Scholar]
- Moreno, S.; Parra, B.; Botero, J.E.; Moreno, F.; Vásquez, D.; Fernández, H.; Alba, S.; Gallego, S.; Castillo, G.; Contreras, A. Periodontal microbiota and microorganisms isolated from heart valves in patients undergoing valve replacement surgery in a clinic in Cali, Colombia. Biomedica 2017, 37, 516–525. [Google Scholar] [CrossRef] [Green Version]
- Kinane, D.F.; Riggio, M.P.; Walker, K.F.; MacKenzie, D.; Shearer, B. Bacteraemia following periodontal procedures. J. Clin. Periodontol. 2005, 32, 708–713. [Google Scholar] [CrossRef]
- Folwaczny, M.; Wilberg, S.; Bumm, C.; Hollatz, S.; Oberhoffer, R.; Neidenbach, R.C.; Kaemmerer, H.; Frasheri, I. Oral Health in Adults with Congenital Heart Disease. J. Clin. Med. 2019, 8, 1255. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.M.; Tsai, P.H.; Ye, Z.S.; Huang, Y.W.; Shieh, H.R.; Wu, C.H.; Lin, Y.J.; Miller, J.H.; Abranches, J.; Chiu, C.H. Functional analysis of the collagen binding proteins of Streptococcus parasanguinis FW213. mSphere 2020, 5, e00863-20. [Google Scholar] [CrossRef] [PubMed]
- Goret, J.; Baudinet, T.; Camou, F.; Issa, N.; Gaillard, P.; Wirth, G.; Greib, C.; Barandon, L.; Mégraud, F.; Bébéar, C.; et al. Identification of Streptococcus sinensis from a patient with endocarditis using MALDI-TOF mass spectrometry, 16S rDNA- and sodA-based phylogeny. J. Microbiol. Immunol. Infect. 2019, 52, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Hirunagi, T.; Kawanishi, H.; Mitsuma, N.; Goto, Y.; Mano, K. Aggregatibacter segnis endocarditis mimicking antineutrophil cytoplasmic antibody-associated vasculitis presenting with cerebral hemorrhage: A case report. Rinsho Shinkeigaku 2015, 55, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.K.; Park, S.N.; Shin, J.H.; Chang, Y.H.; Shin, Y.; Paek, J.; Kim, H.; Kook, J.K. Streptococcus periodonticum sp. nov., isolated from human subgingival dental plaque of periodontitis lesion. Curr. Microbiol. 2019, 76, 835–841. [Google Scholar] [CrossRef]
- Bolstad, A.I.; Jensen, H.B.; Bakken, V. Taxonomy, biology, and periodontal aspects of Fusobacterium nucleatum. Clin. Microbiol. Rev. 1996, 98, 55–71. [Google Scholar]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Souza, A.F.; Rocha, A.L.; Castro, W.H.; Gelape, C.L.; Nunes, M.C.P.; Oliveira, S.R.; Travassos, D.V.; Silva, T.A. Dental management for patients undergoing heart valve surgery. J. Card. Surg. 2017, 32, 627–632. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | n (%) |
|---|---|
| Sex | |
| male | 15 (57.69) |
| female | 11 (42.31) |
| Age | 72 ± 10 years |
| Smoking | |
| no | 24 (92.31) |
| yes (>25 cigarettes/day) | 2 (7.69) |
| Cardiovascular disease | |
| aortic valve regurgitation | 3 (11.54) |
| severe aortic stenosis | 17 (65.38) |
| severe aortic stenosis + coronopathy | 6 (23.08) |
| Previous endocarditis episodes | |
| no | 25 (96.15) |
| yes | 1 (3.85) |
| Antiplatelet therapy | |
| no | 12 (46.15) |
| yes | 14 (53.85) |
| Anticoagulant therapy | |
| no | 23 (88.46) |
| yes | 3 (11.54) |
| Type of oral examination | |
