
First-Trimester Screening for Gestational Diabetes Mellitus in Twin Pregnancies

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measure
2.4. Statistical Analysis
3. Results
Study Population
4. Discussion
4.1. Main Findings
4.2. Interpretation of Findings and Comparison with Results of Previous Studies
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Casey, B.M.; Lucas, M.J.; Mclntire, D.D.; Leveno, K.J. Pregnancy Outcomes in Women with Gestational Diabetes Compared with the General Obstetric Population. Obstet. Gynecol. 1997, 90, 869–873. [Google Scholar] [CrossRef]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of treatment of gestational diabetes on pregnancy outcomes. Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clausen, T.D.; Mathiesen, E.; Hansen, T.; Pedersen, O.; Jensen, D.M.; Lauenborg, J.; Damm, P. High Prevalence of Type 2 Diabetes and Pre-Diabetes in Adult Offspring of Women With Gestational Diabetes Mellitus or Type 1 Diabetes: The role of intrauterine hyperglycemia. Diabetes Care 2007, 31, 340–346. [Google Scholar] [CrossRef] [Green Version]
- HAPO Study Cooperative Research Group; Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [PubMed] [Green Version]
- Feig, D.S.; Zinman, B.; Wang, X.; Hux, J.E. Risk of development of diabetes mellitus after diagnosis of gestational diabetes. CMAJ 2008, 179, 229–234. [Google Scholar] [CrossRef] [Green Version]
- Bellamy, L.; Casas, J.-P.; Hingorani, A.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.D.; Hod, M.; Kitzmiler, J.L.; et al. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- National Collaborating Centre for Women’s and Children’s Health. Diabetes in Pregnancy: Management of Diabetes and ITS Complications from Pre-Conception to the Postnatal Period. 2008. Available online: www.nice.org.uk/CG063fullguideline (accessed on 26 April 2021).
- Syngelaki, A.; Pastides, A.; Kotecha, R.; Wright, A.; Akolekar, R.; Nicolaides, K.H. First-Trimester Screening for Gestational Diabetes Mellitus Based on Maternal Characteristics and History. Fetal Diagn. Ther. 2014, 38, 14–21. [Google Scholar] [CrossRef]
- Litwinska, E.; Syngelaki, A.; Cimpoca, B.; Frei, L.; Nicolaides, K.H. Outcome of twin pregnancy with two live fetuses at 11–13 weeks’ gestation. Ultrasound Obstet. Gynecol. 2019, 55, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francisco, C.; Wright, D.; Benkő, Z.; Syngelaki, A.; Nicolaides, K. Hidden high rate of pre-eclampsia in twin compared with singleton pregnancy. Ultrasound Obstet. Gynecol. 2017, 50, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Benkő, Z.; Wright, A.; Rehal, A.; Cimpoca, B.; Syngelaki, A.; Delgado, J.L.; Tsokaki, T.; De Alvarado, M.; Vojtassakova, D.; Ntalianis, K.M.; et al. Prediction of pre-eclampsia in twin pregnancy by maternal factors and biomarkers at 11–13 weeks’ gestation: Data from EVENTS trial. Ultrasound Obstet. Gynecol. 2020, 57, 257–265. [Google Scholar] [CrossRef]
