
Poorer Exercise Accommodation of Regional Systolic Myocardial Motion after Spironolactone Treatment in Heart Failure Patients with Preserved Ejection Fraction and Ventricular Dyssynchrony

Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Follow-Up and Safety Monitoring
2.3. Echocardiography
2.4. Exercise Protocol
2.5. Quality of Life Evaluation
2.6. Laboratory Measurement
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparisons at Follow-Up
3.3. Comparisons of Systolic Motion at Baseline and Follow-Up
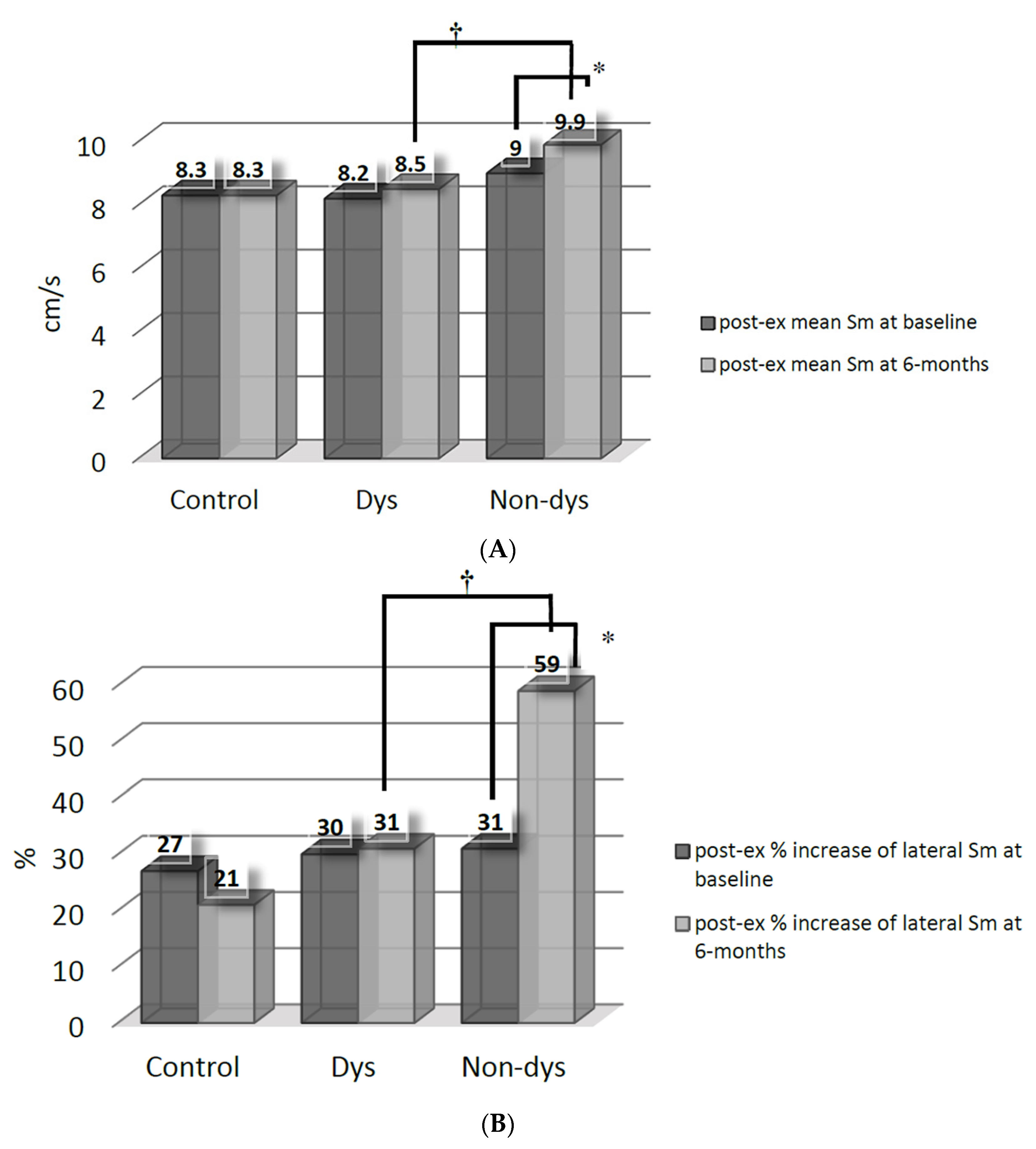
3.4. Impacts of Ventricular Dyssynchrony on Post-Exercise Accommodation of Systolic Myocardial Velocity after Spironolactone Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yip, G.; Wang, M.; Zhang, Y.; Fung, J.W.H.; Ho, P.Y.; Sanderson, J.E. Left ventricular long axis function in diastolic heart failure is reduced in both diastole and systole: Time for a redefinition? Heart 2002, 87, 121–125. [Google Scholar] [CrossRef]
- Petrie, M.C.; Caruana, L.; Berry, C.; McMurray, J.J.V. “Diastolic heart failure” or heart failure caused by subtle left ventricular systolic dysfunction? Heart 2002, 87, 29–31. [Google Scholar] [CrossRef][Green Version]
- Yu, C.M.; Lin, H.; Yang, H.; Kong, S.L.; Zhang, Q.; Lee, W.L. Progression of systolic abnormalities in patients with “isolated” diastolic heart failure and diastolic dysfunction. Circulation 2002, 105, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.T.; Wenzelburger, F.; Lee, E.; Heatlie, G.; Leyva, F.; Patel, K.; Frenneaux, M.; Sanderson, J.E. The pathophysiology of heart failure with normal ejection fraction: Exercise echocardiography reveals complex abnormalities of both systolic and diastolic ventricular function involving torsion, untwist, and longitudinal motion. J. Am. Coll. Cardiol. 2009, 54, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Deswal, A.; Richardson, P.; Bozkurt, B.; Mann, D.L. Results of the randomized aldosterone antagonism in heart failure with preserved ejection fraction trial (RAAM-PEF). J. Cardiac. Fail. 2011, 17, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Edelmann, F.; Wachter, R.; Schmidt, A.G.; Kraigher-Krainer, E.; Colantonio, C.; Kamke, W.; Duvinage, A.; Stahrenberg, R.; Durstewitz, K.; Löffler, M.; et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction. The