| edentulous patient | 7 (26.92) |
| tooth site | 19 (73.08) |
| Type of oral sample | |
| saliva (edentulous patient) | 6 (23.08) |
| plaque (tooth site) | 10 (38.46) |
| saliva + plaque (edentulous patient) | 10 (38.46) |
| Overall | Oral and Periodontal Conditions | |||||
|---|---|---|---|---|---|---|
| Oral Health n (%) | Moderate Periodontitis n (%) | Severe Periodontitis n (%) | Edentulousn (%) | p Value | ||
| Oral professional hygiene/year | ||||||
| not regular | 4 (15.39) | 0 (0.00) | 2 (16.67) | 0 (0.00) | 2 (28.57) | 0.62 |
| 1/year | 15 (57.69) | 3 (75.00) | 5 (41.67) | 3 (100.00) | 4 (57.14) | |
| 2/year | 7 (26.92) | 1 (25.00) | 5 (41.67) | 0 0.00) | 1 (14.29) | |
| Use of daily interproximal oral hygiene devices | ||||||
| no | 20 (76.92) | 3 (75.00) | 8 (66.67) | 2 (66.67) | 7 (100.00) | 0.34 |
| yes | 6 (23.08) | 1 (25.00) | 4 (33.33) | 1 (33.33) | 0 (0.00) | |
| Overall | Periodontal Conditions | ||||
|---|---|---|---|---|---|
| Oral Health | Moderate Periodontitis | Severe Periodontitis | p Value | ||
| PPD (mm) | 4.2 (0.5) | 4.2 (0.25) | 4.2 (0.2) | 4.6 (1.4) | 0.04 * |
| BOP (%) | 14 (12) | 4 (3) | 17 (11) | 20 (17) | 0.03 * |
| VPI (%) | 22 (43) | 33 (61) | 21 (52) | 56 (34) | 0.52 |
| CAL (mm) | 4.4 (0.6) | 4.4 (0.4) | 4.3 (0.4) | 5 (1) | 0.051 |
| Tooth loss | 12 (7) | 10 (3) | 11 (7) | 14 (10) | 0.77 |
| Oral Samples | Overall | Oral and Periodontal Conditions | ||||
|---|---|---|---|---|---|---|
| n (%) | Oral Health n (%) | Moderate Periodontitis n (%) | Severe Periodontitis n (%) | Edentulous n (%) | p Value | |
| P. gingivalis | ||||||
| no | 5 (19.23) | 1 (25.00) | 1 (8.33) | 0 (0.00) | 3 (42.86) | |
| yes | 21 (80.77) | 3 (75.00) | 11 (91.67) | 3 (100.00) | 4 (57.14) | 0.28 |
| P. intermedia | ||||||
| no | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| yes | 26 (100.00) | 4 (100.00) | 12 (100.00) | 3 (100.00) | 7 (100.00) | / |
| A. actinomycetemcomitans | ||||||
| no | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| yes | 26 (100.00) | 4 (100.00) | 12 (100.00) | 3 (100.00) | 7 (100.00) | / |
| T. denticola | ||||||
| no | 21 (80.77) | 3 (75.00) | 9 (75.00) | 2 (66.67) | 7 (100.00) | |
| yes | 5 (19.23) | 1 (25.00) | 3 (25.00) | 1 (33.33) | 0 (0.00) | 0.39 |
| A. naeslundii | ||||||
| no | 10 (38.46) | 1 (25.00) | 4 (33.33) | 0 (0.00) | 5 (71.43) | |
| yes | 16 (61.54) | 3 (75.00) | 8 (66.67) | 3 (100.00) | 2 (28.57) | 0.18 |
| S. mutans | ||||||
| no | 20 (76.92) | 2 (50.00) | 9 (75.00) | 3 (100.00) | 6 (85.71) | |
| yes | 6 (23.08) | 2 (50.00) | 3 (25.00) | 0 (0.00) | 1 (14.29) | 0.55 |
| T. forsythia | ||||||
| no | 9 (34.62) | 1 (25.00) | 3 (25.00) | 1 (33.33) | 4 (57.14) | |
| yes | 17 (65.38) | 3 (75.00) | 9 (75.00) | 2 (66.67) | 3 (42.86) | 0.59 |
| Valve Specimens | Overall | Oral and Periodontal Conditions | ||||
|---|---|---|---|---|---|---|
| n (%) | Oral Health n (%) | Moderate Periodontitis n (%) | Severe Periodontitis n (%) | Edentulous n (%) | p Value | |
| S. periodonticum | ||||||
| no | 22 (84.62) | 2 (50.00) | 11 (91.67) | 2 (66.67) | 7 (100.00) | |