- Schwartz, D.B.; Daoud, Y.; Zazula, P.; Goyert, G.; Bronsteen, R.; Wright, D.; Copes, J. Gestational diabetes mellitus: Metabolic and blood glucose parameters in singleton versus twin pregnancies. Am. J. Obstet. Gynecol. 1999, 181, 912–914. [Google Scholar] [CrossRef]
- Rauh-Hain, J.A.; Rana, S.; Tamez, H.; Wang, A.; Cohen, B.; Cohen, A.; Brown, F.; Ecker, J.L.; Karumanchi, S.A.; Thadhani, R. Risk for developing gestational diabetes in women with twin pregnancies. J. Matern. Fetal Neonatal Med. 2009, 22, 293–299. [Google Scholar] [CrossRef]
- Weissman, A.; Drugan, A. Glucose tolerance in singleton, twin and triplet pregnancies. J. Perinat. Med. 2016, 44, 893–897. [Google Scholar] [CrossRef]
- Hiersch, L.; Berger, H.; Okby, R.; Ray, J.G.; Geary, M.; Mcdonald, S.D.; Murry-Davis, B.; Riddell, C.; Halperin, I.; Hasan, H.; et al. Incidence and risk factors for gestational diabetes mellitus in twin versus singleton pregnancies. Arch Gynecol Obstet. 2018, 29, 579–587. [Google Scholar] [CrossRef]
- Buhling, K.J.; Henrich, W.; Starr, E.; Lubke, M.; Bertram, S.; Siebert, G.; Dudenhausen, J.W. Risk for gestational diabetes and hypertension for women with twin pregnancy compared to singleton pregnancy. Arch. Gynecol. Obstet. 2003, 269, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, M.; Yamada, T.; Akaishi, R.; Kojima, T.; Nishida, R.; Koyama, T.; Cho, K.; Minakami, H. Prevalence of hyperglycaemia in singleton versus twin pregnancy. Diabetes Metab. Res. Rev. 2014, 31, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Robinson, H.P.; Fleming, J.E.E. A Critical Evaluation of Sonar Crown-Rump Length Measurements. Br. J. Obstet. Gynaecol. 1975, 82, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Syngelaki, A.; Cimpoca, B.; Litwinska, E.; Akolekar, R.; Nicolaides, K.H. Diagnosis of non-chromosomal fetal abnormalities in twin pregnancies at routine ultrasound examination at 11–13 weeks’ gestation. Ultrasound Obs. Gynecol. 2020, 55, 474–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snijders, R.; Noble, P.; Sebire, N.; Souka, A.; Nicolaides, K. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10–14 weeks of gestation. Fetal Medicine Foundation First Trimester Screening Group Lancet 1998, 352, 343–346. [Google Scholar] [CrossRef]
- Sepulveda, W.; Sebire, N.J.; Hughes, K.; Odibo, A.; Nicolaides, K. The lambda sign at 10-14 weeks of gestation as a predictor of chorionicity in twin pregnancies. Ultrasound Obstet. Gynecol. 1996, 7, 421–423. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Department of Noncommunicable Disease Surveillance: Definition, diagnosis and classification of diabetes mellitus and its complications. In Report of a WHO Consultation. Part 1. Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/ (accessed on 20 June 2021).