Aldo-DHF randomized controlled trial. JAMA 2013, 309, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Yu, C.C.; Chiu, F.C.; Klepfer, R.; Hilpisch, K.; Splett, V.; Tsai, C.T.; Lai, L.P.; Hwang, J.J.; Lin, J.L. Impact of ventricular dyssynchrony on post-exercise accommodation of systolic myocardial motion in hypertensive patients with heart failure and a normal ejection fraction: A tissue-Doppler echocardiography study. J. Cardiac. Fail. 2012, 18, 134–139. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, J.M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation 2013, 128, 240–327. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s guidelines and standard committee and the chamber quantification writing group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar]
- Wang, Y.C.; Hwang, J.J.; Lai, L.P.; Tsai, C.T.; Lin, L.C.; Katra, R.; Lin, J.L. Coexistence and exercise exacerbation of intra-left ventricular contractile dyssynchrony in hypertensive patients with diastolic heart failure. Am. Heart J. 2007, 154, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.M.; Lin, H.; Zhang, Q.; Sanderson, J.E. High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS duration. Heart 2003, 89, 54–60. [Google Scholar] [CrossRef]
- Mottram, P.M.; Haluska, B.; Leano, R.; Cowley, D.; Stowasser, M.; Marwick, T.H. Effect of aldosterone antagonism on myocardial dysfunction in hypertensive patients with diastolic heart failure. Circulation 2004, 110, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.M.; Zhang, Q.; Yip, G.W.K.; Lee, P.W.; Kum, L.C.C.; Lam, Y.Y.; Fung, J.W. Diastolic and systolic asynchrony in patients with diastolic heart failure: A common but ignored condition. J. Am. Coll. Cardiol. 2007, 49, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Kurrelmeyer, K.M.; Torre-Amione, G.; Nagueh, S.F. Systolic and diastolic dyssynchrony in patients with diastolic heart failure and the effect of medical therapy. J. Am. Coll. Cardiol. 2007, 49, 88–96. [Google Scholar] [CrossRef] [PubMed]
- De Sutter, J.; Van de Veire, N.R.; Muyldermans, L.; De Backer, T.; Hoffer, E.; Vaerenberg, M.; Paelinck, B.; Decoodt, P.; Gabriel, L.; Gillebert, T.C.; et al. Prevalence of mechanical dyssynchrony in patients with heart failure and preserved left ventricular function (a report from the Belgian Multicenter Registry on dyssynchrony). Am. J. Cardiol. 2005, 96, 1543–1548. [Google Scholar] [CrossRef] [PubMed]