| yes | 4 (15.38) | 2 (50.00) | 1 (8.33) | 1 (33.33) | 0 (0.00) | 0.09 |
| S. mutans | ||||||
| no | 23 (88.46) | 4 (100.00) | 9 (75.00) | 3 (100.00) | 7 (100.00) | |
| yes | 3 (11.54) | 0 (0.00) | 3 (25.00) | 0 (0.00) | 0 (0.00) | 0.39 |
| S. sinensis | ||||||
| no | 24 (92.31) | 4 (100.00) | 11 (91.67) | 2 (66.67) | 7 (100.00) | |
| yes | 2 (7.69) | 0 (0.00) | 1 (8.33) | 1 (33.33) | 0 (0.00) | 0.39 |
| S. infantis | ||||||
| no | 25 (96.15) | 3 (75.00) | 12 (100.00) | 3 (100.00) | 7 (100.00) | |
| yes | 1 (3.85) | 1 (25.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.26 |
| S. parasanguinis | ||||||
| no | 25 (96.15) | 4 (100.00) | 12 (100.00) | 2 (66.67) | 7 (100.00) | |
| yes | 1 (3.85) | 0 (0.00) | 0 (0.00) | 1 (33.33) | 0 (0.00) | 0.11 |
| F. nucleatum | ||||||
| no | 25 (96.15) | 4 (100.00) | 11 (91.67) | 3 (100.00) | 7 (100.00) | |
| yes | 1 (3.85) | 0 (0.00) | 1 (8.33) | 0 (0.00) | 0 (0.00) | 0.75 |
| F. periodonticum | ||||||
| no | 25 (96.15) | 4 (100.00) | 12 (100.00) | 2 (66.67) | 7 (100.00) | |
| yes | 1 (3.85) | 0 (0.00) | 0 (0.00) | 1 (33.33) | 0 (0.00) | 0.11 |
| P. pasteri | ||||||
| no | 25 (96.15) | 4 (100.00) | 12 (100.00) | 2 (66.67) | 7 (100.00) | |
| yes | 1 (3.85) | 0 (0.00) | 0 (0.00) | 1 (33.33) | 0 (0.00) | 0.11 |
| A. segnis | ||||||
| no | 25 (96.15) | 4 (100.00) | 11 (91.67) | 3 (100.00) | 7 (100.00) | |
| yes | 1 (3.85) | 0 (0.00) | 1 (8.33) | 0 (0.00) | 0 (0.00) | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardo, A.; Signoriello, A.; Signoretto, C.; Messina, E.; Carelli, M.; Tessari, M.; De Manna, N.D.; Rossetti, C.; Albanese, M.; Lombardo, G.; et al. Detection of Periodontal Pathogens in Oral Samples and Cardiac Specimens in Patients Undergoing Aortic Valve Replacement: A Pilot Study. J. Clin. Med. 2021, 10, 3874. https://doi.org/10.3390/jcm10173874
Pardo A, Signoriello A, Signoretto C, Messina E, Carelli M, Tessari M, De Manna ND, Rossetti C, Albanese M, Lombardo G, et al. Detection of Periodontal Pathogens in Oral Samples and Cardiac Specimens in Patients Undergoing Aortic Valve Replacement: A Pilot Study. Journal of Clinical Medicine. 2021; 10(17):3874. https://doi.org/10.3390/jcm10173874
Chicago/Turabian StylePardo, Alessia, Annarita Signoriello, Caterina Signoretto, Elena Messina, Maria Carelli, Maddalena Tessari, Nunzio Davide De Manna, Cecilia Rossetti, Massimo Albanese, Giorgio Lombardo, and et al. 2021. "Detection of Periodontal Pathogens in Oral Samples and Cardiac Specimens in Patients Undergoing Aortic Valve Replacement: A Pilot Study" Journal of Clinical Medicine 10, no. 17: 3874. https://doi.org/10.3390/jcm10173874
APA StylePardo, A., Signoriello, A., Signoretto, C., Messina, E., Carelli, M., Tessari, M., De Manna, N. D., Rossetti, C., Albanese, M., Lombardo, G., & Luciani, G. B. (2021). Detection of Periodontal Pathogens in Oral Samples and Cardiac Specimens in Patients Undergoing Aortic Valve Replacement: A Pilot Study. Journal of Clinical Medicine, 10(17), 3874. https://doi.org/10.3390/jcm10173874