- Feng, B.; Zhai, J.; Cai, Y. Effect of twin pregnancy chorionic properties on maternal and fetal outcomes. Taiwan J. Obstet. Gynecol. 2018, 57, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Madsen, H.N.; Ball, S.; Wright, D.; Tørring, N.; Petersen, O.B.; Nicolaides, K.; Spencer, K. A reassessment of biochemical marker distributions in trisomy 21-affected and unaffected twin pregnancies in the first trimester. Ultrasound Obstet. Gynecol. 2010, 37, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Savvidou, M.D.; Syngelaki, A.; Muhaisen, M.; Emelyanenko, E.; Nicolaides, K.H. First trimester maternal serum free beta-human chorionic gonadotropin and pregnancy-associated plasma protein A in pregnancies complicated by diabetes mellitus. BJOG 2012, 119, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.Y.T.; Liao, A.W.; Spencer, K.; Munim, S.; Nicolaides, K. First trimester maternal serum free beta human chorionic gonadotrophin and pregnancy associated plasma protein A as predictors of pregnancy complications. BJOG 2000, 107, 1265–1270. [Google Scholar] [CrossRef]
- Syngelaki, A.; Kotecha, R.; Pastides, A.; Wright, A.; Nicolaides, K.H. First-trimester biochemical markers of placentation in screening for gestational diabetes mellitus. Metabolism 2015, 64, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Rodriguez, R.; Ziegler, R.; DeSouza, T.; Majid, S.; Madore, A.S.; Amir, N.; Pace, V.A.; Nachreiner, D.; Alfego, D.; Mathew, J.; et al. PAPPA-mediated adipose tissue remodeling mitigates insulin resistance and protects against gestational diabetes in mice and humans. Sci. Transl. Med. 2020, 12, eaay4145. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Singleton Pregnancies | Twin Pregnancies | ||||
|---|---|---|---|---|---|---|
| No GDM (n = 13,243) | GDM (n = 517) | p-Value | No GDM (n = 1286) | GDM (n = 90) | p-Value | |
| Maternal age (years) | 32.5 (28.7, 35.7) | 34.0 (30.5, 37.1) | <0.0001 | 34.25 (30.4, 37.4) | 35.5 (31.4, 38.8) | 0.068 |
| Maternal weight (kg) | 66.5 (59.4, 76.3) | 76.1 (65.0, 91.0) | <0.0001 | 68.8 (61.0, 79.0) | 75.0 (64.5, 90.9) | 0.0005 |
| Maternal height (cm) | 165 (161, 170) | 164 (159, 168) | <0.0001 | 166 (162, 170) | 164 (158, 169) | 0.003 |
| Body mass index (kg/m2) | 24.2 (21.8, 27.8) | 28.6 (24.3, 33.3) | <0.0001 | 24.6 (22.1, 28.2) | 28.0 (24.6, 33.3) | <0.0001 |
| Gestational age (weeks) | 12.7 (12.3, 13.1) | 12.7 (12.4, 13.1) | 0.015 | 12.7 (12.3, 13.1) | 12.9 (12.4, 13.1) | 0.329 |
| Racial origin | <0.0001 | 0.002 | ||||
| White | 9231 (69.7%) | 276 (53.4%) | 892 (69.4%) | 56 (62.2%) | ||
| Black | 2735 (20.7%) | 132 (25.5%) | 285 (22.2%) | 21 (23.3%) | ||
| South Asian | 550 (4.2%) | 58 (11.2%) | 40 (3.1%) | 10 (11.1%) | ||
| East Asian | 252 (1.9%) | 26 (5.0%) | 21 (1.6%) | 0 | ||
| Mixed | 475 (3.6%) | 25 (4.8%) | 48 (3.7%) | 3 (3.3%) | ||
| Family history of diabetes | <0.0001 | 0.018 | ||||
| 1st degree | 1525 (11.5%) | 121 (23.4%) | 167 (13.0%) | 19 (21.1%) | ||
| 2nd degree | 1231 (9.3%) | 56 (10.8%) | 141 (11%) | 16 (17.8%) | ||
| 3rd degree | 259 (2.0%) | 11 (2.1%) | 19 (1.5%) | 1 (1.1%) | ||
| Method of conception | 0.387 | 0.107 | ||||