- Prestle, J.; Dieterich, S.; Preuss, M.; Bieligk, U.; Hasenfuss, G. Heterogeneous transmural gene expression of calcium-handling proteins and natriuretic peptides in the failing human heart. Cardiovasc. Res. 1999, 43, 323–331. [Google Scholar] [CrossRef][Green Version]
- Spragg, D.D.; Leclercq, C.; Loghmani, M.; Faris, O.P.; Tunin, R.S.; DiSilvestre, D.; McVeigh, E.R.; Tomaselli, G.F.; Kass, D.A. Regional alterations in protein expression in the dyssynchronous failing heart. Circulation 2003, 108, 929–932. [Google Scholar] [CrossRef]
- Labovitz, A.J.; Lewen, M.K.; Kern, M.; Vandormael, M.; Deligonal, U.; Kennedy, H.L. Evaluation of left ventricular systolic and diastolic dysfunction during transient myocardial ischemia produced by angioplasty. J. Am. Coll. Cardiol. 1987, 10, 748–755. [Google Scholar] [CrossRef]
- Reduto, L.A.; Wickemeyer, W.J.; Youngs, J.B.; Del Ventura, L.A.; Reid, J.W.; Glaeser, D.H.; Quinones, M.A.; Miller, R.R. Left ventricular diastolic performance at rest and during exercise in patients with coronary artery disease. Circulation 1981, 63, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone for heart failure with preserved ejection fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Lam, G.C.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; Redfield, M.M.; et al. Angiotensin–Neprilysin inhibition in heart failure with preserved ejection fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Redfield, M.M.; Jacobsen, S.J.; Burnett, J.C., Jr.; Mahoney, D.W.; Bailey, K.R.; Rodeheffer, R.J. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. JAMA 2003, 289, 194–202. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control (n = 24) | Spironolactone (n = 25) | p-Value | |
|---|---|---|---|
| Age (years) | 64 ± 12 | 66 ± 10 | 0.540 |
| Gender (male/female) | 10/14 | 14/11 | 0.326 |
| Body mass index (kg/m2) | 26.0 ± 3.2 | 26.0 ± 3.3 | 0.965 |
| Smoking (n) | 1 | 0 | 0.289 |
| Diabetes (n) | 6 | 4 | 0.445 |
| Hyperlipidemia (n) | 10 | 8 | 0.493 |
| CAD (n) | 3 | 5 | 0.488 |
| History of AF (n) | 3 | 6 | 0.431 |
| NYHA class II/III (n/n) | 16/8 | 14/11 | 0.454 |
| Aspirin (n) | 4 | 6 | 0.534 |
| CCB (n) | 16 | 21 | 0.165 |