| Natural | 12,611 (95.2%) | 486 (94.0%) | 886 (68.90%) | 53 (58.9%) | ||
| In-vitro fertilization | 530 (4.0%) | 25 (4.8%) | 379 (29.5%) | 36 (40.0%) | ||
| Ovulation drugs | 102 (0.8%) | 6 (1.2%) | 21 (1.6%) | 1 (1.1%) | ||
| Parity | <0.0001 | <0.0001 | ||||
| Nulliparous | 6532 (49.3%) | 210 (40.6%) | 678 (52.7%) | 46 (51.1%) | ||
| Parous, previous GDM | 105 (0.8%) | 82 (15.9%) | 9 (0.7%) | 8 (8.9%) | ||
| Parous, no previous GDM | 6606 (49.9%) | 225 (43.5%) | 599 (46.6%) | 36 (40.0%) | ||
| Birthweight of last neonate (g) | 3350 (3015, 3689) | 3433 (3036, 3860) | 0.024 | 3349 (3000, 3660) | 3405 (3178, 3750) | 0.195 |
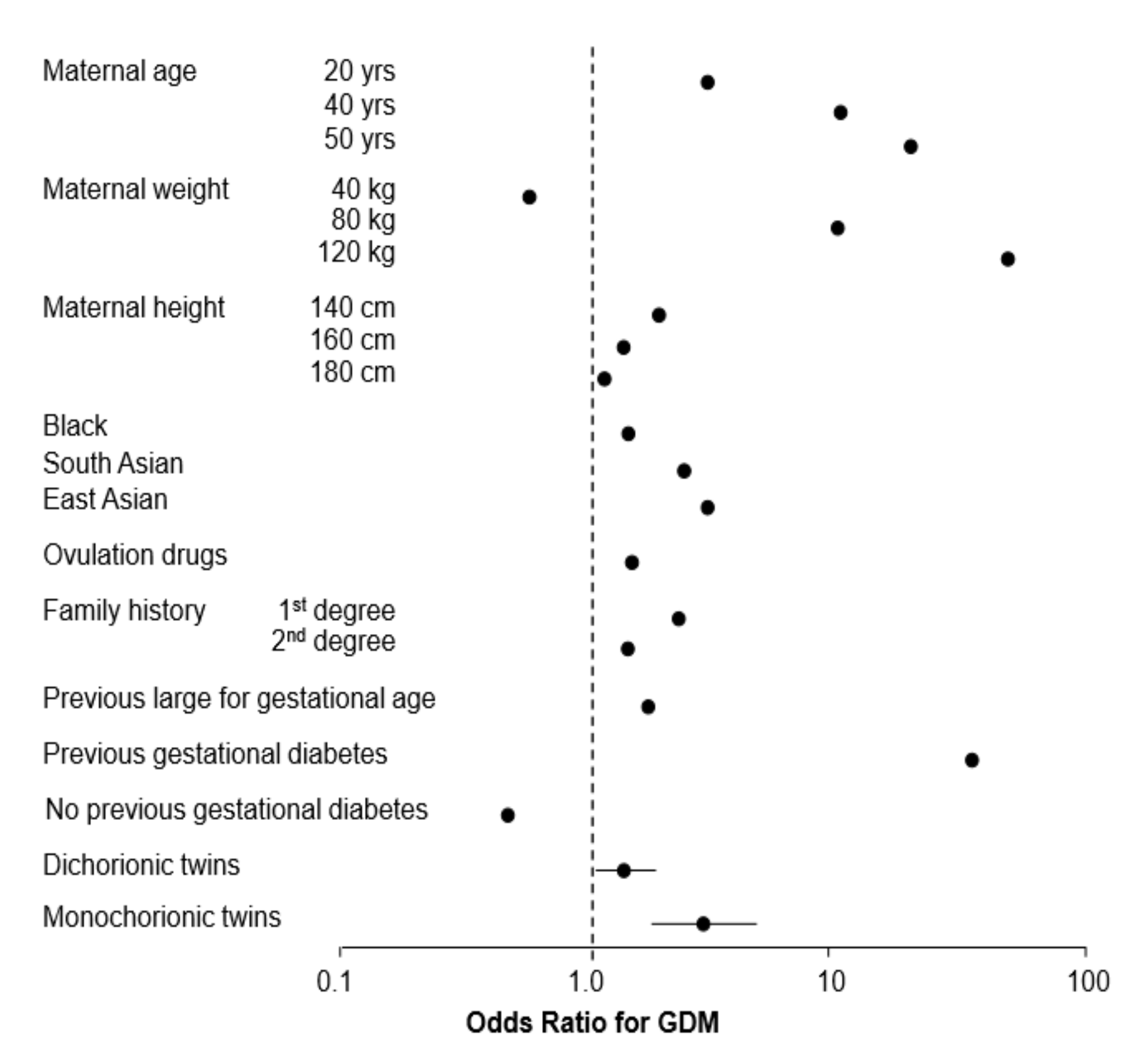
| Term | Odds Ratio (95% CI) | Coefficient | p-Value |
|---|---|---|---|
| Intercept | - | −3.53042 | <0.0001 |
| Twins: dischorionic | 1.3601 (1.0213–1.8115) | 0.30759 | 0.035 |
| Twins: monochorionic | 2.7771 (1.7205–4.4823) | 1.02139 | <0.0001 |
| Previous GDM | 50.44 | 3.92090 | |
| Weight in kg—69 | 1.0208 | 0.02060 | |
| Nulliparous or parous with no previous GDM | |||
| Parous: no previous GDM | 0.4545 | −0.78850 | |
| Age in years—35 | 1.0841 | 0.08070 | |
| Weight in kg—69 | 1.0389 | 0.03810 | |
| Height in cm—164 | 0.9426 | −0.05910 | |
| 1st-degree relative with DM | 2.5427 | 0.93320 | |
| 2nd-degree relative with DM | 1.7984 | 0.58690 | |
| Ovulation drugs | 1.6019 | 0.47120 | |
| Black racial origin | 1.5780 | 0.45620 | |
| East Asian racial origin | 2.9232 | 1.07270 | |
| South Asian racial origin | 2.3165 | 0.84010 | |
| Birth weight z-score of previous pregnancy | 1.2520 | 0.22470 |
| Pregnancy | FPR (%) | DR (LCL–UCL) % |
|---|---|---|
| Singleton | 10.0 | 221/517; 42.8 (38.4–47.1) |
| Twins | 26.9 | 57/90; 63.3 (52.5–73.3) |
| Singleton | 20.0 | 300/517; 58.0 (53.6–62.3) |
| Twins | 47.0 | 73/90; 81.1 (71.5–88.6) |
| Singleton | 40.0 | 386/517; 74.7 (70.7–78.4) |
| Twins | 71.1 | 82/90; 91.1 (83.2–96.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buerger, O.; Elger, T.; Varthaliti, A.; Syngelaki, A.; Wright, A.; Nicolaides, K.H. First-Trimester Screening for Gestational Diabetes Mellitus in Twin Pregnancies. J. Clin. Med. 2021, 10, 3814. https://doi.org/10.3390/jcm10173814
Buerger O, Elger T, Varthaliti A, Syngelaki A, Wright A, Nicolaides KH. First-Trimester Screening for Gestational Diabetes Mellitus in Twin Pregnancies. Journal of Clinical Medicine. 2021; 10(17):3814. https://doi.org/10.3390/jcm10173814
Chicago/Turabian StyleBuerger, Olga, Tania Elger, Antonia Varthaliti, Argyro Syngelaki, Alan Wright, and Kypros H. Nicolaides. 2021. "First-Trimester Screening for Gestational Diabetes Mellitus in Twin Pregnancies" Journal of Clinical Medicine 10, no. 17: 3814. https://doi.org/10.3390/jcm10173814
APA StyleBuerger, O., Elger, T., Varthaliti, A., Syngelaki, A., Wright, A., & Nicolaides, K. H. (2021). First-Trimester Screening for Gestational Diabetes Mellitus in Twin Pregnancies. Journal of Clinical Medicine, 10(17), 3814. https://doi.org/10.3390/jcm10173814