| β-blocker (n) | 20 | 21 | 0.951 |
| ACEI/ARB (n) | 7 | 3 | 0.142 |
| Diuretics (n) | 14 | 15 | 0.908 |
| Digitalis (n) | 0 | 0 | |
| AAA (n) | 2 | 5 | 0.252 |
| Statins (n) | 5 | 6 | 0.796 |
| QRS duration (ms) | 88 ± 8 | 88 ± 8 | 0.982 |
| Control (n = 24) | Spironolactone (n = 25) | p-Value | ||
|---|---|---|---|---|
| Systolic BP (mmHg) | Baseline | 131 ± 6 | 131 ± 6 | 0.965 |
| 6 months | 131 ± 6 | 129 ± 5 | 0.191 | |
| Diastolic BP (mmHg) | Baseline | 77 ± 7 | 77 ± 5 | 0.980 |
| 6 months | 76 ± 6 | 77 ± 5 | 0.807 | |
| Potassium (mmol/L) | Baseline | 4.1 ± 0.3 | 4.3 ± 0.4 | 0.213 |
| 6 months | 4.3 ± 0.4 | 4.5 ± 0.4 * | 0.010 | |
| QOL score | Baseline | 27 ± 22 | 30 ± 20 | 0.623 |
| 6 months | 24 ± 22 | 22 ± 20 * | 0.818 | |
| NT-proBNP (pg/mL) | Baseline | 229 ± 281 | 337 ± 653 | 0.459 |
| 6 months | 182 ± 173 | 183 ± 213 | 0.994 | |
| LA diameter (mm) | Baseline | 37 ± 6 | 36 ± 5 | 0.498 |
| 6 months | 37 ± 5 | 36 ± 4 | 0.212 | |
| LAVI (ml/m2) | Baseline | 24.8 ± 9.2 | 23.1 ± 9.5 | 0.548 |
| 6 months | 22.9 ± 6.1 | 21.6 ± 6.1 | 0.472 | |
| IVS (mm) | Baseline | 11.3 ± 1.8 | 11.5 ± 1.9 | 0.682 |
| 6 months | 11.9 ± 1.7 | 11.9 ± 1.3 | 0.953 | |
| PW (mm) | Baseline | 11.4 ± 1.9 | 11.7 ± 1.9 | 0.564 |
| 6 months | 11.5 ± 1.4 | 11.1 ± 1.3 | 0.323 | |
| LVEDD (mm) | Baseline | 44.5 ± 5.0 | 46.6 ± 4.1 | 0.116 |
| 6 months | 43.9 ± 5.3 | 45.0 ± 4.5 | 0.445 | |
| LVESD (mm) | Baseline | 28.2 ± 4.6 | 29.7 ± 3.6 | 0.223 |
| 6 months | 28.0 ± 4.2 | 28.3 ± 3.8 | 0.776 | |
| RWT | Baseline | 0.52 ± 0.10 | 0.50 ± 0.08 | 0.519 |
| 6 months | 0.54 ± 0.07 | 0.52 ± 0.05 | 0.349 | |
| LVM/Ht2.7 (g/m2.7) | Baseline | 60.5 ± 17.5 | 65.9 ± 20.1 | 0.317 |
| 6 months | 62.9 ± 19.2 | 62.6 ± 14.2 | 0.944 | |
| LVEF (%) | Baseline | 67 ± 7 | 66 ± 6 | 0.542 |
| 6 months | 66 ± 5 | 67 ± 7 | 0.684 | |
| Mitral E/A | Baseline | 0.99 ± 0.23 | 1.02 ± 0.34 | 0.708 |
| 6 months | 0.95 ± 0.32 | 0.86 ± 0.23 * | 0.318 | |
| E flow DT (ms) | Baseline | 234 ± 50 | 214 ± 37 | 0.135 |
| 6 months | 230 ± 56 | 230 ± 53 | 0.958 | |
| IVRT (ms) | Baseline | 99 ± 21 | 100 ± 30 | 0.891 |
| 6 months | 92 ± 17 | 95 ± 20 | 0.629 | |
| Mitral Ea (cm/s) | Baseline | 7.7 ± 1.5 | 8.0 ± 2.2 | 0.583 |
| 6 months | 7.6 ± 2.4 | 9.0 ± 2.4 * | 0.063 | |
| Mitral E/Ea | Baseline | 9.7 ± 1.1 | 10.6 ± 2.7 | 0.158 |
| 6 months | 10.4 ± 3.5 | 8.7 ± 3.7 * | 0.096 |
| Control (n = 24) | Spironolactone (n = 25) | p-Value | ||
|---|---|---|---|---|
| HR (1/s) | 66 ± 13 | 68 ± 12 | 0.640 | 0.676 |
| 68 ± 14 | 72 ± 15 | 0.963 | 0.287 | |
| Post-exercise HR (1/s) | Baseline | 118 ± 16 | 115 ± 18 | 0.640 |
| 6 months | 122 ± 18 | 122 ± 20 | 0.963 | |
| Mean Sm (cm/s) | Baseline | 7.0 ± 0.9 | 7.1 ± 1.2 | 0.628 |
| 6 months | 7.1 ± 0.8 | 7.2 ± 1.3 | 0.627 | |
| Post-exercise mean Sm (cm/s) | Baseline | 8.3 ± 1.1 | 8.6 ± 1.5 | 0.410 |
| 6 months | 8.3 ± 1.0 | 9.2 ± 1.6 * | 0.021 | |
| Post-exercise % increase of septal Sm | Baseline | 33 ± 28 | 30 ± 32 | 0.757 |
| 6 months | 29 ± 20 | 29 ± 24 | 0.956 | |
| Post-exercise % increase of lateral Sm | Baseline | 27 ± 28 | 30 ± 19 | 0.568 |
| 6 months | 21 ± 21 | 44 ± 30 * | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.-C.; Chiu, F.-C.; Tsai, C.-T.; Wang, Y.-C.; Lai, L.-P.; Hwang, J.-J.; Lin, J.-L. Poorer Exercise Accommodation of Regional Systolic Myocardial Motion after Spironolactone Treatment in Heart Failure Patients with Preserved Ejection Fraction and Ventricular Dyssynchrony. J. Clin. Med. 2021, 10, 3827. https://doi.org/10.3390/jcm10173827
Yu C-C, Chiu F-C, Tsai C-T, Wang Y-C, Lai L-P, Hwang J-J, Lin J-L. Poorer Exercise Accommodation of Regional Systolic Myocardial Motion after Spironolactone Treatment in Heart Failure Patients with Preserved Ejection Fraction and Ventricular Dyssynchrony. Journal of Clinical Medicine. 2021; 10(17):3827. https://doi.org/10.3390/jcm10173827
Chicago/Turabian StyleYu, Chih-Chieh, Fu-Chun Chiu, Chia-Ti Tsai, Yi-Chih Wang, Ling-Ping Lai, Juey-Jen Hwang, and Jiunn-Lee Lin. 2021. "Poorer Exercise Accommodation of Regional Systolic Myocardial Motion after Spironolactone Treatment in Heart Failure Patients with Preserved Ejection Fraction and Ventricular Dyssynchrony" Journal of Clinical Medicine 10, no. 17: 3827. https://doi.org/10.3390/jcm10173827
APA StyleYu, C.-C., Chiu, F.-C., Tsai, C.-T., Wang, Y.-C., Lai, L.-P., Hwang, J.-J., & Lin, J.-L. (2021). Poorer Exercise Accommodation of Regional Systolic Myocardial Motion after Spironolactone Treatment in Heart Failure Patients with Preserved Ejection Fraction and Ventricular Dyssynchrony. Journal of Clinical Medicine, 10(17), 3827. https://doi.org/10.3390/jcm10173827